
Comparison of Bioelectrical Impedance Analysis (BIA)-Derived Parameters in Healthy Volunteers and Critically Ill Patients

 , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Regulations
2.2. Study Design
2.3. Data Collection
2.4. BIA Measurements
- –
- TBW, ICW, and ECW (liter and %)
- –
- The ECW/ICW ratio
- –
- Volume excess (VE, L)
- –
- Fat-free mass (FFM, kg and %), fat-free mass hydration (FFMH, %), and fat mass (FM, kg and %)
- –
- Protein mass (kg), mineral mass (kg), bone mass (kg), muscle mass (kg)
- –
- Resting metabolic rate (RMR), glycogen deposits (g)
- –
- Total body calcium (TBCa, g)
- –
- Malnutrition index.
2.5. Statistical Analysis
3. Results
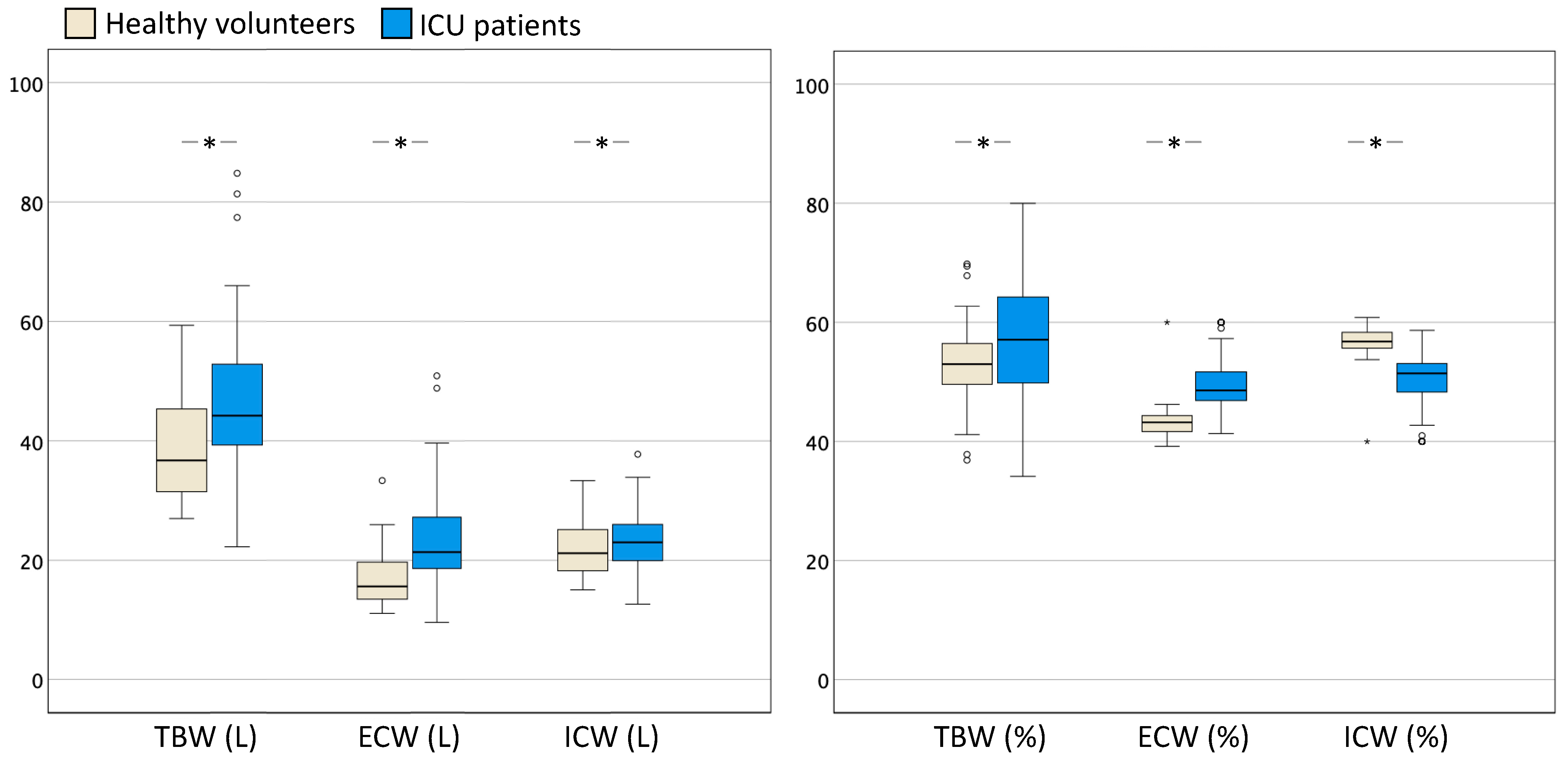
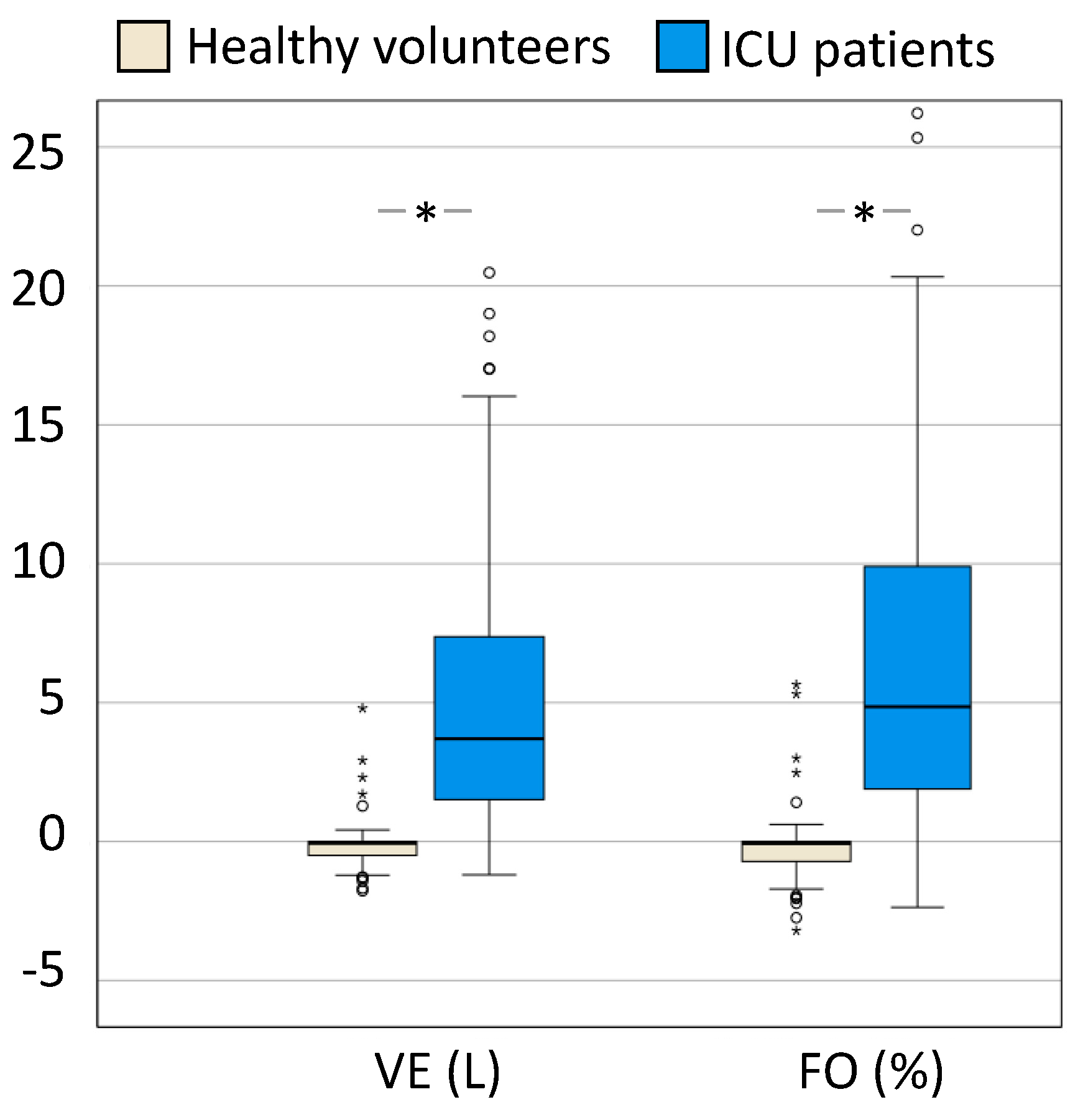
3.1. ICU Patients vs. Healthy Volunteers
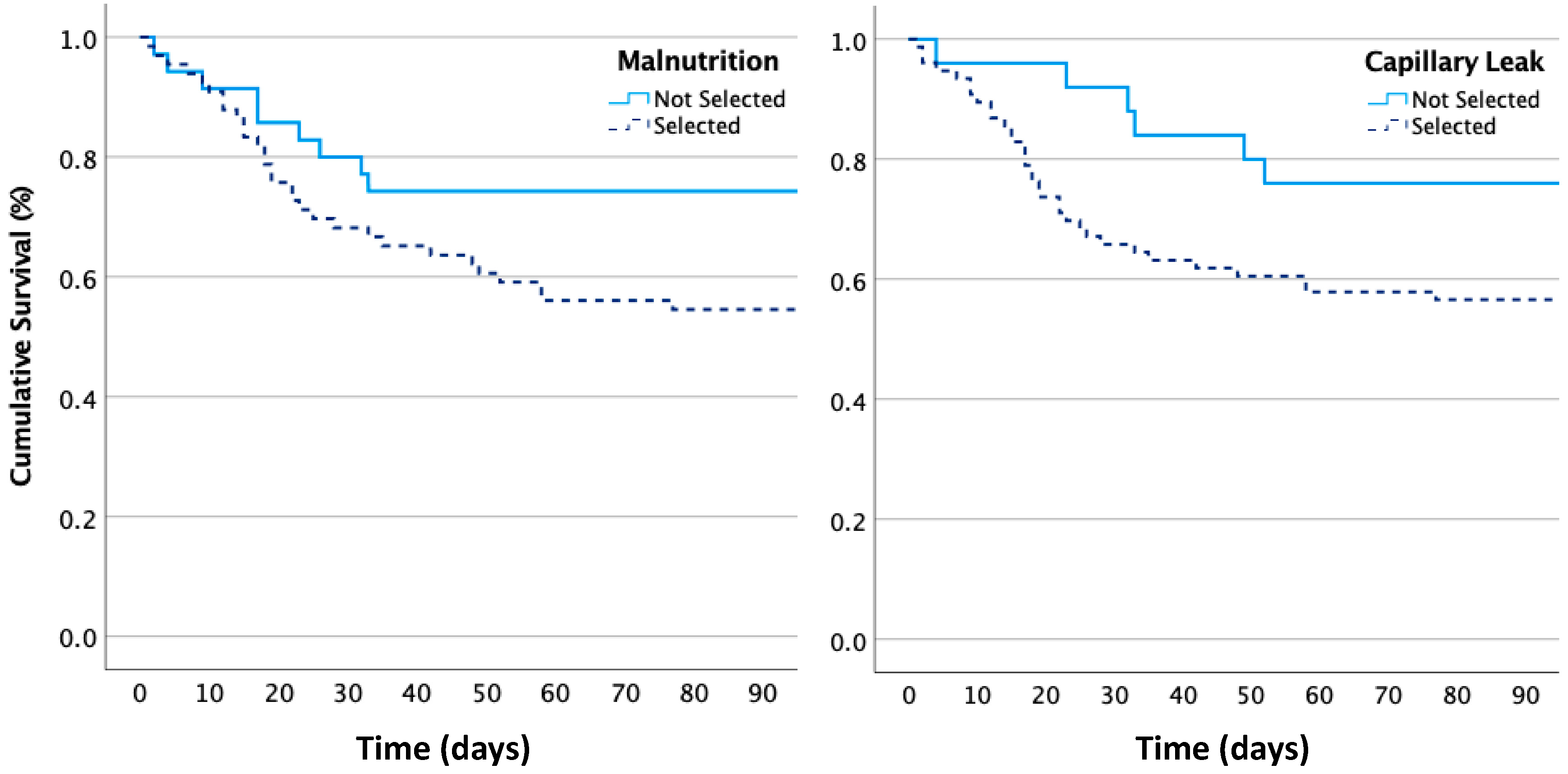
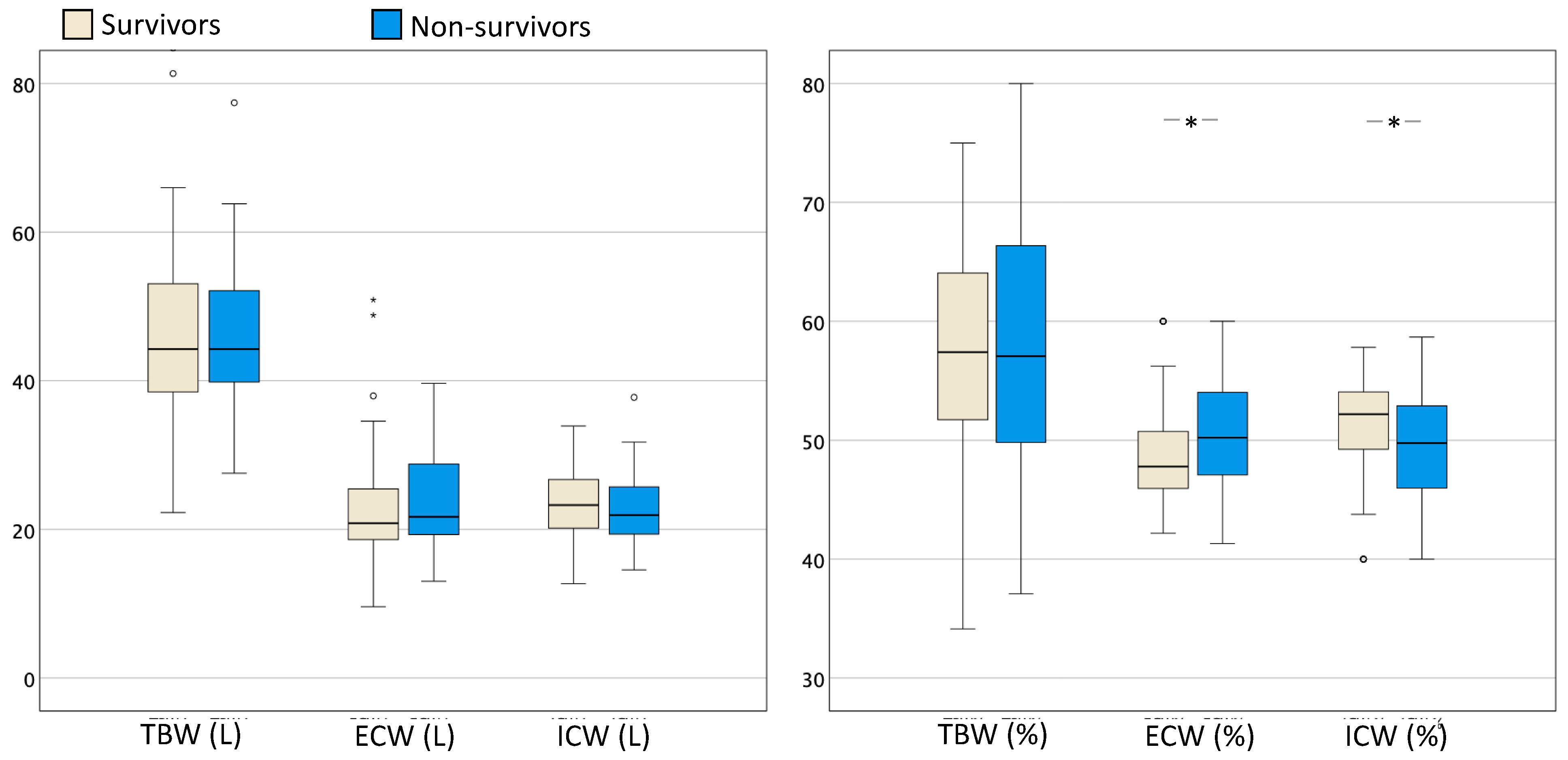
3.2. Survivors vs. Non-Survivors in the ICU Population
4. Discussion
4.1. Differences between Healthy Volunteers and ICU Patients
4.2. Differences between Survivors and Non-Survivors
4.3. Importance of Fluid Overload and Intra-Abdominal Hypertension
4.4. Study Limitations
5. Conclusions
6. Take Home Messages
- Overall, this study contributes to the growing body of literature on the utility of BIA-derived parameters in critically ill patients and underscores the impact of inflammation and capillary leak on fluid distribution in this population.
- This study highlights the importance of considering gender-specific differences in BIA-derived parameters when assessing fluid status in healthy volunteers as well as critically ill patients. By considering these differences, clinicians can tailor their fluid management strategies more effectively to optimize patient outcomes.
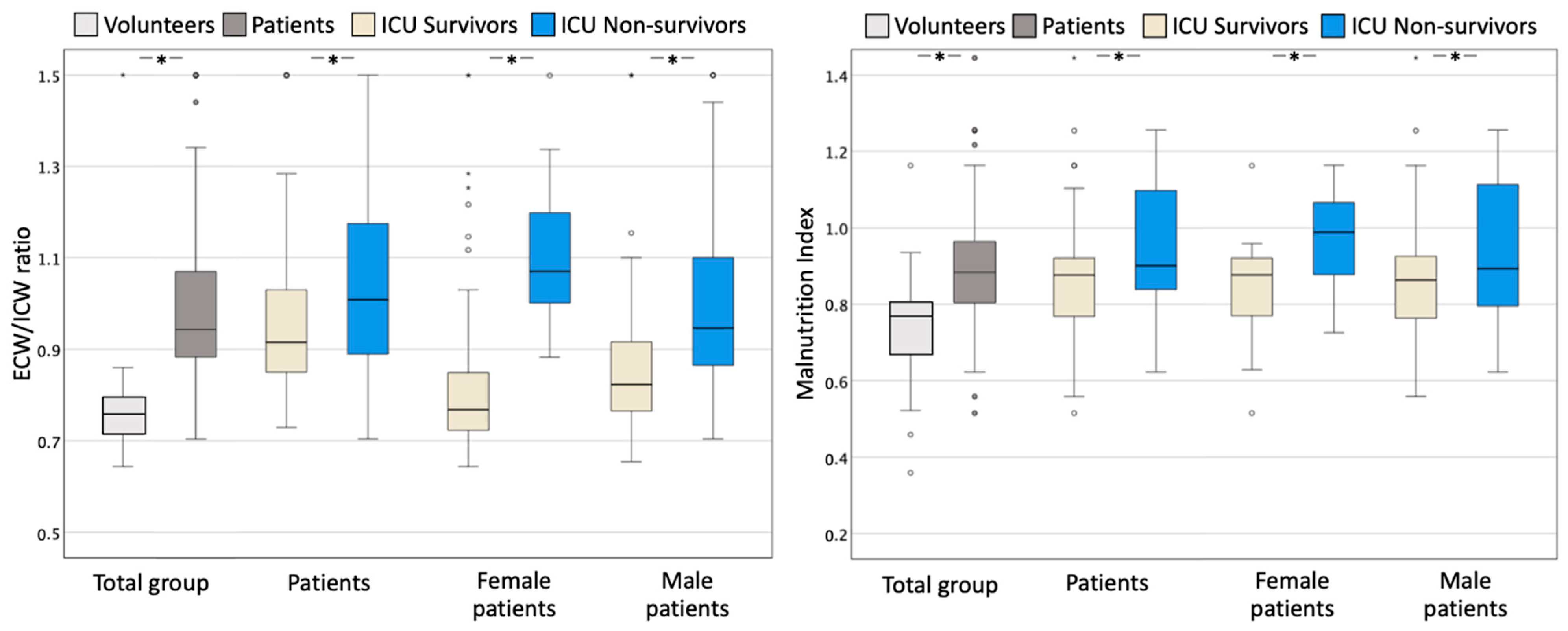
- The results add to the growing body of evidence that BIA-derived parameters (showing a decrease in ICW and increase in ECW and the ECW/ICW ratio) can provide valuable insights into the fluid status of critically ill patients.
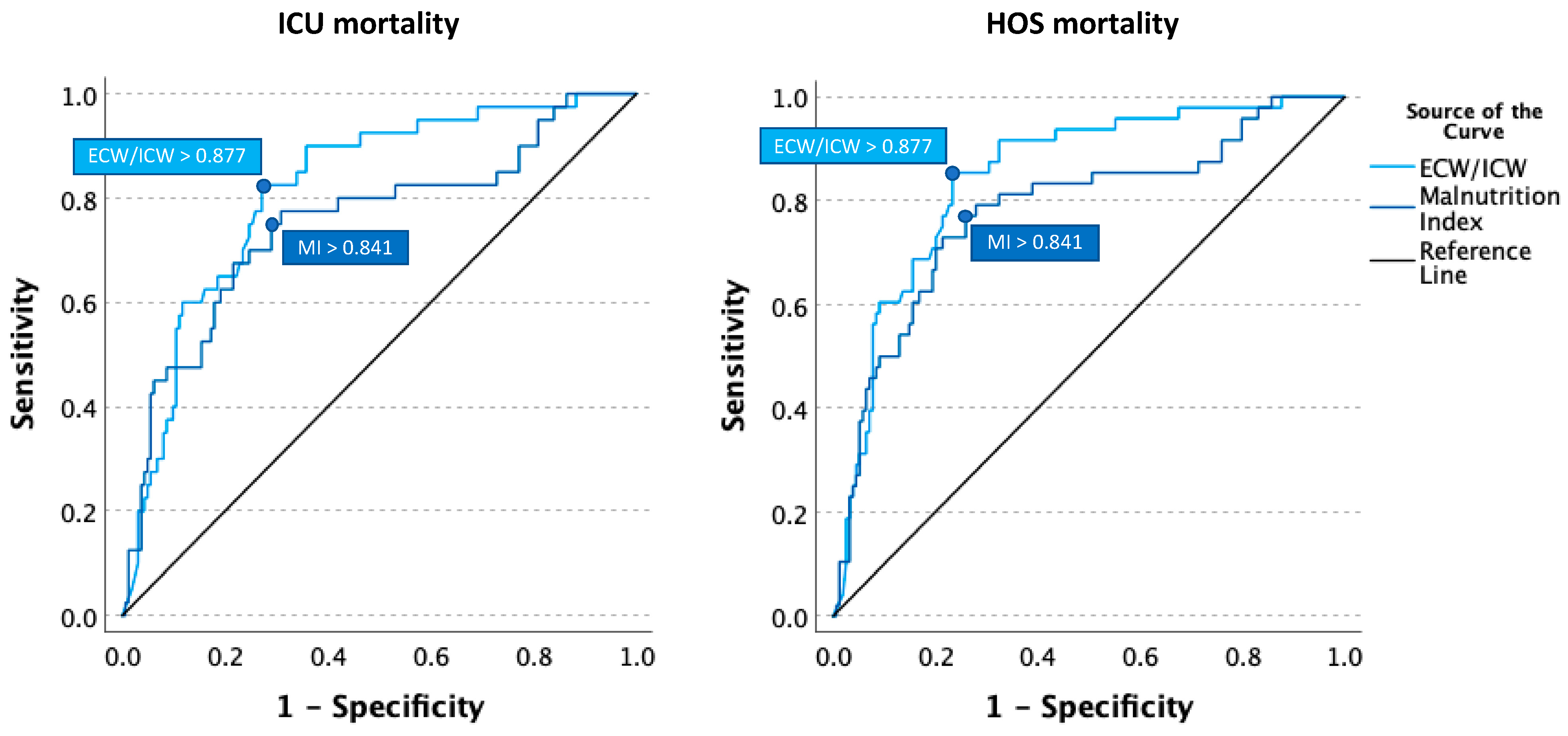
- We propose to identify capillary leak as an increased ECW/ICW ratio above 0.9, as was shown with the AUROC analysis.
- Findings highlight the importance of using a comprehensive approach that considers clinical factors, such as the SAPS-II score, when assessing the prognosis of ICU patients.
- Findings also highlight the importance of PhA and the malnutrittion index as prognostic factors in critically ill patients and suggest that they may be a useful addition to routine BIA-derived parameters for assessing mortality risk in ICU patients.
- We identified a malnutrition index above 0.8 to be associated with poor outcomes.
- While the relationship between ICW and mortality remains unclear, this study demonstrated that several BIA-derived parameters, including ECW/ICW, were related to mortality in ICU patients.
- Further studies are needed to validate these findings and to better understand the relationship between BIA-derived parameters and clinical outcomes in critically ill patients.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| APACHE II | Acute Physiology and Chronic Health Evaluation II |
| BIA | Bio-electrical impedance analysis |
| BIVA | Bioelectrical impedance vector analysis |
| BVA | Blood volume assessment |
| BCM | Body cell mass |
| BMI | Body mass index |
| CCR | Creatinine clearance rate |
| COPD | Chronic obstructive pulmonary disease |
| CRP | C-reactive protein |
| DEXA | Dual-energy X-ray absorptiometry |
| ECF | Extracellular fluid |
| ECS | Extracellular solids |
| ECW | Extracellular water |
| ECW% | Extracellular water percentage |
| FA | Fluid accumulation |
| FAS | Fluid accumulation syndrome |
| FAT% | Fat in percentage |
| FFM | Fat-free mass |
| FFMH% | Fat-free mass hydration percentage |
| GFR | Glomerular filtration rate |
| FO | Fluid overload |
| Hct | Haematocrit |
| IAP | Intra-abdominal pressure |
| IAH | Intra-abdominal hypertension |
| ICU | Intensive care unit |
| ICW | Intracellular water |
| ICW% | Intracellular water percentage |
| PhA | Phase angle |
| RMR | Resting metabolic rate |
| ROC | Receiver operating characteristics |
| SAPS | Simplified Acute Physiology Score |
| SOFA | Sequential Organ Failure Assessment |
| TBCa | Total body calcium |
| TBK | Total body potassium |
| TBW | Total body water |
| VE | Volume excess |
| ZNA | Ziekenhuisnetwerk Antwerpen |
References
- Rhodes, A.; Evans, L.E.; Alhazzani, W.; Levy, M.M.; Antonelli, M.; Ferrer, R.; Kumar, A.; Sevransky, J.E.; Sprung, C.L.; Nunnally, M.E.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Intensive Care Med. 2017, 43, 304–377. [Google Scholar] [CrossRef]
- Basso, F.; Berdin, G.; Virzi, G.M.; Mason, G.; Piccinni, P.; Day, S.; Cruz, D.N.; Wjewodzka, M.; Giuliani, A.; Brendolan, A.; et al. Fluid management in the intensive care unit: Bioelectrical impedance vector analysis as a tool to assess hydration status and optimal fluid balance in critically ill patients. Blood Purif. 2013, 36, 192–199. [Google Scholar] [CrossRef]
- Slobod, D.; Yao, H.; Mardini, J.; Natkaniec, J.; Correa, J.A.; Jayaraman, D.; Weber, C.L. Bioimpedance-measured volume overload predicts longer duration of mechanical ventilation in intensive care unit patients. Can. J. Anaesth. 2019, 66, 1458–1463. [Google Scholar] [CrossRef]
- Vincent, J.L.; Sakr, Y.; Sprung, C.L.; Ranieri, V.M.; Reinhart, K.; Gerlach, H.; Moreno, R.; Carlet, J.; Le Gall, J.R.; Payen, D.; et al. Sepsis in European intensive care units: Results of the SOAP study. Crit. Care Med. 2006, 34, 344–353. [Google Scholar] [CrossRef]
- Alsous, F.; Khamiees, M.; DeGirolamo, A.; Amoateng-Adjepong, Y.; Manthous, C.A. Negative fluid balance predicts survival in patients with septic shock: A retrospective pilot study. Chest 2000, 117, 1749–1754. [Google Scholar] [CrossRef]
- Murphy, C.V.; Schramm, G.E.; Doherty, J.A.; Reichley, R.M.; Gajic, O.; Afessa, B.; Micek, S.T.; Kollef, M.H. The importance of fluid management in acute lung injury secondary to septic shock. Chest 2009, 136, 102–109. [Google Scholar] [CrossRef]
- Cleymaet, R.; Scheinok, T.; Maes, H.; Stas, A.; Malbrain, L.; De Laet, I.; Schoonheydt, K.; Dits, H.; van Regenmortel, N.; Mekeirele, M.; et al. Prognostic value of bioelectrical impedance analysis for assessment of fluid overload in ICU patients: A pilot study. Anaesthesiol. Intensive Ther. 2021, 53, 10–17. [Google Scholar] [CrossRef]
- Malbrain, M.L.; Chiumello, D.; Cesana, B.M.; Reintam Blaser, A.; Starkopf, J.; Sugrue, M.; Pelosi, P.; Severgnini, P.; Hernandez, G.; Brienza, N.; et al. A systematic review and individual patient data meta-analysis on intra-abdominal hypertension in critically ill patients: The wake-up project. World initiative on Abdominal Hypertension Epidemiology, a Unifying Project (WAKE-Up!). Minerva Anestesiol. 2014, 80, 293–306. [Google Scholar]
- Malbrain, M.; Van Regenmortel, N.; Saugel, B.; De Tavernier, B.; Van Gaal, P.J.; Joannes-Boyau, O.; Teboul, J.L.; Rice, T.W.; Mythen, M.; Monnet, X. Principles of fluid management and stewardship in septic shock: It is time to consider the four D’s and the four phases of fluid therapy. Ann. Intensive Care 2018, 8, 66. [Google Scholar] [CrossRef] [PubMed]
- Malbrain, M.L.; Marik, P.E.; Witters, I.; Cordemans, C.; Kirkpatrick, A.W.; Roberts, D.J.; Van Regenmortel, N. Fluid overload, de-resuscitation, and outcomes in critically ill or injured patients: A systematic review with suggestions for clinical practice. Anaesthesiol. Intensive Ther. 2014, 46, 361–380. [Google Scholar] [CrossRef] [PubMed]
- Samoni, S.; Vigo, V.; Resendiz, L.I.; Villa, G.; De Rosa, S.; Nalesso, F.; Ferrari, F.; Meola, M.; Brendolan, A.; Malacarne, P.; et al. Impact of hyperhydration on the mortality risk in critically ill patients admitted in intensive care units: Comparison between bioelectrical impedance vector analysis and cumulative fluid balance recording. Crit. Care 2016, 20, 95. [Google Scholar] [CrossRef] [PubMed]
- Malbrain, M.; Martin, G.; Ostermann, M. Everything you need to know about deresuscitation. Intensive Care Med. 2022, 48, 1781–1786. [Google Scholar] [CrossRef] [PubMed]
- Jones, S.L.; Tanaka, A.; Eastwood, G.M.; Young, H.; Peck, L.; Bellomo, R.; Martensson, J. Bioelectrical impedance vector analysis in critically ill patients: A prospective, clinician-blinded investigation. Crit. Care 2015, 19, 290. [Google Scholar] [CrossRef] [PubMed]
- You, J.W.; Lee, S.J.; Kim, Y.E.; Cho, Y.J.; Jeong, Y.Y.; Kim, H.C.; Lee, J.D.; Kim, J.R.; Hwang, Y.S. Association between weight change and clinical outcomes in critically ill patients. J. Crit. Care 2013, 28, 923–927. [Google Scholar] [CrossRef] [PubMed]
- Schneider, A.G.; Baldwin, I.; Freitag, E.; Glassford, N.; Bellomo, R. Estimation of fluid status changes in critically ill patients: Fluid balance chart or electronic bed weight? J. Crit. Care 2012, 27, 745.e7–745.e12. [Google Scholar] [CrossRef] [PubMed]
- Koster, M.; Dennhardt, S.; Juttner, F.; Hopf, H.B. Cumulative changes in weight but not fluid volume balances reflect fluid accumulation in ICU patients. Acta Anaesthesiol. Scand. 2017, 61, 205–215. [Google Scholar] [CrossRef]
- Eastwood, G.M. Evaluating the reliability of recorded fluid balance to approximate body weight change in patients undergoing cardiac surgery. Heart Lung 2006, 35, 27–33. [Google Scholar] [CrossRef]
- Mulasi, U.; Kuchnia, A.J.; Cole, A.J.; Earthman, C.P. Bioimpedance at the bedside: Current applications, limitations, and opportunities. Nutr. Clin. Pract. 2015, 30, 180–193. [Google Scholar] [CrossRef]
- Madsen, J.M.; Wichmann, S.; Bestle, M.H.; Itenov, T.S. Bioimpedance as a measure of fluid status in critically ill patients: A systematic review. Acta Anaesthesiol. Scand. 2021, 65, 1155–1167. [Google Scholar] [CrossRef]
- Jacobs, D.O. Use of bioelectrical impedance analysis measurements in the clinical management of critical illness. Am. J. Clin. Nutr. 1996, 64 (Suppl. S3), 498S–502S. [Google Scholar] [CrossRef]
- Frankenfield, D.C.; Cooney, R.N.; Smith, J.S.; Rowe, W.A. Bioelectrical impedance plethysmographic analysis of body composition in critically injured and healthy subjects. Am. J. Clin. Nutr. 1999, 69, 426–431. [Google Scholar] [CrossRef] [PubMed]
- Moonen, H.; Van Zanten, A.R.H. Bioelectric impedance analysis for body composition measurement and other potential clinical applications in critical illness. Curr. Opin. Crit. Care 2021, 27, 344–353. [Google Scholar] [CrossRef] [PubMed]
- Khalil, S.F.; Mohktar, M.S.; Ibrahim, F. The theory and fundamentals of bioimpedance analysis in clinical status monitoring and diagnosis of diseases. Sensors 2014, 14, 10895–10928. [Google Scholar] [CrossRef] [PubMed]
- Gijsen, M.; Simons, E.; De Cock, P.; Malbrain, L.N.G.M.; Wauters, J.; Spriet, I. Reproducibility of fluid status measured by bioelectrical impedance analysis in healthy volunteers: A key requirement to monitor fluid status in the intensive care unit. Anaesthesiol. Intensive Ther. 2021, 53, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Moonen, H.P.; Bos, A.E.; Hermans, A.J.; Stikkelman, E.; van Zanten, F.J.; van Zanten, A.R. Bioelectric impedance body composition and phase angle in relation to 90-day adverse outcome in hospitalized COVID-19 ward and ICU patients: The prospective BIAC-19 study. Clin. Nutr. ESPEN 2021, 46, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, L.H.; van de Kerkhof, J.J.; Mingels, A.M.; Passos, V.L.; Kleijnen, V.W.; Mazairac, A.H.; van der Sande, F.M.; Wodzig, W.K.; Konings, C.J.; Leunissen, K.M.; et al. Inflammation, overhydration and cardiac biomarkers in haemodialysis patients: A longitudinal study. Nephrol. Dial. Transpl. 2010, 25, 243–248. [Google Scholar] [CrossRef]
- Di Somma, S.; Gori, C.S.; Grandi, T.; Risicato, M.G.; Salvatori, E. Fluid assessment and management in the emergency department. Contrib. Nephrol. 2010, 164, 227–236. [Google Scholar] [CrossRef]
- Cordemans, C.; De Laet, I.; Van Regenmortel, N.; Schoonheydt, K.; Dits, H.; Huber, W.; Malbrain, M.L. Fluid management in critically ill patients: The role of extravascular lung water, abdominal hypertension, capillary leak, and fluid balance. Ann. Intensive Care 2012, 2, S1. [Google Scholar] [CrossRef]
- Dabrowski, W.; Kotlinska-Hasiec, E.; Schneditz, D.; Zaluska, W.; Rzecki, Z.; De Keulenaer, B.; Malbrain, M.L. Continuous veno-venous hemofiltration to adjust fluid volume excess in septic shock patients reduces intra-abdominal pressure. Clin. Nephrol. 2014, 82, 41–50. [Google Scholar] [CrossRef]
- Malbrain, M.L.; Huygh, J.; Dabrowski, W.; De Waele, J.J.; Staelens, A.; Wauters, J. The use of bio-electrical impedance analysis (BIA) to guide fluid management, resuscitation and deresuscitation in critically ill patients: A bench-to-bedside review. Anaesthesiol. Intensive Ther. 2014, 46, 381–391. [Google Scholar] [CrossRef]
- Myatchin, I.; Abraham, P.; Malbrain, M. Bio-electrical impedance analysis in critically ill patients: Are we ready for prime time? J. Clin. Monit. Comput. 2019, 34, 401–410. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.; Kwon, O.; Shin, C.S.; Lee, S.M. Use of bioelectrical impedance analysis for the assessment of nutritional status in critically ill patients. Clin. Nutr. Res. 2015, 4, 32–40. [Google Scholar] [CrossRef] [PubMed]
- Yao, J.; Zhou, M.; Xu, B.; Li, C.; Chen, H.; Gong, D. The association of bioimpedance analysis parameters with the outcomes of critically ill patients. Clin. Nutr. 2020, 39, 2848–2855. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.H.; Lee, J.D.; Kang, D.R.; Hong, J.; Lee, J.M. Bioelectrical impedance analysis values as markers to predict severity in critically ill patients. J. Crit. Care 2017, 40, 103–107. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.H.; Wang, C.H.; Huang, Y.Y.; Tung, T.H.; Lee, C.M.; Yang, N.I.; Liu, P.C.; Cherng, W.J. Edema index established by a segmental multifrequency bioelectrical impedance analysis provides prognostic value in acute heart failure. J. Cardiovasc. Med. 2012, 13, 299–306. [Google Scholar] [CrossRef]
- Fan, S.; Sayed, R.H.; Davenport, A. Extracellular volume expansion in peritoneal dialysis patients. Int. J. Artif. Organs 2012, 35, 338–345. [Google Scholar] [CrossRef]
- Schuller, D.; Mitchell, J.P.; Calandrino, F.S.; Schuster, D.P. Fluid balance during pulmonary edema. Fluid balance during pulmonary edema. Is fluid gain a marker or a cause of poor outcome? Chest 1991, 100, 1068–1075. [Google Scholar] [CrossRef]
- Razzera, E.L.; Marcadenti, A.; Rovedder, S.W.; Alves, F.D.; Fink, J.D.S.; Silva, F.M. Parameters of Bioelectrical Impedance Are Good Predictors of Nutrition Risk, Length of Stay, and Mortality in Critically Ill Patients: A Prospective Cohort Study. JPEN J. Parenter. Enter. Nutr. 2020, 44, 849–854. [Google Scholar] [CrossRef]
- Garlini, L.M.; Alves, F.D.; Ceretta, L.B.; Perry, I.S.; Souza, G.C.; Clausell, N.O. Phase angle and mortality: A systematic review. Eur. J. Clin. Nutr. 2019, 73, 495–508. [Google Scholar] [CrossRef]
- Moonen, H.; van Zanten, F.J.L.; Driessen, L.; de Smet, V.; Slingerland-Boot, R.; Mensink, M.; van Zanten, A.R.H. Association of bioelectric impedance analysis body composition and disease severity in COVID-19 hospital ward and ICU patients: The BIAC-19 study. Clin. Nutr. 2021, 40, 2328–2336. [Google Scholar] [CrossRef]
- Santos, M.D.-D.L. Correlación entre índices de bioimpedancia eléctrica y score Apache II en pacientes con shock séptico. Rev. Medica Hered. 2011, 21, 111–117. [Google Scholar] [CrossRef]
- Thibault, R.; Makhlouf, A.M.; Mulliez, A.; Cristina Gonzalez, M.; Kekstas, G.; Kozjek, N.R.; Preiser, J.C.; Rozalen, I.C.; Dadet, S.; Krznaric, Z.; et al. Fat-free mass at admission predicts 28-day mortality in intensive care unit patients: The international prospective observational study Phase Angle Project. Intensive Care Med. 2016, 42, 1445–1453. [Google Scholar] [CrossRef]
- Vaara, S.T.; Korhonen, A.M.; Kaukonen, K.M.; Nisula, S.; Inkinen, O.; Hoppu, S.; Laurila, J.J.; Mildh, L.; Reinikainen, M.; Lund, V.; et al. Fluid overload is associated with an increased risk for 90-day mortality in critically ill patients with renal replacement therapy: Data from the prospective FINNAKI study. Crit. Care 2012, 16, R197. [Google Scholar] [CrossRef]
- Malbrain, M.L. Different techniques to measure intra-abdominal pressure (IAP): Time for a critical re-appraisal. Intensive Care Med. 2004, 30, 357–371. [Google Scholar] [CrossRef]
- Pereira, B.M. Abdominal compartment syndrome and intra-abdominal hypertension. Curr. Opin. Crit. Care 2019, 25, 688–696. [Google Scholar] [CrossRef]
- Jacobs, R.; Wise, R.D.; Myatchin, I.; Vanhonacker, D.; Minini, A.; Mekeirele, M.; Kirkpatrick, A.W.; Pereira, B.M.; Sugrue, M.; De Keulenaer, B.; et al. Fluid Management, Intra-Abdominal Hypertension and the Abdominal Compartment Syndrome: A Narrative Review. Life 2022, 12, 1390. [Google Scholar] [CrossRef]
- Le Gall, J.R.; Lemeshow, S.; Saulnier, F. A new Simplified Acute Physiology Score (SAPS II) based on a European/North American multicenter study. JAMA 1993, 270, 2957–2963. [Google Scholar] [CrossRef]
- Dabrowski, W.; Kotlinska-Hasiec, E.; Jaroszynski, A.; Zadora, P.; Pilat, J.; Rzecki, Z.; Zaluska, W.; Schneditz, D. Intra-abdominal pressure correlates with extracellular water content. PLoS ONE 2015, 10, e0122193. [Google Scholar] [CrossRef]
- Yang, E.M.; Park, E.; Ahn, Y.H.; Choi, H.J.; Kang, H.G.; Cheong, H.I.; Ha, I.S. Measurement of Fluid Status Using Bioimpedance Methods in Korean Pediatric Patients on Hemodialysis. J. Korean Med. Sci. 2017, 32, 1828–1834. [Google Scholar] [CrossRef]
- Madsen, J.M.; Itenov, T.S.; Koch, E.B.; Bestle, M.H. Bioimpedance as a measure of fluids in patients with septic shock. A prospective observational study. Acta Anaesthesiol. Scand. 2023, 67, 319–328. [Google Scholar] [CrossRef]
- Koch, E.B.; Madsen, J.M.; Wichmann, S.; Bestle, M.H.; Itenov, T.S. Bioimpedance and Duration of Organ Dysfunction in Septic Shock-A Prospective Observational Study. J. Intensive Care Med. 2023, 38, 966–974. [Google Scholar] [CrossRef]
- O’Brien, C.; Young, A.J.; Sawka, M.N. Bioelectrical impedance to estimate changes in hydration status. Int. J. Sports Med. 2002, 23, 361–366. [Google Scholar] [CrossRef]
- Ritz, P.; Vol, S.; Berrut, G.; Tack, I.; Arnaud, M.J.; Tichet, J. Influence of gender and body composition on hydration and body water spaces. Clin. Nutr. 2008, 27, 740–746. [Google Scholar] [CrossRef]
- Malczyk, E.; Dziegielewska-Gesiak, S.; Fatyga, E.; Ziolko, E.; Kokot, T.; Muc-Wierzgon, M. Body composition in healthy older persons: Role of the ratio of extracellular/total body water. J. Biol. Regul. Homeost. Agents 2016, 30, 767–772. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Female | Male | |||||
|---|---|---|---|---|---|---|
| Variable | Healthy Volunteers (n = 68) | ICU Patients (n = 35) | p-Value | Healthy Volunteers (n = 33) | ICU Patients (n = 66) | p-Value |
| Patient demographics | ||||||
| Height (cm) | 169.3 ± 8.1 | 163.7 ± 5.5 | <0.001 | 181.0 ± 6.6 | 175.5 ± 8.3 | <0.001 |
| Weight (kg) | 67.4 ± 12.4 | 77.4 ± 20.4 | 0.005 | 83.1 ± 14.3 | 84.0 ± 20.4 | NS |
| BMI (kg m−2) | 23.4 ± 3.3 | 28.9 ± 7.3 | <0.001 | 25.3 ± 4.0 | 27.3 ± 6.7 | NS |
| Age (years) | 37.6 ± 12.6 | 60.3 ± 16.9 | <0.001 | 38.9 ± 12.5 | 65.2 ± 14.8 | <0.001 |
| Raw BIA values at 50 kHz | ||||||
| Impedance (Ohm) | 586.8 ± 105.3 | 404.7 ± 113.7 | <0.001 | 506.9 ± 62.6 | 381.7 ± 96.4 | <0.001 |
| Phase angle | 9.3 ± 1.5 | 7.9 ± 1.5 | <0.001 | 9.5 ± 1.0 | 8.6 ± 3.8 | 0.038 |
| Resistance (Ohm) | 579.5 ± 104.2 | 401.3 ± 112.8 | <0.001 | 500.5 ± 61.6 | 377.3 ± 96.1 | <0.001 |
| Reactance (Ohm) | 94.2 ± 20.6 | 55.1 ± 17.9 | <0.001 | 83.6 ± 14.2 | 56.4 ± 24.7 | <0.001 |
| Capacitance (Ohm) | 35.7 ± 11.3 | 63.6 ± 20.4 | <0.001 | 39.0 + 5.0 | 65.4 ± 25.2 | <0.001 |
| Female | Male | |||||
|---|---|---|---|---|---|---|
| Variable | Healthy Volunteers (n = 68) | ICU Patients (n = 35) | p-Value | Healthy Volunteers (n = 33) | ICU Patients (n = 66) | p-Value |
| Body fluid composition | ||||||
| Dry Weight (kg) | 67.8 ± 13.4 | 72.4 ± 18.7 | NS | 83.1 ± 14.3 | 78.1 ± 18.9 | NS |
| Volume excess (L) | −0.2 ± 0.7 | 5.0 ± 5.2 | <0.001 | −0.0 ± 1.0 | 5.9 ± 6.6 | <0.001 |
| Fluid Overload (%) | 0.0 ± 0.1 | 6.2 ± 5.8 | <0.001 | 0.0 ± 0.1 | 6.9 ± 7.0 | <0.001 |
| TBW (L) | 35.0 ± 6.7 | 40.2 ± 8.6 | 0.003 | 45.7 ± 5.0 | 49.6 ± 10.3 | 0.013 |
| TBW (%) | 52.0 ± 5.5 | 53.1 ± 9.2 | NS | 55.7 ± 5.7 | 60.2 ± 9.3 | 0.002 |
| ECW (L) | 15.2 ± 3.7 | 20.5 ± 5.7 | <0.001 | 19.8 ± 2.5 | 24.6 ±7.0 | <0.001 |
| ECW (%) | 43.2 ± 2.7 | 50.6 ± 4.3 | <0.001 | 43.2 ± 1.7 | 49.1 ± 4.8 | <0.001 |
| ICW (L) | 19.8 ± 3.4 | 19.7 ± 3.6 | NS | 25.9 ± 2.8 | 25.0 ± 4.2 | NS |
| ICW (%) | 56.8 ± 2.7 | 49.4 ± 4.3 | <0.001 | 56.8 ± 1.7 | 50.9 ± 4.8 | <0.001 |
| ECW/ICW | 0.8 ± 0.1 | 1.0 ± 0.2 | <0.001 | 0.8 ± 0.1 | 1.0 ± 0.2 | <0.001 |
| ECS (L) | 5.2 ± 0.9 | 4.8 ± 0.8 | NS | 6.8 ± 0.7 | 6.3 ± 1.0 | 0,006 |
| ECF (L) | 15.8 ± 3.8 | 21.4 ± 5.9 | <0.001 | 20.6 ± 2.6 | 25.6 ± 7.3 | <0.001 |
| Plasma Fluid (L) | 3.0 ± 0.8 | 4.0 ± 1.2 | <0.001 | 4.0 ± 0.6 | 4.7 ± 1.4 | 0.001 |
| Interstitial Fluid (L) | 11.3 ± 2.7 | 15.3 ± 4.2 | <0.001 | 14.5 ± 1.8 | 18.5 ± 5.3 | <0.001 |
| FFMH (%) | 72.7 ± 2.4 | 79.0 ± 4.3 | <0.001 | 72.5 ± 2.1 | 78.1 ± 4.3 | <0.001 |
| Body Density (Kg/L) | 1.04 ± 0.01 | 1.03 ± 0.02 | 0.026 | 1.05 ± 0.02 | 1.05 ± 0.02 | NS |
| Female | Male | |||||
|---|---|---|---|---|---|---|
| Variable | Healthy Volunteers (n = 68) | ICU Patients (n = 35) | p-Value | Healthy Volunteers (n = 33) | ICU Patients (n = 66) | p-Value |
| Nutritional Status | ||||||
| Phase angle | 9.3 ± 1.5 | 7.9 ± 1.5 | <0.001 | 9.5 ± 1.0 | 8.6 ± 3.8 | 0.038 |
| Malnutrition Index | 0.73 ± 0.12 | 0.89 ± 0.14 | <0.001 | 0.77 ± 0.08 | 0.90 ± 0.18 | <0.001 |
| RMR (kcal) | 1571.2 ± 205.9 | 1445.8 ± 186.4 | 0.003 | 1971.5 ± 202.2 | 1753.0 ± 282.4 | <0.001 |
| FFM (kg) | 48.1 ± 8.5 | 50.6 ± 9.0 | NS | 63.0 ± 6.3 | 63.4 ± 11.3 | NS |
| FFM (%) | 71.5 ± 6.5 | 67.1 ± 10.2 | 0.025 | 76.8 ± 7.4 | 76.8 ± 8.9 | NS |
| Fat (kg) | 19.8 ± 7.4 | 26.8 ± 15.4 | 0.014 | 20.1 ± 10.5 | 20.6 ± 12.2 | NS |
| Fat (%) | 28.5 ± 6.5 | 32.9 ± 10.2 | 0.025 | 23.2 ± 7.4 | 23.1 ± 8.9 | NS |
| BCM (kg) | 28.0 ± 5.1 | 26.9 ± 5.5 | NS | 35.6 ± 4.0 | 33.5 ± 6.0 | 0.035 |
| ECM (kg) | 20.1 ± 4.4 | 23.7 ± 4.7 | <0.001 | 27.4 ± 3.1 | 29.9 ± 6.9 | 0.014 |
| Protein (kg) | 11.2 ± 2.0 | 10.9 ± 2.1 | NS | 14.4 ± 1.5 | 13.4 ± 2.4 | 0.013 |
| Mineral (kg) | 4.4 ± 0.6 | 4.3 ± 0.9 | NS | 5.0 ± 0.5 | 4.7 ± 0.8 | 0.014 |
| Muscle (kg) | 24.6 ± 5.2 | 22.8 ± 5.1 | NS | 33.0 ± 3.5 | 30.0 ± 5.5 | 0.001 |
| TBK (g) | 124.1 ± 25.0 | 116.2 ± 22.9 | NS | 169.1 ± 17.7 | 154.7 ± 26.7 | 0.006 |
| TBCa (g) | 1020.5 ± 180.6 | 963.6 ± 165.4 | NS | 1346.0 ± 128.2 | 1241.9 ± 192.9 | 0.006 |
| Glycogen (g) | 468.5 ± 82.3 | 442.7 ± 87.2 | NS | 599.8 ± 63.0 | 545.1 ± 94.1 | 0.003 |
| Variable | Total | Alive (n = 61) | Died (n = 40) | p-Value |
|---|---|---|---|---|
| Patient demographics | ||||
| Male/female | 2/1 | 2/1 | 2/1 | NS |
| Hospital stay (days) | 51.9 ± 47.5 | 65.5 ± 53.3 | 31 ± 26.2 | <0.001 |
| ICU stay (days) | 31.2 ± 26.7 | 34.6 ± 28.8 | 26 ± 22.4 | NS |
| Day measurement | 4.8 ± 2.1 | 5 ± 2.1 | 4.6 ± 2.2 | NS |
| Height (cm) | 171.4 ± 9.4 | 172.1 ± 9.3 | 170.4 ± 9.5 | NS |
| Weight (kg) | 81.7 ± 20.6 | 82.9 ± 21.9 | 79.9 ± 18.6 | NS |
| BMI (kg/m2) | 27.8 ± 6.9 | 28 ± 7.1 | 27.6 ± 6.7 | NS |
| Age (years) | 63.5 ± 15.7 | 60.1 ± 16.6 | 68.7 ± 12.7 | 0.007 |
| APACHE | 23.3 ± 9.1 | 21 ± 8.7 | 26.8 ± 8.6 | 0.001 |
| SAPS | 55.5 ± 18.9 | 49.1 ± 16.8 | 65 ± 17.9 | <0.001 |
| SOFA | 9.8 ± 4.1 | 8.7 ± 3.2 | 11.4 ± 4.7 | 0.001 |
| IAP (mmHg) | 13.2 ± 3.9 | 12.5 ± 3.8 | 14.1 ± 4 | 0.065 |
| EVLWI (mL/kgPBW) | 10.6 ± 3.2 | 10.4 ± 2.7 | 10.8 ± 3.8 | NS |
| Laboratory results | ||||
| Hematocrit (%) | 28.9 ± 5.8 | 29.2 ± 5.8 | 28.4 ± 5.9 | NS |
| Total protein (g/L) | 49.6 ± 8.4 | 48.7 ± 8.6 | 51 ± 8.1 | NS |
| Albumin (g/L) | 24.5 ± 5.2 | 24.7 ± 6.2 | 24.2 ± 3.5 | NS |
| CRP (mg/dL) | 164.2 ± 113.6 | 169.4 ± 114.4 | 156.5 ± 113.5 | NS |
| Urea (mg/DL) | 69.6 ± 45.9 | 62.8 ± 43.8 | 79.5 ± 47.5 | 0.075 |
| Osmol (measured) | 298 ± 18 | 297.3 ± 19.8 | 299.3 ± 14.7 | NS |
| Osmol (calculated) | 314.4 ± 40.4 | 309.2 ± 48 | 322.1 ± 23.4 | NS |
| Glucose (mg/dL) | 142.8 ± 52.2 | 142.4 ± 52.2 | 143.4 ± 52.9 | NS |
| Na (mmol/L) | 142.4 ± 8 | 142.1 ± 8.8 | 142.9 ± 6.7 | NS |
| K (mmol/L) | 4.2 ± 0.6 | 4.2 ± 0.6 | 4.1 ± 0.6 | NS |
| Creatine (mg/dL) | 1.3 ± 1 | 1.1 ± 0.6 | 1.8 ± 1.2 | <0.001 |
| CCR (mL/min) | 99.5 ± 48.8 | 113.4 ± 48.3 | 78.3 ± 41.7 | <0.001 |
| GFR (mL/min) | 82.6 ± 45.4 | 95.1 ± 44.8 | 63.6 ± 39.7 | <0.001 |
| Raw BIA values at 50 kHz | ||||
| Impedance (Ohm) | 389.7 ± 102.8 | 401 ± 99 | 372.4 ± 107.1 | NS |
| Phase angle | 8.3 ± 3.2 | 8.7 ± 3.8 | 7.8 ± 2.2 | NS |
| Resistance (Ohm) | 385.6 ± 102.2 | 396.4 ± 99.1 | 369.3 ± 106.1 | NS |
| Reactance (Ohm) | 55.9 ± 22.5 | 59.7 ± 23.8 | 50.2 ± 19.4 | 0.039 |
| Capacitance (Ohm) | 64.8 ± 23.5 | 60 ± 20.9 | 72.1 ± 25.6 | 0.010 |
| Variable | Total | Alive (n = 61) | Died (n = 40) | p-Value |
|---|---|---|---|---|
| Body fluid composition | ||||
| Dry Weight (kg) | 76.1 ± 19 | 77.9 ± 18.9 | 73.4 ± 19 | NS |
| Cumulative FB (L) | 7.1 ± 6.2 | 7 ± 6.1 | 7.2 ± 6.5 | NS |
| Volume excess (L) | 5.6 ± 6.1 | 5 ± 6.4 | 6.5 ± 5.7 | NS |
| Fluid Overload (%) | 6.7 ± 6.6 | 5.5 ± 5.5 | 8.4 ± 7.6 | 0.033 |
| TBW (L) | 46.3 ± 10.7 | 46.6 ± 11.3 | 46 ± 9.8 | NS |
| TBW (%) | 57.8 ± 9.8 | 57.2 ± 9.5 | 58.6 ± 10.3 | NS |
| ECW (L) | 23.2 ± 6.8 | 23 ± 7.3 | 23.5 ± 6.1 | NS |
| ECW (%) | 49.6 ± 4.7 | 48.9 ± 4.3 | 50.7 ± 5.1 | 0.047 |
| ICW (L) | 23.1 ± 4.8 | 23.6 ± 4.8 | 22.5 ± 4.7 | NS |
| ICW (%) | 50.4 ± 4.7 | 51.1 ± 4.3 | 49.2 ± 5.1 | 0.047 |
| ECW/ICW | 1 ± 0.2 | 0.97 ± 0.19 | 1.05 ± 0.22 | 0.049 |
| ECS (L) | 5.8 ± 1.2 | 5.9 ± 1.2 | 5.6 ± 1.1 | NS |
| ECF (L) | 24.1 ± 7.1 | 23.9 ± 7.6 | 24.4 ± 6.3 | NS |
| Plasma Fluid (L) | 4.5 ± 1.4 | 4.5 ± 1.5 | 4.5 ± 1.1 | NS |
| Interstitial Fluid (L) | 17.4 ± 5.2 | 17.1 ± 5.4 | 17.7 ± 4.9 | NS |
| FFMH (%) | 78.4 ± 4.3 | 78 ± 4 | 79 ± 4.7 | NS |
| Body Density (kg/L) | 1.039 ± 0.023 | 1.039 ± 0.023 | 1.04 ± 0.022 | NS |
| Nutritional status | ||||
| Phase angle | 8.3 ± 3.2 | 8.7 ± 3.8 | 7.8 ± 2.2 | NS |
| Malnutrition Index | 0.9 ± 0.16 | 0.87 ± 0.16 | 0.94 ± 0.17 | 0.048 |
| RMR (kcal) | 1646.5 ± 291.9 | 1680.1 ± 306.5 | 1595.3 ± 263.6 | NS |
| FFM (kg) | 58.9 ± 12.2 | 59.5 ± 12.7 | 58.1 ± 11.3 | NS |
| FFM (%) | 73.5 ± 10.4 | 73.2 ± 10.6 | 73.9 ± 10.2 | NS |
| Fat (kg) | 22.8 ± 13.7 | 23.4 ± 14.6 | 21.8 ± 12.1 | NS |
| Fat (%) | 26.5 ± 10.4 | 26.8 ± 10.6 | 26.2 ± 10.2 | NS |
| BCM (kg) | 31.2 ± 6.6 | 31.8 ± 6.4 | 30.2 ± 6.9 | NS |
| ECM (kg) | 27.7 ± 6.8 | 27.7 ± 7.5 | 27.9 ± 5.8 | NS |
| Protein (kg) | 12.5 ± 2.6 | 12.8 ± 2.6 | 12.1 ± 2.6 | NS |
| Mineral (kg) | 4.6 ± 0.9 | 4.7 ± 0.9 | 4.4 ± 0.8 | NS |
| Muscle (kg) | 27.5 ± 6.3 | 28.1 ± 6.3 | 26.5 ± 6.2 | NS |
| TBK (g) | 141.4 ± 31.3 | 145 ± 32.1 | 135.9 ± 29.5 | NS |
| TBCa (g) | 1145.4 ± 226.3 | 1171.4 ± 232.4 | 1105.9 ± 213.4 | NS |
| Glycogen (g) | 509.6 ± 103.6 | 523.6 ± 106.4 | 488.2 ± 96.7 | 0.092 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cleymaet, R.; D’Hondt, M.; Scheinok, T.; Malbrain, L.; De Laet, I.; Schoonheydt, K.; Dits, H.; Van Regenmortel, N.; Mekeirele, M.; Cordemans, C.; et al. Comparison of Bioelectrical Impedance Analysis (BIA)-Derived Parameters in Healthy Volunteers and Critically Ill Patients. Life 2024, 14, 27. https://doi.org/10.3390/life14010027
Cleymaet R, D’Hondt M, Scheinok T, Malbrain L, De Laet I, Schoonheydt K, Dits H, Van Regenmortel N, Mekeirele M, Cordemans C, et al. Comparison of Bioelectrical Impedance Analysis (BIA)-Derived Parameters in Healthy Volunteers and Critically Ill Patients. Life. 2024; 14(1):27. https://doi.org/10.3390/life14010027
Chicago/Turabian StyleCleymaet, Robbert, Marvin D’Hondt, Thomas Scheinok, Luca Malbrain, Inneke De Laet, Karen Schoonheydt, Hilde Dits, Niels Van Regenmortel, Michael Mekeirele, Colin Cordemans, and et al. 2024. "Comparison of Bioelectrical Impedance Analysis (BIA)-Derived Parameters in Healthy Volunteers and Critically Ill Patients" Life 14, no. 1: 27. https://doi.org/10.3390/life14010027
APA StyleCleymaet, R., D’Hondt, M., Scheinok, T., Malbrain, L., De Laet, I., Schoonheydt, K., Dits, H., Van Regenmortel, N., Mekeirele, M., Cordemans, C., Minini, A., Severgnini, P., Dabrowski, W., Wong, A., & Malbrain, M. L. N. G. (2024). Comparison of Bioelectrical Impedance Analysis (BIA)-Derived Parameters in Healthy Volunteers and Critically Ill Patients. Life, 14(1), 27. https://doi.org/10.3390/life14010027