
Prospects of Intravenous Coenzyme Q10 Administration in Emergency Ischemic Conditions

 , and
, and
Abstract
:1. Introduction
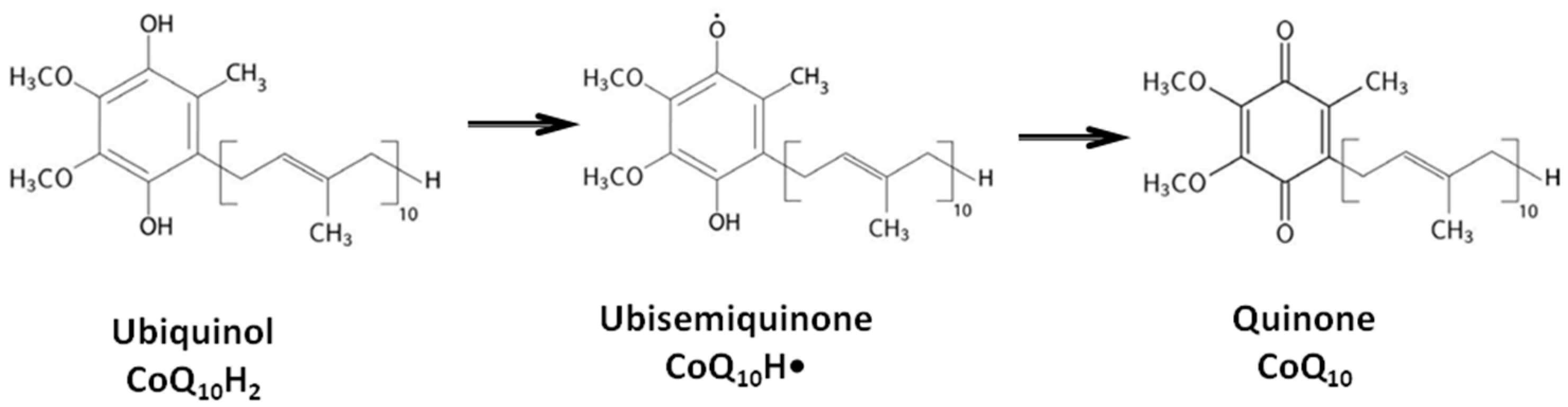
2. Biological Functions of Coenzyme Q10
3. Efficacy of Coenzyme Q10 Therapy When Administered Orally
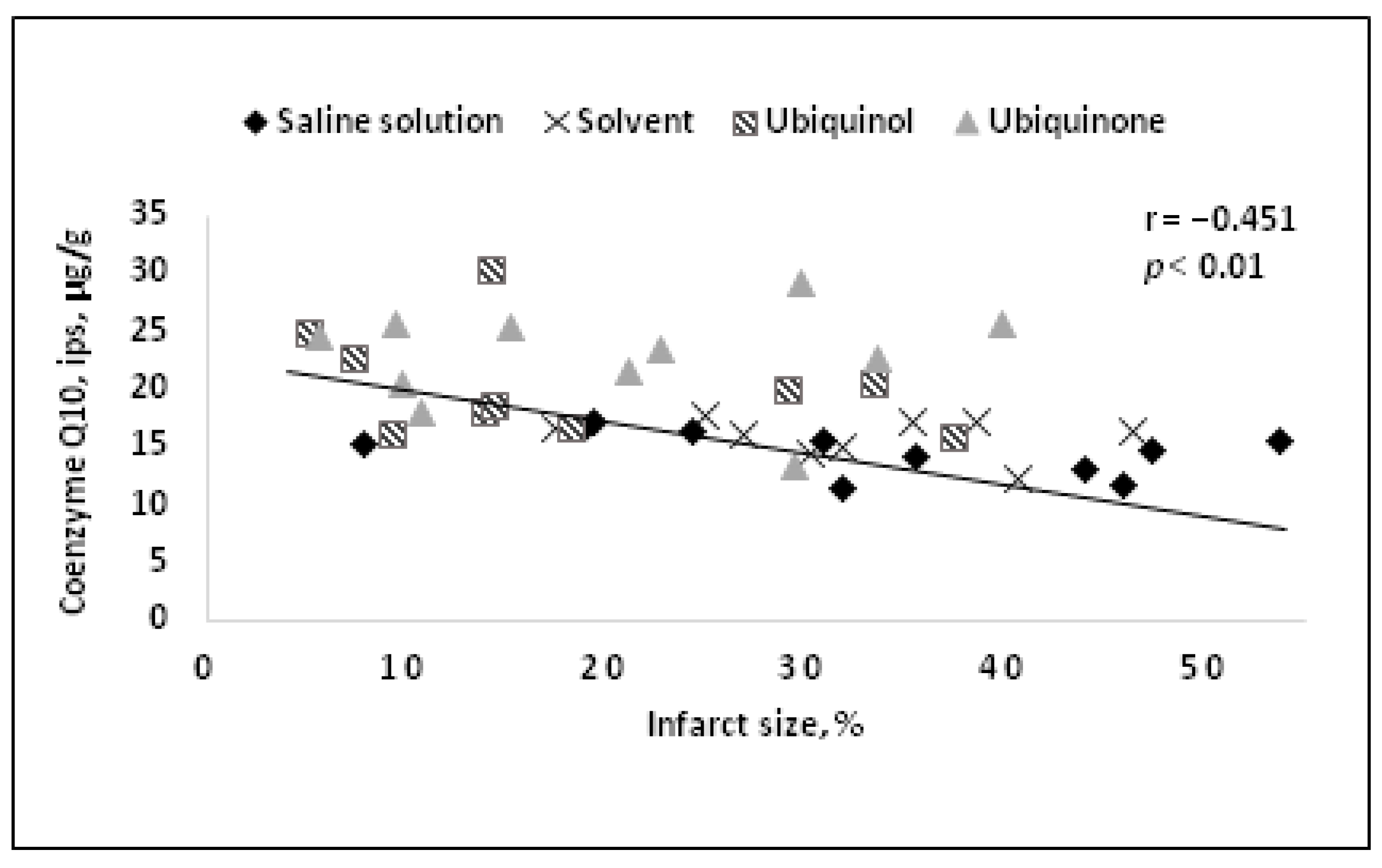
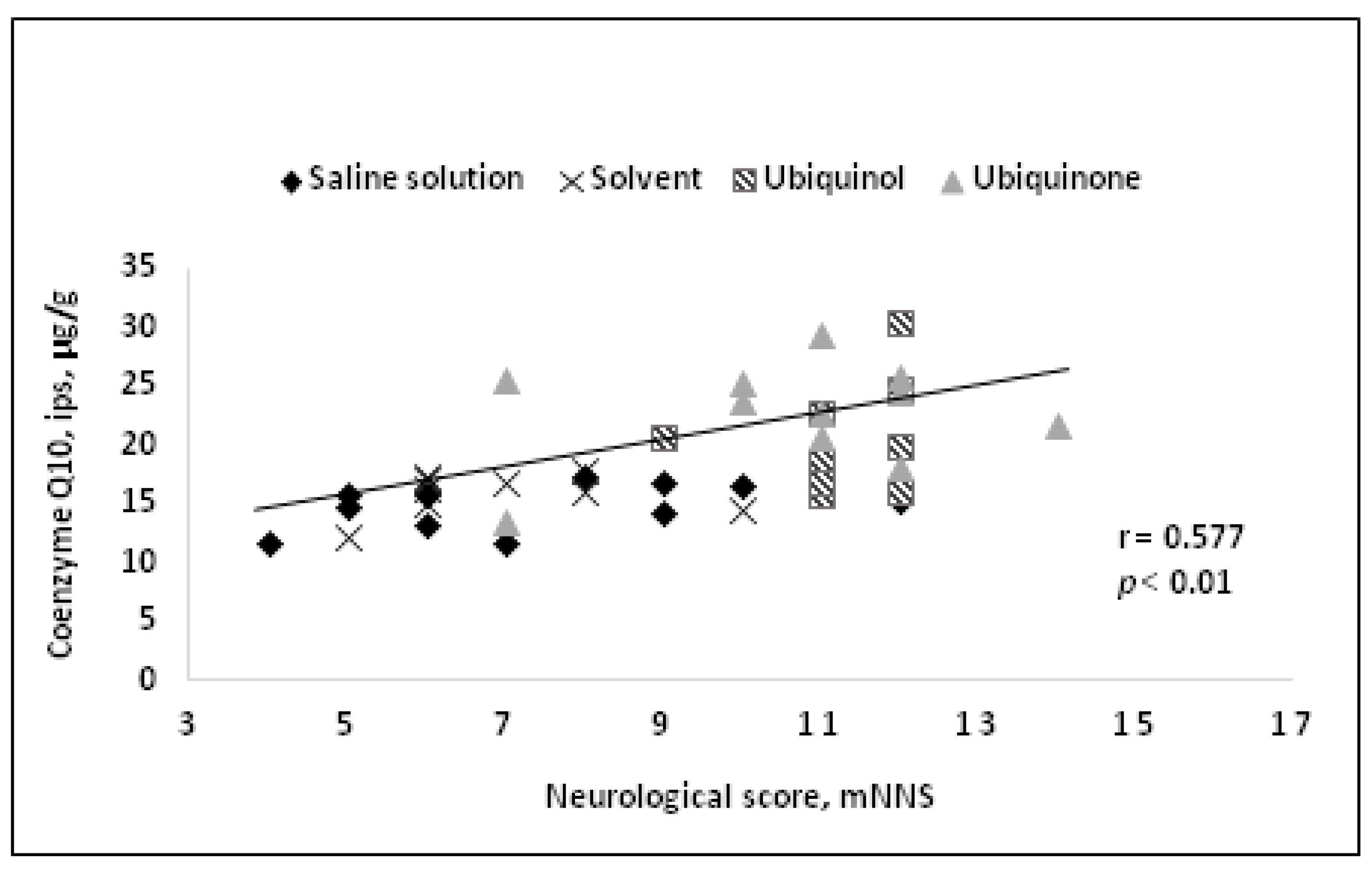
4. Results of Intravenous Coenzyme Q10 Administration in Experimental Models In Vivo
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Crane, F.L.; Hatef, Y.; Lester, R.L.; Widmer, C. Isolation of quinine from beef heart mitochondria. Biochim. Biophys. Acta 1957, 25, 220–221. [Google Scholar] [CrossRef] [PubMed]
- Raizner, A.E. Coenzyme Q10. Methodist DeBakeyCardiovasc. J. 2019, 15, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Li, H.N.; Zimmerman, M.; Milledge, G.Z.; Hou, X.L.; Cheng, J.; Wang, Z.H.; Li, P.A. Water-Soluble Coenzyme Q10 Reduces Rotenone-Induced Mitochondrial Fission. Neurochem. Res. 2017, 42, 1096–1103. [Google Scholar] [CrossRef] [PubMed]
- Bagheri, S.; Haddadi, R.; Saki, S.; Kourosh-Arami, M.; Rashno, M.; Mojaver, A.; Komaki, A. Neuroprotective effects of coenzyme Q10 on neurological diseases: A review article. Front. Neurosci. 2023, 17, 1188839. [Google Scholar] [CrossRef]
- Erol, B.; Bozlu, M.; Hanci, V.; Tokgoz, H.; Bektas, S.; Mungan, G. Coenzyme Q10 treatment reduces lipid peroxidation, inducible and endothelial nitric oxide synthases, and germ cell-specific apoptosis in a rat model of testicular ischemia/reperfusion injury. Fertil. Steril. 2010, 93, 280–282. [Google Scholar] [CrossRef]
- Sattarinezhad, E.; Shafaroodi, H.; Sheikhnouri, K.; Mousavi, Z.; Moezi, L. The effects of coenzyme Q10 on seizures in mice: The involvement of nitric oxide. Epilepsy Behav. 2014, 37, 36–42. [Google Scholar] [CrossRef]
- Guo, J.; Wang, W.Q.; Gong, H. Effects of milk and coenzyme Q10 on the interference of acrylonitrile on vascular endothelial functions. Zhonghua Yi Xue Za Zhi 2011, 91, 1136–1138. (In Chinese) [Google Scholar]
- Gutierrez-Mariscal, F.M.; Arenas-de Larriva, A.P.; Limia-Perez, L.; Romero-Cabrera, J.L.; Yubero-Serrano, E.M.; López-Miranda, J. Coenzyme Q10 Supplementation for the Reduction of Oxidative Stress: Clinical Implications in the Treatment of Chronic Diseases. Int. J. Mol. Sci. 2020, 21, 7870. [Google Scholar] [CrossRef]
- Lopez-Moreno, J.; Quintana-Navarro, G.M.; Delgado-Lista, J.; Garcia-Rios, A.; Alcala-Diaz, J.F.; Gomez-Delgado, F.; Camargo, A.; Perez-Martinez, P.; Tinahones, F.J.; Striker, G.E.; et al. Mediterranean Diet Supplemented with Coenzyme Q10 Modulates the Postprandial Metabolism of Advanced Glycation End Products in Elderly Men and Women. J. Gerontol. A Biol. Sci. Med. Sci. 2018, 73, 340–346. [Google Scholar] [CrossRef]
- Tsuneki, H.; Sekizaki, N.; Suzuki, T.; Kobayashi, S.; Wada, T.; Okamoto, T.; Kimura, I.; Sasaoka, T. Coenzyme Q10 prevents high glucose-induced oxidative stress in human umbilical vein endothelial cells. Eur. J. Pharmacol. 2007, 566, 1–10. [Google Scholar] [CrossRef]
- Tsai, K.-L.; Chen, L.-H.; Chiou, S.-H.; Chiou, G.-Y.; Chen, Y.-C.; Chou, H.-Y.; Chen, L.-K.; Chen, H.-Y.; Chiu, T.-H.; Tsai, C.-S.; et al. Coenzyme Q10 suppresses oxLDL-induced endothelial oxidative injuries by the modulation of LOX-1-mediated ROS generation via the AMPK/PKC/NADPH oxidase signaling pathway. Mol. Nutr. Food Res. 2011, 55, S227–S240. [Google Scholar] [CrossRef]
- Kozaeva, L.P.; Gorodetskaya, E.A.; Ruuge, E.K.; Kalenikova, E.I.; Medvedev, O.S. Beneficial effect of coenzyme Q10 injection on nitric oxide -related dilation of the rat aorta. Eur. J. Pharmacol. 2017, 794, 15–19. [Google Scholar] [CrossRef]
- Gutierrez-Mariscal, F.M.; de la Cruz-Ares, S.; Torres-Peña, J.D.; Alcalá-Diaz, J.F.; Yubero-Serrano, E.M.; López-Miranda, J. Coenzyme Q10 and Cardiovascular Diseases. Antioxidants 2021, 10, 906. [Google Scholar] [CrossRef]
- Ivanova, A.Y.; Shirokov, I.V.; Toshchakov, S.V.; Kozlova, A.D.; Obolenskaya, O.N.; Mariasina, S.S.; Ivlev, V.A.; Gartseev, I.B.; Medvedev, O.S. Effects of Coenzyme Q10 on the Biomarkers (Hydrogen, Methane, SCFA and TMA) and Composition of the Gut Microbiome in Rats. Pharmaceuticals 2023, 16, 686. [Google Scholar] [CrossRef] [PubMed]
- Hargreaves, I.; Heaton, R.A.; Mantle, D. Disorders of Human Coenzyme Q10 Metabolism: An Overview. Int. J. Mol. Sci. 2020, 21, 6695. [Google Scholar] [CrossRef] [PubMed]
- Garrido-Maraver, J.; Cordero, M.D.; Oropesa-Avila, M.; Vega, A.F.; de la Mata, M.; Pavon, A.D.; Alcocer-Gomez, E.; Calero, C.P.; Paz, M.V.; Alanis, M.; et al. Clinical applications of coenzyme Q10. Front.Biosci. (Landmark Ed.) 2014, 19, 619–633. [Google Scholar] [CrossRef] [PubMed]
- Testai, L.; Martelli, A.; Flori, L.; Cicero, A.F.G.; Colletti, A. Coenzyme Q10: Clinical Applications beyond Cardiovascular Diseases. Nutrients 2021, 13, 1697. [Google Scholar] [CrossRef]
- Kadian, M.; Sharma, G.; Pandita, S.; Sharma, K.; Shrivasatava, K.; Saini, N.; Kumar, A. The Impact of Coenzyme Q10 on Neurodegeneration: A Comprehensive Review. Curr. Pharmacol. Rep. 2022, 8, 1–19. [Google Scholar] [CrossRef]
- Zhang, Y.; Aberg, F.; Appelkvist, E.L.; Dallner, G.; Ernster, L. Uptake of dietary coenzyme Q supplement is limited in rats. J. Nutr. 1995, 125, 446–453. [Google Scholar] [CrossRef]
- Nepal, P.R.; Han, H.K.; Choi, H.K. Enhancement of solubility and dissolution of coenzyme Q10 using solid dispersion formulation. Int. J. Pharm. 2010, 383, 147–153. [Google Scholar] [CrossRef]
- López-Lluch, G.; Del Pozo-Cruz, J.; Sánchez-Cuesta, A.; Cortés-Rodríguez, A.B.; Navas, P. Bioavailability of coenzyme Q10 supplements depends on carrier lipids and solubilization. Nutrition 2019, 57, 133–140. [Google Scholar] [CrossRef] [PubMed]
- Arenas-Jal, M.; Suñé-Negre, J.M.; García-Montoya, E. Coenzyme Q10 supplementation: Efficacy, safety, and formulation challenges. Compr. Rev. Food Sci. Food Saf. 2020, 19, 574–594. [Google Scholar] [CrossRef] [PubMed]
- Pastor-Maldonado, C.J.; Suárez-Rivero, J.M.; Povea-Cabello, S.; Álvarez-Córdoba, M.; Villalón-García, I.; Munuera-Cabeza, M.; Suárez-Carrillo, A.; Talaverón-Rey, M.; Sánchez-Alcázar, J.A. Coenzyme Q10: Novel Formulations and Medical Trends. Int. J. Mol. Sci. 2020, 21, 8432. [Google Scholar] [CrossRef]
- Pravst, I.; Aguilera, J.C.R.; Rodriguez, A.B.C.; Jazbar, J.; Locatelli, I.; Hristov, H.; Žmitek, K. Comparative Bioavailability of Different Coenzyme Q10 Formulations in Healthy Elderly Individuals. Nutrients 2020, 12, 784. [Google Scholar] [CrossRef]
- Kalenikova, E.I.; Kharitonova, E.V.; Gorodetskaya, E.A.; Tokareva, O.G.; Medvedev, O.S. Redox status and pharmacokinetics of coenzyme Q10 in rat plasma after its single intravenous administration. Biochem. Moscow Suppl. Ser. B 2014, 8, 267–272. [Google Scholar] [CrossRef]
- Mortensen, A.L.; Rosenfeldt, F.; Filipiak, K.J. Effect of coenzyme Q10 in Europeans with chronic heart failure: A sub-group analysis of the Q-SYMBIO randomized double-blind trial. Cardiol. J. 2019, 26, 147–156. [Google Scholar] [CrossRef]
- Mitsui, J.; Matsukawa, T.; Tanaka, M.; Saito-Sato, N.; Nakamoto, F.K.; Yasuda, T.; Naruse, H.; Matsukawa, M.K.; Ishiura, H.; Nagase, M.; et al. Randomized, double-blind, placebo-controlled phase 1study to evaluate the safety and pharmacokinetics of high doses of ubiquinol in healthy adults. Neurol. Clin. Neurosci. 2022, 10, 14–24. [Google Scholar] [CrossRef]
- Al Saadi, T.; Assaf, Y.; Farwati, M.; Turkmani, K.; Al-Mouakeh, A.; Shebli, B.; Khoja, M.; Essali, A.; Madmani, M.E. Coenzyme Q10 for heart failure. Cochrane Database Syst. Rev. 2021, 2, CD008684. [Google Scholar] [CrossRef]
- de Frutos, F.; Gea, A.; Hernandez-Estefania, R.; Rabago, G. Prophylactic treatment with coenzyme Q10 in patients undergoing cardiac surgery: Could an antioxidant reduce complications? A systematic review and meta-analysis. Interact. Cardiovasc. Thorac. Surg. 2015, 20, 254–259. [Google Scholar] [CrossRef]
- Aslanabadi, N.; Safaie, N.; Asgharzadeh, Y.; Houshmand, F.; Ghaffari, S.; Garjani, A.; Dousti, S.; Hamishehkar, H.; Entezari-Maleki, T. The randomized clinical trial of coenzyme Q10 for the prevention of periprocedural myocardial injury following elective percutaneous coronary intervention. Cardiovasc. Ther. 2016, 34, 254–260. [Google Scholar] [CrossRef]
- Liu, Z.; Tian, Z.; Zhao, D.; Liang, Y.; Dai, S.; Liu, M.; Hou, S.; Dong, X.; Zhaxinima; Yang, Y. Effects of Coenzyme Q10 Supplementation on Lipid Profiles in Adults: A Meta-analysis of Randomized Controlled Trials. J. Clin. Endocrinol. Metab. 2022, 108, 232–249. [Google Scholar] [CrossRef] [PubMed]
- Jorat, M.V.; Tabrizi, R.; Mirhosseini, N.; Lankarani, K.B.; Akbari, M.; Heydari, S.T.; Mottaghi, R.; Asemi, Z. The effects of coenzyme Q10 supplementation on lipid profiles among patients with coronary artery disease: A systematic review and meta-analysis of randomized controlled trials. Lipids Health Dis. 2018, 17, 230. [Google Scholar] [CrossRef] [PubMed]
- Hou, S.; Tian, Z.; Zhao, D.; Liang, Y.; Dai, S.; Ji, Q.; Fan, Z.; Liu, Z.; Liu, M.; Yang, Y. Efficacy and Optimal Dose of Coenzyme Q10 Supplementation on Inflammation-Related Biomarkers: AGRADE-Assessed Systematic Review and Updated Meta-Analysis of Randomized Controlled Trials. Mol. Nutr. Food Res. 2023, 67, 220800. [Google Scholar] [CrossRef]
- Qu, H.; Guo, M.; Chai, H.; Wang, W.T.; Gao, Z.Y.; Shi, D.Z. Effects of Coenzyme Q10 on Statin-Induced Myopathy: An Updated Meta-Analysis of Randomized Controlled Trials. J. Am. Heart Assoc. 2018, 7, e009835. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, C.; Köller, Y.; Surkova, E. Effect of Coenzyme Q10 on statin-associated myalgia and adherence to statin therapy: A systematic review and meta-analysis. Atherosclerosis 2020, 299, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Rosenfeldt, F.L.; Haas, S.J.; Krum, H.; Hadj, A.; Ng, K.; Leong, J.Y.; Watts, G.F. Coenzyme Q10 in the treatment of hypertension: A meta-analysis of the clinical trials. J. Hum. Hypertens. 2007, 21, 297–306. [Google Scholar] [CrossRef]
- Tabrizi, R.; Akbari, M.; Sharifi, N.; Lankarani, K.B.; Moosazadeh, M.; Kolahdooz, F.; Taghizadeh, M.; Asemi, Z. The Effects of Coenzyme Q10 Supplementation on Blood Pressures Among Patients with Metabolic Diseases: A Systematic Review and Meta-analysis of Randomized Controlled Trials. High. Blood Press. Cardiovasc. Prev. 2018, 25, 41–50. [Google Scholar] [CrossRef]
- Ramezani, M.; Sahraei, Z.; Simani, L.; Heydari, K.; Shahidi, F. Coenzyme Q10 supplementation in acute ischemic stroke: Is it beneficial in short-term administration? Nutr. Neurosci. 2020, 23, 640–645. [Google Scholar] [CrossRef]
- Sazali, S.; Badrin, S.; Norhayati, M.N.; Idris, N.S. Coenzyme Q10 supplementation for prophylaxis in adult patients with migraine-a meta-analysis. BMJ 2021, 11, e039358. [Google Scholar] [CrossRef]
- Cochrane Library. Available online: https://www.cochranelibrary.com/advanced-search/search-manager (accessed on 14 November 2023).
- World Health Organisation. International Clinical Trial Registry Platform. Available online: https://trialsearch.who.int/Trial2.aspx?TrialID=IRCT20210907052400N1 (accessed on 14 November 2023).
- World Health Organisation. International Clinical Trial Registry Platform. Available online: https://trialsearch.who.int/Trial2.aspx?TrialID=ChiCTR1900025513 (accessed on 14 November 2023).
- World Health Organisation. International Clinical Trial Registry Platform. Available online: https://trialsearch.who.int/Trial2.aspx?TrialID=ACTRN12605000545662 (accessed on 14 November 2023).
- Ali, S.H.; Dizaye, K.F. Influence of ubiquinol on angina severity and dyspnea in patients with acute coronary syndrome. J. Popul. Ther. Clin. Pharmacol. 2023, 30, e405–e414. [Google Scholar] [CrossRef]
- Sangouni, A.A.; Taghdir, M.; Mirahmadi, J.; Sepandi, M.; Parastouei, K. Effects of curcumin and/or coenzyme Q10 supplementation on metabolic control in subjects with metabolic syndrome: A randomized clinical trial. Nutr. J. 2022, 21, 62. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. International Clinical Trial Registry Platform. Available online: https://trialsearch.who.int/Trial2.aspx?TrialID=ChiCTR2100045256 (accessed on 14 November 2023).
- Samuel, T.Y.; Hasin, T.; Gotsman, I.; Weitzman, T.; Ben Ivgi, F.; Dadon, Z.; Asher, E.; Amir, O.; Glikson, M.; Alcalai, R.; et al. Coenzyme Q10 in the Treatment of Heart Failure with Preserved Ejection Fraction: A Prospective, Randomized, Double-Blind, Placebo-Controlled Trial. Drugs R D 2022, 22, 25–33. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. International Clinical Trial Registry Platform. Available online: https://trialsearch.who.int/Trial2.aspx?TrialID=ChiCTR2100053923 (accessed on 14 November 2023).
- ClinicalTrial.gov. Available online: https://clinicaltrials.gov/ct2/show/NCT05984745 (accessed on 14 November 2023).
- ClinicalTrial.gov. Available online: https://clinicaltrials.gov/show/NCT05731596 (accessed on 14 November 2023).
- Zhang, P.; Chen, K.; He, T.; Guo, H.; Chen, X. Coenzyme Q10 supplementation improves adipokine profile in dyslipidemic individuals: A randomized controlled trial. Nutr. Metab. 2022, 19, 13. [Google Scholar] [CrossRef]
- Golmohammadi, S. Effects of coenzyme Q10 supplementation on renal function parameters in patients with diabetic nephropathy: A randomized controlled trial. Kidney Int. Rep. 2022, 7, S226. [Google Scholar] [CrossRef]
- Cochrane Library. Available online: https://www.cochranelibrary.com/central/doi/10.1002/central/CN-02586031/full (accessed on 12 January 2024).
- ClinicalTrial.gov. Available online: https://clinicaltrials.gov/study/NCT05871086#study-plan (accessed on 14 November 2023).
- Karamali, M.; Gholizadeh, M. The effects of coenzyme Q10 supplementation on metabolic profiles and parameters of mental health in women with polycystic ovary syndrome. Gynecol. Endocrinol. 2022, 38, 45–49. [Google Scholar] [CrossRef]
- Ahmadi, A.; Begue, G.; Valencia, A.P.; Norman, J.E.; Lidgard, B.; Bennett, B.J.; Van Doren, M.P.; Marcinek, D.J.; Fan, S.; Prince, D.K.; et al. Randomized crossover clinical trial of coenzyme Q10 and nicotinamide ribosome in chronic kidney disease. JCI Insight 2023, 8, e167274. [Google Scholar] [CrossRef] [PubMed]
- Amini, P.; Sajedi, F.; Mirjalili, M.; Mohammadi, Y.; Mehrpooya, M. Coenzyme Q10 as a potential add-on treatment for patients suffering from painful diabetic neuropathy: Results of a placebo-controlled randomized trial. Eur. J. Clin. Pharmacol. 2022, 78, 1899–1910. [Google Scholar] [CrossRef] [PubMed]
- Holmberg, M.J.; Andersen, L.W.; Moskowitz, A.; Berg, K.M.; Cocchi, M.N.; Chase, M.; Liu, X.; Kuhn, D.M.; Grossestreuer, A.V.; Hoeyer-Nielsen, A.K.; et al. Ubiquinol (reduced coenzyme Q10) as a metabolic resuscitator in post-cardiac arrest: A randomized, double-blind, placebo-controlled trial. Resuscitation 2021, 162, 388–395. [Google Scholar] [CrossRef]
- Ho, M.J.; Li, E.C.; Wright, J.M. Blood pressure lowering efficacy of coenzyme Q10 for primary hypertension. Cochrane Database Syst. Rev. 2016, 3, CD007435. [Google Scholar] [CrossRef]
- Mantle, D.; Lopez-Lluch, G.; Hargreaves, I.P. Coenzyme Q10 Metabolism: A Review of Unresolved Issues. Int. J. Mol. Sci. 2023, 24, 2585. [Google Scholar] [CrossRef]
- Wang, Y.; Hekimi, S. Understanding Ubiquinone. Trends Cell Biol. 2016, 26, 367–378. [Google Scholar] [CrossRef] [PubMed]
- Hernansanz-Agustín, P.; Choya-Foces, C.; Carregal-Romero, S.; Ramos, E.; Oliva, T.; Villa-Piña, T.; Moreno, L.; Izquierdo-Álvarez, A.; Cabrera-García, J.D.; Cortés, A.; et al. Na+ controls hypoxic signalling by the mitochondrial respiratory chain. Nature 2020, 586, 287–291. [Google Scholar] [CrossRef]
- Grieb, P.; Ryba, M.S.; Sawicki, J.; Chrapusta, S.J. Oral coenzyme Q10 administration prevents the development of ischemic brain lesions in a rabbit model of symptomatic vasospasm. Acta Neuropathol. 1997, 94, 363–368. [Google Scholar] [CrossRef] [PubMed]
- Kramer, D.R.; Fujii, T.; Ohiorhenuan, I.; Liu, C.Y. Cortical spreading depolarization: Pathophysiology, Implications, and future directions. J. Clin. Neurosci. 2016, 24, 22–27. [Google Scholar] [CrossRef] [PubMed]
- Awad, K.; Sayed, A.; Banach, M. Coenzyme Q10 Reduces Infarct Size in Animal Models of Myocardial Ischemia-Reperfusion Injury: A Meta-Analysis and Summary of Underlying Mechanisms. Front. Cardiovasc. Med. 2022, 9, 857364. [Google Scholar] [CrossRef] [PubMed]
- Ghasemloo, E.; Oryan, S.; Bigdeli, M.R.; Mostafavi, H.; Eskandari, M. The neuroprotective effect of MicroRNA-149-5p and coenzymeQ10 by reducing levels of inflammatory cytokines and metalloproteinases following focal brain ischemia in rats. Brain Res. Bull. 2021, 169, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Singh, R.B.; Fedacko, J.; Mojto, V.; Pella, D. Coenzyme Q10 Modulates Remodeling Possibly by Decreasing Angiotensin-Converting Enzyme in Patients with Acute Coronary Syndrome. Antioxidants 2018, 7, 99. [Google Scholar] [CrossRef]
- Zhou, M.; Zhi, Q.; Tang, Y.; Yu, D.; Han, J. Effects of coenzyme Q10 on myocardial protection during cardiac valve replacement and scavenging free radical activity in vitro. J. Cardiovasc. Surg. 1999, 40, 355–361. [Google Scholar]
- Wang, Y.; Hekimi, S. Micellization of coenzyme Q by the fungicide caspofungin allows for safe intravenous administration to reach extreme supraphysiological concentrations. Redox Biol. 2020, 36, 101680. [Google Scholar] [CrossRef]
- Honardoust, P.; Najafpour, A.; Mohammadi, R. Influence of Systemic Administration of CoQ10 Nanoparticles on Ischemia-Reperfusion Injury on Ovaries in Rat. Evid. Based Complement. Alternat Med. 2021, 2021, 2303417. [Google Scholar] [CrossRef]
- Niibori, K.; Yokoyama, H.; Crestanello, J.A.; Whitman, G.J. Acute administration of liposomal coenzyme Q10 increases myocardial tissue levels and improves tolerance to ischemia reperfusion injury. J. Surg. Res. 1998, 79, 141–145. [Google Scholar] [CrossRef] [PubMed]
- Takada, M.; Watanabe, J. A possible mode of solubilization of coenzyme Q10 with HCO-60. J. Pharmacobiodyn. 1987, 10, 124–127. [Google Scholar] [CrossRef]
- Verma, D.D.; Hartner, W.C.; Thakkar, V.; Levchenko, T.S.; Torchilin, V.P. Protective effect of coenzyme Q10-loaded liposomes on the myocardium in rabbits with an acute experimental myocardial infarction. Pharm. Res. 2007, 24, 2131–2137. [Google Scholar] [CrossRef]
- Eleawa, S.M.; Alkhateeb, M.; Ghosh, S.; Al-Hashem, F.; Shatoor, A.S.; Alhejaily, A.; Khalil, M.A. Coenzyme Q10 protects against acute consequences of experimental myocardial infarction in rats. Int. J. Physiol. Pathophysiol. Pharmacol. 2015, 7, 1–13. [Google Scholar]
- Dadali, Y.V.; Fomichev, Y.S.; Gorodetskaya, E.A.; Kalenikova, E.I.; Karlina, M.V.; Makarov, V.G.; Makarova, M.N.; Medvedev, O.S.; Pozharitskaya, O.N.; Shikov, A.N. Ubiquinol Composition for Parenteral Administration and Method for Its. Production. Patent RU2635993-C1, 17 November 2017. (In Russian). [Google Scholar]
- Kalenikova, E.I.; Gorodetskaya, E.A.; Obolenskaya, O.N.; Shapavo, N.S.; Medvedev, O.S. Pharmacokinetics and Tissue Distribution of Oxidized and Reduced Coenzyme Q10 Upon Intravenous Administration. Pharm. Chem. J. 2021, 55, 633–637. [Google Scholar] [CrossRef]
- Ivanov, A.; Gorodetskaya, E.; Kalenikova, E.; Medvedev, O. Single intravenous injection of CoQ10 reduces infarct size in a rat model of ischemia and reperfusion injury. World J. Cardiovasc. Dis. 2013, 3, 1–7. [Google Scholar] [CrossRef]
- Ivanov, A.V.; Gorodetskaya, E.A.; Kalenikova, E.I.; Medvedev, O.S. Single intravenous injection of coenzyme Q10 protects the myocardium after irreversible ischemia. Bull. Exp. Biol. Med. 2013, 155, 771–774. [Google Scholar] [CrossRef]
- Ivanov, A.V.; Tokareva, O.G.; Gorodetskaya, E.A.; Kalenikova, E.I.; Medvedev, O.S. Cardioprotection with Intravenous Injection of Coenzyme Q10 is limited by Time of Administration after Onset of Myocardial Infarction in Rats. J. Clin. Exp. Cardiolog. 2014, 5, 299. [Google Scholar] [CrossRef]
- Kulyak, O.Y.; Gorodetskaya, E.A.; Kalenikova, E.I.; Makarova, M.N.; Pozharitskaya, O.N.; Medvedev, O.S. Evaluation of cardioprotective efficacy of innovative dosage form of ubiqinol for intravenous administration. Eksp. Klin. Farmakol. 2018, 81, 8–11. [Google Scholar] [CrossRef]
- Belousova, M.; Tokareva, O.G.; Gorodetskaya, E.A.; Kalenikova, E.I.; Medvedev, O.S. Intravenous Treatment with Coenzyme Q10 Improves Neurological Outcome and Reduces Infarct Volume after Transient Focal Brain Ischemia in Rats. J. Cardiovasc. Pharmacol. 2016, 67, 103–109. [Google Scholar] [CrossRef]
- Belousova, M.A.; Tokareva, O.G.; Gorodetskaya, E.A.; Kalenikova, E.I.; Medvedev, O.S. Neuroprotective Effectiveness of Intravenous Ubiquinone in Rat Model of Irreversible Cerebral Ischemia. Bull. Exp. Biol. Med. 2016, 161, 205–207. [Google Scholar] [CrossRef] [PubMed]
- Obolenskaia, O.N.; Gorodetskaya, E.A.; Kalenikova, E.I.; Belousova, M.A.; Gulyaev, M.V.; Makarov, V.G.; Pirogov, Y.A.; Medvedev, O.S. Intravenous Administration of Coenzyme Q10 in Acute Period of Cerebral Ischemia Decreases Mortality by Reducing Brain Necrosis and Limiting its Increase within 4 Days in Rat Stroke Model. Antioxidants 2020, 9, 1240. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Disease | Name of Study | Daily Dose of CoQ10, Duration of Administration | Results | Country, Year of Registration |
|---|---|---|---|---|
| Ischemic stroke | Evaluation of the effects of coenzyme Q10 on stroke | 600 mg/day for 30 days, per os | Not yet published | Iran, 2021 [41] |
| Children with tetralogy of Fallot | The safety and efficacy of preoperative oral supplementation of coenzyme Q10 in improving postoperative cardiac function in children with tetralogy of Fallot (pulmonary atresia): a preliminary study | Different dosages before surgery: 2.5 mg; 5 mg; 10 mg; 20 mg. Duration not specified, per os | Not yet published | China, 2019 [42] |
| Statin-induced myalgia | Coenzyme Q10 and tolerability of simvastatin in subjects with a history of statin-induced myalgia | 200 mg/day for about 3 months, per os | Not yet published | New Zealand, since 2005 (update 2020) [43] |
| Acute coronary syndrome (ACS) | Influence of ubiquinol on angina severity and dyspnea in patients with acute coronary syndrome | 200 mg/day of ubiquinol for 8 weeks | Ubiquinol addition to optimal medical therapy (OMT) after ACS has a highly significant effect on improving clinical outcomes and patients’ quality of life through greater reductions in angina frequency, physical limitations, and dyspnea severity. This suggests an effective and safe strategy for optimizing therapeutic outcomes and secondary prevention | Iraq, 2023 [44] |
| Metabolic syndrome | Effects of curcumin and/or coenzyme Q10 supplementation on metabolic control in subjects with metabolic syndrome: a randomized clinical trial | 60 mg/day for 12 weeks, per os | CoQ10 showed no therapeutic effects | Iraq, 2021 [45] |
| Acute myocardial infarction | A randomized controlled trial on the effect of Co Q10 on vascular endothelial and cardiac function after percutaneous coronary intervention therapy for acute myocardial infarction | Dose and duration of administration not specified, per os | Not yet published | China, 2021 [46] |
| Heart failure with preserved ejection fraction (HFpEF) | Coenzyme Q10 in the treatment of heart failure with preserved ejection fraction: a prospective, randomized, double-blind, placebo-controlled trial | 300 mg/day of ubiquinol for 4 months, per os | In this pilot trial in elderly patients with HFpEF, treatment with CoQ10 did not significantly affect echocardiographic indices of diastolic function and serum N-terminal pro-B-type natriuretic peptide (NT-proBNP) levels. | Israel, 2021 [47] |
| Prevention of high-altitude heart disease | Effect of Coenzyme Q10 on prevention of high-altitude heart disease and improvement of cardiac function | Different dosages, dose and duration not specified, per os | Not yet published | China, 2021 [48] |
| Metabolic associated fatty liver disease (MAFLD) | Effect of CoQ10 on the outcome of MAFLD patients | 200 mg/day for 12 weeks, per os | Not yet published | Egypt, 2023 [49] |
| Nonalcoholic steatohepatitis | Comparative clinical study to evaluate the efficacy and safety of rosuvastatin vs. CoQ10 on nonalcoholic steatohepatitis | 100 mg/day for 3 months, per os | Not yet published | Egypt, 2023 [50] |
| Dyslipidemia | Coenzyme Q10 supplementation improves adipokine profile in dyslipidemic individuals: a randomized controlled trial | 120 mg/day for 24 weeks, per os | This study shows that CoQ10 ameliorates glucolipid profile and adipokines dysfunction in dyslipidemic patients in 24 weeks’ intervention. The beneficial effect of CoQ10 on glucolipid profile was mediated by adiponectin. | China, 2022 [51] |
| Diabetic nephropathy | Effects of coenzyme Q10 supplementation on renal function parameters in patients with diabetic nephropathy: a randomized controlled trial | 100 mg/day for 6 months, per os | This study found that daily administration of 100 mg CoQ10 improved the mean proteinuria, glomerular filtration rate (GFR) and creatinine levels in patients with diabetic nephropathy. | Iran, 2022 [52] |
| Acute herpes zoster | To evaluate the analgesic effect of Co Q10 in acute herpes zoster | 100 mg/day for 4 weeks, per os | Not yet published | India, 2023 [53] |
| Juvenile idiopathic arthritis | Coenzyme Q10 in juvenile idiopathic arthritis patients | 100 mg/day for 3 months, per os | Not yet published | Egypt, 2023 [54] |
| Polycystic ovary syndrome (PCOS) | The effects of coenzyme Q10 supplementation on metabolic profiles and parameters of mental health in women with polycystic ovary syndrome | 100 mg/day for 12 weeks, per os | 12-week supplementation of CoQ10 to women with PCOS showed beneficial impact on the scores of Beck Depression Inventory(BDI), Beck Anxiety Inventory(BAI), high-sensitivity C-reactive protein(hs-CRP), total testosterone, dehydroepiandrosterone sulfate (DHEAS), hirsutism, sex hormone-binding globulin (SHBG), total antioxidant capacity (TAC) and malondialdehyde (MDA) levels. | Iran, 2021 [55] |
| Chronic kidney disease | Randomized crossover clinical trial of coenzyme Q10 and nicotinamide ribosome (NR) in chronic kidney disease | 1200 mg/day for 6 weeks, per os | Six-weeks of treatment with NR or CoQ10 improved markers of systemic mitochondrial metabolism and lipid profiles but did not improve VO2 peak or total work efficiency. CoQ10 increased free fatty acids and decreased complex medium/long chain triglycerides. | USA, 2023 [56] |
| Diabetic neuropathy | Coenzyme Q10 as a potential add-on treatment for patients suffering from painful diabetic neuropathy: results of a placebo-controlled randomized trial | 100 mg every 8 h for 8 weeks, per os | This trial support the idea that diabetic patients suffering from painful diabetic neuropathy may benefit from using antioxidant and anti-inflammatory supplements like CoQ10. However, further studies are required before supplementation with CoQ10 can be recommended for treating painful diabetic neuropathy. | Iran, 2021 [57] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kalenikova, E.I.; Gorodetskaya, E.A.; Povarova, O.V.; Medvedev, O.S. Prospects of Intravenous Coenzyme Q10 Administration in Emergency Ischemic Conditions. Life 2024, 14, 134. https://doi.org/10.3390/life14010134
Kalenikova EI, Gorodetskaya EA, Povarova OV, Medvedev OS. Prospects of Intravenous Coenzyme Q10 Administration in Emergency Ischemic Conditions. Life. 2024; 14(1):134. https://doi.org/10.3390/life14010134
Chicago/Turabian StyleKalenikova, Elena I., Evgeniya A. Gorodetskaya, Oxana V. Povarova, and Oleg S. Medvedev. 2024. "Prospects of Intravenous Coenzyme Q10 Administration in Emergency Ischemic Conditions" Life 14, no. 1: 134. https://doi.org/10.3390/life14010134
APA StyleKalenikova, E. I., Gorodetskaya, E. A., Povarova, O. V., & Medvedev, O. S. (2024). Prospects of Intravenous Coenzyme Q10 Administration in Emergency Ischemic Conditions. Life, 14(1), 134. https://doi.org/10.3390/life14010134