The Assessment of Myocardial Strain by Cardiac Imaging in Healthy Infants with Acute Bronchiolitis: A Systematic Review and Meta-Analysis

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Selection Criteria
2.2.1. Inclusion Criteria
- AB diagnosed following the recommendations of international guidelines [6].
- Age younger than 2-year-old. Children without CHD.
- Systematic echocardiography for screening of MD and PH.
2.2.2. Exclusion Criteria
- Adult or animal studies.
- Investigations of other diseases than AB.
- Presence of well-known risk factors for severe AB, such as CHD.
- Studies in which echocardiography was performed for clinical indications.
- Pilot studies, retrospective studies, multiple papers from the same study and not primary research (reviews, letters, guidelines, case reports, case series).
2.3. Data Extraction
2.4. Quality Assessment
2.5. Statistical Analysis
3. Results
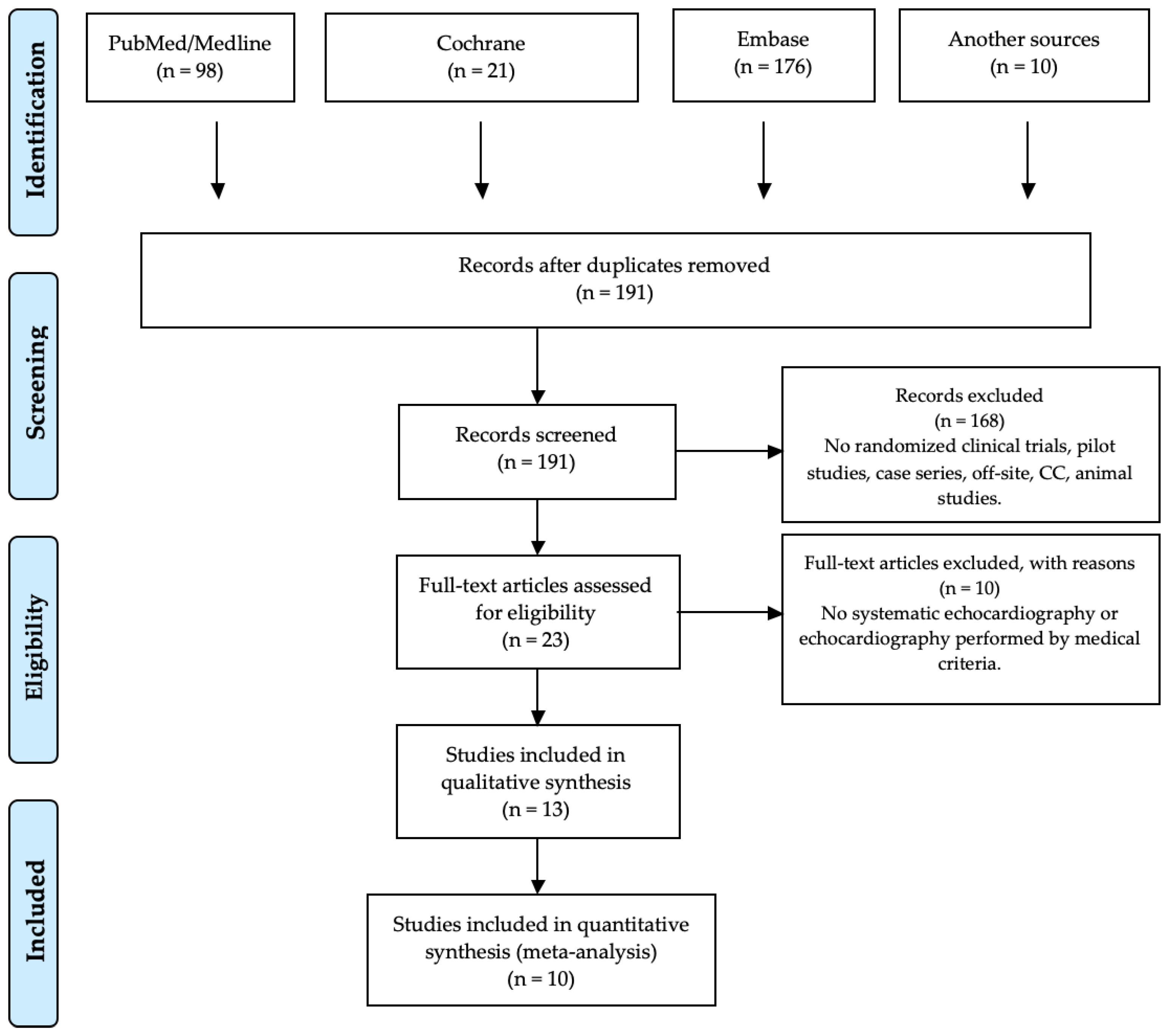
3.1. Eligible Studies
3.2. Quality Assessment of the Included Studies
3.3. Qualitative Analysis
3.3.1. Baseline Characteristics
3.3.2. Assessment of Myocardial Strain
Echocardiographic Timing and Techniques
Cardiac Biomarkers
3.3.3. Research Outcome and Incidence of Severe AB
3.4. Quantitative Analysis
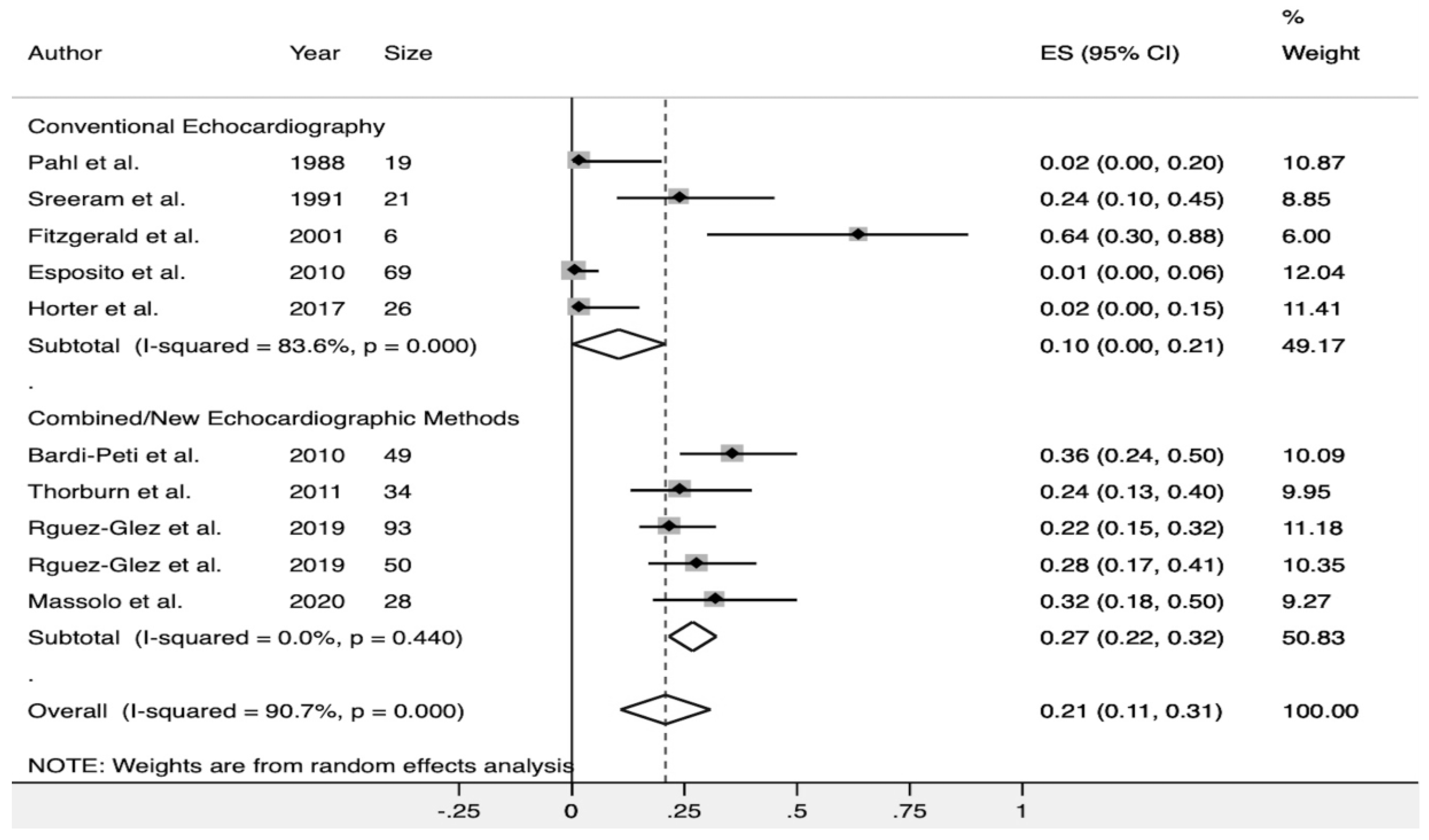
3.4.1. Incidence and Type of Myocardial Strain in AB
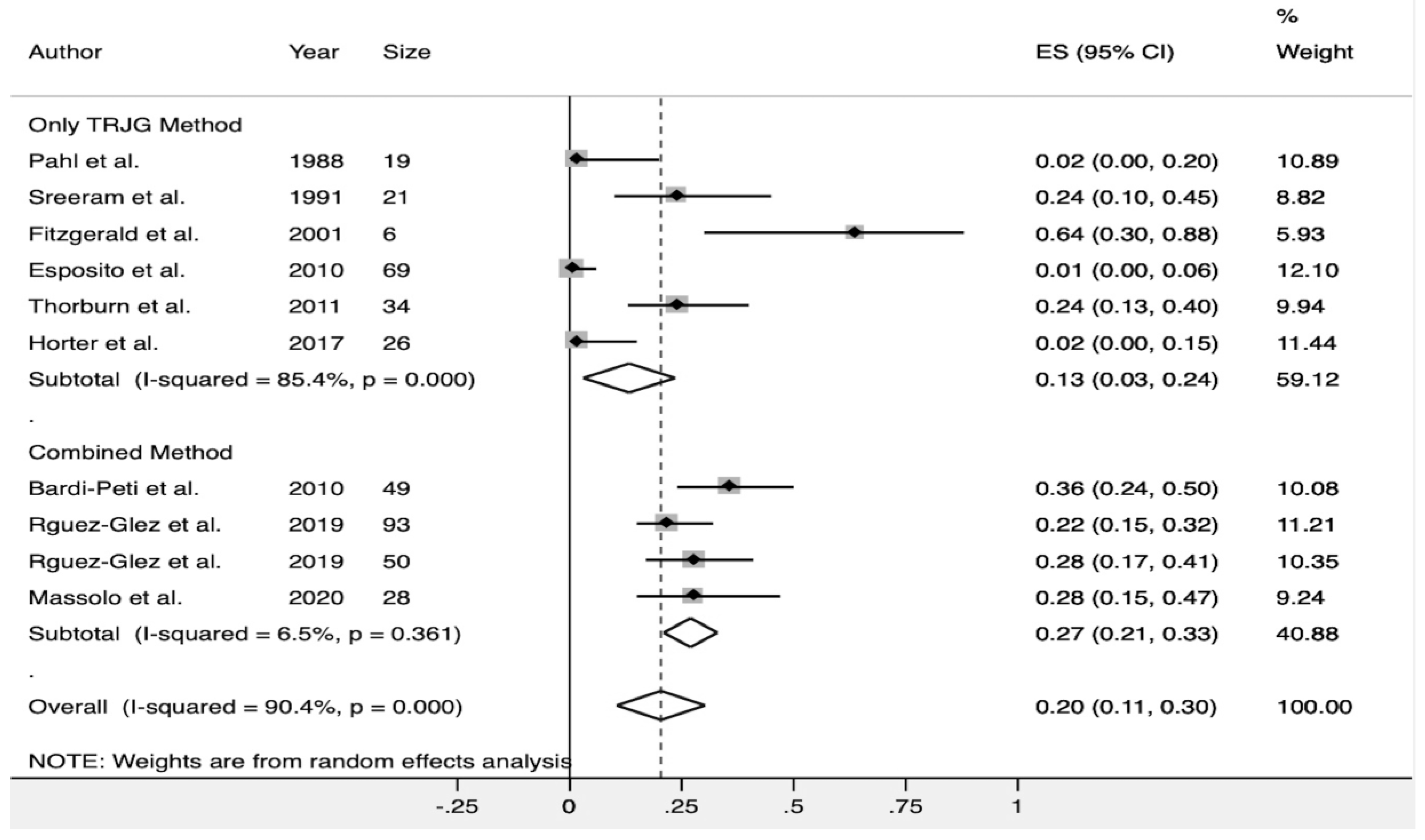
Incidence of Pulmonary Hypertension
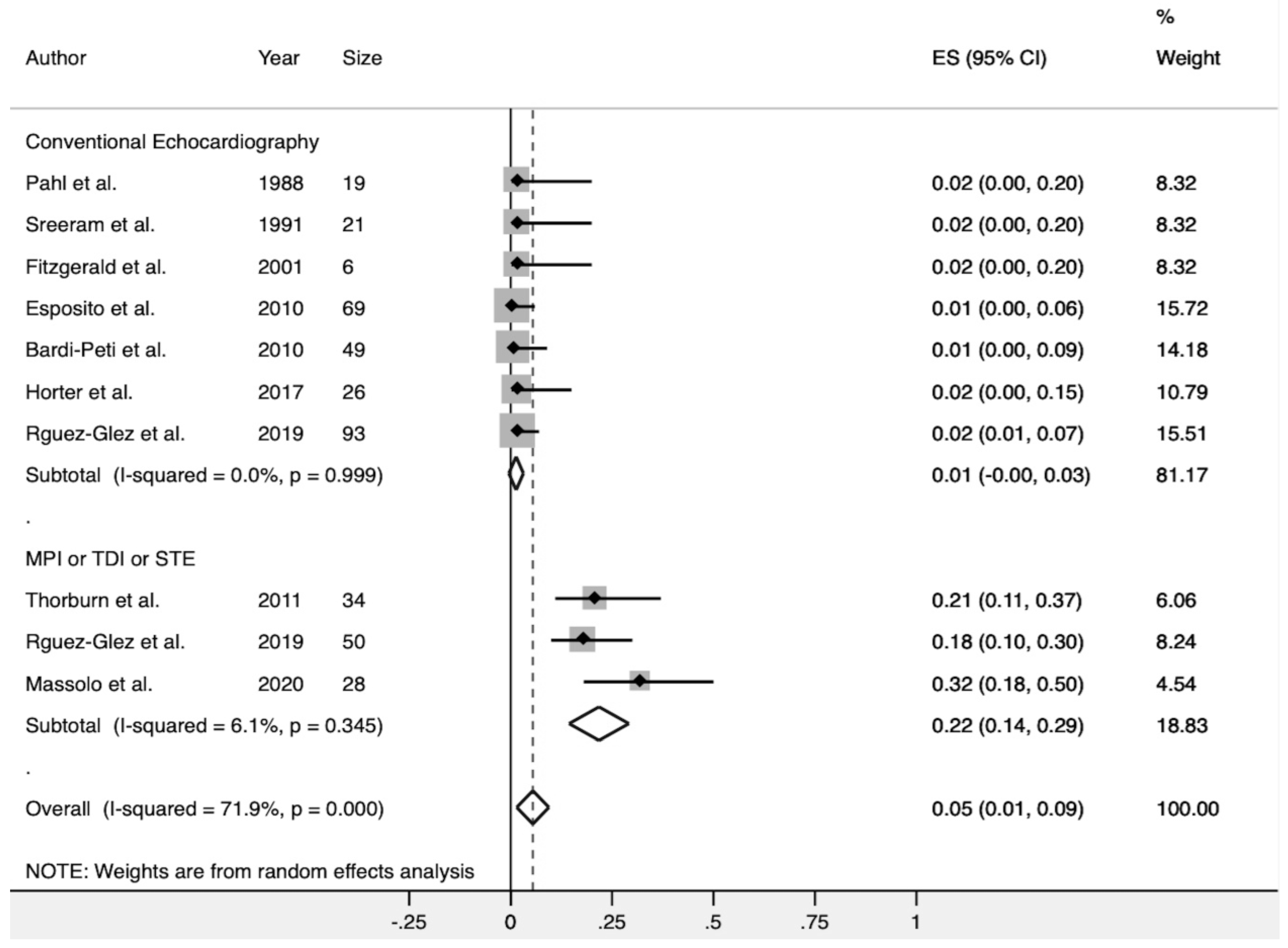
Myocardial Dysfunction
3.4.2. Association of Myocardial Strain and Severe AB
3.4.3. Sensitivity Analysis
4. Discussion
4.1. Analysis of the Studies that Did Not Detect Myocardial Strain in AB
4.2. Incidence of Myocardial Strain in AB
4.2.1. Pulmonary Hypertension
4.2.2. Myocardial Dysfunction
4.3. Myocardial Strain as a Predictor for Adverse Outcomes
4.4. Cardiac Biomarkers to Assess Myocardial Strain in AB
4.4.1. Cardiac Troponin
4.4.2. NT-ProBNP
4.5. Limitations
5. Conclusions and Future Perspectives
Author Contributions
Funding
Conflicts of Interest
References
- Bont, L.; Checchia, P.A.; Fauroux, B.; Figueras-Aloy, J.; Manzoni, P.; Paes, B.; Simões, E.A.F.; Carbonell-Estrany, X. Defining the Epidemiology and Burden of Severe Respiratory Syncytial Virus Infection Among Infants and Children in Western Countries. Infect. Dis. Ther. 2016, 5, 271–298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, D.K.; Seales, S.; Budzik, C. Respiratory Syncytial Virus Bronchiolitis in Children. Am. Fam. Physician 2017, 95, 94–99. [Google Scholar] [PubMed]
- Fauroux, B.; Simões, E.A.F.; Checchia, P.A.; Paes, B.; Figueras-Aloy, J.; Manzoni, P.; Bont, L.; Carbonell-Estrany, X. The Burden and Long-term Respiratory Morbidity Associated with Respiratory Syncytial Virus Infection in Early Childhood. Infect. Dis. Ther. 2017, 6, 173–197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, T.; McAllister, D.A.; O’Brien, K.L.; Simões, E.A.F.; Madhi, S.A.; Gessner, B.D.; Polack, F.P.; Balsells, E.; Acacio, S.; Aguayo, C.; et al. RSV Global Epidemiology Network Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in young children in 2015: A systematic review and modelling study. Lancet 2017, 390, 946–958. [Google Scholar] [CrossRef] [Green Version]
- Stein, R.T.; Bont, L.J.; Zar, H.; Polack, F.P.; Park, C.; Claxton, A.; Borok, G.; Butylkova, Y.; Wegzyn, C. Respiratory syncytial virus hospitalization and mortality: Systematic review and meta-analysis. Pediatr. Pulmonol. 2016, 52, 556–569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ralston, S.L.; Lieberthal, A.S.; Meissner, H.C.; Alverson, B.K.; Baley, J.E.; Gadomski, A.M.; Johnson, D.W.; Light, M.J.; Maraqa, N.F.; Mendonca, E.A.; et al. American Academy of Pediatrics Clinical practice guideline: The diagnosis, management, and prevention of bronchiolitis. Pediatrics 2014, 134, e1474–e1502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manzoni, P.; Figueras-Aloy, J.; Simões, E.A.F.; Checchia, P.A.; Fauroux, B.; Bont, L.; Paes, B.; Carbonell-Estrany, X. Defining the Incidence and Associated Morbidity and Mortality of Severe Respiratory Syncytial Virus Infection Among Children with Chronic Diseases. Infect. Dis. Ther. 2017, 6, 383–411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, T.; Balsells, E.; Wastnedge, E.; Singleton, R.; Rasmussen, Z.A.; Zar, H.J.; Rath, B.A.; Madhi, S.A.; Campbell, S.; Vaccari, L.C.; et al. Risk factors for respiratory syncytial virus associated with acute lower respiratory infection in children under five years: Systematic review and meta-analysis. J. Glob. Health 2015, 5, 020416. [Google Scholar] [CrossRef]
- Fernandes, R.M.; Plint, A.C.; Terwee, C.B.; Sampaio, C.; Klassen, T.P.; Offringa, M.; van der Lee, J.H. Validity of bronchiolitis outcome measures. Pediatrics 2015, 135, e1399–e1408. [Google Scholar] [CrossRef] [Green Version]
- Schaller, A.; Galloway, C.S. Bronchiolitis in Infants and Children. S D Med. 2017, 70, 274–277. [Google Scholar]
- Destino, L.; Weisgerber, M.C.; Soung, P.; Bakalarski, D.; Yan, K.; Rehborg, R.; Wagner, D.R.; Gorelick, M.H.; Simpson, P. Validity of respiratory scores in bronchiolitis. Hosp. Pediatr. 2012, 2, 202–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCallum, G.B.; Morris, P.S.; Wilson, C.C.; Versteegh, L.A.; Ward, L.M.; Chatfield, M.D.; Chang, A.B. Severity scoring systems: Are they internally valid, reliable and predictive of oxygen use in children with acute bronchiolitis? Pediatr. Pulmonol. 2013, 48, 797–803. [Google Scholar] [CrossRef] [PubMed]
- Rödl, S.; Resch, B.; Hofer, N.; Marschitz, I.; Madler, G.; Eber, E.; Zobel, G. Prospective evaluation of clinical scoring systems in infants with bronchiolitis admitted to the intensive care unit. Eur. J. Clin. Microbiol. Infect. Dis. 2012, 31, 2667–2672. [Google Scholar] [CrossRef] [PubMed]
- Tulloh, R.M.R.; Medrano-Lopez, C.; Checchia, P.A.; Stapper, C.; Sumitomo, N.; Gorenflo, M.; Jung Bae, E.; Juanico, A.; Gil-Jaurena, J.M.; Wu, M.-H.; et al. CHD and respiratory syncytial virus: Global expert exchange recommendations. Cardiol. Young 2017, 27, 1504–1521. [Google Scholar] [CrossRef]
- Checchia, P.A.; Paes, B.; Bont, L.; Manzoni, P.; Simões, E.A.F.; Fauroux, B.; Figueras-Aloy, J.; Carbonell-Estrany, X. Defining the Risk and Associated Morbidity and Mortality of Severe Respiratory Syncytial Virus Infection Among Infants with Congenital Heart Disease. Infect. Dis. Ther. 2017, 6, 37–56. [Google Scholar] [CrossRef] [Green Version]
- Willson, D.F.; Landrigan, C.P.; Horn, S.D.; Smout, R.J. Complications in infants hospitalized for bronchiolitis or respiratory syncytial virus pneumonia. J. Pediatr. 2003, 143, S142–S149. [Google Scholar] [CrossRef]
- Menchise, A. Myocarditis in the setting of RSV bronchiolitis. Fetal Pediatr. Pathol. 2011, 30, 64–68. [Google Scholar] [CrossRef]
- Fantacci, C.; Ferrara, P.; Franceschi, F.; Chiaretti, A. Pneumopericardium, pneumomediastinum, and pneumorrachis complicating acute respiratory syncytial virus bronchiolitis in children. Eur. Rev. Med. Pharm. Sci. 2017, 21, 3465–3468. [Google Scholar]
- Moynihan, J.A.; Brown, L.; Sehra, R.; Checchia, P.A. Cardiac troponin I as a predictor of respiratory failure in children hospitalized with respiratory syncytial virus (RSV) infections: A pilot study. Am. J. Emerg. Med. 2003, 21, 479–482. [Google Scholar] [CrossRef]
- Kim, K.K.; Frankel, L.R. The need for inotropic support in a subgroup of infants with severe life-threatening respiratory syncytial viral infection. J. Investig. Med. 1997, 45, 469–473. [Google Scholar]
- Pahl, E.; Gidding, S.S. Echocardiographic assessment of cardiac function during respiratory syncytial virus infection. Pediatrics 1988, 81, 830–834. [Google Scholar] [PubMed]
- Sreeram, N.; Watson, J.G.; Hunter, S. Cardiovascular effects of acute bronchiolitis. Acta. Paediatr. Scand. 1991, 80, 133–136. [Google Scholar] [CrossRef] [PubMed]
- Fitzgerald, D.; Davis, G.M.; Rohlicek, C.; Gottesman, R. Quantifying pulmonary hypertension in ventilated infants with bronchiolitis: A pilot study. J. Paediatr. Child. Health 2001, 37, 64–66. [Google Scholar] [CrossRef] [PubMed]
- Esposito, S.; Salice, P.; Bosis, S.; Ghiglia, S.; Tremolati, E.; Tagliabue, C.; Gualtieri, L.; Barbier, P.; Galeone, C.; Marchisio, P.; et al. Altered cardiac rhythm in infants with bronchiolitis and respiratory syncytial virus infection. Bmc Infect. Dis. 2010, 10, 305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bardi-Peti, L.; Ciofu, E.P. [Bronchiolitis and pulmonary hypertension]. Pneumologia 2010, 59, 95–100. [Google Scholar] [PubMed]
- Thorburn, K.; Eisenhut, M.; Shauq, A.; Narayanswamy, S.; Burgess, M. Right ventricular function in children with severe respiratory syncytial virus (RSV) bronchiolitis. Minerva Anestesiol. 2011, 77, 46–53. [Google Scholar] [PubMed]
- Horter, T.; Nakstad, B.; Ashtari, O.; Solevåg, A.L. Right and left ventricular function in hospitalized children with respiratory syncytial virus infection. Infect. Drug Resist. 2017, 10, 419–424. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez-Gonzalez, M.; Benavente Fernández, I.; Castellano-Martinez, A.; Lechuga-Sancho, A.M.; Lubián-López, S.P. NT-proBNP plasma levels as biomarkers for pulmonary hypertension in healthy infants with respiratory syncytial virus infection. Biomark. Med. 2019, 13, 605–618. [Google Scholar] [CrossRef]
- Rodriguez-Gonzalez, M.; Perez-Reviriego, A.A.; Castellano-Martinez, A.; Lubian-Lopez, S.; Benavente-Fernandez, I. Left Ventricular Dysfunction and Plasmatic NT-proBNP Are Associated with Adverse Evolution in Respiratory Syncytial Virus Bronchiolitis. Diagnostics 2019, 9, 85. [Google Scholar] [CrossRef] [Green Version]
- Claudia Massolo, A.; Vanina Cantone, G.; Maria Caterina Musolino, A.; Corsini, I.; Patel, N.; Evangelisti, M.; Monaco, F.; Pia Villa, M.; Braguglia, A. Myocardial strain on admission predicts disease severity in infants hospitalized for bronchiolitis. Pediatr. Pulmonol. 2020, 69, 2607–2609. [Google Scholar] [CrossRef]
- Ploegstra, M.-J.; Roofthooft, M.T.R.; Douwes, J.M.; Bartelds, B.; Elzenga, N.J.; van de Weerd, D.; Hillege, H.L.; Berger, R.M.F. Echocardiography in pediatric pulmonary arterial hypertension: Early study on assessing disease severity and predicting outcome. Circ. Cardiovasc. Imaging 2015, 8, e000878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koestenberger, M.; Apitz, C.; Abdul-Khaliq, H.; Hansmann, G. Transthoracic echocardiography for the evaluation of children and adolescents with suspected or confirmed pulmonary hypertension. Expert consensus statement on the diagnosis and treatment of paediatric pulmonary hypertension. The European Paediatric Pulmonary Vascular Disease Network, endorsed by ISHLT and D6PK. Heart 2016, 102 (Suppl. 2), ii14–ii22. [Google Scholar] [PubMed] [Green Version]
- Bronicki, R.A. Cardiopulmonary Interactions in Children with Heart Failure. Curr. Cardiol. Rev. 2016, 12, 104–106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pinsky, M.R. Cardiopulmonary Interactions: Physiologic Basis and Clinical Applications. Ann. Am. Thorac. Soc. 2018, 15, S45–S48. [Google Scholar] [CrossRef]
- Motoji, Y.; Tanaka, H.; Fukuda, Y.; Sano, H.; Ryo, K.; Imanishi, J.; Miyoshi, T.; Sawa, T.; Mochizuki, Y.; Matsumoto, K.; et al. Interdependence of right ventricular systolic function and left ventricular filling and its association with outcome for patients with pulmonary hypertension. Int. J. Cardiovasc. Imaging 2015, 31, 691–698. [Google Scholar] [CrossRef]
- Burkett, D.A.; Slorach, C.; Patel, S.S.; Redington, A.N.; Ivy, D.D.; Mertens, L.; Younoszai, A.K.; Friedberg, M.K. Impact of Pulmonary Hemodynamics and Ventricular Interdependence on Left Ventricular Diastolic Function in Children With Pulmonary Hypertension. Circ. Cardiovasc. Imaging 2016, 9, e004612. [Google Scholar] [CrossRef] [Green Version]
- Van der Hulst, A.E.; Delgado, V.; Ten Harkel, A.D.J.; Klitsie, L.M.; Filippini, L.H.P.M.; Bax, J.J.; Blom, N.A.; Roest, A.A.W. Tissue Doppler imaging in the left ventricle and right ventricle in healthy children: Normal age-related peak systolic velocities, timings, and time differences. Eur. J. Echocardiogr. 2011, 12, 953–960. [Google Scholar] [CrossRef]
- Cui, W.; Roberson, D.A. Left ventricular Tei index in children: Comparison of tissue Doppler imaging, pulsed wave Doppler, and M-mode echocardiography normal values. J. Am. Soc. Echocardiogr. 2006, 19, 1438–1445. [Google Scholar] [CrossRef]
- Goroshi, M.; Chand, D. Myocardial Performance Index (Tei Index): A simple tool to identify cardiac dysfunction in patients with diabetes mellitus. Indian Heart J. 2016, 68, 83–87. [Google Scholar] [CrossRef] [Green Version]
- MD, Y.O.; Norikazu Yamada, P.F.; Kaoru Dohi, P.F.; MD, A.M.; Akihiro Tsuji, P.; Satoshi Ota, P.; Ken Ishikura, P.; Mashio Nakamura, P.F.; Masaaki Ito, P.F. Utility of right ventricular Tei-index for assessing disease severity and determining response to treatment in patients with pulmonary arterial hypertension. J. Cardiol. 2014, 63, 149–153. [Google Scholar]
- Yadav, D.K.; Choudhary, S.; Gupta, P.K.; Beniwal, M.K.; Agarwal, S.; Shukla, U.; Dubey, N.K.; Sankar, J.; Kumar, P. The Tei Index and Asymptomatic Myocarditis in Children With Severe Dengue. Pediatr. Cardiol. 2013, 34, 1307–1313. [Google Scholar] [CrossRef] [PubMed]
- Gupta-Malhotra, M.; Hamzeh, R.K.; Poffenbarger, T.; McNiece-Redwine, K.; Hashmi, S.S. Myocardial Performance Index in Childhood Onset Essential Hypertension and White Coat Hypertension. AJHYPE 2015, 28, 123–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, S.-M.; Lin, C.-C.; Hsiao, S.-H.; Lee, C.-Y.; Yang, S.-H.; Lin, S.-K.; Huang, W.-C. Pulmonary Hypertension and Left Heart Function: Insights from Tissue Doppler Imaging and Myocardial Performance Index. Echocardiography 2007, 24, 366–373. [Google Scholar] [CrossRef] [PubMed]
- Cevik, A.; Kula, S.; Olgunturk, R.; Saylan, B.; Pektas, A.; Oguz, D.; Tunaoglu, S. Doppler tissue imaging provides an estimate of pulmonary arterial pressure in children with pulmonary hypertension due to congenital intracardiac shunts. Congenit. Heart Dis. 2013, 8, 527–534. [Google Scholar] [CrossRef] [PubMed]
- Abo-Haded, H.M.; Barakat, T.S.; Hafez, M.M. Myocardial performance in children with autoimmune hepatitis: Doppler tissue imaging study. Eur. J. Pediatr. 2013, 172, 1511–1519. [Google Scholar] [CrossRef] [PubMed]
- Özkan, E.A.; Khosroshahi, H.E. Evaluation of the left and right ventricular systolic and diastolic function in asthmatic children. BMC Cardiovasc. Disord. 2016, 16, 1–7. [Google Scholar]
- Lammers, A.E.; Haworth, S.G.; Riley, G.; Maslin, K.; Diller, G.-P.; Marek, J. Value of tissue Doppler echocardiography in children with pulmonary hypertension. J. Am. Soc. Echocardiogr. 2012, 25, 504–510. [Google Scholar] [CrossRef]
- Friesen, R.M.; Schäfer, M.; Burkett, D.A.; Cassidy, C.J.; Ivy, D.D.; Jone, P.-N. Right Ventricular Tissue Doppler Myocardial Performance Index in Children with Pulmonary Hypertension: Relation to Invasive Hemodynamics. Pediatr. Cardiol. 2017, 39, 98–104. [Google Scholar] [CrossRef]
- Jingi, A.; Czitrom, D.; Hamadou, B.; Mankoubi, L.; Sondes, S.; Kingue, S. Sensitivity, specificity, and accuracy of left ventricular systolic function indices and structure in detecting early systolic dysfunction assessed by speckle-tracking two-dimensional strain: An echocardiographic cross-sectional study. Res. Cardiovasc. Med. 2018, 7, 176–178. [Google Scholar] [CrossRef]
- Dedeoglu, R.; Barut, K.; Oztunc, F.; Atik, S.; Adrovic, A.; Sahin, S.; Cengiz, D.; Kasapcopur, O. Evaluation of myocardial deformation in patients with Kawasaki disease using speckle-tracking echocardiography during mid-term follow-up - CORRIGENDUM. Cardiol. Young 2017, 27, 1386. [Google Scholar] [CrossRef] [Green Version]
- Reisner, S.A.; Lysyansky, P.; Agmon, Y.; Mutlak, D.; Lessick, J.; Friedman, Z. Global longitudinal strain: A novel index of left ventricular systolic function. J. Am. Soc. Echocardiogr. 2004, 17, 630–633. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hematian, M.-N.; Torabi, S.; MalaKan-Rad, E.; Sayadpour-Zanjani, K.; Ziaee, V.; Lotfi-Tolkaldany, M. Noninvasive Evaluation of Myocardial Systolic Dysfunction in the Early Stage of Kawasaki Disease: A Speckle-Tracking Echocardiography Study. Iran. J. Pediatr. 2015, 25, e198. [Google Scholar] [CrossRef]
- Checchia, P.A.; Appel, H.J.; Kahn, S.; Smith, F.A.; Shulman, S.T.; Pahl, E.; Baden, H.P. Myocardial injury in children with respiratory syncytial virus infection. Pediatric Crit. Care Med. 2000, 1, 146–150. [Google Scholar] [CrossRef] [PubMed]
- Milas, A.; Shah, A.; Anand, N.; Saunders-Kurban, M.; Patel, S. Respiratory Syncytial Virus Associated Myocarditis Requiring Venoarterial Extracorporeal Membrane Oxygenation. Case Rep. Infect. Dis. 2017, 2017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, K.C.; Gaze, D.C.; Collinson, P.O.; Marber, M.S. Cardiac troponins: From myocardial infarction to chronic disease. Cardiovasc. Res. 2017, 113, 1708–1718. [Google Scholar] [CrossRef]
- Rodriguez-Gonzalez, M.; Sanchez-Codez, M.I.; Lubian-Gutierrez, M.; Castellano-Martinez, A. Clinical presentation and early predictors for poor outcomes in pediatric myocarditis: A retrospective study. World J. Clin. Cases 2019, 7, 548–561. [Google Scholar] [CrossRef]
- Dionne, A.; Kheir, J.N.; Sleeper, L.A.; Esch, J.J.; Breitbart, R.E. Value of Troponin Testing for Detection of Heart Disease in Previously Healthy Children. J. Am. Heart Assoc. 2020, 9, e012897. [Google Scholar] [CrossRef]
- Eisenhut, M. Causes of cardiac troponin elevation in critically ill children. Minerva Anestesiol. 2013, 79, 451. [Google Scholar]
- Yoldaş, T.; Örün, U.A. What is the Significance of Elevated Troponin I in Children and Adolescents? A Diagnostic Approach. Pediatr. Cardiol. 2019, 40, 1–7. [Google Scholar] [CrossRef]
- Castellano-Martinez, A.; Rodriguez-Gonzalez, M. Coronary artery spasm due to intravenous atropine infusion in a child: Possible Kounis syndrome. Cardiol. Young 2018, 28, 616–618. [Google Scholar] [CrossRef]
- Eisenhut, M. Extrapulmonary manifestations of severe respiratory syncytial virus infection--a systematic review. Crit. Care 2006, 10, R107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clerico, A.; Recchia, F.A.; Passino, C.; Emdin, M. Cardiac endocrine function is an essential component of the homeostatic regulation network: Physiological and clinical implications. Am. J. Physiol. -Heart Circ. Physiol. 2006, 290, H17–H29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodriguez-Gonzalez, M.; Perez-Reviriego, A.A.; Castellano-Martinez, A.; Cascales-Poyatos, H.M. N-terminal probrain natriuretic peptide as biomarker for diagnosis of Kawasaki disease. Biomark. Med. 2019, 13, 307–323. [Google Scholar] [CrossRef] [PubMed]
- Ten Kate, C.A.; Tibboel, D.; Kraemer, U.S. B-type natriuretic peptide as a parameter for pulmonary hypertension in children. A systematic review. Eur. J. Pediatr. 2015, 174, 1267–1275. [Google Scholar] [CrossRef] [PubMed]
- Medar, S.S.; Hsu, D.T.; Ushay, H.M.; Lamour, J.M.; Cohen, H.W.; Killinger, J.S. Serial Measurement of Amino-Terminal Pro-B-Type Natriuretic Peptide Predicts Adverse Cardiovascular Outcome in Children With Primary Myocardial Dysfunction and Acute Decompensated Heart Failure. Pediatric Crit. Care Med. 2015, 16, 529–534. [Google Scholar] [CrossRef] [Green Version]
- Calzetta, L.; Orlandi, A.; Page, C.; Rogliani, P.; Rinaldi, B.; Rosano, G.; Cazzola, M.; Matera, M.G. Brain natriuretic peptide: Much more than a biomarker. Int. J. Cardiol. 2016, 221, 1031–1038. [Google Scholar] [CrossRef] [Green Version]
- Takatsuki, S.; Wagner, B.D.; Ivy, D.D. B-type natriuretic peptide and amino-terminal pro-B-type natriuretic peptide in pediatric patients with pulmonary arterial hypertension. Congenit. Heart Dis. 2012, 7, 259–267. [Google Scholar] [CrossRef] [Green Version]
- Lohani, O.; Colvin, K.L.; Yeager, M.E. Biomarkers for pediatric pulmonary arterial hypertension: Challenges and recommendations. Paediatr. Respir. Rev. 2015, 16, 225–231. [Google Scholar] [CrossRef]
- Lin, C.-W.; Tang, W.; Wen, F.; Chen, J.-J.; Zeng, X.-L.; Chen, Z.-G. Diagnostic Accuracy of NT-ProBNP for Heart Failure with Sepsis in Patients Younger than 18 Years. PLoS ONE 2016, 11, e0147930. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez-Gonzalez, M.; Castellano-Martinez, A.; Alonso-Ojembarrena, A. Usefulness of age-adjusted N-terminal prohormone of brain natriuretic peptide level as a diagnostic marker for incomplete Kawasaki disease in children. Emergencias 2019, 31, 111–114. [Google Scholar]
- Edwards, K.D.; Tighe, M.P. How to use N-terminal pro-brain natriuretic peptide (NT-proBNP) in assessing disease severity in bronchiolitis. Arch. Dis Child. Educ. Pr. Ed. 2019, edpract–2019–316896. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Gonzalez, M.; Benavente Fernández, I.; Castellano-Martinez, A. Plasmatic NT-proBNP could help to select cases for screening echocardiography in healthy infants with Respiratory Syncytial Virus infection. Cardiol Young 2019, 29, 1414–1415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Samuel, N.; Hershkovitz, T.; Brik, R.; Lorber, A.; Shavit, I. Diagnosing heart failure in children with congenital heart disease and respiratory syncytial virus bronchiolitis. Am. J. Emerg. Med. 2014, 32, 1510–1512. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Article | Reporting | External Validity | Internal Validity | Confounding & Selection Bias | Power | Total |
|---|---|---|---|---|---|---|
| Pahl et al. [21] | 8/10 | 2/3 | 5/7 | 3/6 | 0/1 | 18 |
| Sreeram et al. [22] | 8/10 | 1/3 | 5/7 | 3/6 | 0/1 | 17 |
| Fitzgerald et al. [23] | 8/10 | 1/3 | 5/7 | 2/6 | 0/1 | 16 |
| Esposito et al. [24] | 9/10 | 1/3 | 5/7 | 3/6 | 0/1 | 18 |
| Bardi-Peti et al. [25] | 8/10 | 1/3 | 5/7 | 3/6 | 0/1 | 17 |
| Thorburn et al. [26] | 9/10 | 1/3 | 5/7 | 2/6 | 0/1 | 17 |
| Horter et al. [27] | 9/10 | 1/3 | 5/7 | 3/6 | 0/1 | 18 |
| Rguez-Glez et al. [28] | 9/10 | 2/3 | 6/7 | 4/6 | 0/1 | 21 |
| Rguez-Glez et al. [29] | 9/10 | 2/3 | 6/7 | 4/6 | 0/1 | 21 |
| Massolo et al. [30] | 9/10 | 2/3 | 6/7 | 3/6 | 0/1 | 20 |
| Author (Year) | Study Design & Duration | Number & Age of Participants | Characteristics of Participants & Setting | Rate of Severe AB | Echo Technique & Timing | Biomarker | Rate of MS |
|---|---|---|---|---|---|---|---|
| Pahl et al. [21] | Prospective not controlled. (?) | 19 AB. Age 4.4 m (3 w–10 m) | 17 healthy and 2 cystic fibrosis CHD excluded. Setting not mentioned | 10/19 (52%) | Conventional 2D doppler echo Within 72 h of admission | No | No |
| Sreeram et al. [22] | Prospective not controlled. (?) | 21 AB. Age (1–24 months) | 20 healthy infants & 1 Down Sd. CHD excluded. Setting not mentioned | 4/21 (16%) | Conventional 2D doppler echo Within 24 h of admission | No | Yes (24%) |
| Fitzgerald et al. [23] | Prospective not controlled. (3 m) | 6 AB. Age 13 (4–24) w | 4 premature & 2 term infants admitted at NICU CHD excluded | 6/6 (100%) | Conventional 2D doppler echo Within 72 h of intubation | No | Yes (66%) |
| Esposito et al. [24] | Prospective not controlled (2 y) | 69 AB. Age 4.2 (2.5) m | All healthy infants admitted at pediatric ward CHD excluded | 0/69 (0%) | Conventional 2D doppler echo Within 24 h of admission | Yes | No |
| Bardi-Peti et al. [25] | Prospective controlled (2 y) | 49 AB & 62 age-matched controls Age 1–12 m | All healthy infants admitted at pediatric ward CHD excluded | 17/49 (34%) | Conventional 2D doppler echo Within 24 h of admission | No | Yes (36%) |
| Thorburn et al. [26] | Prospective not controlled (2 y) | 34 AB. Age 1.4 (0.4–11.7) m. | All healthy infants admitted at PICU | 34/34 (100%) | Conventional 2D doppler echo Within 24-48 h of admission | Yes | Yes (24%) |
| Horter et al. [27] | Prospective not controlled (2 y) | 26 AB. Age 2 (1–24) m. | 26 healthy infants admitted at pediatric ward CHD excluded | 0 (26%) | Conventional 2D doppler echo Within 24 h of admission | Yes | No |
| Rguez-Glez et al. [28] | Prospective not controlled (3 y) | 93 AB. Age 2 (1–10) m. | All healthy infants admitted at pediatric ward CHD excluded | 21/93 (22%) | Conventional 2D doppler echo Within 24 h of admission | Yes | Yes (22%) |
| Rguez-Glez et al. [29] | Prospective controlled (1 y) | 50 AB & 50 age-matched controls Age 2 (1–6.5) m. | All healthy infants admitted at pediatric ward CHD excluded | 10/50 ((20%) | Conventional & TDI-echo Within 24 h of admission | Yes | Yes (28%) |
| Massolo et al. [30] | Prospective controlled (5 m) | 28 AB & 10 age-matched controls Age 30 (20) d. | All healthy infants admitted at pediatric ward CHD excluded | 10/28 (35%) | Conventional & STE-echo Within 24 h of admission | No | Yes (32%) |
| Author (Year) | Echo Parameters | Incidence & Type of Myocardial Strain | Significant Outcome |
|---|---|---|---|
| Sreeram et al. [22] | LVFS, TRJG, PVV | Mild PH in 23%. No CD | PH associated with 100% of severe infections and 100% exitus (1 patient with Down syndrome and PH). PH disappeared with clinical improvement. |
| Fitzgerald et al. [23] | LVFS, TRJG | Mild PH in 66%. No CD | 100% of patients with PH presented a severe disease and adverse outcomes. |
| Bardi-Peti et al. [25] | TRGJ, ATET | PH in 28%. No CD | PH was associated to moderate/severe wheezing episodes and prolonged LOS hospitalization. |
| Thorburn et al. [26] | LVFS, PW-doppler derived RVMPI, TRJG | RVD in 20% (RVD). No PH | All patients with RVD presented a severe clinical state. There was no difference with those patients without RVD. |
| Rguez-Glez et al. [28] | LVFS, TAPSE, TRJG, ATET, LVEI, SF | PH 22%. RVD 2% | PH was associated with a worse clinical state and impaired gas exchange. Up to 85% of cases with PH presented significantly adverse outcomes (PICU admission). |
| Rguez-Glez et al. [29] | LVFS, TAPSE, TRJG, ATET, LVEI, SF, TDI derived RVMPI & LVMPI | LVD in 18%. RVD in 20%. PH 28% | LVD, RVD and PH were associated with a severe clinical presentation and impaired gas exchange. Up to 89% of cases with LVD presented significantly adverse outcomes (PICU admission). |
| Massolo et al. [30] | LVEF, RVFAC, RVFS, LS, CS, RS, TRJG, LVEI, SF | LVD 32%. BD in 32%. PH in 29% | BD was associated with higher frequency of hypoxia and hypercarbia. BD was associated with higher levels of respiratory support. |
| Author (Year) | Cardiac Biomarker | Values | Correlation with Echo | Details |
|---|---|---|---|---|
| Esposito et al. [24] | Troponin I (Abbott AxSYM system) | Normal values (0.011 (0.02) IU/L) | No | All cases were mild without need of PICU admission |
| Thorburn et al. [26] | Troponin T (ELISA, Roche Diagnostics) | cTnT elevated (> 10ng/L) in 41% | No | All cases were severe and required mechanical ventilation and PICU admission |
| Horter et al. [27] | Troponin T (ELISA, Roche Diagnostics) | cTnT elevated (>10ng/L) in 23% | No | All cases were mild without need of PICU admission |
| Rguez-Glez et al. [28] | NT-proBNP (ELISA, Roche Diagnostics) | Elevated (>1635 pg/mL) in 25% | Associated with PH | Increased NT-proBNP was an independent and accurate predictor for PH in AB (AUC = 0.932; p < 0.001). The optimal cut-off value yielded a sensitivity of 0.86, specificity of 0.89; PPV of 0.70 and NPV of 0.95) |
| Troponin T (Abbott AxSYM system) | Elevated (>10ng/L) in 14% | Associated with PH | cTnT was not an independent predictor for PH in the multivariate analysis (p = 0.354) | |
| Rguez-Glez et al. [29] | NT-proBNP (ELISA, Roche Diagnostics) | Elevated in patients with CD (2221 pg/mL vs. 377 pg/mL; p < 0.001) | Associated with LVD | The diagnostic performance of NT-proBNP to predict LVD in infants with AB resulted in high (AUC = 0.91). The best estimated cut-off value to predict was 1500 pg/mL, with a sensitivity of 0.80, specificity of 0.95, a PPV of 0.80), and an NPV of 0.95. |
| Group | N | t-Value | P-Value | CI95% |
|---|---|---|---|---|
| Combined MS | 10 | −0.26 | 0.809 | −10.8 to 9.2 |
| Pulmonary Hypertension | 10 | 0.10 | 0.921 | −6.5 to 7 |
| Myocardial dysfunction | 10 | −0.87 | 0.545 | −132 to 115 |
| Severe AB | 5 | 0.07 | 0.951 | −1.2 to 1.2 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodriguez-Gonzalez, M.; Perez-Reviriego, A.A.; Castellano-Martinez, A.; Cascales-Poyatos, H.M. The Assessment of Myocardial Strain by Cardiac Imaging in Healthy Infants with Acute Bronchiolitis: A Systematic Review and Meta-Analysis. Diagnostics 2020, 10, 382. https://doi.org/10.3390/diagnostics10060382
Rodriguez-Gonzalez M, Perez-Reviriego AA, Castellano-Martinez A, Cascales-Poyatos HM. The Assessment of Myocardial Strain by Cardiac Imaging in Healthy Infants with Acute Bronchiolitis: A Systematic Review and Meta-Analysis. Diagnostics. 2020; 10(6):382. https://doi.org/10.3390/diagnostics10060382
Chicago/Turabian StyleRodriguez-Gonzalez, Moises, Alvaro Antonio Perez-Reviriego, Ana Castellano-Martinez, and Helena Maria Cascales-Poyatos. 2020. "The Assessment of Myocardial Strain by Cardiac Imaging in Healthy Infants with Acute Bronchiolitis: A Systematic Review and Meta-Analysis" Diagnostics 10, no. 6: 382. https://doi.org/10.3390/diagnostics10060382
APA StyleRodriguez-Gonzalez, M., Perez-Reviriego, A. A., Castellano-Martinez, A., & Cascales-Poyatos, H. M. (2020). The Assessment of Myocardial Strain by Cardiac Imaging in Healthy Infants with Acute Bronchiolitis: A Systematic Review and Meta-Analysis. Diagnostics, 10(6), 382. https://doi.org/10.3390/diagnostics10060382