

Research Advances in the Application of AI for Preoperative Measurements in Total Knee Arthroplasty

Abstract
:1. Introduction
2. Traditional Plain Film Radiographic Measurements
3. Digital Templating Measurements
4. Computer Navigation Technology-Aided Measurement
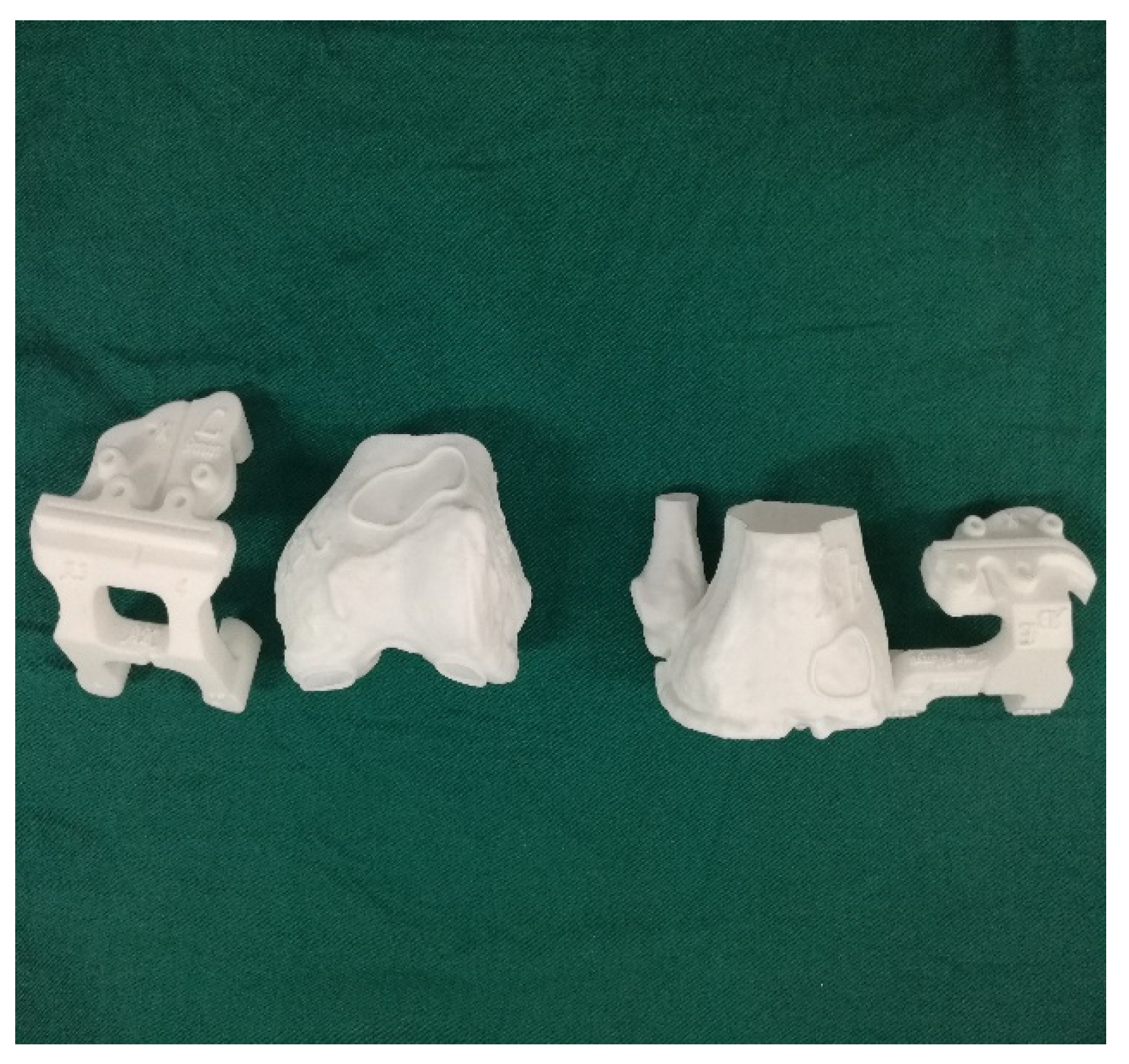
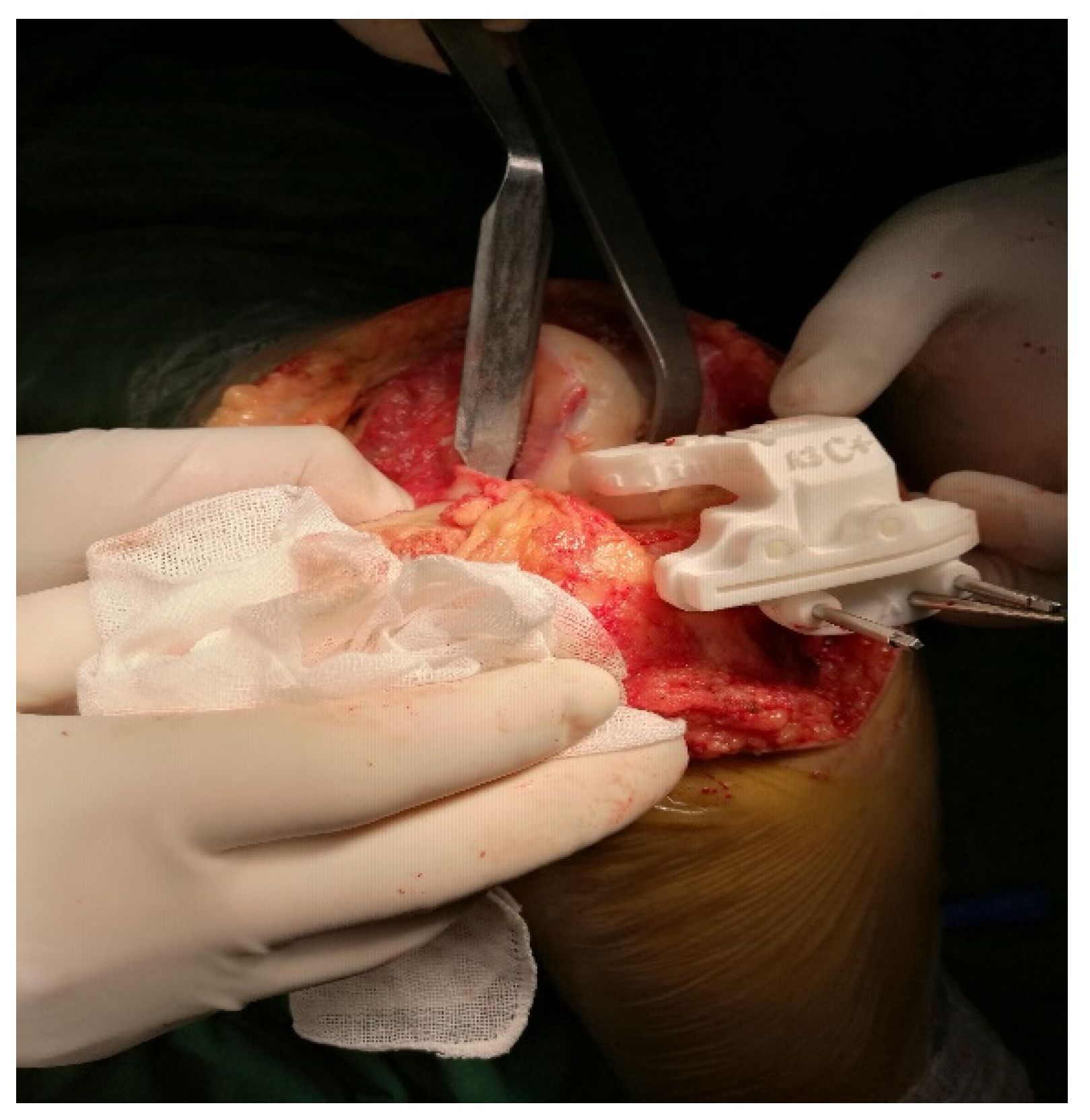
5. Patient-Specific Instrumentation Measurement Technology
6. Preoperative Planning of Robot-Assisted TKA
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bothra, V.; Lemon, G.; Lang, D. Reliability of templating in estimating the size of uni-condylar knee arthroplasty. J. Arthroplast. 2003, 18, 780–783. [Google Scholar] [CrossRef]
- Kasis, A.G.; Pacheco, R.J.; Hekal, W.; Farhan, M.J.; Smith, D.M.; Ali, A.M. The precision and accuracy of templating the size of unicondylar knee arthroplasty. Knee 2004, 11, 395–398. [Google Scholar] [CrossRef]
- Arora, J.; Sharma, S.; Blyth, M. The role of pre-operative templating in primary total knee replacement. Knee Surg. Sport. Traumatol. Arthrosc. 2005, 13, 187–189. [Google Scholar] [CrossRef]
- Levine, B.; Fabi, D.; Deirmengian, C. Digital templating in primary total hip and knee arthroplasty. Orthopedics 2010, 33, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Schotanus, M.G.; Schoenmakers, D.A.; Sollie, R.; Kort, N.P. Patient-specific instruments for total knee arthroplasty can accurately predict the component size as used peroperative. Knee Surg. Sport. Traumatol. Arthrosc. 2017, 25, 3844–3848. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Z.; Li, G. Construction of 3D human distal femoral surface models using a 3D statistical deformable mode. J. Biomech. 2011, 44, 2362–2368. [Google Scholar] [CrossRef]
- Zheng, G.; Gollmer, S.; Schumann, S.; Dong, X.; Feilkas, T.; Ballester, M.A.G. A 2D/3D correspondence building method for reconstruction of a patient-specific 3D bone surface model using point distribution models and calibrated X-ray images. Med. Image Anal. 2009, 13, 883–899. [Google Scholar] [CrossRef]
- Du, H.; Zhang, J.; Tang, H.; Lv, M.; Zhou, Y.X. Observation on the effect of computer-assisted navigation artificial knee arthroplasty. Shandong Med. 2014, 54, 74–77. [Google Scholar]
- Mason, J.B.; Fehring, T.K.; Estok, R.; Banel, D.; Fahrbach, K. Meta-analysis of alignment outcomes in computer-assisted total knee arthroplasty surgery. J. Arthroplast. 2007, 22, 1097–1106. [Google Scholar] [CrossRef] [PubMed]
- Cheng, T.; Zhang, G.; Zhang, X. Imageless navigation system does not improve component rotational alignment in total knee arthroplasty. J. Surg. Res. 2011, 171, 590–600. [Google Scholar] [CrossRef]
- Zhao, L.; Xu, F.; Lao, S.; Zhao, J.; Wei, Q. Comparison of the clinical effects of computer-assisted and traditional techniques in bilateral total knee arthroplasty: A meta-analysis of randomized controlled trials. PLoS ONE 2020, 15, e0239341. [Google Scholar] [CrossRef] [PubMed]
- Stiehl, J.B.; Konermann, W.H.; Haaker, R.G.; Saragaglia, D.; Picard, F. Computer-assisted implantation of total knee endoprosthesis with no preoperative imaging: The kinematic model. Navig. Robot. Total Jt. Spine Surg. 2004, 22, 226–233. [Google Scholar]
- Eric, J.H. Computer-assisted orthopaedic surgery: A new paradigm. Tech. Orthop. 2003, 18, 221–229. [Google Scholar]
- Fehring, T.K.; Mason, J.B.; Moskal, J.; Pollock, D.C.; Mann, J.; Williams, V.J. When computer-assisted knee replacement is the best alternative. Clin. Orthop. Relat. Res. 2006, 452, 132–136. [Google Scholar] [CrossRef] [PubMed]
- Selvanayagam, R.; Kumar, V.; Malhotra, R.; Srivastava, D.N.; Digge, V.K. A prospective randomized study comparing navigation versus conventional total knee arthroplasty. J. Orthop. Surg. 2019, 27, 2309499019848079. [Google Scholar] [CrossRef]
- Hanada, M.; Furuhashi, H.; Matsuyama, Y. Investigation of the control of rotational alignment in the tibial component during total knee arthroplasty. Eur. J. Orthop. Surg. Traumatol. 2019, 29, 1313–1317. [Google Scholar] [CrossRef] [PubMed]
- Thiengwittayaporn, S.; Fusakul, Y.; Kangkano, N.; Jarupongprapa, C.; Charoenphandhu, N. Hand-held navigation may improve accuracy in minimally invasive total knee arthroplasty: A prospective randomized controlled trial. Int. Orthop. 2016, 40, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Goh, G.S.H.; Liow, M.H.L.; Lim, W.S.R.; Tay, D.K.J.; Yeo, S.J.; Tan, M.H. Accelerometer-based navigation is as accurate as optical computer navigation in restoring the joint line and mechanical axis after total knee arthroplasty: A prospective matched study. J. Arthroplast. 2016, 31, 92–97. [Google Scholar] [CrossRef]
- Iorio, R.; Mazza, D.; Drogo, P.; Bolle, G.; Conteduca, F.; Redler, A.; Ferretti, A. Clinical and radiographic outcomes of an accelerometer-based system for the tibial resection in total knee arthroplasty. Int. Orthop. 2015, 39, 461–466. [Google Scholar] [CrossRef]
- Nam, D.; Nawabi, D.H.; Cross, M.B.; Heyse, T.J.; Mayman, D.J. Accelerometer-based computer navigation for performing the distal femoral resection in total knee arthroplasty. J. Arthroplast. 2012, 27, 1717–1722. [Google Scholar] [CrossRef]
- Novoa-Parra, C.D.; Sanjuan-Cerveró, R.; Franco-Ferrando, N.; Larrainzar-Garijo, R.; Egea-Castro, G.; Lizaur-Utrilla, A. Complications of computer-assisted navigation in total knee replacement: Retrospective cohort of eight hundred and seventy eight consecutive knees. Int. Orthop. 2020, 44, 2621–2626. [Google Scholar] [CrossRef] [PubMed]
- Blue, M.; Douthit, C.; Dennison, J.; Caroom, C.; Jenkins, M. Periprosthetic fracture through a unicortical tracking pin site after computer navigated total knee replacement. Case Rep. Orthop. 2018, 2018, 2381406. [Google Scholar] [CrossRef]
- Kamara, E.; Berliner, Z.P.; Hepinstall, M.S.; Cooper, H.J. Pin site complications associated with computer-assisted navigation in hip and knee arthroplasty. J. Arthroplast. 2017, 32, 2842–2846. [Google Scholar] [CrossRef]
- Brown, M.J.; Matthews, J.R.; Bayers-Thering, M.T.; Phillips, M.J.; Krackow, K.A. Low incidence of postoperative complications with navigated total knee arthroplasty. J. Arthroplast. 2017, 32, 2120–2126. [Google Scholar] [CrossRef]
- Smith, T.J.; Siddiqi, A.; Forte, S.A.; Judice, A.; Sculco, P.K.; Vigdorchik, J.M.; Springer, B.D. Periprosthetic fractures through tracking pin sites following computer navigated and robotic total and unicompartmental knee arthroplasty: A systematic review. JBJ Rev. 2021, 9, e20.00091. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.Z.; Pei, G.X.; Lu, S.; Li, Z.J.; Zhao, J.M.; Wang, Y.W. Establishing lower-extremity mechanical axis by computer-aided design and its application in total knee arthroplasty. Chin. J. Orthop. 2013, 33, 1196–1203. [Google Scholar] [CrossRef]
- Levengood, G.A.; Dupee, J. Accuracy of coronal plane mechanical alignment in a customized, individually made total knee replacement with patient-specific instrumentation. J. Knee Surg. 2018, 31, 792–796. [Google Scholar] [CrossRef] [PubMed]
- Tian, S.C.; Yao, Q.Q.; Yin, X.D.; Liu, S.; Zhou, J.; Hu, J.; Wang, L.M. Effects of iASSIST navigation system and personal specific instrument assisted total knee arthroplasty in the treatment of osteoarthritis. Chin. J. Surg. 2017, 55, 423–429. [Google Scholar]
- Qiu, B.; Tang, B.S.; Deng, B.Y.; Liu, F.; Liu, F.; Zhen, D.; Zhu, W.M.; Zhang, M.J. Intelligentized surgery based on 3D printing technology for personalized total knee arthroplasty. Chin. J. Orthop. Trauma 2016, 18, 35–41. [Google Scholar] [CrossRef]
- Pauzenberger, L.; Munz, M.; Brandl, G.; Frank, J.K.; Heuberer, P.R.; Laky, B.; Anderl, W. Patient-specific instrumentation improved three-dimensional accuracy in total knee arthroplasty: A comparative radiographic analysis of 1257 to tall knee arthroplasties. J. Orthop. Surg. Res. 2019, 14, 437. [Google Scholar] [CrossRef] [PubMed]
- Netravali, N.A.; Shen, F.; Park, Y.; Bargar, W.L. A perspective on robotic assistance for knee arthroplasty. Adv. Orthop. 2013, 2013, 970703. [Google Scholar] [CrossRef] [PubMed]
- Jacofsky, D.J.; Allen, M. Robotics in Arthoplasty: A Comprehensive Review. J. Arthroplast. 2016, 31, 2353–2363. [Google Scholar] [CrossRef] [PubMed]
- Magnussen, R.A.; Trojani, C.; Granan, L.P.; Neyret, P.; Colombet, P.; Engebretsen, L.; SFA Revision ACL Group. Patient demographics and surgical characteristics in ACL revision: A comparison of French, Norwegian, and North American cohorts. Knee Surg. Sport. Traumatol. Arthrosc. 2015, 23, 2339–2348. [Google Scholar] [CrossRef]
- Seon, J.K.; Song, E.K.; Park, S.J. Comparison of minimally invasive unicompartmental knee arthroplasty with or without a navigation system. J. Arthroplast. 2009, 24, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Liow, M.H.L.; Chin, P.L.; Tay, K.J.D.; Chia, S.L.; Lo, N.N.; Yeo, S.J. Early experiences with robot-assisted total knee arthroplasty using the DigiMatch™ ROBODOC® surgical system. Singap. Med. J. 2014, 55, 529–534. [Google Scholar] [CrossRef]
- Dettmer, M.; Kreuzer, S.W. Bi-Unicompartmental, robot-assisted knee arthroplasty. Oper. Tech. Orthop. 2015, 25, 155–162. [Google Scholar] [CrossRef]
- Davies, B.; Jakopec, M.; Harris, S.J.; Baena, F.R.Y.; Barrett, A.; Evangelidis, A.; Cobb, J. Active-constraint robotics for surgery. Proc. IEEE 2006, 94, 1696–1704. [Google Scholar] [CrossRef]
- van der List, J.P.; Chawla, H.; Joskowicz, L.; Pearle, A.D. Current state of computer navigation and robotics in unicompartmental and total knee arthroplasty: A systematic review with meta-analysis. Knee Surg. Sport. Traumatol. Arthrosc. 2016, 24, 3482–3495. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Z.J.; Liu, Y.C. A new computer-assisted total knee arthroplasty system: WATO. Chin. Orthop. Jt. Surg. 2009, 2, 279283. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Name | Author(s) |
|---|---|
| Artificial Intelligence: A Modern Approach | Stuart Russell, Peter Norvig |
| Human-Compatible Artificial Intelligence and the Problem of Control | Stuart Russell |
| The Sentient Machine: The Coming Age of Artificial Intelligence | Amir Husain |
| Deep Medicine–How Artificial Intelligence Can Make Healthcare Human Again | Eric Topol |
| life 3.0: Being Human in the Age of Artificial Intelligence | Max Tegmark |
| The Society of Mind | Marvin Minsky |
| DEEP MEDICINE | Eric Topol |
| Deep Learning | Ian Goodfellow, Yoshua Bengio, Aaron Courville |
| Date | Event |
|---|---|
| 1956 | Dartmouth Conference–birth of AI |
| 1959 | Arthur Lee Samuel put forward the concept of Advice Taker–birth of machine learning |
| concept | |
| 1966 | Joseph invented ELIZA, a robot that can chat–the first man–machine dialogue |
| 1973 | Waseda University in Japan has built the first humanoid robot, WABOT-1 |
| 1997 | DEEP BLUE of IBM won the man–machine battle in the chess match |
| 2006–2009 | ImageNet was invented–the foundation of image recognition technology of AI |
| 2016 | The emergence of AlphaGo raised the world’s expectation of AI to an unprecedented level |
| 2018–2019 | IBM AI debate robot “IBM Project Debater” is the champion of human debate |
| Robot Systems | Company | Classification | Application |
|---|---|---|---|
| ROBODOC | Think Surgical (Fremont, CA, USA) | active | Hip/knee arthroplasty |
| CASPAR | Universal Robot Systems Ortho (Odense, Denmark) | active | Hip arthroplasty |
| ACROBOT | Acrobot (London, UK) | active | Hip arthroplasty |
| Rio MAKO robot | Stryker (karamazu, MI, USA) | semi-active | Hip/knee arthroplasty |
| NAVIO | Blue Belt Technologues (Texas, USA) | semi-active | Condylar/knee arthroplasty |
| iBlock | OMNIlife (Fort, TX, USA) | semi-active | Knee arthroplasty |
| ROSA | Zimmer (Warsaw, IA, USA) | semi-active | Spinal surgery/knee arthroplasty |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, W.; Xu, S.-M.; Zhang, D.-B.; Bi, H.-Y.; Gu, G.-S. Research Advances in the Application of AI for Preoperative Measurements in Total Knee Arthroplasty. Life 2023, 13, 451. https://doi.org/10.3390/life13020451
Li W, Xu S-M, Zhang D-B, Bi H-Y, Gu G-S. Research Advances in the Application of AI for Preoperative Measurements in Total Knee Arthroplasty. Life. 2023; 13(2):451. https://doi.org/10.3390/life13020451
Chicago/Turabian StyleLi, Wei, Sheng-Ming Xu, De-Bao Zhang, Huang-Yi Bi, and Gui-Shan Gu. 2023. "Research Advances in the Application of AI for Preoperative Measurements in Total Knee Arthroplasty" Life 13, no. 2: 451. https://doi.org/10.3390/life13020451
APA StyleLi, W., Xu, S. -M., Zhang, D. -B., Bi, H. -Y., & Gu, G. -S. (2023). Research Advances in the Application of AI for Preoperative Measurements in Total Knee Arthroplasty. Life, 13(2), 451. https://doi.org/10.3390/life13020451