
Association between Inflammatory Bowel Disease and Subsequent Development of Restless Legs Syndrome and Parkinson’s Disease: A Retrospective Cohort Study of 35,988 Primary Care Patients in Germany

 ,
,  , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Database
2.2. Study Population
2.3. Study Outcomes and Statistical Analyses
3. Results
3.1. Basic Characteristics of the Study Sample
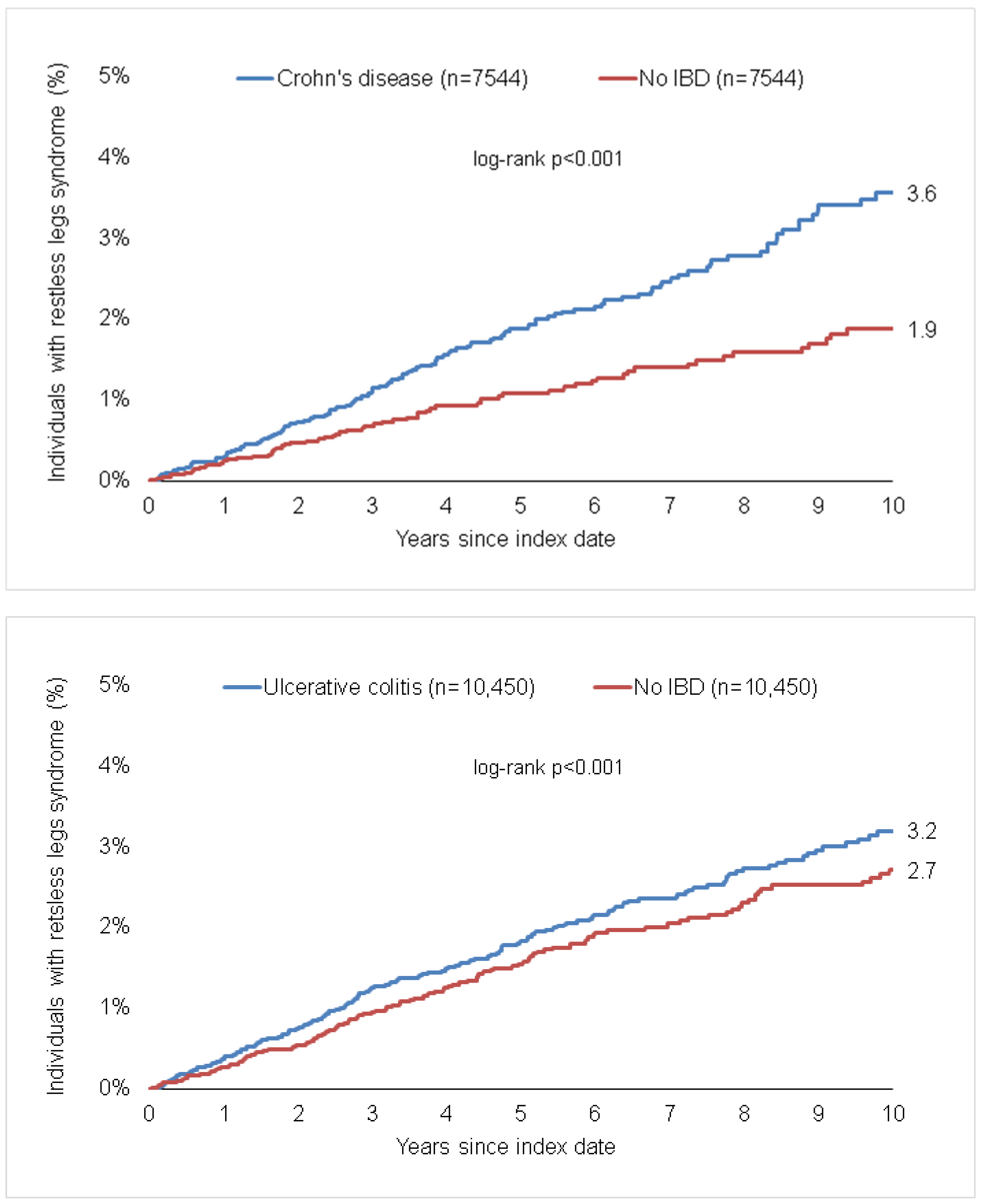
3.2. Association of IBD and A Subsequent Diagnosis of Restless Legs Syndrome
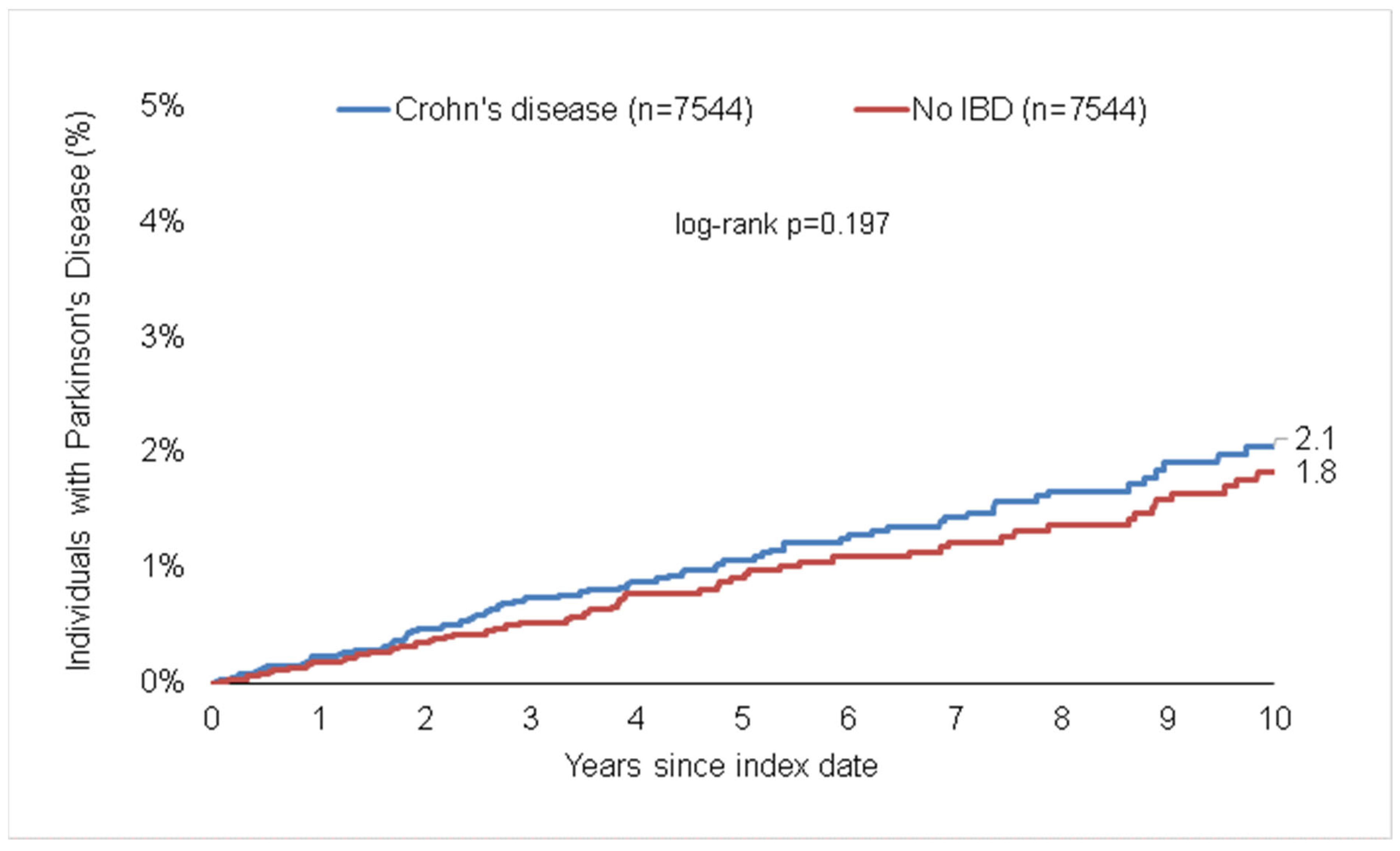
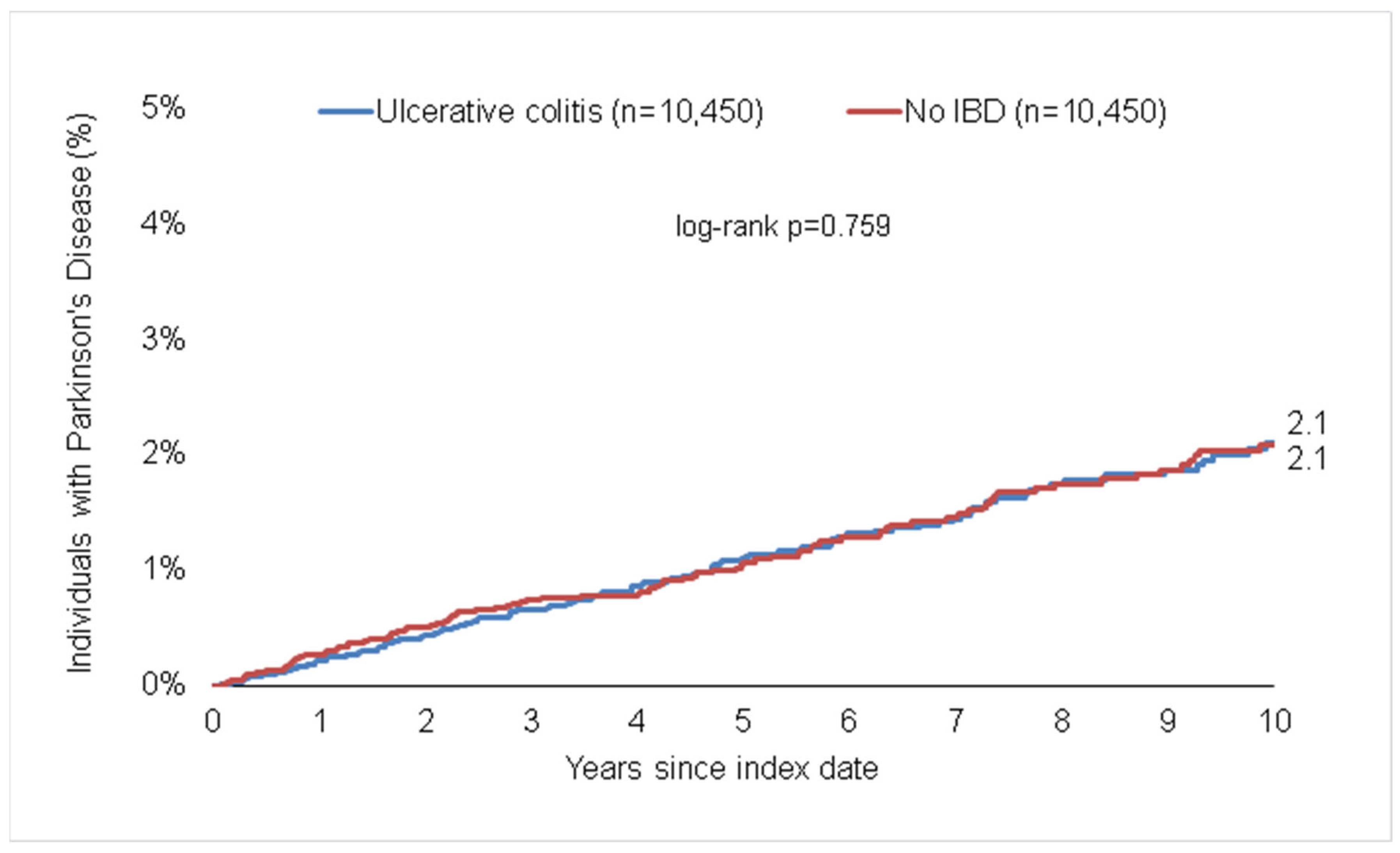
3.3. Association of IBD and A Subsequent Diagnosis of Parkinson’s Disease
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Argollo, M.; Gilardi, D.; Peyrin-Biroulet, C.; Chabot, J.F.; Peyrin-Biroulet, L.; Danese, S. Comorbidities in Inflammatory Bowel Disease: A Call for Action. Lancet Gastroenterol. Hepatol. 2019, 4, 643–654. [Google Scholar] [CrossRef] [PubMed]
- Masanetz, R.K.; Winkler, J.; Winner, B.; Günther, C.; Süß, P. The Gut–Immune–Brain Axis: An Important Route for Neuropsychiatric Morbidity in Inflammatory Bowel Disease. Int. J. Mol. Sci. 2022, 23, 11111. [Google Scholar] [CrossRef]
- El-Hakim, Y.; Bake, S.; Mani, K.K.; Sohrabji, F. Impact of Intestinal Disorders on Central and Peripheral Nervous System Diseases. Neurobiol. Dis. 2022, 165, 105627. [Google Scholar] [CrossRef] [PubMed]
- Weimers, P.; Halfvarson, J.; Sachs, M.C.; Saunders-Pullman, R.; Ludvigsson, J.F.; Peter, I.; Burisch, J.; Olén, O. Inflammatory Bowel Disease and Parkinson’s Disease: A Nationwide Swedish Cohort Study. Inflamm. Bowel Dis. 2019, 25, 111–123. [Google Scholar] [CrossRef] [PubMed]
- Szandruk-Bender, M.; Wiatrak, B.; Szeląg, A. The Risk of Developing Alzheimer’s Disease and Parkinson’s Disease in Patients with Inflammatory Bowel Disease: A Meta-Analysis. J. Clin. Med. 2022, 11, 3704. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Kim, J.; Chun, J.; Han, K.; Soh, H.; Kang, E.A.; Lee, H.J.; Im, J.P.; Kim, J.S. Patients with Inflammatory Bowel Disease Are at an Increased Risk of Parkinson’s Disease: A South Korean Nationwide Population-Based Study. J. Clin. Med. 2019, 8, 1191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weinstock, L.B.; Bosworth, B.P.; Scherl, E.J.; Li, E.; Iroku, U.; Munsell, M.A.; Mullen, G.E.; Walters, A.S. Crohn’s Disease Is Associated with Restless Legs Syndrome. Inflamm. Bowel Dis. 2010, 16, 275–279. [Google Scholar] [CrossRef] [Green Version]
- Becker, J.; Berger, F.; Schindlbeck, K.A.; Poddubnyy, D.; Koch, P.M.; Preiß, J.C.; Siegmund, B.; Marzinzik, F.; Maul, J. Restless Legs Syndrome Is a Relevant Comorbidity in Patients with Inflammatory Bowel Disease. Int. J. Colorectal Dis. 2018, 33, 955–962. [Google Scholar] [CrossRef]
- Mosli, M.H.; Bukhari, L.M.; Khoja, A.A.; Ashour, N.A.; Aljahdali, H.R.; Khoja, O.A.; Alhejaili, F.F.; Saadah, O.I. Inflammatory Bowel Disease and Restless Leg Syndrome. Neurosciences 2020, 25, 301–307. [Google Scholar] [CrossRef]
- Freuer, D.; Meisinger, C. Association between Inflammatory Bowel Disease and Parkinson’s Disease: A Mendelian Randomization Study. NPJ Parkinsons Dis. 2022, 8, 55. [Google Scholar] [CrossRef]
- Abetz, L.; Allen, R.; Follet, A.; Washburn, T.; Early, C.; Kirsch, J.; Knight, H. Evaluating the Quality of Life of Patients with Restless Legs Syndrome. Clin. Ther. 2004, 26, 925–935. [Google Scholar] [CrossRef] [PubMed]
- Zhao, N.; Yang, Y.; Zhang, L.; Zhang, Q.; Balbuena, L.; Ungvari, G.S.; Zang, Y.F.; Xiang, Y.T. Quality of Life in Parkinson’s Disease: A Systematic Review and Meta-Analysis of Comparative Studies. CNS Neurosci. Ther. 2021, 27, 270–279. [Google Scholar] [CrossRef] [PubMed]
- Schrag, A.; Jahanshahi, M.; Quinn, N. What Contributes to Quality of Life in Patients with Parkinson’s Disease? J. Neurol. Neurosurg. Psychiatry 2000, 69, 308–312. [Google Scholar] [CrossRef] [Green Version]
- Svetel, M.V.; Jovic, J.S.; Pekmezovic, T.D.; Kostic, V.S. Quality of Life in Patients with Primary Restless Leg Syndrome: Community-Based Study. Neurol. Sci. 2015, 36, 1345–1351. [Google Scholar] [CrossRef]
- Rathmann, W.; Bongaerts, B.; Carius, H.J.; Kruppert, S.; Kostev, K. Basic Characteristics and Representativeness of the German Disease Analyzer Database. Int. J. Clin. Pharmacol. Ther. 2018, 56, 459–466. [Google Scholar] [CrossRef] [PubMed]
- Peeraully, T.; Tan, E.K. Linking Restless Legs Syndrome with Parkinson’s Disease: Clinical, Imaging and Genetic Evidence. Transl. Neurodegener. 2012, 1, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Connor, J.R.; Wang, X.S.; Allen, R.P.; Beard, J.L.; Wiesinger, J.A.; Felt, B.T.; Earley, C.J. Altered Dopaminergic Profile in the Putamen and Substantia Nigra in Restless Leg Syndrome. Brain 2009, 132, 2403–2412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jellinger, K. Post Mortem Studies in Parkinson’s Disease—Is It Possible to Detect Brain Areas for Specific Symptoms. In Proceedings of the Journal of Neural Transmission, Supplement; Springer: Vienna, Austria, 1999; pp. 1–29. [Google Scholar]
- Tan, E.K. Restless Legs Syndrome and Parkinson’s Disease: Is There an Etiologic Link? J. Neurol. 2006, 253, vii33–vii37. [Google Scholar] [CrossRef]
- Krishnan, P.R.; Bhatia, M.; Behari, M. Restless Legs Syndrome in Parkinson’s Disease: A Case-Controlled Study. Mov. Disord. 2003, 18, 181–185. [Google Scholar] [CrossRef]
- Nomura, T.; Inoue, Y.; Miyake, M.; Yasui, K.; Nakashima, K. Prevalence and Clinical Characteristics of Restless Legs Syndrome in Japanese Patients with Parkinson’s Disease. Mov. Disord. 2006, 21, 380–384. [Google Scholar] [CrossRef]
- Calzetti, S.; Negrotti, A.; Bonavina, G.; Angelini, M.; Marchesi, E. Absence of Co-Morbidity of Parkinson Disease and Restless Legs Syndrome: A Case-Control Study in Patients Attending a Movement Disorders Clinic. Neurol. Sci. 2009, 30, 119–122. [Google Scholar] [CrossRef]
- Verbaan, D.; van Rooden, S.M.; van Hilten, J.J.; Rijsman, R.M. Prevalence and Clinical Profile of Restless Legs Syndrome in Parkinson’s Disease. Mov. Disord. 2010, 25, 2142–2147. [Google Scholar] [CrossRef] [PubMed]
- Oshiro, S.; Morioka, M.S.; Kikuchi, M. Dysregulation of Iron Metabolism in Alzheimer’s Disease, Parkinson’s Disease, and Amyotrophic Lateral Sclerosis. Adv. Pharmacol. Sci. 2011, 2011, 378278. [Google Scholar] [CrossRef] [PubMed]
- Earley, C.J.; Allen, R.P.; Beard, J.L.; Connor, J.R. Insight into the Pathophysiology of Restless Legs Syndrome. J. Neurosci. Res. 2000, 62, 623–628. [Google Scholar] [CrossRef] [PubMed]
- Dauvilliers, Y.; Winkelmann, J. Restless Legs Syndrome: Update on Pathogenesis. Curr. Opin. Pulm. Med. 2013, 19, 594–600. [Google Scholar] [CrossRef]
- Takahara, I.; Takeshima, F.; Ichikawa, T.; Matsuzaki, T.; Shibata, H.; Miuma, S.; Akazawa, Y.; Miyaaki, H.; Taura, N.; Nakao, K. Prevalence of Restless Legs Syndrome in Patients with Inflammatory Bowel Disease. Dig. Dis. Sci. 2017, 62, 761–767. [Google Scholar] [CrossRef]
- Vavricka, S.R.; Schoepfer, A.; Scharl, M.; Lakatos, P.L.; Navarini, A.; Rogler, G. Extraintestinal Manifestations of Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2015, 21, 1982–1992. [Google Scholar] [CrossRef] [Green Version]
- Cappellini, M.D.; Comin-Colet, J.; de Francisco, A.; Dignass, A.; Doehner, W.; Lam, C.S.; Macdougall, I.C.; Rogler, G.; Camaschella, C.; Kadir, R.; et al. Iron Deficiency across Chronic Inflammatory Conditions: International Expert Opinion on Definition, Diagnosis, and Management. Am. J. Hematol. 2017, 92, 1068–1078. [Google Scholar] [CrossRef] [Green Version]
- Fertrin, K.Y. Diagnosis and Management of Iron Deficiency in Chronic Inflammatory Conditions (CIC): Is Too Little Iron Making Your Patient Sick? Hematology 2020, 20, 478–486. [Google Scholar] [CrossRef]
- Atreya, R.; Neurath, M.F. Involvement of IL-6 in the Pathogenesis of Inflammatory Bowel Disease and Colon Cancer. Clin. Rev. Allergy Immunol. 2005, 28, 187–195. [Google Scholar] [CrossRef]
- Mudter, J.; Neurath, M.F. IL-6 Signaling in Inflammatory Bowel Disease: Pathophysiological Role and Clinical Relevance. Inflamm. Bowel Dis. 2007, 13, 1016–1023. [Google Scholar] [CrossRef] [PubMed]
- Kaitha, S.; Bashir, M.; Ali, T. Iron Deficiency Anemia in Inflammatory Bowel Disease. World J. Gastrointest. Pathophysiol. 2015, 6, 62. [Google Scholar] [CrossRef] [PubMed]
- Coad, J.; Pedley, K. Iron Deficiency and Iron Deficiency Anemia in Women. Scand. J. Clin. Lab. Investig. Inf. Healthc. 2014, 74, 82–89. [Google Scholar] [CrossRef] [PubMed]
- Coad, J.; Conlon, C. Iron Deficiency in Women: Assessment, Causes and Consequences. Curr. Opin. Clin. Nutr. Metab. Care 2011, 14, 625–634. [Google Scholar] [CrossRef]
- Lin, J.C.; Lin, C.S.; Hsu, C.W.; Lin, C.L.; Kao, C.H. Association between Parkinson’s Disease and Inflammatory Bowel Disease: A Nationwide Taiwanese Retrospective Cohort Study. Inflamm. Bowel Dis. 2016, 22, 1049–1055. [Google Scholar] [CrossRef] [Green Version]
- Peter, I.; Dubinsky, M.; Bressman, S.; Park, A.; Lu, C.; Chen, N.; Wang, A. Anti-Tumor Necrosis Factor Therapy and Incidence of Parkinson Disease among Patients with Inflammatory Bowel Disease. JAMA Neurol. 2018, 75, 939–946. [Google Scholar] [CrossRef]
- Camacho-Soto, A.; Gross, A.; Searles Nielsen, S.; Dey, N.; Racette, B.A. Inflammatory Bowel Disease and Risk of Parkinson’s Disease in Medicare Beneficiaries. Parkinsonism Relat. Disord. 2018, 50, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Braak, H.; del Tredici, K.; Rüb, U.; de Vos, R.A.I.; Jansen Steur, E.N.H.; Braak, E. Staging of Brain Pathology Related to Sporadic Parkinson’s Disease. Neurobiol. Aging 2003, 24, 197–211. [Google Scholar] [CrossRef]
- Hawkes, C.H.; del Tredici, K.; Braak, H. Parkinson’s Disease: A Dual-Hit Hypothesis. Neuropathol. Appl. Neurobiol. 2007, 33, 599–614. [Google Scholar] [CrossRef]
- Visanji, N.P.; Brooks, P.L.; Hazrati, L.N.; Lang, A.E. The Prion Hypothesis in Parkinson’s Disease: Braak to the Future. Acta Neuropathol. Commun. 2014, 1, 2. [Google Scholar] [CrossRef] [Green Version]
- Sánchez-Ferro, Á.; Rábano, A.; Catalán, M.J.; Rodríguez-Valcárcel, F.C.; Díez, S.F.; Herreros-Rodríguez, J.; García-Cobos, E.; Álvarez-Santullano, M.M.; López-Manzanares, L.; Mosqueira, A.J.; et al. In Vivo Gastric Detection of α-Synuclein Inclusions in Parkinson’s Disease. Mov. Disord. 2015, 30, 517–524. [Google Scholar] [CrossRef] [PubMed]
- Grathwohl, S.A.; Steiner, J.A.; Britschgi, M.; Brundin, P. Mind the Gut: Secretion of α-Synuclein by Enteric Neurons. J. Neurochem. 2013, 125, 487–490. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Kwon, S.H.; Kam, T.I.; Panicker, N.; Karuppagounder, S.S.; Lee, S.; Lee, J.H.; Kim, W.R.; Kook, M.; Foss, C.A.; et al. Transneuronal Propagation of Pathologic α-Synuclein from the Gut to the Brain Models Parkinson’s Disease. Neuron 2019, 103, 627–641.e7. [Google Scholar] [CrossRef] [PubMed]
- Uemura, N.; Yagi, H.; Uemura, M.T.; Hatanaka, Y.; Yamakado, H.; Takahashi, R. Inoculation of α-Synuclein Preformed Fibrils into the Mouse Gastrointestinal Tract Induces Lewy Body-like Aggregates in the Brainstem via the Vagus Nerve. Mol. Neurodegener. 2018, 13, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klann, E.M.; Dissanayake, U.; Gurrala, A.; Farrer, M.; Shukla, A.W.; Ramirez-Zamora, A.; Mai, V.; Vedam-Mai, V. The Gut-Brain Axis and Its Relation to Parkinson’s Disease: A Review. Front. Aging Neurosci. 2021, 13, 782082. [Google Scholar] [CrossRef]
- Lee, H.S.; Lobbestael, E.; Vermeire, S.; Sabino, J.; Cleynen, I. Inflammatory Bowel Disease and Parkinson’s Disease: Common Pathophysiological Links. Gut 2021, 70, 408–417. [Google Scholar] [CrossRef] [PubMed]
- Herrick, M.K.; Tansey, M.G. Is LRRK2 the Missing Link between Inflammatory Bowel Disease and Parkinson’s Disease? NPJ Parkinsons Dis. 2021, 7, 26. [Google Scholar] [CrossRef]
- Mogi, M.; Harada, M.; Kondo, T.; Riederer, P.; Inagaki, H.; Minami, M.; Nagatsu, T. Interleukin-1β, Interleukin-6, Epidermal Growth Factor and Transforming Growth Factor-α Are Elevated in the Brain from Parkinsonian Patients. Neurosci. Lett. 1994, 180, 147–150. [Google Scholar] [CrossRef]
- Mogi, M.; Harada, M.; Riederer, P.; Narabayashi, H.; Fujita, K.; Nagatsu, T. Tumor Necrosis Factor-α (TNF-α) Increases Both in the Brain and in the Cerebrospinal Fluid from Parkinsonian Patients. Neurosci. Lett. 1994, 165, 208–210. [Google Scholar] [CrossRef]
- Devos, D.; Lebouvier, T.; Lardeux, B.; Biraud, M.; Rouaud, T.; Pouclet, H.; Coron, E.; Bruley des Varannes, S.; Naveilhan, P.; Nguyen, J.M.; et al. Colonic Inflammation in Parkinson’s Disease. Neurobiol. Dis. 2013, 50, 42–48. [Google Scholar] [CrossRef]
- Brudek, T. Inflammatory Bowel Diseases and Parkinson’s Disease. J. Parkinsons Dis. 2019, 9, S331–S344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pinel Ríos, J.; Madrid Navarro, C.J.; Pérez Navarro, M.J.; Cabello Tapia, M.J.; Piña Vera, M.J.; Campos Arillo, V.; Gómez García, M.R.; Mínguez Castellanos, A.; Escamilla Sevilla, F. Association of Parkinson’s Disease and Treatment with Aminosalicylates in Inflammatory Bowel Disease: A Cross-Sectional Study in a Spain Drug Dispensation Records. BMJ Open 2019, 9, e025574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ford, A.C.; Achkar, J.P.; Khan, K.J.; Kane, S.V.; Talley, N.J.; Marshall, J.K.; Moayyedi, P. Efficacy of 5-Aminosalicylates in Ulcerative Colitis: Systematic Review and Meta-Analysis. Am. J. Gastroenterol. 2011, 106, 601–616. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Proportion among Individuals with IBD (%) n = 17,994 | Proportion among Individuals without IBD (%) n = 17,994 | p-Value |
|---|---|---|---|
| Age (Mean, SD) | 59.7 (12.8) | 59.7 (12.8) | 0.759 |
| Age 40–50 | 29.4 | 29.1 | 0.535 |
| Age 51–60 | 27.0 | 27.1 | |
| Age 61–70 | 20.0 | 20.6 | |
| Age 71–80 | 16.6 | 16.2 | |
| Age > 80 | 7.0 | 7.0 | |
| Women | 55.5 | 55.5 | 0.958 |
| Men | 44.5 | 44.5 | |
| Number of physician visits per year during the follow-up (Mean, SD) | 10.7 (9.0) | 10.6 (9.0) | 0.101 |
| Diabetes | 22.7 | 22.6 | 0.940 |
| Depression | 24.8 | 24.8 | 0.971 |
| Head injury | 4.6 | 4.6 | 0.980 |
| Patient Group | Crohn’s Disease | Ulcerative Colitis | ||
|---|---|---|---|---|
| HR (95% CI) | p–value | HR (95% CI) | p–value | |
| Parkinson’s Disease | ||||
| Total | 1.23 (0.90–1.69) | 0.198 | 0.96 (0.75–1.23) | 0.759 |
| Women | 0.99 (0.63–1.54) | 0.946 | 0.90 (0.63–1.28) | 0.561 |
| Men | 1.55 (0.98–2.45) | 0.064 | 1.02 (0.72–1.43) | 0.927 |
| Restless Legs Syndrome | ||||
| Total | 1.60 (1.23–2.09) | <0.001 | 1.26 (1.02–1.55) | 0.031 |
| Women | 1.58 (1.14–2.20) | 0.006 | 1.18 (0.91–1.51) | 0.210 |
| Men | 1.64 (1.04–2.61) | 0.035 | 1.49 (1.02–2.18) | 0.041 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Loosen, S.H.; Yaqubi, K.; May, P.; Konrad, M.; Gollop, C.; Luedde, T.; Kostev, K.; Roderburg, C. Association between Inflammatory Bowel Disease and Subsequent Development of Restless Legs Syndrome and Parkinson’s Disease: A Retrospective Cohort Study of 35,988 Primary Care Patients in Germany. Life 2023, 13, 897. https://doi.org/10.3390/life13040897
Loosen SH, Yaqubi K, May P, Konrad M, Gollop C, Luedde T, Kostev K, Roderburg C. Association between Inflammatory Bowel Disease and Subsequent Development of Restless Legs Syndrome and Parkinson’s Disease: A Retrospective Cohort Study of 35,988 Primary Care Patients in Germany. Life. 2023; 13(4):897. https://doi.org/10.3390/life13040897
Chicago/Turabian StyleLoosen, Sven H., Kaneschka Yaqubi, Petra May, Marcel Konrad, Celina Gollop, Tom Luedde, Karel Kostev, and Christoph Roderburg. 2023. "Association between Inflammatory Bowel Disease and Subsequent Development of Restless Legs Syndrome and Parkinson’s Disease: A Retrospective Cohort Study of 35,988 Primary Care Patients in Germany" Life 13, no. 4: 897. https://doi.org/10.3390/life13040897
APA StyleLoosen, S. H., Yaqubi, K., May, P., Konrad, M., Gollop, C., Luedde, T., Kostev, K., & Roderburg, C. (2023). Association between Inflammatory Bowel Disease and Subsequent Development of Restless Legs Syndrome and Parkinson’s Disease: A Retrospective Cohort Study of 35,988 Primary Care Patients in Germany. Life, 13(4), 897. https://doi.org/10.3390/life13040897