

Diagnosis of Fibrotic Hypersensitivity Pneumonitis: Is There a Role for Biomarkers?

 , , ,
, , ,
Abstract
:1. Introduction
2. Biomarkers in Fibrotic HP
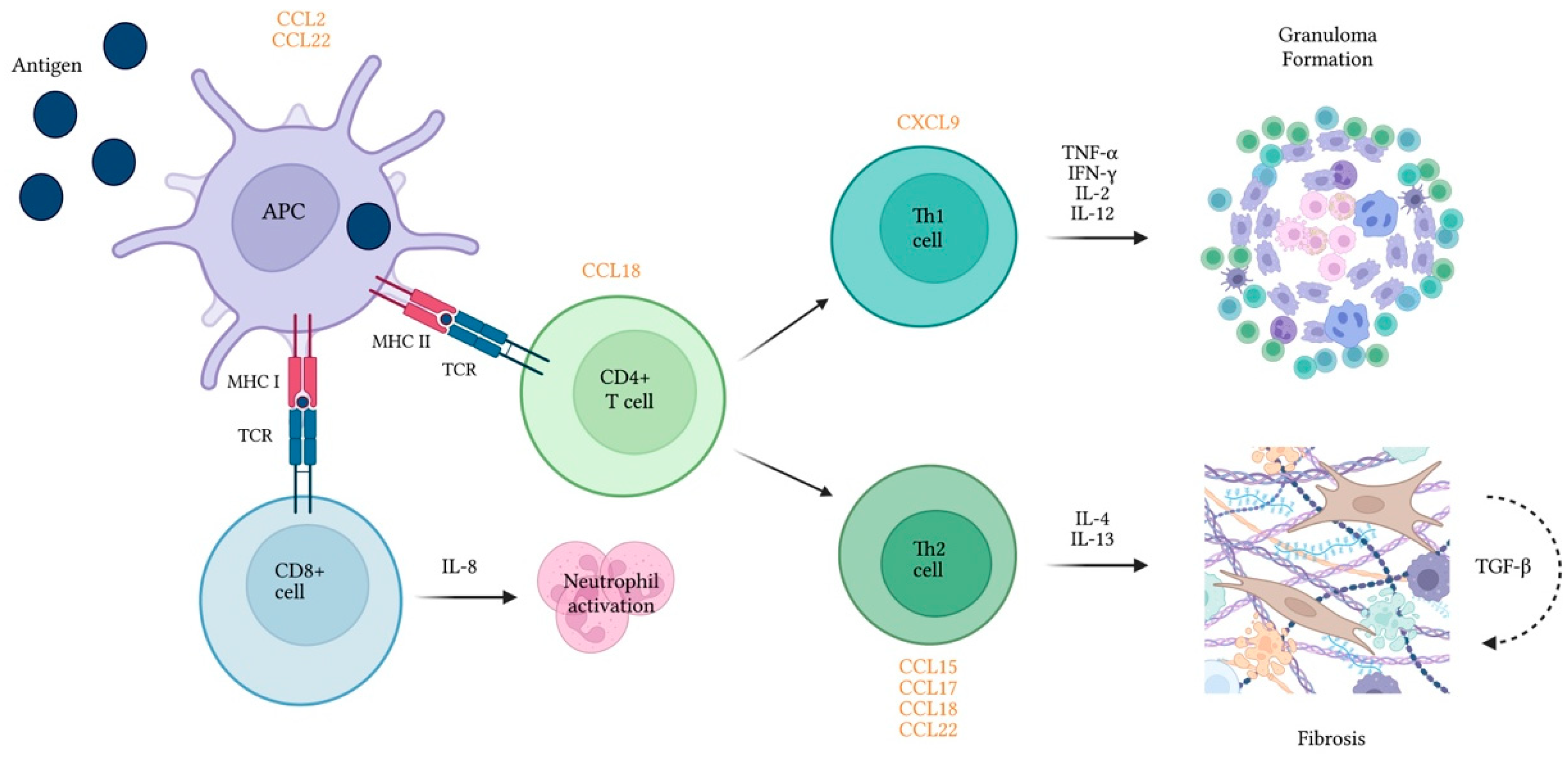
2.1. Immune Dysregulation
2.1.1. BAL Lymphocyte Count
2.1.2. BAL CD4/CD8 Ratio
2.1.3. Cytokines and Cytokine Receptors
2.1.4. Chemokines and Receptors
2.1.5. Specific IgG Antibodies
2.1.6. Markers of Macrophage Activation
YKL-40
2.1.7. Acute Phase Reactants
Serum Amyloid A (SSA)

{kind=link}
{kind=link}
| Biomarker | Investigator | Type of Study | Population/Methods | Threshold Analysis (Cutoffs)/Other Results | Conclusion(s) of Interest | Main Limitations |
|---|---|---|---|---|---|---|
| BAL Lymphocytes | Patolia et al. [60] | Systematic review and meta-analysis | Studies on BAL cell counts in ILDs; comparison of BAL% lymphocytes in HP vs. IPF or sarcoidosis | No 20% BAL lymphocytes: fHP vs. IPF: Sen 69% Sp 61% fHP vs. sarcoidosis: Sen 69% Sp 26% | BAL lymphocytes: Higher in HP vs. IPF Higher in HP vs. sarcoidosis | No RCTs Possible incorporation bias of the studies reviewed cHP used as surrogate for fibrotic HP |
| Adderley et al. [61] | Systematic review and meta-analysis | Studies on BAL cell analysis in ILDs; estimation of pooled BAL% lymphocytes for cHP vs. non-cHP ILDs | Yes 21.3% BAL lymphocytes: CHP vs. non-CHP ILD Sen 66.5% Sp 65.9% 21% BAL lymphocytes CHP vs. IPF/non-IPF IIP Sen 70.7% Sp 67.6% | BAL lymphocytes: Higher in cHP vs. non-cHP ILD | No RCTs Possible incorporation bias affecting the included studies Heterogeneity of cHP diagnostic criteria among studies | |
| BAL CD4/CD8 cell ratio | Adderley et al. [61] | Systematic review and meta-analysis | Studies on BAL cell analysis in ILDs; estimation of pooled BAL ratios for CHP vs. non-cHP ILDs | No. CD4/CD8 Ratio pooled estimates: cHP 1.6 IPF 1.6 Sarc 4.6 | CD4/CD8 Ratio: CHP vs. IPF not different cHP ≠ sarcoidosis | Small sample size of non-CHP groups Possible incorporation bias affecting the included studies High between-study heterogeneity |
| Barrera et al. [9] | Prospective cohort | Patients with aHP, saHP, cHP and healthy controls; comparison of BAL CD4/CD8 and cytokines in BAL cell culture supernatant | No. Median CD4/CD8 Ratio: cHP 3.05 SaHP 1.3 Controls 1.3 IL-4 (pg/mL): cHP 80 saHP 25 IFN-γ (pg/mL): cHP 3.82 saHP 100 TGF-β1: No difference | CD4/CD8 Ratio: Higher in CHP vs. subacute HP and healthy controls | Former diagnostic criteria and classification of HP Only Pidgeon Breeder’s Disease included Single center study: small sample | |
| Cytokines, Chemokines and receptors | Ye et al. [74] | Cross-sectional study | Patients with aHP, cHP and healthy controls; comparison of cytokine concentration in alveolar macrophage culture supernatant | No. IL-12 (pg/mL): cHP 15.4 Controls 1.1 IL-18 (pg/mL): aHP 201 cHP 224 Controls 56 TNF-α (pg/mL): aHP 3219 cHP 1522 controls 249 | No difference between aHP and cHP | Own diagnostic and classification criteria Single center study; Small sample size |
| Matěj et al. [81] | Cross-sectional study (case-control analysis) | Patients with HP and sarcoidosis; comparison of BAL cytokine concentration at diagnosis | No IL-4R (pg/mL): HP 1182 Sarc 303 PAR-2 (pg/mL): HP 2009 Sarc 330 TGF- β and TNF-α: No difference | PAR-2 as a potential tool in the differential diagnosis | Single center study; small sample HP diagnostic criteria and inciting antigens not detailed | |
| Sterclova et al. [82] | Cross-sectional study (case-control analysis) | Patients with cHP and sarcoidosis; determination of IL-4/IL-4R axis role | No. IL-4Ra: cHP 1190 Sarc 303 IL-4: No difference | BAL IL-4Ra significantly higher in cHP vs. sarcoidosis | Own HP diagnostic criteria Single center study; Small sample size | |
| Stijn et al. [85] | Cross-sectional study (case-control analysis) | Patients with cHP, IPF and controls without pulmonary disease. BAL protein comparison (multiplex) at diagnosis | No. TGF-β1 lower in cHP vs. IPF and controls IL-8 lower in cHP vs. controls MMP-8, MMP-9, MCP-1, MDC, MPO and Protein-C higher in cHP vs. controls IL-17a and IL-23, RAGE, SP-C, TIMP-1, fibronectin, eotaxin, IL-17A, IL-23, PARC, RANTES, TSLP, PlGF, FGFb, and tissue factor: no difference | No considerations on use as tools in differential diagnosis. | Multidisciplinary meeting diagnoses—criteria and inciting antigens not detailed Single center study; Small sample size | |
| Bruzova et al. [86] | Cross-sectional study (case-control analysis) | Patients with IPF, fIIP, CTD-ILD and cHP Comparison of BAL supernatant protein levels | No TNF-α HP 3.41 fIIP 1.52 CTD-ILD 2.33 IL4R-α and PAR2: no differences MMP-7: no differences | TNF-α higher in cHP vs. fIIP and CTD-ILD No differences in IL-4Ra, PAR-2 and MMP-7 TNF-α as a potential diagnostic tool in IIP | Inciting antigens not detailed Predominance of non-fibrotic cases in HP Single center study; relatively small sample | |
| Sterclova et al. [87] | Cross-sectional study (case-control analysis) | Patients with IPF and cHP. Comparison of BAL supernatant protein levels | No. I-TAC/CXCL11, IP-10/CXCL10, IL-8/ CXCL8 and ENA-78/CXCL5: no differences | No difference in the studied proteins | Former diagnostic criteria of IPF; own criteria of HP and little detailed Inciting antigens not detailed Single center study; Small sample size | |
| Sugiyama et al. [88] | Cross-sectional study (case-control analysis) | Patients with summer-type aHP, pulmonary sarcoidosis and control. Comparison of BAL supernatant protein levels | No. IL-8: aHP 30.8 Sarc 11.7 Controls 7.4 MCP-1: aHP 34.8 Sarc 45 Controls 10.6 | IL-8 higher in HP than sarcoidosis MCP-1 higher in aHP vs. controls, not sarcoidosis | Only summer-type HP included Single center study; Small sample size | |
| Inoue et al. [89] | Cross-sectional study (case-control analysis) | Patients with HP and other ILDs; comparison of BAL and serum potential biomarkers after IPT with pigeon extract in avian HP and other ILDs (including non-avian HP) | No BAL G-CSF, IL-6, and IL-17 higher after IPT only in avian HP Serum leukocytes and neutrophils elevated after IPT only in avian HP | Neutrophils and the cytokine/chemokine-associated millieu increase with IPT in avian HP but changes in cytokines/chemokines should be carefully interpreted (risks of multiple comparisons) | Former diagnostic/classification criteria Single center study; small sample Only avian IPT performed | |
| Watanabe et al. [91] | Cross-sectional study (case-control analysis) | Patients with cHP, IPF and healthy controls; comparison of serum and BAL CC15 | No Serum (μg/mL): cHP 29.1 IPF 19.7 controls19.5 BAL (μg/mL): cHP 0.76 IPF 0.54 | Serum CCL15 higher in cHP vs. IPF; | Former diagnostic/classification criteria Single center study; Small sample size The assessment of inciting antigens was performed using precipitins only | |
| Nukui et al. [93] | Retrospective cohort (case-control analysis) | Patients with cHP and healthy volunteers; comparison of serum CXCL9, CCL17 and KL-6 | No KL-6 (U/mL): cHP 1182 controls 184 CXCL9 (pg/mL) cHP 19.3 controls 10.5 CCL17 (pg/mL) cHP 543 controls 274 | KL-6, CXCL9 and CCL17 higher in avian cHP vs. healthy controls | Former diagnostic criteria Only avian cHP defined only by IPT | |
| Cai et al. [95] | Cross-sectional study (case-control analysis) | Patients with HP and other ILDs; comparison of serum and BAL CCL18 levels | No Serum (ng/mL): HP 190 IPF 149 COP 146 Sarc 108 BAL (ng/mL) HP 13 IPF 6 RB-IL/DIP 54 COP 5 Sarc 7 iNSIP 9 | CL18 level highest in HP among the investigated ILDs | Own diagnostic criteria for HP and former for IIP; saHP and cHP considered in the same group Single center study; Small sample size | |
| Garcia de Alba [97] | Cross-sectional study (case-control analysis) | Patients with cHP and healthy controls; comparison of serum and BAL CXCL12 levels | No Serum (pg/mL): cHP 2302 controls 813 BAL (pg/mL) cHP 493 controls undetectable | CXCL12 levels higher in cHP vs. controls. No considerations on use as diagnostic tool | Own/former HP criteria Only bird-related HP Single center study; Small sample size | |
| Suga et al. [98] | Cohort study (case-control analysis) | Patients with ILD (IPF, AIP, CTD-ILD, OP and HP); Comparison of serum and BAL MCP-1/CCL2 levels | No BAL levels higher in IPF vs. HP Serum levels higher in IPF, Sarc, and CTD-ILD vs. HP and controls | Differences in the pattern of MCP-1 in BALF and serum may help in the differential diagnosis of ILD. | Former diagnostic criteria Single center study; Small sample size | |
| Specific IgG antibodies | Jenkins et al. [104] | Systematic Review and meta-analysis | Studies on serum IgG testing and questionnaires in HP | No. HP vs. other ILDs Sen 83% Sp 68% HP vs. E-controls Sen 90% Sp 91% HP vs. u-controls Sen 93% Sp 100% | IgG testing insufficient to distinguish HP from other ILDs but can be useful in screening for exposures and provide supportive of HP | No RCTs Small studies included Risk of incorporation bias |
| Chitinase-3-like protein 1 (YKL-40) | Long et al. [114] | Retrospective cohort (case-control analysis) | Patients with HP, IPF, iNSIP, COP and healthy controls; Comparison of serum and BAL YKL-40 | Yes Serum (ng/mL) HP 127 IPF 214 iNSIP 184 COP 213 controls 39 a/saHP 179 cHP 117 BAL (ng/mL) HP 21 IPF 9 a/saHP 42 cHP 15 control 3 Optimal cutoff serum: HP vs. controls: 47 AUC 0.90 HP vs. IPF: 134 AUC 0.727 | Serum YKL-40 higher in HP vs. controls but lower vs. other ILDs BAL YKL-40 higher in HP vs. controls and IPF No considerations on use as diagnostic tool | Former diagnostic and classification criteria Single center study; Small sample size |
| Sanchez-Diaz et al. [115] | Cross-sectional study (case-control analysis) | Patients with HP, IPF, sarcoidosis and healthy controls; Comparison of serum YKL-40 and KL-6 | Yes Serum YKL-40 HP 56 ng/mL IPF NM Optimal cutoff for HP vs. IPF: Serum YKL-40 121 ng/mL AUC 0.741 Serum KL-60: 1441 U/mL AUC 0.702 | Serum HP higher in HP vs. IPF | Ancient diagnostic criteria; own classification criteria Single center study; Small sample size | |
| Serum Amyloid A | Vietri et al. [127] | Prospective cohort (case-control analysis) | Patients with IPF and non-IPF ILDs including sarcoidosis, cHP, PLC and healthy controls; comparison of SAA concentrations in the different groups | No SAA: IPF6418 ng/mL; cHP 4494 ng/mL Optimal cutoff for IPF vs. cHP: 5397 ng/mL AUC 0.79 | SAA Higher in IP levels vs. other ILDs; potential to differentiate IPF from cHP | Diagnostic criteria of diseases not detailed; inciting antigens not detailed Single center study; Small sample size |
| Bergantini et al. [128] | Coss-sectional study (case-control analysis) | Patients with IPF, sarcoidosis, cH. Comparison of fibrotic/inflammatory markers | Yes. KL-6 (U/mL) cHP 1146 Sarc 537 IPF 2062 SAA (ng/mL) cHP 4022 Sarc 4370 IPF 7031 Optimal cutoff for cHP vs. IPF: KL-6: 2206 AUC 0.74 SAA: 53,971 AUC 0.85 KL-6 + SAA: AUC 0.79 | KL-5 different in cHP vs. IPF and sarcoidosis SAA different in cHP vs. IPF Combined panel might improve diagnostic accuracy in multidisciplinary setting | Diagnostic and classification criteria not detailed Single center study; Small sample size |
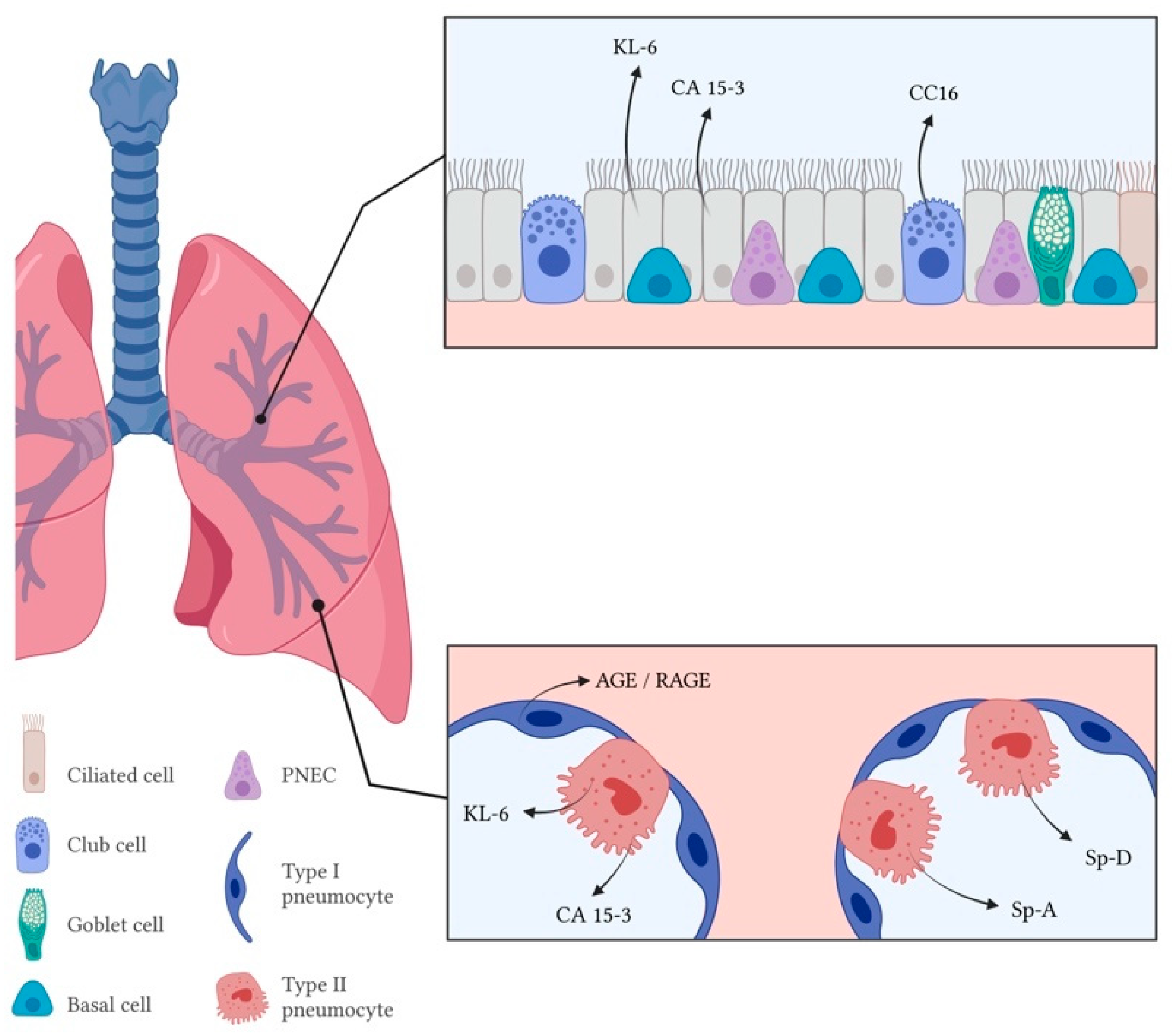
2.2. Epithelial Cell Dysfunction
2.2.1. Mucin-Associated Antigens
Krebs Von Den Lungen-6 (KL-6)
CA 15-3 and CA125
2.2.2. Surfactant-Associated Proteins
2.2.3. Club-Cell Protein
2.2.4. AGE and RAGE
| Biomarker | Investigator | Type of Study | Population(s)/Methods | Threshold Analysis (Cutoffs)/Other Results | Conclusion(s) of Interest | Main Limitations |
|---|---|---|---|---|---|---|
| Krebs von der Lungen (KL-6) and surfactant proteins (SPs) | Takahashi et al. [137] | Cross-sectional study (case-control analysis) | Dairy farmers with and without HP (controls); comparison of serum KL-6 levels in HP, precipitin positive (Ab+) and precipitin negative (Ab−) controls | No KL-6 (U/mL): HP 1263 Ab+ controls: 328; Ab− controls: 207 | KL-6 higher in farmers with HP vs. controls and higher in seropositive vs. seronegative controls KL-6 higher in individuals after diagnosis vs. before diagnosis | Only farmers’ lung disease; Single center study; Small sample size |
| Okamoto et al. [142] | Retrospective longitudinal study (case-control analysis) | Patients with cHP, aHP, IPF, CVD-ILD; Comparison and validation of serum KL-6 and SP-D | Yes KL-6 and SP-D higher in aHP and cHP vs. IPD, CVD-ILD and sarcoidosis Not different in aHP vs. cHP Optimal cutoff for cHP vs. IPF: KL-6 1115 U/mL AUC 0.771 SP-D 209 ng/mL AUC 0.729 KL-6 and SP-D lower after 1-month steroid therapy | Higher KL-6 and SP-D shoul raise suspicion of HP Potential use in disease management | Own HP diagnostic criteria of HP; Former diagnostic criteria of IPF and sarcoidosis; Single center study. | |
| Onishi et al. [143] | Cross-sectional study (case-control analysis) | Patients with cHP and IPF; comparison of serum biomarkers | No KL-6: cHP 1506 U/mL IPF 914 U7 mL SPD cHP 235 ng/mL IPF 156 ng/mL | KL-6 and SP-D higher in cHP vs. IPF Both biomarkers included in proposed composite criteria for chronic summer-type HP | Only summer-type HP Former diagnostic/classification criteria Single center study; small sample | |
| Janssen et al. [155] | Retrospective longitudinal study (case-control analysis) | Patients with HP and healthy exposed and unexposed controls; comparison and validation of serum KL-6 and SP-D | Yes KL-6: cHP 883 U/mL E-controls 371 U/mL U-controls 177 U/mL SP-D: cHP 201 ng/mL U-controls 68 ng/mL Optimal cutoff: KL-6 275 U/mL AUC 0.98 SP-D 98 ng/mL AUC 0.96 | KL-6 and SP-D decrease with antigen avoidance; potential markers of disease | Criteria for diagnosis and classification of HP not detailed Only bird fancers’ lung disease Single center study; Small sample size | |
| Hamm et al. [157] | Cross-sectional study (case-control analysis) | Patients with HP, sarcoidosis and controls without ILD; comparsion of BAL supernatant SP-A levels | No BAL SpA: HP 9 μg/mL Sarc 8 μg/mL Controls 4.0μg/mL | BAL SP-A are elevated in sarcoidosis and HP but not specific or diagnostic | Own diagnostic criteria for HP and sarcoidosis Single center study; Small sample size | |
| Phelps et al. [159] | Cross-sectional study (case-control analysis) | Patients with IPF, HP and controls; comparison of SP-A | No BAL SP-A: HP 13.11 ug/mL IPF 7.99 μg/mL controls 4.77 μg/mL | BAL SP-A elevated in IPF (both vs. HP and controls); significance of the finding incompletely understood | IPF diagnostic criteria not detailed; Own HP criteria Only avian antigen-induced HP Single center study; Small sample size | |
| Club-cell protein (CC16) | Buendia-Roldan et al. [169] | Cross-sectional study (case-control analysis) | Patients with IPF, non-IPF ILD (CTD-ILD + cHP) and healthy controls; comparison and validation of serum and BAL CC16 | Yes. Serum CC16 higher in non-IPF vs. controls Optimal cutoff for IPF vs. non-IPF: 41 ng/mL; AUC 0.68 | High CC16 levels may increase suspicion of IPF and may complement other findings | Outdated diagnostic criteria for IPF and HP Time of blood sample collection not mentioned/Patient treatment at the time not detailed Single center study; Small sample size |
| Barnes et al. [170] | Case-control study | Patients with HP and age-matched controls; comparison of selected serum biomarkers (secondary outcome) | No CC16 HP: 36.3 ng/m controls 15.0 ng/mL | CC16 associated with increased odds of HP | HP diagnosis based on administrative data/partly on clinical unmentioned criteria Patient treatment at the time of sample collectionnot detailed | |
| Advanced glycation end products/Receptor for Advanced glycation end products (AGE/RAGE) | Machahua er al. [183] | Prospective cohort (case-control analysis) | Patients with IPF, cHP, fNSIP and controls; Comparison and validation of serum AGEs, sRAGE and AGEs/sRAGE | Yes Optimal cutoff for cHP vs. NSIP: AGEs 19.25 ug/mL (AUC 0.883); sRAGE 782.6 pg/mL (AUC 0.887); AGE/sRAGE 25.7‰ (AUC 0.882) Optimal cutoff for cHP vs. IPF: AGEs and sRAGE: NM (low AUC), AGE/sRAGE NM (AUC = 0.713) | AGE higher in cHP vs. controls; sRAGE lower in cHP vs. fNSIP and vs. controls IPF vs. cHP: AGE and sRAge not different; AGE/sRAGE as potential diagnostic tools in fibrosing ILDs | Outdated diagnostic criteria for IPF and HP Patient treatment at the time not detailed Single center study; Small sample size |
2.3. Fibrogenesis and ECM Remodeling
Matrix Metalloproteinases (MMPs)
| Biomarker | Investigator | Type of Study | Population(s)/Methods | Threshold Analysis (Cutoffs)/Other Results | Conclusion(s) of Interest | Main Limitations |
|---|---|---|---|---|---|---|
| Matrix metalloproteinases (MMPs) | Rosas et al. [187] | Cross-sectional study (case-control analysis) | Patients with IPF, saHP/cHP, Sarcoidosis, COPD; Comparison of serum protein concentration (multiplex assay) | Yes. MMP7 and MMP1 higher in IPF vs. HP (2.3 and 1.31-fold, respectively) Optimal cutoffs and AUC: not mentioned Combination of high MMP1 + High MMP7: S 96.3% Sp 87.2% | Serum MMP1 and MMP7 as potential biomarkers in the differential diagnosis of IPF and HP | Outdated diagnostic criteria for IPF and HP Only avian inciting antigens/exposure Time of sample collection not mentioned/Patient treatment at the time not detailed Single center study; Small sample size |
| Morais et al. [188] | Cross-sectional study (case-control analysis) | Patients with IPF and non-IPF ILD (including HP); Comparison of serum MMP-7 and MMP-1 | Yes (IPF vs. other ILDs) MMP-1 higher in IPF vs. non-IPF-UIP Optimal cutoff for IPF vs. ther ILDs: MMP-1: 4.15 ng/mL AUC 0.63 MMP-7: 3.91 ng/mL, AUC 0.73 Combination: AUC 0.74 | Potential role of serum MMP-1 and MMP-7 as diagnostic biomarkers in IPF | HP not as independent group; Former diagnostic criteria of IPF and HP Single center study; Small sample size | |
| Maldonado et al. [189] | Cross-sectional study (case-control analysis) | Patients with IPF and non-IPF fibrosis (including fHP) and healthy controls; Comparison and validation of MMP28 concentration in two cohorts | Yes. MMP28 higher in IPF vs. non-IPF and controls; Optimal cutoff for IPF vs. non-IPF: 4.5 ng/mL AUC 0.72 and 0.69 | MMP28 as new biomarker ofr differential diagnosis of IPF with cHP and fibrotic autoimmune driven-ILD | HP not as independent group and diagnostic criteria not detailed | |
| Lipid mediators/Adipokines | D’Alessandro et al. [99] | Cross-sectional study (case-control analysis) | Patients with IPF and fHP; comparison and validation of BAL and serum multiplex lipid profiling | Yes. Optimal cutoff BAL: Apo A1 20.99 ng/mL; Apo C3 3.62 ng/mL Apo C3 3.62 ng/mL. Combined performance: AUC 81% Optimal cutoff serum: Apo A1 12.0 ng/mL; CCL2 0.88 ng/mL Apo C3 11.53 ng/mL. Combined model performance: AUC 93% | BAL Apo A1, adipsin, Apo C3 and APN higher in HP vs. IPF Serum Apo A1 higher in HP; MCP-1 (CCL2) and Apo C3 lower in HP vs. IPF Overall performance better in BAL vs. serum | Diagnostic criteria of fHP not detailed Single center study; Small sample size |
2.4. Other Sources
2.4.1. Metabolic Biomarkers
Lipid Mediators
Adipokines
2.5. Future Directions
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Selman, M.; Pardo, A.; King, T.E., Jr. Hypersensitivity pneumonitis: Insights in diagnosis and pathobiology. Am. J. Respir. Crit. Care Med. 2012, 186, 314–324. [Google Scholar] [CrossRef] [Green Version]
- Riario Sforza, G.G.; Marinou, A. Hypersensitivity pneumonitis: A complex lung disease. Clin. Mol. Allergy 2017, 15, 6. [Google Scholar] [CrossRef] [Green Version]
- Pepys, J.; Riddell, R.W.; Citron, K.M.; Clayton, Y.M. Precipitins Against Extracts of Hay and Moulds in the Serum of Patients with Farmer’s Lung, Aspergillosis, Asthma, and Sarcoidosis. Thorax 1962, 17, 366–374. [Google Scholar] [CrossRef] [Green Version]
- Kobayashi, M.; Stahmann, M.A.; Rankin, J.; Dickie, H.A. Antigens in moldy hay as the cause of farmer’s lung. Proc. Soc. Exp. Biol. Med. 1963, 113, 472–476. [Google Scholar] [CrossRef]
- Bishop, J.M.; Melnick, S.C.; Raine, J. Farmer’s Lung: Studies of Pulmonary Function and Aetiology. Q. J. Med. 1963, 32, 257–278. [Google Scholar]
- Arranz, I.O. Diagnosis and Follow up of Chronic Hypersensitivity Pneumonitis: Utility of Non-Invasive Measurement of Airway Inflammation. Ph.D. Thesis, Universitat Autonoma de Barcelona, Barcelona, Spain, 2016. [Google Scholar]
- Salvaggio, J.E. Robert A. Cooke memorial lecture. Hypersensitivity pneumonitis. J. Allergy Clin. Immunol. 1987, 79, 558–571. [Google Scholar] [CrossRef]
- Vasakova, M.; Selman, M.; Morell, F.; Sterclova, M.; Molina-Molina, M.; Raghu, G. Hypersensitivity Pneumonitis: Current Concepts of Pathogenesis and Potential Targets for Treatment. Am. J. Respir. Crit. Care Med. 2019, 200, 301–308. [Google Scholar] [CrossRef]
- Barrera, L.; Mendoza, F.; Zuniga, J.; Estrada, A.; Zamora, A.C.; Melendro, E.I.; Ramirez, R.; Pardo, A.; Selman, M. Functional diversity of T-cell subpopulations in subacute and chronic hypersensitivity pneumonitis. Am. J. Respir. Crit. Care Med. 2008, 177, 44–55. [Google Scholar] [CrossRef] [Green Version]
- Mitaka, K.; Miyazaki, Y.; Yasui, M.; Furuie, M.; Miyake, S.; Inase, N.; Yoshizawa, Y. Th2-biased immune responses are important in a murine model of chronic hypersensitivity pneumonitis. Int. Arch. Allergy Immunol. 2011, 154, 264–274. [Google Scholar] [CrossRef]
- Kishi, M.; Miyazaki, Y.; Jinta, T.; Furusawa, H.; Ohtani, Y.; Inase, N.; Yoshizawa, Y. Pathogenesis of cBFL in common with IPF? Correlation of IP-10/TARC ratio with histological patterns. Thorax 2008, 63, 810–816. [Google Scholar] [CrossRef] [Green Version]
- Raghu, G.; Remy-Jardin, M.; Ryerson, C.J.; Myers, J.L.; Kreuter, M.; Vasakova, M.; Bargagli, E.; Chung, J.H.; Collins, B.F.; Bendstrup, E.; et al. Diagnosis of Hypersensitivity Pneumonitis in Adults. An Official ATS/JRS/ALAT Clinical Practice Guideline. Am. J. Respir. Crit. Care Med. 2020, 202, e36–e69. [Google Scholar] [CrossRef]
- Fernandez Perez, E.R.; Travis, W.D.; Lynch, D.A.; Brown, K.K.; Johannson, K.A.; Selman, M.; Ryu, J.H.; Wells, A.U.; Tony Huang, Y.C.; Pereira, C.A.C.; et al. Diagnosis and Evaluation of Hypersensitivity Pneumonitis: CHEST Guideline and Expert Panel Report. Chest 2021, 160, e97–e156. [Google Scholar] [CrossRef]
- Richerson, H.B.; Bernstein, I.L.; Fink, J.N.; Hunninghake, G.W.; Novey, H.S.; Reed, C.E.; Salvaggio, J.E.; Schuyler, M.R.; Schwartz, H.J.; Stechschulte, D.J. Guidelines for the clinical evaluation of hypersensitivity pneumonitis. Report of the Subcommittee on Hypersensitivity Pneumonitis. J. Allergy Clin. Immunol. 1989, 84, 839–844. [Google Scholar] [CrossRef]
- Lacasse, Y.; Selman, M.; Costabel, U.; Dalphin, J.C.; Ando, M.; Morell, F.; Erkinjuntti-Pekkanen, R.; Muller, N.; Colby, T.V.; Schuyler, M.; et al. Clinical diagnosis of hypersensitivity pneumonitis. Am. J. Respir. Crit. Care Med. 2003, 168, 952–958. [Google Scholar] [CrossRef] [Green Version]
- Vasakova, M.; Morell, F.; Walsh, S.; Leslie, K.; Raghu, G. Hypersensitivity Pneumonitis: Perspectives in Diagnosis and Management. Am. J. Respir. Crit. Care Med. 2017, 196, 680–689. [Google Scholar] [CrossRef]
- Walsh, S.L.F.; Wells, A.U.; Desai, S.R.; Poletti, V.; Piciucchi, S.; Dubini, A.; Nunes, H.; Valeyre, D.; Brillet, P.Y.; Kambouchner, M.; et al. Multicentre evaluation of multidisciplinary team meeting agreement on diagnosis in diffuse parenchymal lung disease: A case-cohort study. Lancet Respir. Med. 2016, 4, 557–565. [Google Scholar] [CrossRef] [Green Version]
- Travis, W.D.; Costabel, U.; Hansell, D.M.; King, T.E., Jr.; Lynch, D.A.; Nicholson, A.G.; Ryerson, C.J.; Ryu, J.H.; Selman, M.; Wells, A.U.; et al. An official American Thoracic Society/European Respiratory Society statement: Update of the international multidisciplinary classification of the idiopathic interstitial pneumonias. Am. J. Respir. Crit. Care Med. 2013, 188, 733–748. [Google Scholar] [CrossRef]
- Morell, F.; Villar, A.; Montero, M.A.; Munoz, X.; Colby, T.V.; Pipvath, S.; Cruz, M.J.; Raghu, G. Chronic hypersensitivity pneumonitis in patients diagnosed with idiopathic pulmonary fibrosis: A prospective case-cohort study. Lancet Respir. Med. 2013, 1, 685–694. [Google Scholar] [CrossRef]
- Mohr, L.C. Hypersensitivity pneumonitis. Curr. Opin. Pulm. Med. 2004, 10, 401–411. [Google Scholar] [CrossRef]
- Fernandez Perez, E.R.; Swigris, J.J.; Forssen, A.V.; Tourin, O.; Solomon, J.J.; Huie, T.J.; Olson, A.L.; Brown, K.K. Identifying an inciting antigen is associated with improved survival in patients with chronic hypersensitivity pneumonitis. Chest 2013, 144, 1644–1651. [Google Scholar] [CrossRef] [Green Version]
- Terho, E.O.; Heinonen, O.P.; Lammi, S.; Laukkanen, V. Incidence of clinically confirmed farmer’s lung in Finland and its relation to meteorological factors. Eur. J. Respir. Dis. Suppl. 1987, 152, 47–56. [Google Scholar] [PubMed]
- Thomeer, M.J.; Costabe, U.; Rizzato, G.; Poletti, V.; Demedts, M. Comparison of registries of interstitial lung diseases in three European countries. Eur. Respir. J. Suppl. 2001, 32, 114s–118s. [Google Scholar]
- Okamoto, T.; Miyazaki, Y.; Ogura, T.; Chida, K.; Kohno, N.; Kohno, S.; Taniguchi, H.; Akagawa, S.; Mochizuki, Y.; Yamauchi, K.; et al. Nationwide epidemiological survey of chronic hypersensitivity pneumonitis in Japan. Respir. Investig. 2013, 51, 191–199. [Google Scholar] [CrossRef] [PubMed]
- Rittig, A.H.; Hilberg, O.; Ibsen, R.; Lokke, A. Incidence, comorbidity and survival rate of hypersensitivity pneumonitis: A national population-based study. ERJ Open Res. 2019, 5, 00259-2018. [Google Scholar] [CrossRef] [PubMed]
- Solaymani-Dodaran, M.; West, J.; Smith, C.; Hubbard, R. Extrinsic allergic alveolitis: Incidence and mortality in the general population. QJM 2007, 100, 233–237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hyldgaard, C.; Hilberg, O.; Muller, A.; Bendstrup, E. A cohort study of interstitial lung diseases in central Denmark. Respir. Med. 2014, 108, 793–799. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernandez Perez, E.R.; Kong, A.M.; Raimundo, K.; Koelsch, T.L.; Kulkarni, R.; Cole, A.L. Epidemiology of Hypersensitivity Pneumonitis among an Insured Population in the United States: A Claims-based Cohort Analysis. Ann. Am. Thorac. Soc. 2018, 15, 460–469. [Google Scholar] [CrossRef]
- King, T.E., Jr. Hypersensitivity Pneumonitis (Extrinsic Allergic Alveolitis): Epidemiology, Causes, and Pathogenesis; Hollingsworth, H., Ed.; UpToDate: Waltham, MA, USA, 2019. [Google Scholar]
- Hilberg, O.; Hoffmann-Vold, A.M.; Smith, V.; Bouros, D.; Kilpeläinen, M.; Guiot, J.; Morais, A.; Clemente, S.; Daniil, Z.; Papakosta, D.; et al. Epidemiology of interstitial lung diseases and their progressive-fibrosing behaviour in six European countries. ERJ Open Res. 2022, 8, 00597-2021. [Google Scholar] [CrossRef]
- Singh, S.; Collins, B.F.; Sharma, B.B.; Joshi, J.M.; Talwar, D.; Katiyar, S.; Singh, N.; Ho, L.; Samaria, J.K.; Bhattacharya, P.; et al. Interstitial Lung Disease in India. Results of a Prospective Registry. Am. J. Respir. Crit. Care Med. 2017, 195, 801–813. [Google Scholar] [CrossRef]
- Costabel, U.; Miyazaki, Y.; Pardo, A.; Koschel, D.; Bonella, F.; Spagnolo, P.; Guzman, J.; Ryerson, C.J.; Selman, M. Hypersensitivity pneumonitis. Nat. Rev. Dis. Primers 2020, 6, 65. [Google Scholar] [CrossRef]
- Nasser, M.; Larrieu, S.; Boussel, L.; Si-Mohamed, S.; Bazin, F.; Marque, S.; Massol, J.; Thivolet-Bejui, F.; Chalabreysse, L.; Maucort-Boulch, D.; et al. Estimates of epidemiology, mortality and disease burden associated with progressive fibrosing interstitial lung disease in France (the PROGRESS study). Respir. Res. 2021, 22, 162. [Google Scholar] [CrossRef] [PubMed]
- Quaresma, M.; Coleman, M.P.; Rachet, B. 40-year trends in an index of survival for all cancers combined and survival adjusted for age and sex for each cancer in England and Wales, 1971–2011: A population-based study. Lancet 2015, 385, 1206–1218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernandez Perez, E.R.; Sprunger, D.B.; Ratanawatkul, P.; Maier, L.A.; Huie, T.J.; Swigris, J.J.; Solomon, J.J.; Mohning, M.P.; Keith, R.C.; Brown, K.K. Increasing Hypersensitivity Pneumonitis-related Mortality in the United States from 1988 to 2016. Am. J. Respir. Crit. Care Med. 2019, 199, 1284–1287. [Google Scholar] [CrossRef] [PubMed]
- Biomarkers Definitions Working, G. Biomarkers and surrogate endpoints: Preferred definitions and conceptual framework. Clin. Pharmacol. Ther. 2001, 69, 89–95. [Google Scholar]
- Califf, R.M. Biomarker definitions and their applications. Exp. Biol. Med. 2018, 243, 213–221. [Google Scholar] [CrossRef]
- Kern, S.E. Why your new cancer biomarker may never work: Recurrent patterns and remarkable diversity in biomarker failures. Cancer Res. 2012, 72, 6097–6101. [Google Scholar] [CrossRef] [Green Version]
- Alfaro, T.M.; Robalo Cordeiro, C. Comorbidity in idiopathic pulmonary fibrosis—What can biomarkers tell us? Ther. Adv. Respir. Dis. 2020, 14, 1753466620910092. [Google Scholar] [CrossRef] [Green Version]
- Crespo, A.; Alfaro, T.; Somogyi, V.; Kreuter, M. Updates in using a molecular classifier to identify usual interstitial pneumonia in conventional transbronchial lung biopsy samples. Breathe 2020, 16, 200067. [Google Scholar] [CrossRef]
- Ohnishi, H.; Yokoyama, A.; Kondo, K.; Hamada, H.; Abe, M.; Nishimura, K.; Hiwada, K.; Kohno, N. Comparative study of KL-6, surfactant protein-A, surfactant protein-D, and monocyte chemoattractant protein-1 as serum markers for interstitial lung diseases. Am. J. Respir. Crit. Care Med. 2002, 165, 378–381. [Google Scholar] [CrossRef]
- Ohtsuki, Y.; Nakanishi, N.; Fujita, J.; Yoshinouchi, T.; Kobayashi, M.; Ueda, N.; Lee, G.H.; Furihata, M. Immunohistochemical distribution of SP-D, compared with that of SP-A and KL-6, in interstitial pneumonias. Med. Mol. Morphol. 2007, 40, 163–167. [Google Scholar] [CrossRef]
- Prasse, A.; Muller-Quernheim, J. Non-invasive biomarkers in pulmonary fibrosis. Respirology 2009, 14, 788–795. [Google Scholar] [CrossRef] [PubMed]
- Tzouvelekis, A.; Kouliatsis, G.; Anevlavis, S.; Bouros, D. Serum biomarkers in interstitial lung diseases. Respir. Res. 2005, 6, 78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inoue, Y.; Kaner, R.J.; Guiot, J.; Maher, T.M.; Tomassetti, S.; Moiseev, S.; Kuwana, M.; Brown, K.K. Diagnostic and Prognostic Biomarkers for Chronic Fibrosing Interstitial Lung Diseases With a Progressive Phenotype. Chest 2020, 158, 646–659. [Google Scholar] [CrossRef] [PubMed]
- Campo, I.; Zorzetto, M.; Bonella, F. Facts and promises on lung biomarkers in interstitial lung diseases. Expert. Rev. Respir. Med. 2015, 9, 437–457. [Google Scholar] [CrossRef] [PubMed]
- Guiot, J.; Moermans, C.; Henket, M.; Corhay, J.L.; Louis, R. Blood Biomarkers in Idiopathic Pulmonary Fibrosis. Lung 2017, 195, 273–280. [Google Scholar] [CrossRef] [Green Version]
- Bonella, F.; Costabel, U. Biomarkers in connective tissue disease-associated interstitial lung disease. Semin. Respir. Crit. Care Med. 2014, 35, 181–200. [Google Scholar] [CrossRef]
- Hwang, S.J.; Kim, H.S.; Chung, D.H. Fas/Fas ligand-mediated apoptosis promotes hypersensitivity pneumonitis in mice by enhancing maturation of dendritic cells. Am. J. Respir. Crit. Care Med. 2010, 181, 1250–1261. [Google Scholar] [CrossRef]
- Takemura, T.; Akashi, T.; Kamiya, H.; Ikushima, S.; Ando, T.; Oritsu, M.; Sawahata, M.; Ogura, T. Pathological differentiation of chronic hypersensitivity pneumonitis from idiopathic pulmonary fibrosis/usual interstitial pneumonia. Histopathology 2012, 61, 1026–1035. [Google Scholar] [CrossRef]
- Espoladore, L.M.; Gregorio, B.B.; Lima, M.S.; de Pereira, C.A.; Soares, M.R.; Coletta, E.N. Cytological analysis of bronchoalveolar lavage in patients with interstitial lung diseases and the relation of cytological analysis to fibrosis in high-resolution computed tomography. Anal. Quant. Cytopathol. Histpathol. 2014, 36, 206–212. [Google Scholar]
- Adams, T.N.; Newton, C.A.; Batra, K.; Abu-Hijleh, M.; Barbera, T.; Torrealba, J.; Glazer, C.S. Utility of Bronchoalveolar Lavage and Transbronchial Biopsy in Patients with Hypersensitivity Pneumonitis. Lung 2018, 196, 617–622. [Google Scholar] [CrossRef]
- Gaxiola, M.; Buendia-Roldan, I.; Mejia, M.; Carrillo, G.; Estrada, A.; Navarro, M.C.; Rojas-Serrano, J.; Selman, M. Morphologic diversity of chronic pigeon breeder’s disease: Clinical features and survival. Respir. Med. 2011, 105, 608–614. [Google Scholar] [CrossRef] [Green Version]
- Hill, M.; Petnak, T.; Moua, T. Bronchoalveolar lavage lymphocytosis in hypersensitivity pneumonitis: A retrospective cohort analysis with elimination of incorporation bias. BMC Pulm. Med. 2022, 22, 49. [Google Scholar] [CrossRef]
- Salvaggio, J.E.; Karr, R.M. Hypersensitivity pneumonitis; state of the art. Chest 1979, 75, 270–274. [Google Scholar] [CrossRef]
- Schuyler, M.; Cormier, Y. The diagnosis of hypersensitivity pneumonitis. Chest 1997, 111, 534–536. [Google Scholar] [CrossRef] [PubMed]
- American Thoracic, S.; European Respiratory, S. American Thoracic Society/European Respiratory Society International Multidisciplinary Consensus Classification of the Idiopathic Interstitial Pneumonias. This joint statement of the American Thoracic Society (ATS), and the European Respiratory Society (ERS) was adopted by the ATS board of directors, June 2001 and by the ERS Executive Committee, June 2001. Am. J. Respir. Crit. Care Med. 2002, 165, 277–304. [Google Scholar]
- Bonella, F.; Costabel, U. The perpetual enigma of bronchoalveolar lavage fluid lymphocytosis in chronic hypersensitivity pneumonitis: Is it of diagnostic value? Eur. Respir. J. 2020, 56, 2001534. [Google Scholar] [CrossRef]
- Tzilas, V.; Tzouvelekis, A.; Bouros, E.; Karampitsakos, T.; Ntasiou, M.; Katsaras, M.; Costabel, U.; Wells, A.; Bouros, D. Diagnostic value of BAL lymphocytosis in patients with indeterminate for usual interstitial pneumonia imaging pattern. Eur. Respir. J. 2019, 54, 1901144. [Google Scholar] [CrossRef] [PubMed]
- Patolia, S.; Tamae Kakazu, M.; Chami, H.A.; Chua, A.; Diaz-Mendoza, J.; Duggal, A.; Jenkins, A.R.; Knight, S.L.; Raghu, G.; Wilson, K.C. Bronchoalveolar Lavage Lymphocytes in the Diagnosis of Hypersensitivity Pneumonitis among Patients with Interstitial Lung Disease. Ann. Am. Thorac. Soc. 2020, 17, 1455–1467. [Google Scholar] [CrossRef]
- Adderley, N.; Humphreys, C.J.; Barnes, H.; Ley, B.; Premji, Z.A.; Johannson, K.A. Bronchoalveolar lavage fluid lymphocytosis in chronic hypersensitivity pneumonitis: A systematic review and meta-analysis. Eur. Respir. J. 2020, 56, 2000206. [Google Scholar] [CrossRef]
- Yoshizawa, Y.; Ohtani, Y.; Hayakawa, H.; Sato, A.; Suga, M.; Ando, M. Chronic hypersensitivity pneumonitis in Japan: A nationwide epidemiologic survey. J. Allergy Clin. Immunol. 1999, 103, 315–320. [Google Scholar] [CrossRef]
- Caillaud, D.M.; Vergnon, J.M.; Madroszyk, A.; Melloni, B.M.; Murris, M.; Dalphin, J.C.; French Group of Environmental Immunoallergic Bronchopulmonary Diseases. Bronchoalveolar lavage in hypersensitivity pneumonitis: A series of 139 patients. Inflamm. Allergy Drug Targets 2012, 11, 15–19. [Google Scholar] [CrossRef] [PubMed]
- Santos, V.; Martins, N.; Sousa, C.; Jacob, M.; Padrao, E.; Melo, N.; Mota, P.C.; Bastos, H.N.; Guimaraes, S.; Moura, C.S.; et al. Hypersensitivity pneumonitis: Main features characterization in a Portuguese cohort. Pulmonology 2020, 26, 130–137. [Google Scholar] [CrossRef] [PubMed]
- Morell, F.; Roger, A.; Reyes, L.; Cruz, M.J.; Murio, C.; Munoz, X. Bird fancier’s lung: A series of 86 patients. Medicine 2008, 87, 110–130. [Google Scholar] [CrossRef] [PubMed]
- Ratjen, F.; Costabel, U.; Griese, M.; Paul, K. Bronchoalveolar lavage fluid findings in children with hypersensitivity pneumonitis. Eur. Respir. J. 2003, 21, 144–148. [Google Scholar] [CrossRef] [Green Version]
- Ando, M.; Konishi, K.; Yoneda, R.; Tamura, M. Difference in the phenotypes of bronchoalveolar lavage lymphocytes in patients with summer-type hypersensitivity pneumonitis, farmer’s lung, ventilation pneumonitis, and bird fancier’s lung: Report of a nationwide epidemiologic study in Japan. J. Allergy Clin. Immunol. 1991, 87, 1002–1009. [Google Scholar] [CrossRef]
- Cordeiro, C.R.; Jones, J.C.; Alfaro, T.; Ferreira, A.J. Bronchoalveolar lavage in occupational lung diseases. Semin. Respir. Crit. Care Med. 2007, 28, 504–513. [Google Scholar] [CrossRef] [Green Version]
- Alfaro, T.; Robalo Cordeiro, C. Bronchoalveolar Lavage. In Idiopathic Pulmonary Fibrosis: ERS Monograph; Costabel, U., Crestani, B., Wells, A.U., Eds.; European Respiratory Society: Sheffield, UK, 2016; Volume 71, pp. 74–81. [Google Scholar]
- Murayama, J.; Yoshizawa, Y.; Ohtsuka, M.; Hasegawa, S. Lung fibrosis in hypersensitivity pneumonitis. Association with CD4+ but not CD8+ cell dominant alveolitis and insidious onset. Chest 1993, 104, 38–43. [Google Scholar] [CrossRef]
- Drent, M.; Jacobs, J.A.; Cobben, N.A.; Costabel, U.; Wouters, E.F.; Mulder, P.G. Computer program supporting the diagnostic accuracy of cellular BALF analysis: A new release. Respir. Med. 2001, 95, 781–786. [Google Scholar] [CrossRef] [Green Version]
- Crouser, E.D.; Maier, L.A.; Wilson, K.C.; Bonham, C.A.; Morgenthau, A.S.; Patterson, K.C.; Abston, E.; Bernstein, R.C.; Blankstein, R.; Chen, E.S.; et al. Diagnosis and Detection of Sarcoidosis. An Official American Thoracic Society Clinical Practice Guideline. Am. J. Respir. Crit. Care Med. 2020, 201, e26–e51. [Google Scholar] [CrossRef]
- Meyer, K.C.; Raghu, G.; Baughman, R.P.; Brown, K.K.; Costabel, U.; du Bois, R.M.; Drent, M.; Haslam, P.L.; Kim, D.S.; Nagai, S.; et al. An official American Thoracic Society clinical practice guideline: The clinical utility of bronchoalveolar lavage cellular analysis in interstitial lung disease. Am. J. Respir. Crit. Care Med. 2012, 185, 1004–1014. [Google Scholar] [CrossRef]
- Ye, Q.; Nakamura, S.; Sarria, R.; Costabel, U.; Guzman, J. Interleukin 12, interleukin 18, and tumor necrosis factor alpha release by alveolar macrophages: Acute and chronic hypersensitivity pneumonitis. Ann. Allergy Asthma Immunol. 2009, 102, 149–154. [Google Scholar] [CrossRef] [PubMed]
- Gudmundsson, G.; Hunninghake, G.W. Interferon-gamma is necessary for the expression of hypersensitivity pneumonitis. J. Clin. Investig. 1997, 99, 2386–2390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nance, S.; Cross, R.; Yi, A.K.; Fitzpatrick, E.A. IFN-gamma production by innate immune cells is sufficient for development of hypersensitivity pneumonitis. Eur. J. Immunol. 2005, 35, 1928–1938. [Google Scholar] [CrossRef] [PubMed]
- Raymond, T.; Schaller, M.; Hogaboam, C.M.; Lukacs, N.W.; Rochford, R.; Kunkel, S.L. Toll-like receptors, Notch ligands, and cytokines drive the chronicity of lung inflammation. Proc. Am. Thorac. Soc. 2007, 4, 635–641. [Google Scholar] [CrossRef] [Green Version]
- Fong, D.J.; Hogaboam, C.M.; Matsuno, Y.; Akira, S.; Uematsu, S.; Joshi, A.D. Toll-like receptor 6 drives interleukin-17A expression during experimental hypersensitivity pneumonitis. Immunology 2010, 130, 125–136. [Google Scholar] [CrossRef]
- Joshi, A.D.; Fong, D.J.; Oak, S.R.; Trujillo, G.; Flaherty, K.R.; Martinez, F.J.; Hogaboam, C.M. Interleukin-17-mediated immunopathogenesis in experimental hypersensitivity pneumonitis. Am. J. Respir. Crit. Care Med. 2009, 179, 705–716. [Google Scholar] [CrossRef]
- Simonian, P.L.; Roark, C.L.; Wehrmann, F.; Lanham, A.K.; Diaz del Valle, F.; Born, W.K.; O’Brien, R.L.; Fontenot, A.P. Th17-polarized immune response in a murine model of hypersensitivity pneumonitis and lung fibrosis. J. Immunol. 2009, 182, 657–665. [Google Scholar] [CrossRef] [Green Version]
- Matěj, R.; Smětáková, M.; Vašáková, M.; Nováková, J.; Sterclová, M.; Kukal, J.; Olejár, T. PAR-2, IL-4R, TGF-β and TNF-α in bronchoalveolar lavage distinguishes extrinsic allergic alveolitis from sarcoidosis. Exp. Ther. Med. 2014, 8, 533–538. [Google Scholar] [CrossRef] [Green Version]
- Sterclova, M.; Matej, R.; Mandakova, P.; Skibova, J.; Vasakova, M. Role of interleukin 4 and its receptor in clinical presentation of chronic extrinsic allergic alveolitis: A pilot study. Multidiscip. Respir. Med. 2013, 8, 35. [Google Scholar] [CrossRef] [Green Version]
- Simonian, P.L.; Roark, C.L.; Wehrmann, F.; Lanham, A.M.; Born, W.K.; O’Brien, R.L.; Fontenot, A.P. IL-17A-expressing T cells are essential for bacterial clearance in a murine model of hypersensitivity pneumonitis. J. Immunol. 2009, 182, 6540–6549. [Google Scholar] [CrossRef] [Green Version]
- Zakaria, M.W.; El-Korashy, R.I.; Selim, S.; Badawy, I.; Amum, K.J. Serum level of transforming growth factor-beta1 in major idiopathic interstitial pneumonia. Egypt. J. Bronchol. 2020, 14, 22. [Google Scholar] [CrossRef]
- Willems, S.; Verleden, S.E.; Vanaudenaerde, B.M.; Wynants, M.; Dooms, C.; Yserbyt, J.; Somers, J.; Verbeken, E.K.; Verleden, G.M.; Wuyts, W.A. Multiplex protein profiling of bronchoalveolar lavage in idiopathic pulmonary fibrosis and hypersensitivity pneumonitis. Ann. Thorac. Med. 2013, 8, 38–45. [Google Scholar] [PubMed]
- Bruzova, M.; Pavlova, M.; Matej, R.; Sterclova, M.; Vasakova, M. Interstitial Score and Concentrations of IL-4Rα, PAR-2, and MMP-7 in Bronchoalveolar Lavage Fluid Could Be Useful Markers for Distinguishing Idiopathic Interstitial Pneumonias. Diagnostics 2021, 11, 693. [Google Scholar] [CrossRef] [PubMed]
- Martina, S.; Martina, V.; Monika, M.; Jan, P.; Libor, K.; Ilja, S. Angiostatic versus angiogenic chemokines in IPF and EAA. Respir. Med. 2009, 103, 1651–1656. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sugiyama, Y.; Kasahara, T.; Mukaida, N.; Matsushima, K.; Kitamura, S. Chemokines in bronchoalveolar lavage fluid in summer-type hypersensitivity pneumonitis. Eur. Respir. J. 1995, 8, 1084–1090. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inoue, Y.; Ishizuka, M.; Furusawa, H.; Honda, T.; Kawahara, T.; Tateishi, T.; Miyazaki, Y. Acute inflammatory and immunologic responses against antigen in chronic bird-related hypersensitivity pneumonitis. Allergol. Int. 2019, 68, 321–328. [Google Scholar] [CrossRef]
- Miyazaki, Y.; Unoura, K.; Tateishi, T.; Akashi, T.; Takemura, T.; Tomita, M.; Inase, N.; Yoshizawa, Y. Higher serum CCL17 may be a promising predictor of acute exacerbations in chronic hypersensitivity pneumonitis. Respir. Res. 2013, 14, 57. [Google Scholar] [CrossRef] [Green Version]
- Watanabe, M.; Horimasu, Y.; Iwamoto, H.; Yamaguchi, K.; Sakamoto, S.; Masuda, T.; Nakashima, T.; Miyamoto, S.; Ohshimo, S.; Fujitaka, K.; et al. C-C Motif Chemokine Ligand 15 May Be a Useful Biomarker for Predicting the Prognosis of Patients with Chronic Hypersensitivity Pneumonitis. Respiration 2019, 98, 212–220. [Google Scholar] [CrossRef] [Green Version]
- Inoue, T.; Fujishima, S.; Ikeda, E.; Yoshie, O.; Tsukamoto, N.; Aiso, S.; Aikawa, N.; Kubo, A.; Matsushima, K.; Yamaguchi, K. CCL22 and CCL17 in rat radiation pneumonitis and in human idiopathic pulmonary fibrosis. Eur. Respir. J. 2004, 24, 49–56. [Google Scholar] [CrossRef]
- Nukui, Y.; Yamana, T.; Masuo, M.; Tateishi, T.; Kishino, M.; Tateishi, U.; Tomita, M.; Hasegawa, T.; Aritsu, T.; Miyazaki, Y. Serum CXCL9 and CCL17 as biomarkers of declining pulmonary function in chronic bird-related hypersensitivity pneumonitis. PLoS ONE 2019, 14, e0220462. [Google Scholar] [CrossRef] [Green Version]
- Pardo, A.; Smith, K.M.; Abrams, J.; Coffman, R.; Bustos, M.; McClanahan, T.K.; Grein, J.; Murphy, E.E.; Zlotnik, A.; Selman, M. CCL18/DC-CK-1/PARC up-regulation in hypersensitivity pneumonitis. J. Leukoc. Biol. 2001, 70, 610–616. [Google Scholar] [CrossRef]
- Cai, M.; Bonella, F.; He, X.; Sixt, S.U.; Sarria, R.; Guzman, J.; Costabel, U. CCL18 in serum, BAL fluid and alveolar macrophage culture supernatant in interstitial lung diseases. Respir. Med. 2013, 107, 1444–1452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iyonaga, K.; Takeya, M.; Saita, N.; Sakamoto, O.; Yoshimura, T.; Ando, M.; Takahashi, K. Monocyte chemoattractant protein-1 in idiopathic pulmonary fibrosis and other interstitial lung diseases. Hum. Pathol. 1994, 25, 455–463. [Google Scholar] [CrossRef] [PubMed]
- García de Alba, C.; Buendia-Roldán, I.; Salgado, A.; Becerril, C.; Ramírez, R.; González, Y.; Checa, M.; Navarro, C.; Ruiz, V.; Pardo, A.; et al. Fibrocytes contribute to inflammation and fibrosis in chronic hypersensitivity pneumonitis through paracrine effects. Am. J. Respir. Crit. Care Med. 2015, 191, 427–436. [Google Scholar] [CrossRef]
- Suga, M.; Iyonaga, K.; Ichiyasu, H.; Saita, N.; Yamasaki, H.; Ando, M. Clinical significance of MCP-1 levels in BALF and serum in patients with interstitial lung diseases. Eur. Respir. J. 1999, 14, 376–382. [Google Scholar] [CrossRef] [PubMed]
- d’Alessandro, M.; Bergantini, L.; Cameli, P.; Lanzarone, N.; Perillo, F.; Perrone, A.; Bargagli, E. BAL and serum multiplex lipid profiling in idiopathic pulmonary fibrosis and fibrotic hypersensitivity pneumonitis. Life Sci. 2020, 256, 117995. [Google Scholar] [CrossRef]
- Panina-Bordignon, P.; Papi, A.; Mariani, M.; Di Lucia, P.; Casoni, G.; Bellettato, C.; Buonsanti, C.; Miotto, D.; Mapp, C.; Villa, A.; et al. The C-C chemokine receptors CCR4 and CCR8 identify airway T cells of allergen-challenged atopic asthmatics. J. Clin. Investig. 2001, 107, 1357–1364. [Google Scholar] [CrossRef] [Green Version]
- Miyazaki, E.; Nureki, S.; Fukami, T.; Shigenaga, T.; Ando, M.; Ito, K.; Ando, H.; Sugisaki, K.; Kumamoto, T.; Tsuda, T. Elevated levels of thymus- and activation-regulated chemokine in bronchoalveolar lavage fluid from patients with eosinophilic pneumonia. Am. J. Respir. Crit. Care Med. 2002, 165, 1125–1131. [Google Scholar] [CrossRef]
- Shanley, T.P.; Peters, J.L.; Jones, M.L.; Chensue, S.W.; Kunkel, S.L.; Ward, P.A. Regulatory effects of endogenous interleukin-1 receptor antagonist protein in immunoglobulin G immune complex-induced lung injury. J. Clin. Investig. 1996, 97, 963–970. [Google Scholar] [CrossRef] [Green Version]
- Costabel, U.; Bonella, F.; Guzman, J. Chronic hypersensitivity pneumonitis. Clin. Chest Med. 2012, 33, 151–163. [Google Scholar] [CrossRef]
- Jenkins, A.R.; Chua, A.; Chami, H.; Diaz-Mendoza, J.; Duggal, A.; Knight, S.; Patolia, S.; Tamae-Kakazu, M.; Raghu, G.; Wilson, K.C. Questionnaires or Serum Immunoglobulin G Testing in the Diagnosis of Hypersensitivity Pneumonitis among Patients with Interstitial Lung Disease. Ann. Am. Thorac. Soc. 2021, 18, 130–147. [Google Scholar] [CrossRef] [PubMed]
- Morell, F. Idiopathic pulmonary fibrosis: Importance of accurate diagnosis and treatment. Arch. Bronconeumol. 2013, 49, 319–320. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.G.; Da Silva, C.A.; Dela Cruz, C.S.; Ahangari, F.; Ma, B.; Kang, M.J.; He, C.H.; Takyar, S.; Elias, J.A. Role of chitin and chitinase/chitinase-like proteins in inflammation, tissue remodeling, and injury. Annu. Rev. Physiol. 2011, 73, 479–501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, C.G.; Dela Cruz, C.S.; Herzog, E.; Rosenberg, S.M.; Ahangari, F.; Elias, J.A. YKL-40, a chitinase-like protein at the intersection of inflammation and remodeling. Am. J. Respir. Crit. Care Med. 2012, 185, 692–694. [Google Scholar] [CrossRef]
- Liu, C.; Li, Q.; Zhou, X.; Kolosov, V.P.; Perelman, J.M. The chitinase-like protein YKL-40 increases mucin5AC production in human bronchial epithelial cells. Exp. Cell Res. 2013, 319, 2866–2873. [Google Scholar] [CrossRef]
- Johansen, J.S. Studies on serum YKL-40 as a biomarker in diseases with inflammation, tissue remodelling, fibroses and cancer. Dan. Med. Bull. 2006, 53, 172–209. [Google Scholar]
- Johansen, J.S.; Milman, N.; Hansen, M.; Garbarsch, C.; Price, P.A.; Graudal, N. Increased serum YKL-40 in patients with pulmonary sarcoidosis--a potential marker of disease activity? Respir. Med. 2005, 99, 396–402. [Google Scholar] [CrossRef] [Green Version]
- Furuhashi, K.; Suda, T.; Nakamura, Y.; Inui, N.; Hashimoto, D.; Miwa, S.; Hayakawa, H.; Kusagaya, H.; Nakano, Y.; Nakamura, H.; et al. Increased expression of YKL-40, a chitinase-like protein, in serum and lung of patients with idiopathic pulmonary fibrosis. Respir. Med. 2010, 104, 1204–1210. [Google Scholar] [CrossRef] [Green Version]
- Korthagen, N.M.; van Moorsel, C.H.; Barlo, N.P.; Ruven, H.J.; Kruit, A.; Heron, M.; van den Bosch, J.M.; Grutters, J.C. Serum and BALF YKL-40 levels are predictors of survival in idiopathic pulmonary fibrosis. Respir. Med. 2011, 105, 106–113. [Google Scholar] [CrossRef] [Green Version]
- Tong, X.; Ma, Y.; Liu, T.; Li, Z.; Liu, S.; Wu, G.; Fan, H. Can YKL-40 be used as a biomarker for interstitial lung disease?: A systematic review and meta-analysis. Medicine 2021, 100, e25631. [Google Scholar] [CrossRef]
- Long, X.; He, X.; Ohshimo, S.; Griese, M.; Sarria, R.; Guzman, J.; Costabel, U.; Bonella, F. Serum YKL-40 as predictor of outcome in hypersensitivity pneumonitis. Eur. Respir. J. 2017, 49, 1501924. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanchez-Diez, S.; Munoz, X.; Ojanguren, I.; Romero-Mesones, C.; Espejo, D.; Villar, A.; Gomez-Olles, S.; Cruz, M.J. YKL-40 and KL-6 Levels in Serum and Sputum of Patients Diagnosed With Hypersensitivity Pneumonitis. J. Allergy Clin. Immunol. Pract. 2022, 10, 2414–2423. [Google Scholar] [CrossRef] [PubMed]
- Mandrekar, J.N. Receiver operating characteristic curve in diagnostic test assessment. J. Thorac. Oncol. 2010, 5, 1315–1316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vietri, L.; Fui, A.; Bergantini, L.; d’Alessandro, M.; Cameli, P.; Sestini, P.; Rottoli, P.; Bargagli, E. Serum amyloid A: A potential biomarker of lung disorders. Respir. Investig. 2020, 58, 21–27. [Google Scholar] [CrossRef]
- Chen, E.S.; Song, Z.; Willett, M.H.; Heine, S.; Yung, R.C.; Liu, M.C.; Groshong, S.D.; Zhang, Y.; Tuder, R.M.; Moller, D.R. Serum amyloid A regulates granulomatous inflammation in sarcoidosis through Toll-like receptor-2. Am. J. Respir. Crit. Care Med. 2010, 181, 360–373. [Google Scholar] [CrossRef]
- Rubinstein, I.; Knecht, A.; de Beer, F.C.; Baum, G.L.; Pras, M. Serum amyloid-A protein concentrations in sarcoidosis. Isr. J. Med. Sci. 1989, 25, 461–462. [Google Scholar]
- Salazar, A.; Mana, J.; Fiol, C.; Hurtado, I.; Argimon, J.M.; Pujol, R.; Pinto, X. Influence of serum amyloid A on the decrease of high density lipoprotein-cholesterol in active sarcoidosis. Atherosclerosis 2000, 152, 497–502. [Google Scholar] [CrossRef]
- Miyoshi, S.; Hamada, H.; Kadowaki, T.; Hamaguchi, N.; Ito, R.; Irifune, K.; Higaki, J. Comparative evaluation of serum markers in pulmonary sarcoidosis. Chest 2010, 137, 1391–1397. [Google Scholar] [CrossRef] [Green Version]
- Bargagli, E.; Magi, B.; Olivieri, C.; Bianchi, N.; Landi, C.; Rottoli, P. Analysis of serum amyloid A in sarcoidosis patients. Respir. Med. 2011, 105, 775–780. [Google Scholar] [CrossRef] [Green Version]
- Beijer, E.; Roodenburg-Benschop, C.; Schimmelpennink, M.C.; Grutters, J.C.; Meek, B.; Veltkamp, M. Elevated Serum Amyloid a Levels Are not Specific for Sarcoidosis but Associate with a Fibrotic Pulmonary Phenotype. Cells 2021, 10, 585. [Google Scholar] [CrossRef]
- Lakota, K.; Carns, M.; Podlusky, S.; Mrak-Poljsak, K.; Hinchcliff, M.; Lee, J.; Tomsic, M.; Sodin-Semrl, S.; Varga, J. Serum amyloid A is a marker for pulmonary involvement in systemic sclerosis. PLoS ONE 2015, 10, e0110820. [Google Scholar] [CrossRef] [PubMed]
- Migita, K.; Kawabe, Y.; Tominaga, M.; Origuchi, T.; Aoyagi, T.; Eguchi, K. Serum amyloid A protein induces production of matrix metalloproteinases by human synovial fibroblasts. Lab. Investig. 1998, 78, 535–539. [Google Scholar] [PubMed]
- Vietri, L.; d’Alessandro, M.; Bergantini, L.; Carleo, A.; Cameli, P.; Mazzei, M.A.; Sestini, P.; Bargagli, E. Specificity of serum amyloid A as a biomarker of idiopathic pulmonary fibrosis. Intern. Med. J. 2020, 50, 1571–1574. [Google Scholar] [CrossRef] [PubMed]
- Vietri, L.; Bennett, D.; Cameli, P.; Bergantini, L.; Cillis, G.; Sestini, P.; Bargagli, E.; Rottoli, P. Serum amyloid A in patients with idiopathic pulmonary fibrosis. Respir. Investig. 2019, 57, 430–434. [Google Scholar] [CrossRef] [PubMed]
- Bergantini, L.; d’Alessandro, M.; Vietri, L.; Rana, G.D.; Cameli, P.; Acerra, S.; Sestini, P.; Bargagli, E. Utility of serological biomarker’ panels for diagnostic accuracy of interstitial lung diseases. Immunol. Res. 2020, 68, 414–421. [Google Scholar] [CrossRef] [PubMed]
- Hermans, C.; Bernard, A. Lung epithelium-specific proteins: Characteristics and potential applications as markers. Am. J. Respir. Crit. Care Med. 1999, 159, 646–678. [Google Scholar] [CrossRef]
- Jinta, T.; Miyazaki, Y.; Kishi, M.; Akashi, T.; Takemura, T.; Inase, N.; Yoshizawa, Y. The pathogenesis of chronic hypersensitivity pneumonitis in common with idiopathic pulmonary fibrosis: Expression of apoptotic markers. Am. J. Clin. Pathol. 2010, 134, 613–620. [Google Scholar] [CrossRef]
- Kohno, N.; Kyoizumi, S.; Awaya, Y.; Fukuhara, H.; Yamakido, M.; Akiyama, M. New serum indicator of interstitial pneumonitis activity. Sialylated carbohydrate antigen KL-6. Chest 1989, 96, 68–73. [Google Scholar]
- Kohno, N.; Awaya, Y.; Oyama, T.; Yamakido, M.; Akiyama, M.; Inoue, Y.; Yokoyama, A.; Hamada, H.; Fujioka, S.; Hiwada, K. KL-6, a mucin-like glycoprotein, in bronchoalveolar lavage fluid from patients with interstitial lung disease. Am. Rev. Respir. Dis. 1993, 148, 637–642. [Google Scholar] [CrossRef]
- Ishikawa, N.; Hattori, N.; Yokoyama, A.; Kohno, N. Utility of KL-6/MUC1 in the clinical management of interstitial lung diseases. Respir. Investig. 2012, 50, 3–13. [Google Scholar] [CrossRef] [Green Version]
- Hanzawa, S.; Tateishi, T.; Ishizuka, M.; Inoue, Y.; Honda, T.; Kawahara, T.; Tomita, M.; Miyazaki, Y. Changes in serum KL-6 levels during short-term strict antigen avoidance are associated with the prognosis of patients with fibrotic hypersensitivity pneumonitis caused by avian antigens. Respir. Investig. 2020, 58, 457–464. [Google Scholar] [CrossRef]
- Fathi, M.; Barbasso Helmers, S.; Lundberg, I.E. KL-6: A serological biomarker for interstitial lung disease in patients with polymyositis and dermatomyositis. J. Intern. Med. 2012, 271, 589–597. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, J.; Kitamura, S. KL-6: A serum marker for interstitial pneumonia. Chest 1995, 108, 311–315. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, T.; Munakata, M.; Ohtsuka, Y.; Satoh-Kamachi, A.; Sato, R.; Homma, Y.; Kawakami, Y. Serum KL-6 concentrations in dairy farmers. Chest 2000, 118, 445–450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshikawa, S.; Tsushima, K.; Yasuo, M.; Fujimoto, K.; Kubo, K.; Kumagai, T.; Yamazaki, Y. Hypersensitivity pneumonitis caused by Penicillium citrinum, not Enoki spores. Am. J. Ind. Med. 2007, 50, 1010–1017. [Google Scholar] [CrossRef] [PubMed]
- d’Alessandro, M.; Bergantini, L.; Cameli, P.; Vietri, L.; Lanzarone, N.; Alonzi, V.; Pieroni, M.; Refini, M.R.; Sestini, P.; Bonella, F.; et al. Krebs von den Lungen-6 as a biomarker for disease severity assessment in interstitial lung disease: A comprehensive review. Biomark. Med. 2020, 14, 665–674. [Google Scholar] [CrossRef] [PubMed]
- Lanzarone, N.; Gentili, F.; Alonzi, V.; Bergantini, L.; d’Alessandro, M.; Rottoli, P.; Refini, R.M.; Pieroni, M.; Vietri, L.; Bianchi, F.; et al. Bronchoalveolar lavage and serum KL-6 concentrations in chronic hypersensitivity pneumonitis: Correlations with radiological and immunological features. Intern. Emerg. Med. 2020, 15, 1247–1254. [Google Scholar] [CrossRef]
- Ji, Y.; Bourke, S.J.; Spears, M.; Wain, L.V.; Boyd, G.; Lynch, P.P.; Cunningham, M.; Boyd, K.; Donnelly, I.; Kohno, N.; et al. Krebs von den Lungen-6 (KL-6) is a pathophysiological biomarker of early-stage acute hypersensitivity pneumonitis among pigeon fanciers. Clin. Exp. Allergy 2020, 50, 1391–1399. [Google Scholar] [CrossRef]
- Okamoto, T.; Fujii, M.; Furusawa, H.; Tsuchiya, K.; Miyazaki, Y.; Inase, N. The usefulness of KL-6 and SP-D for the diagnosis and management of chronic hypersensitivity pneumonitis. Respir. Med. 2015, 109, 1576–1581. [Google Scholar] [CrossRef]
- Onishi, Y.; Kawamura, T.; Higashino, T.; Kagami, R.; Hirata, N.; Miyake, K. Clinical features of chronic summer-type hypersensitivity pneumonitis and proposition of diagnostic criteria. Respir. Investig. 2020, 58, 59–67. [Google Scholar] [CrossRef]
- Sakamoto, K.; Taniguchi, H.; Kondoh, Y.; Johkoh, T.; Sumikawa, H.; Kimura, T.; Nishiyama, O.; Kato, K.; Kataoka, K.; Ono, K.; et al. Serum KL-6 in fibrotic NSIP: Correlations with physiologic and radiologic parameters. Respir. Med. 2010, 104, 127–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiba, S.; Ohta, H.; Abe, K.; Hisata, S.; Ohkouchi, S.; Hoshikawa, Y.; Kondo, T.; Ebina, M. The Diagnostic Value of the Interstitial Biomarkers KL-6 and SP-D for the Degree of Fibrosis in Combined Pulmonary Fibrosis and Emphysema. Pulm. Med. 2012, 2012, 492960. [Google Scholar] [CrossRef] [Green Version]
- Moll, S.A.; Wiertz, I.A.; Vorselaars, A.D.M.; Ruven, H.J.T.; van Moorsel, C.H.M.; Grutters, J.C. Change in Serum Biomarker CA 15-3 as an Early Predictor of Response to Treatment and Survival in Hypersensitivity Pneumonitis. Lung 2020, 198, 385–393. [Google Scholar] [CrossRef] [PubMed]
- Kruit, A.; Gerritsen, W.B.; Pot, N.; Grutters, J.C.; van den Bosch, J.M.; Ruven, H.J. CA 15-3 as an alternative marker for KL-6 in fibrotic lung diseases. Sarcoidosis Vasc. Diffuse Lung Dis. 2010, 27, 138–146. [Google Scholar] [PubMed]
- Gomes, P.S.; Soares, M.R.; Marchenta, M.; Meirelles, G.S.P.; Ferreira, R.G.; Botelho, A.B.; Martins, R.B.; Pereira, C.A.C. Carbohydrate antigen 15-3 as a marker of disease severity in patients with chronic hypersensitivity pneumonitis. J. Bras. Pneumol. 2021, 47, e20200589. [Google Scholar] [CrossRef]
- Ricci, A.; Mariotta, S.; Bronzetti, E.; Bruno, P.; Vismara, L.; De Dominicis, C.; Lagana, B.; Paone, G.; Mura, M.; Rogliani, P.; et al. Serum CA 15-3 is increased in pulmonary fibrosis. Sarcoidosis Vasc. Diffuse Lung Dis. 2009, 26, 54–63. [Google Scholar]
- Okada, M.; Suzuki, K.; Nakanishi, T.; Nakashima, M. Serum levels of KL-6 are positively correlated with those of CA15-3 in patients with interstitial pneumonia associated with collagen diseases. Respirology 2006, 11, 509–510. [Google Scholar] [CrossRef]
- Sorensen, G.L. Surfactant Protein D in Respiratory and Non-Respiratory Diseases. Front. Med. 2018, 5, 18. [Google Scholar] [CrossRef] [Green Version]
- Wright, J.R. Immunoregulatory functions of surfactant proteins. Nat. Rev. Immunol. 2005, 5, 58–68. [Google Scholar] [CrossRef]
- Kishore, U.; Greenhough, T.J.; Waters, P.; Shrive, A.K.; Ghai, R.; Kamran, M.F.; Bernal, A.L.; Reid, K.B.; Madan, T.; Chakraborty, T. Surfactant proteins SP-A and SP-D: Structure, function and receptors. Mol. Immunol. 2006, 43, 1293–1315. [Google Scholar] [CrossRef]
- Tanaka, H.; Sugawara, H.; Saikai, T.; Tsunematsu, K.; Takahashi, H.; Abe, S. Mushroom worker’s lung caused by spores of Hypsizigus marmoreus (Bunashimeji): Elevated serum surfactant protein D levels. Chest 2000, 118, 1506–1509. [Google Scholar] [CrossRef] [PubMed]
- Janssen, R.; Grutters, J.C.; Sato, H.; van Velzen-Blad, H.; Zanen, P.; Kohno, N.; Welsh, K.I.; du Bois, R.M.; van den Bosch, J.M. Analysis of KL-6 and SP-D as disease markers in bird fancier’s lung. Sarcoidosis Vasc. Diffuse Lung Dis. 2005, 22, 51–57. [Google Scholar]
- Guzman, J.; Wang, Y.M.; Kalaycioglu, O.; Schoenfeld, B.; Hamm, H.; Bartsch, W.; Costabel, U. Increased surfactant protein A content in human alveolar macrophages in hypersensitivity pneumonitis. Acta Cytol. 1992, 36, 668–673. [Google Scholar] [PubMed]
- Hamm, H.; Lührs, J.; Guzman y Rotaeche, J.; Costabel, U.; Fabel, H.; Bartsch, W. Elevated surfactant protein A in bronchoalveolar lavage fluids from sarcoidosis and hypersensitivity pneumonitis patients. Chest 1994, 106, 1766–1770. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cormier, Y.; Israël-Assayag, E.; Desmeules, M.; Lesur, O. Effect of contact avoidance or treatment with oral prednisolone on bronchoalveolar lavage surfactant protein A levels in subjects with farmer’s lung. Thorax 1996, 51, 1210–1215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phelps, D.S.; Umstead, T.M.; Mejia, M.; Carrillo, G.; Pardo, A.; Selman, M. Increased surfactant protein-A levels in patients with newly diagnosed idiopathic pulmonary fibrosis. Chest 2004, 125, 617–625. [Google Scholar] [CrossRef]
- Lee, Y.C.; Zhang, Z.; Mukherjee, A.B. Mice lacking uteroglobin are highly susceptible to developing pulmonary fibrosis. FEBS Lett. 2006, 580, 4515–4520. [Google Scholar] [CrossRef] [Green Version]
- Laucho-Contreras, M.E.; Polverino, F.; Gupta, K.; Taylor, K.L.; Kelly, E.; Pinto-Plata, V.; Divo, M.; Ashfaq, N.; Petersen, H.; Stripp, B.; et al. Protective role for club cell secretory protein-16 (CC16) in the development of COPD. Eur. Respir. J. 2015, 45, 1544–1556. [Google Scholar] [CrossRef] [Green Version]
- Miller, T.L.; Shashikant, B.N.; Pilon, A.L.; Pierce, R.A.; Shaffer, T.H.; Wolfson, M.R. Effects of recombinant Clara cell secretory protein (rhCC10) on inflammatory-related matrix metalloproteinase activity in a preterm lamb model of neonatal respiratory distress. Pediatr. Crit. Care Med. 2007, 8, 40–46. [Google Scholar] [CrossRef]
- Yao, X.L.; Ikezono, T.; Cowan, M.; Logun, C.; Angus, C.W.; Shelhamer, J.H. Interferon-gamma stimulates human Clara cell secretory protein production by human airway epithelial cells. Am. J. Physiol. 1998, 274, L864–L869. [Google Scholar]
- Magdaleno, S.M.; Wang, G.; Jackson, K.J.; Ray, M.K.; Welty, S.; Costa, R.H.; DeMayo, F.J. Interferon-gamma regulation of Clara cell gene expression: In vivo and in vitro. Am. J. Physiol. 1997, 272, L1142–L1151. [Google Scholar] [CrossRef] [PubMed]
- Yoon, J.M.; Lee, K.H.; Lee, S.M.; Lim, J.J.; Yang, S.C.; Yoo, C.G.; Lee, C.T.; Han, S.K.; Shim, Y.S.; Kim, Y.W. The immune modulation of Clara cell-10 in human peripheral monocytes and dendritic cells. Int. J. Mol. Med. 2010, 26, 415–423. [Google Scholar] [PubMed]
- Almuntashiri, S.; Zhu, Y.; Han, Y.; Wang, X.; Somanath, P.R.; Zhang, D. Club Cell Secreted Protein CC16: Potential Applications in Prognosis and Therapy for Pulmonary Diseases. J. Clin. Med. 2020, 9, 4039. [Google Scholar] [CrossRef]
- Doubkova, M.; Karpisek, M.; Mazoch, J.; Skrickova, J.; Doubek, M. Prognostic significance of surfactant protein A, surfactant protein D, Clara cell protein 16, S100 protein, trefoil factor 3, and prostatic secretory protein 94 in idiopathic pulmonary fibrosis, sarcoidosis, and chronic pulmonary obstructive disease. Sarcoidosis Vasc. Diffuse Lung Dis. 2016, 33, 224–234. [Google Scholar]
- Tsoumakidou, M.; Bouloukaki, I.; Thimaki, K.; Tzanakis, N.; Siafakas, N.M. Innate immunity proteins in chronic obstructive pulmonary disease and idiopathic pulmonary fibrosis. Exp. Lung Res. 2010, 36, 373–380. [Google Scholar] [CrossRef]
- Buendia-Roldan, I.; Ruiz, V.; Sierra, P.; Montes, E.; Ramirez, R.; Vega, A.; Salgado, A.; Vargas, M.H.; Mejia, M.; Pardo, A.; et al. Increased Expression of CC16 in Patients with Idiopathic Pulmonary Fibrosis. PLoS ONE 2016, 11, e0168552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnes, H.; Olin, A.C.; Toren, K.; McSharry, C.; Donnelly, I.; Larstad, M.; Iribarren, C.; Quinlan, P.; Blanc, P.D. Occupation versus environmental factors in hypersensitivity pneumonitis: Population attributable fraction. ERJ Open Res. 2020, 6, 00374–2020. [Google Scholar] [CrossRef]
- Milutinovic, P.S.; Englert, J.M.; Crum, L.T.; Mason, N.S.; Ramsgaard, L.; Enghild, J.J.; Sparvero, L.J.; Lotze, M.T.; Oury, T.D. Clearance kinetics and matrix binding partners of the receptor for advanced glycation end products. PLoS ONE 2014, 9, e88259. [Google Scholar] [CrossRef] [Green Version]
- Oczypok, E.A.; Perkins, T.N.; Oury, T.D. All the “RAGE” in lung disease: The receptor for advanced glycation endproducts (RAGE) is a major mediator of pulmonary inflammatory responses. Paediatr. Respir. Rev. 2017, 23, 40–49. [Google Scholar] [CrossRef]
- Chavakis, T.; Bierhaus, A.; Al-Fakhri, N.; Schneider, D.; Witte, S.; Linn, T.; Nagashima, M.; Morser, J.; Arnold, B.; Preissner, K.T.; et al. The pattern recognition receptor (RAGE) is a counterreceptor for leukocyte integrins: A novel pathway for inflammatory cell recruitment. J. Exp. Med. 2003, 198, 1507–1515. [Google Scholar] [CrossRef] [Green Version]
- Schmidt, A.M.; Hori, O.; Chen, J.X.; Li, J.F.; Crandall, J.; Zhang, J.; Cao, R.; Yan, S.D.; Brett, J.; Stern, D. Advanced glycation endproducts interacting with their endothelial receptor induce expression of vascular cell adhesion molecule-1 (VCAM-1) in cultured human endothelial cells and in mice. A potential mechanism for the accelerated vasculopathy of diabetes. J. Clin. Investig. 1995, 96, 1395–1403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boulanger, E.; Wautier, M.P.; Wautier, J.L.; Boval, B.; Panis, Y.; Wernert, N.; Danze, P.M.; Dequiedt, P. AGEs bind to mesothelial cells via RAGE and stimulate VCAM-1 expression. Kidney Int. 2002, 61, 148–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shirasawa, M.; Fujiwara, N.; Hirabayashi, S.; Ohno, H.; Iida, J.; Makita, K.; Hata, Y. Receptor for advanced glycation end-products is a marker of type I lung alveolar cells. Genes Cells 2004, 9, 165–174. [Google Scholar] [CrossRef] [PubMed]
- Demling, N.; Ehrhardt, C.; Kasper, M.; Laue, M.; Knels, L.; Rieber, E.P. Promotion of cell adherence and spreading: A novel function of RAGE, the highly selective differentiation marker of human alveolar epithelial type I cells. Cell Tissue Res. 2006, 323, 475–488. [Google Scholar] [CrossRef] [PubMed]
- Buckley, S.T.; Ehrhardt, C. The receptor for advanced glycation end products (RAGE) and the lung. J. Biomed. Biotechnol. 2010, 2010, 917108. [Google Scholar] [CrossRef] [Green Version]
- Ott, C.; Jacobs, K.; Haucke, E.; Navarrete Santos, A.; Grune, T.; Simm, A. Role of advanced glycation end products in cellular signaling. Redox Biol. 2014, 2, 411–429. [Google Scholar] [CrossRef] [Green Version]
- Avery, N.C.; Bailey, A.J. The effects of the Maillard reaction on the physical properties and cell interactions of collagen. Pathol. Biol. 2006, 54, 387–395. [Google Scholar] [CrossRef]
- Gautieri, A.; Passini, F.S.; Silván, U.; Guizar-Sicairos, M.; Carimati, G.; Volpi, P.; Moretti, M.; Schoenhuber, H.; Redaelli, A.; Berli, M.; et al. Advanced glycation end-products: Mechanics of aged collagen from molecule to tissue. Matrix Biol. 2017, 59, 95–108. [Google Scholar] [CrossRef] [Green Version]
- Machahua, C.; Montes-Worboys, A.; Llatjos, R.; Escobar, I.; Dorca, J.; Molina-Molina, M.; Vicens-Zygmunt, V. Increased AGE-RAGE ratio in idiopathic pulmonary fibrosis. Respir. Res. 2016, 17, 144. [Google Scholar] [CrossRef] [Green Version]
- Machahua, C.; Montes-Worboys, A.; Planas-Cerezales, L.; Buendia-Flores, R.; Molina-Molina, M.; Vicens-Zygmunt, V. Serum AGE/RAGEs as potential biomarker in idiopathic pulmonary fibrosis. Respir. Res. 2018, 19, 215. [Google Scholar] [CrossRef]
- Yamaguchi, K.; Iwamoto, H.; Horimasu, Y.; Ohshimo, S.; Fujitaka, K.; Hamada, H.; Mazur, W.; Kohno, N.; Hattori, N. AGER gene polymorphisms and soluble receptor for advanced glycation end product in patients with idiopathic pulmonary fibrosis. Respirology 2017, 22, 965–971. [Google Scholar] [CrossRef] [Green Version]
- Pardo, A.; Cabrera, S.; Maldonado, M.; Selman, M. Role of matrix metalloproteinases in the pathogenesis of idiopathic pulmonary fibrosis. Respir. Res. 2016, 17, 23. [Google Scholar] [CrossRef] [Green Version]
- Craig, V.J.; Zhang, L.; Hagood, J.S.; Owen, C.A. Matrix metalloproteinases as therapeutic targets for idiopathic pulmonary fibrosis. Am. J. Respir. Cell Mol. Biol. 2015, 53, 585–600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosas, I.O.; Richards, T.J.; Konishi, K.; Zhang, Y.; Gibson, K.; Lokshin, A.E.; Lindell, K.O.; Cisneros, J.; Macdonald, S.D.; Pardo, A.; et al. MMP1 and MMP7 as potential peripheral blood biomarkers in idiopathic pulmonary fibrosis. PLoS Med. 2008, 5, e93. [Google Scholar] [CrossRef] [Green Version]
- Morais, A.; Beltrão, M.; Sokhatska, O.; Costa, D.; Melo, N.; Mota, P.; Marques, A.; Delgado, L. Serum metalloproteinases 1 and 7 in the diagnosis of idiopathic pulmonary fibrosis and other interstitial pneumonias. Respir. Med. 2015, 109, 1063–1068. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maldonado, M.; Buendía-Roldán, I.; Vicens-Zygmunt, V.; Planas, L.; Molina-Molina, M.; Selman, M.; Pardo, A. Identification of MMP28 as a biomarker for the differential diagnosis of idiopathic pulmonary fibrosis. PLoS ONE 2018, 13, e0203779. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Dong, J.B.; Wu, M.P. Human ApoA-I overexpression diminishes LPS-induced systemic inflammation and multiple organ damage in mice. Eur. J. Pharmacol. 2008, 590, 417–422. [Google Scholar] [CrossRef] [PubMed]
- Yan, Y.J.; Li, Y.; Lou, B.; Wu, M.P. Beneficial effects of ApoA-I on LPS-induced acute lung injury and endotoxemia in mice. Life Sci. 2006, 79, 210–215. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.H.; Lee, Y.H.; Kim, K.H.; Lee, S.H.; Cha, J.Y.; Shin, E.K.; Jung, S.; Jang, A.S.; Park, S.W.; Uh, S.T.; et al. Role of lung apolipoprotein A-I in idiopathic pulmonary fibrosis: Antiinflammatory and antifibrotic effect on experimental lung injury and fibrosis. Am. J. Respir. Crit. Care Med. 2010, 182, 633–642. [Google Scholar] [CrossRef]
- Masui, Y.; Asano, Y.; Takahashi, T.; Shibata, S.; Akamata, K.; Aozasa, N.; Noda, S.; Taniguchi, T.; Ichimura, Y.; Toyama, T.; et al. Clinical significance of monitoring serum adiponectin levels during intravenous pulse cyclophosphamide therapy in interstitial lung disease associated with systemic sclerosis. Mod. Rheumatol. 2013, 23, 323–329. [Google Scholar] [CrossRef]
- Enomoto, N.; Oyama, Y.; Yasui, H.; Karayama, M.; Hozumi, H.; Suzuki, Y.; Kono, M.; Furuhashi, K.; Fujisawa, T.; Inui, N.; et al. Analysis of serum adiponectin and leptin in patients with acute exacerbation of idiopathic pulmonary fibrosis. Sci. Rep. 2019, 9, 10484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haley, S.; Shah, D.; Romero, F.; Summer, R. Scleroderma-related lung disease: Are adipokines involved pathogenically? Curr. Rheumatol. Rep. 2013, 15, 381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, Z.; Mo, L.; Feng, X.; Huang, M.; Li, L. Using bioinformatics approach identifies key genes and pathways in idiopathic pulmonary fibrosis. Medicine 2020, 99, e22099. [Google Scholar] [CrossRef] [PubMed]
- Ruwanpura, S.M.; Thomas, B.J.; Bardin, P.G. Pirfenidone: Molecular Mechanisms and Potential Clinical Applications in Lung Disease. Am. J. Respir. Cell Mol. Biol. 2020, 62, 413–422. [Google Scholar] [CrossRef]
- Wollin, L.; Wex, E.; Pautsch, A.; Schnapp, G.; Hostettler, K.E.; Stowasser, S.; Kolb, M. Mode of action of nintedanib in the treatment of idiopathic pulmonary fibrosis. Eur. Respir. J. 2015, 45, 1434–1445. [Google Scholar] [CrossRef] [Green Version]
- Herrmann, F.E.; Hesslinger, C.; Wollin, L.; Nickolaus, P. BI 1015550 is a PDE4B Inhibitor and a Clinical Drug Candidate for the Oral Treatment of Idiopathic Pulmonary Fibrosis. Front. Pharmacol. 2022, 13, 838449. [Google Scholar] [CrossRef]
- Decato, B.E.; Leeming, D.J.; Sand, J.M.B.; Fischer, A.; Du, S.; Palmer, S.M.; Karsdal, M.; Luo, Y.; Minnich, A. LPA 1 antagonist BMS-986020 changes collagen dynamics and exerts antifibrotic effects in vitro and in patients with idiopathic pulmonary fibrosis. Respir. Res. 2022, 23, 61. [Google Scholar] [CrossRef]
- Brown, K.K.; Inoue, Y.; Flaherty, K.R.; Martinez, F.J.; Cottin, V.; Bonella, F.; Cerri, S.; Danoff, S.K.; Jouneau, S.; Goeldner, R.G.; et al. Predictors of mortality in subjects with progressive fibrosing interstitial lung diseases. Respirology 2022, 27, 294–300. [Google Scholar] [CrossRef]
- Chen, X.H.; Huang, S.; Kerr, D. Biomarkers in clinical medicine. IARC Sci. Publ. 2011, 163, 303–322. [Google Scholar]
- Sellarés, J.; Molina-Molina, M. Serum Biomarkers in Diffuse Interstitial Lung Diseases. Arch. Bronconeumol. (Engl. Ed.) 2020, 56, 349–350. [Google Scholar] [CrossRef]


| Name | Class | Mechanism of Action | Target Disease(s) | Biomarker Repercussion | Study Phase |
|---|---|---|---|---|---|
| BI 1015550 | Anti-inflammatory, antifibrotic | Preferential PDE 4B inhibitor | IPF PPF-ILD | Inhibition of TNF-α and IL-2 release [199] | Phase III Clinical Trials (recruiting) NCT05321069 NCT05321082 |
| BMS-986278 | Antifibrotic | LPAR-1 antagonist | IPF PPF-ILD | Potential reduction in serum ECM-neoepitope biomarkers [200] | Phase II Clinical Trial (active) NCT04308681 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pereira, J.O.; Fernandes, V.; Alfaro, T.M.; Freitas, S.; Cordeiro, C.R. Diagnosis of Fibrotic Hypersensitivity Pneumonitis: Is There a Role for Biomarkers? Life 2023, 13, 565. https://doi.org/10.3390/life13020565
Pereira JO, Fernandes V, Alfaro TM, Freitas S, Cordeiro CR. Diagnosis of Fibrotic Hypersensitivity Pneumonitis: Is There a Role for Biomarkers? Life. 2023; 13(2):565. https://doi.org/10.3390/life13020565
Chicago/Turabian StylePereira, João O., Vânia Fernandes, Tiago M. Alfaro, Sara Freitas, and Carlos Robalo Cordeiro. 2023. "Diagnosis of Fibrotic Hypersensitivity Pneumonitis: Is There a Role for Biomarkers?" Life 13, no. 2: 565. https://doi.org/10.3390/life13020565
APA StylePereira, J. O., Fernandes, V., Alfaro, T. M., Freitas, S., & Cordeiro, C. R. (2023). Diagnosis of Fibrotic Hypersensitivity Pneumonitis: Is There a Role for Biomarkers? Life, 13(2), 565. https://doi.org/10.3390/life13020565