Heart Rate Monitor Instead of Ablation? Atrioventricular Nodal Re-Entrant Tachycardia in a Leisure-Time Triathlete: 6-Year Follow-Up


Abstract
:1. Introduction
2. Materials and Methods
2.1. Sports Biography
2.2. Methods
2.2.1. Study Protocol
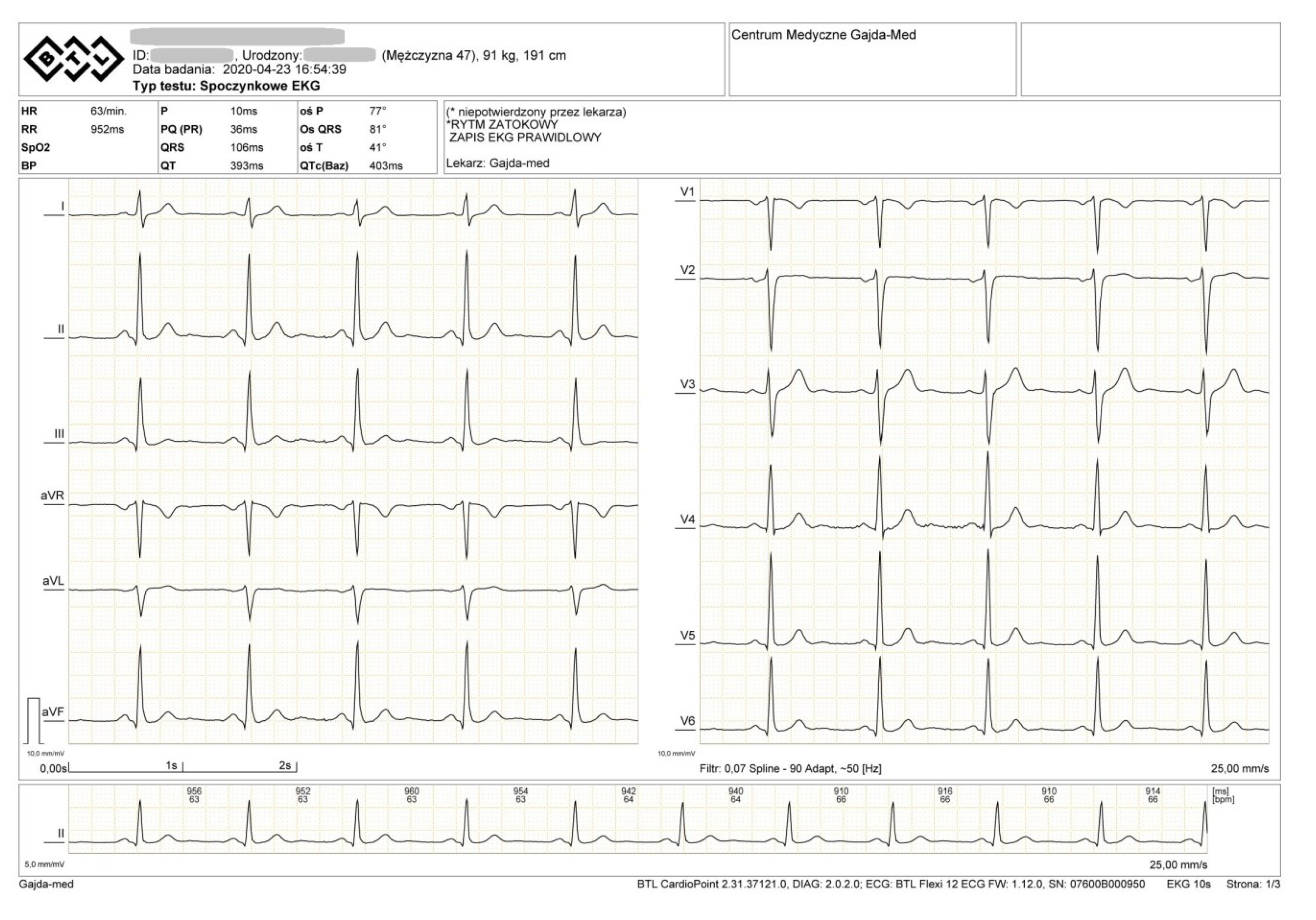
2.2.2. Electrocardiogram (ECG) Tests
2.2.3. Transthoracic Echocardiography
2.2.4. Holter ECG
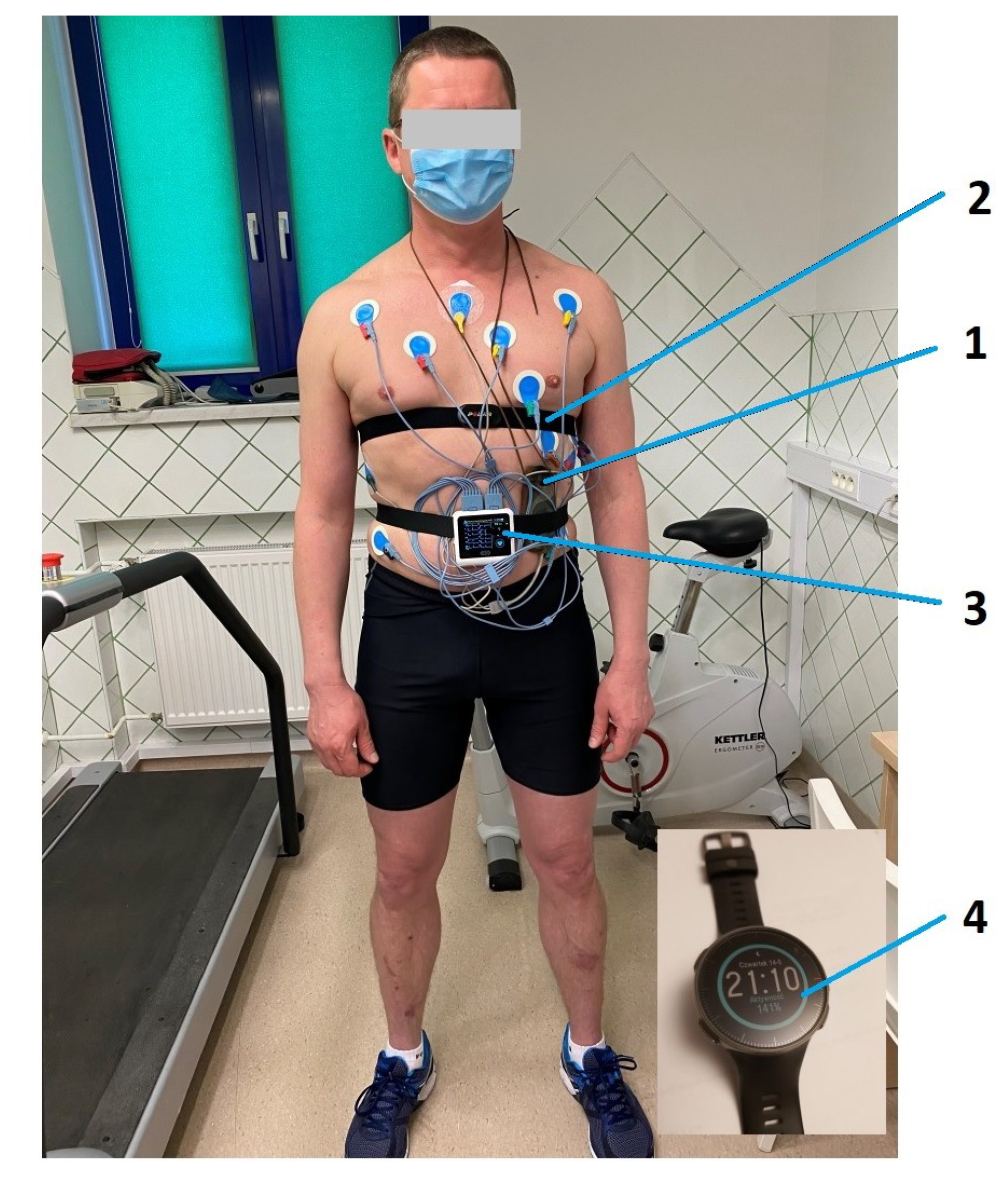
2.2.5. Exercise Stress Test
2.2.6. Heart-Rate Monitor (HRM) Analyses
2.2.7. Statistical Analysis
2.2.8. Ethical Approval
3. Results
3.1. HRM Data Analysis
3.2. ECG Tests
3.3. Echocardiography
3.4. Exercise Stress Test
3.5. Heart-Rate Monitor Tests
4. Discussion
4.1. Discussion of the Results
4.2. Atrioventricular Nodal Re-Entrant Tachycardia (AVNRT) in Athletes
4.3. The Role of HRMs in Recognizing the Type of Arrhythmia in Athletes
4.4. Limitation
4.5. Perspectives
5. Conclusions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Date | Type of Training R-Running B-Bicycle | Time from Start of Training to Tachycardia Event [hh:mm:ss] | HR by Beginning of Tachycardia [bpm] | AVNRT | Time From Start of Training to the End of Tachycardia Event [hh:mm:ss] | Duration of AVNRT [s] | HR by the End of Tachycardia [bpm] | Type of Tachycardia |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 02.03.2014 | R | 00:50:20 | 155 | 192 | 00:52:25 | 125 | 143 | Primary |
| 2 | 10.04.2014 | B | 00:35:16 | 153 | 186 | 00:38:06 | 170 | 120 | Primary |
| 3 | 15.06.2014 | B | 00:59:01 | 145 | 180 | 01:00:06 | 65 | 130 | Primary |
| 4 | 29.07.2014 | R | 00:30:00 | 145 | 170 | 00:31:50 | 110 | 140 | Primary |
| 5 | 30.08.2014 | R | 00:15:40 | 90 | 200 | 00:16:17 | 37 | 90 | Primary |
| 6 | 15.09.2014 | B | 00:10:00 | 120 | 169 | 00:11:12 | 72 | 115 | Primary |
| 7 | 10.10.2014 | R | 01:08:02 | 167 | 227 | 01:11:08 | 186 | 156 | Primary |
| 8 | 10.01.2015 | B | 00:27:32 | 134 | 159 | 00:28:02 | 30 | 132 | Primary |
| 9 | 20.02.2015 | B | 00:05:30 | 120 | 160 | 00:06:10 | 40 | 118 | Primary |
| 10 | 30.03.2015 | R | 00:15:30 | 100 | 190 | 00:15:45 | 15 | 100 | Primary |
| 11 | 04.04.2015 | B | 00:10:00 | 130 | 155 | 00:10:25 | 25 | 120 | Primary |
| 12 | 02.07.2015 | B | 00:04:10 | 118 | 160 | 00:04:37 | 27 | 117 | Primary |
| 13 | 27.08.2015 | R | 00:23:04 | 120 | 190 | 00:24:04 | 60 | 115 | Primary |
| 14 | 15.09.2015 | R | 00:29:30 | 115 | 211 | 00:30:32 | 62 | 115 | Primary |
| 15 | 16.10.2015 | B | 00:08:10 | 125 | 160 | 00:08:40 | 30 | 120 | Primary |
| 16 | 18.01.2016 | B | 01:00:01 | 130 | 172 | 01:01:21 | 80 | 126 | Primary |
| 17 | 15.03.2016 | R | 00:59:53 | 120 | 210 | 01:00:13 | 20 | 110 | Primary |
| 18 | 02.04.2016 | R | 01:50:10 | 125 | 200 | 01:50:50 | 40 | 115 | Primary |
| 19 | 14.04.2016 | B | 00:45:20 | 137 | 202 | 00:46:10 | 50 | 130 | Primary |
| 20 | 30.04.2016 | R | 00:51:27 | 153 | 190 | 00:52:04 | 37 | 139 | Primary |
| 21 | 02.05.2016 | R | 00:31:53 | 144 | 165 | 00:34:25 | 152 | 97 | Primary |
| 22 | 23.05.2016 | R | 00:13:35 | 86 | 199 | 00:14:01 | 26 | 103 | Primary |
| 22a | 23.05.2016 | R | 00:15:26 | 93 | 189 | 00:15:33 | 7 | 109 | Secondary |
| 23 | 23.07.2016 | R | 00:16:14 | 135 | 188 | 00:16:59 | 45 | 130 | Primary |
| 24 | 05.03.2017 | R | 00:22:04 | 117 | 189 | 00:23:00 | 56 | 93 | Primary |
| 25 | 02.04.2017 | R | 00:27:30 | 107 | 210 | 00:28:27 | 57 | 102 | Primary |
| 25a | 02.04.2017 | R | 02:59:53 | 112 | 211 | 03:00:15 | 22 | 79 | Secondary |
| 25b | 02.04.2017 | R | 03:10:14 | 122 | 201 | 03:11:03 | 49 | 112 | Tertiary |
| 26 | 20.04.2017 | B | 00:33:16 | 149 | 185 | 00:34:32 | 76 | 116 | Primary |
| 27 | 17.01.2018 | B | 00:01:35 | 121 | 176 | 00:02:12 | 37 | 98 | Primary |
| 28 | 02.02.2018 | B | 00:04:29 | 104 | 164 | 00:05:05 | 36 | 116 | Primary |
| 28a | 02.02.2018 | B | 00:25:32 | 130 | 158 | 00:25:55 | 23 | 118 | Secondary |
| 29 | 19.02.2018 | B | 00:03:03 | 100 | 159 | 00:03:36 | 33 | 101 | Primary |
| 30 | 08.04.2018 | R | 02:10:55 | 128 | 210 | 02:11:16 | 21 | 119 | Primary |
| 30a | 08.04.2018 | R | 03:10:30 | 114 | 217 | 03:11:26 | 56 | 108 | Secondary |
| 31 | 19.03.2018 | B | 00:20:10 | 135 | 160 | 00:20:50 | 40 | 130 | Primary |
| 32 | 01.05.2018 | R | 00:55:55 | 143 | 190 | 00:56:39 | 44 | 140 | Primary |
| 33 | 19.11.2018 | B | 00:02:58 | 126 | 150 | 00:03:19 | 21 | 117 | Primary |
| 34 | 19.02.2019 | B | 00:02:54 | 118 | 159 | 00:03:04 | 10 | 130 | Primary |
| 35 | 09.05.2019 | B | 00:03:05 | 119 | 157 | 00:03:28 | 23 | 125 | Primary |
| 36 | 02.07.2019 | R | 01:30:30 | 140 | 205 | 01:31:50 | 80 | 133 | Primary |
| 37 | 18.12.2019 | B | 01:03:47 | 124 | 170 | 01:05:02 | 75 | 115 | Primary |
| 38 | 13.01.2020 | B | 00:44:07 | 136 | 199 | 00:45:43 | 96 | 98 | Primary |
| 39 | 30.03.2020 | R | 01:11:50 | 147 | 207 | 01:12:27 | 37 | 140 | Primary |
| 40 | 10.04.2020 | R | 02:00:01 | 130 | 212 | 02:00:36 | 35 | 128 | Primary |
References
- Walsh, J.A., III; Topol, E.J.; Steinhubl, S.R. Novel wireless devices for cardiac monitoring. Circulation 2014, 130, 573–581. [Google Scholar] [CrossRef] [PubMed]
- Gajda, R.; Biernacka, E.K.; Drygas, W. The problem of arrhythmias in endurance athletes: Are heart rate monitors valuable tools for diagnosing arrhythmias? In Horizons in World Cardiovascular Research; Nova Science Publishers, Inc.: New York, NY, USA, 2018; Volume 15, pp. 1–64. [Google Scholar]
- Josephson, M.E. Supraventricular Tachycardias. In Clinical Cardiac Electrophysiology Techniques and Interpretations, 5th ed.; Wolters Kluwer/Lippincott Williams & Wilkins: Philadelphia, PA, USA; Baltimore, MD, USA; New York, NY, USA; London, UK; Buenos Aires, Argentina; Hong Kong, China; Sydney, Australia; Tokyo, Japan, 2008; p. 176. [Google Scholar]
- Miljoen, H.; Ector, J.; Garweg, C.; Saenen, J.; Huybrechts, W.; Sarkozy, A.; Willems, R.; Heidbuchel, H. Differential Presentation of Atrioventricular Nodal Re-Entrant Tachycardia in Athletes and Non-Athletes. Europace 2019, 21, 944–949. [Google Scholar] [CrossRef] [PubMed]
- Heidbüchel, H.; Jackman, W.M. Characterization of Subforms of AV Nodal Reentrant Tachycardia. Europace 2004, 6, 316–329. [Google Scholar] [CrossRef] [PubMed]
- Opel, A.; Murray, S.; Kamath, N.; Dhinoja, M.; Abrams, D.; Sporton, S.; Schilling, R.; Earley, M. Cryoablation versus radiofrequency ablation for treatment of atrioventricular nodal reentrant tachycardia: Cryoablation with 6-mm-tip catheters is still less effective than radiofrequency ablation. Heart Rhythm 2010, 7, 340–343. [Google Scholar] [CrossRef] [PubMed]
- Gajda, R.; Biernacka, E.K.; Drygas, W. Are Heart Rate Monitors Valuable Tools for Diagnosing Arrhythmias in Endurance Athletes? Scand. J. Med. Sci. Sports 2018, 28, 496–516. [Google Scholar] [CrossRef] [PubMed]
- Bhavnani, S.P.; Narula, J.; Sengupta, P.P. Mobile technology and the digitization of healthcare. Eur. Heart J. 2016, 37, 1428–1438. [Google Scholar] [CrossRef] [PubMed]
- Mozos, I.; Caraba, A. Electrocardiographic Predictors of Cardiovascular Mortality. Dis. Markers 2015, 2015, 727401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwaku, K.F.; Josephson, M.E. Typical AVNRT—An Update on Mechanisms and Therapy. Card Electrophysiol. Rev. 2002, 6, 414–421. [Google Scholar] [CrossRef] [PubMed]
- Wilhelm, M.; Roten, L.; Tanner, H.; Wilhelm, I.; Schmid, J.P.; Saner, H. Gender Differences of Atrial and Ventricular Remodeling and Autonomic Tone in Nonelite Athletes. Am. J. Cardiol. 2011, 108, 1489–1495. [Google Scholar] [CrossRef] [PubMed]
- Mohanty, S.; Mohanty, P.; Tamaki, M.; Natale, V.; Gianni, C.; Trivedi, C.; Gokoglan, Y.; Di Biase, L.; Natale, A. Differential Association of Exercise Intensity with Risk of Atrial Fibrillation in Men and Women: Evidence from a Meta-Analysis. J. Cardiovasc. Electrophysiol. 2016, 27, 1021. [Google Scholar] [CrossRef] [PubMed]
- Pesta, D.; Burtscher, M. Importance of Determining Maximal Heart Rate for Providing a Standardized Training Stimulus. JAMA Intern. Med. 2016, 176, 1883. [Google Scholar] [CrossRef] [PubMed]
- Hunt, D.; Tanto, P. Diagnosis of arrhythmias in athletes wearing heart rate monitors. BMJ Mil. Health 2017, 163, 224. [Google Scholar] [CrossRef] [PubMed]
- De Almeida, M.B.; Bottino, A.; Ramos, P.; Araujo, C.G. Measuring Heart Rate During Exercise: From Artery Palpation to Monitors and Apps. Int. J. Cardiovasc. Sci. 2019, 32, 396–407. [Google Scholar] [CrossRef]
- Müssigbrodt, A.; Richter, S.; Wetzel, U.; Van Belle, Y.; Bollmann, A.; Hindricks, G. Diagnosis of Arrhythmias in Athletes Using Leadless, Ambulatory HR Monitors. Med. Sci. Sports Exerc. 2013, 45, 1431–1435. [Google Scholar] [CrossRef] [PubMed]
- Garabelli, P.; Stavrakis, S.; Po, S. Smartphone-based arrhythmia monitoring. Curr. Opin. Cardiol. 2017, 32, 53–57. [Google Scholar] [CrossRef] [PubMed]
- Barbosa, M.P.; da Silva, N.T.; de Azevedo, F.M.; Pastre, C.M.; Vanderlei, L.C. Comparison of Polar® RS800G3TM Heart Rate Monitor with Polar® S810iTM and Electrocardiogram to Obtain the Series of RR Intervals and Analysis of Heart Rate Variability at Rest. Clin. Physiol. Funct. Imaging 2016, 36, 112–117. [Google Scholar] [CrossRef] [PubMed]
- Gajda, R.; Kowalik, E.; Rybka, S.; Rębowska, E.; Śmigielski, W.; Nowak, M.; Kwaśniewska, M.; Hoffman, P.; Drygas, W. Evaluation of the Heart Function of Swimmers Subjected to Exhaustive Repetitive Endurance Efforts During a 500-km Relay. Front. Physiol. 2019, 10, 296. [Google Scholar] [CrossRef] [PubMed]
- Gajda, R.; Klisiewicz, A.; Matsibora, V.; Piotrowska-Kownacka, D.; Biernacka, E.K. Heart of the World’s Top Ultramarathon Runner—Not Necessarily Much Different from Normal. Diagnostics (Basel) 2020, 10, 73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thabouillot, O.; Bostanci, K.; Bouvier, F.; Dumitrescu, N.; Stéfuriac, M.; Paule, P.; Roche, N.C. Syncope During Competitive Events: Interrogating Heart Rate Monitor Watches May Be Useful! Prehosp. Disaster Med. 2017, 32, 691–693. [Google Scholar] [CrossRef] [PubMed]
- Turakhia, M.P.; Desai, M.; Hedlin, H.; Rajmane, A.; Talati, N.; Ferris, T.; Desai, S.; Nag, D.; Patel, M.; Kowey, P.; et al. Rationale and design of a large-scale, app-based study to identify cardiac arrhythmias using a smartwatch: The Apple Heart Study. Am. Heart J. 2019, 207, 66–75. [Google Scholar] [CrossRef] [PubMed]
- Hwang, J.; Kim, J.; Choi, K.J.; Cho, M.S.; Nam, G.B.; Kim, Y.H. Assessing Accuracy of Wrist-Worn Wearable Devices in Measurement of Paroxysmal Supraventricular Tachycardia Heart Rate. Korean Circ. J. 2019, 49, 437–445. [Google Scholar] [CrossRef] [PubMed]
- Walker, J.; Calkins, H.; Nazarian, S. Evaluation of Cardiac Arrhythmia Among Athletes. Am. J. Med. 2010, 123, 1075–1081. [Google Scholar] [CrossRef] [PubMed] [Green Version]




| Age (Years) | Discipline | Training—Number of Hours/Week | Number of Years on Training | Hours of Training in Discipline | X- Endurance Sports—Adult Age—Hours at Training |
|---|---|---|---|---|---|
| 6–8 | swimming | 4 | 3 | 600 | |
| 8–11 | karate kyokushinkai | 4 | 4 | 800 | |
| 12–14 | judo | 4 | 3 | 600 | |
| 15–17 | swimming | 2 | 3 | 300 | |
| 15–19 | volleyball | 7 | 5 | 1750 | |
| 20–26 | kickboxing | 6 | 7 | 2100 | |
| 26–27 | sambo sports | 6 | 2 | 600 | |
| 27–32 | squash | 1 | 6 | 300 | |
| 27–45 | cycling | 2 | 18 | 1800 | X |
| 35–45 | swimming | 2 | 10 | 1000 | X |
| 35–45 | running | 2 | 10 | 1000 | X |
| 35–45 | starts in competitions or tests triathlon/running/cycling/swimming | 0.5 | 10 | 250 | X |
| 17–47 | skiing, sailing, waking, other | occasionally | 30 | ||
| Sport-life in total: 6 to 47 = 41 years | all disciplines | 5 | 40 | 11,100 (about) | X—about 4050 h in total, on average 6 times/week/10 years |
| Characteristic | Parameters | Start of Tachycardia [min] | HR at Beginning of Tachycardia [bpm] | HR at the end of Tachycardia [bpm] | AVNRT [bpm] | Time of AVNRT [s] | |
|---|---|---|---|---|---|---|---|
| Type of activity | All N = 40 | Median | 29 | 127 | 119 | 187 | 40 |
| QD | 23.7 | 11.5 | 8.8 | 19.0 | 21.8 | ||
| Min-Max | 2–131 | 86–167 | 90–156 | 150–227 | 10–186 | ||
| Cycling N = 20 | Median | 41 | 129 | 117 | 200 | 45 | |
| QD | 23.7 | 14.3 | 18.5 | 10.0 | 17.5 | ||
| Min-Max | 14–131 | 86–167 | 90–156 | 165–227 | 15–186 | ||
| Running N = 20 | Median | 10 | 126 | 119 | 162 | 39 | |
| QD | 18.0 | 8.0 | 6.3 | 9.5 | 22.5 | ||
| Min-Max | 2–64 | 100–153 | 98–132 | 150–202 | 10–170 | ||
| p-value (Cyc. vs. Run) | 0.0007 | 0.9679 | 0.681323 | 0.0004 | 0.6149 | ||
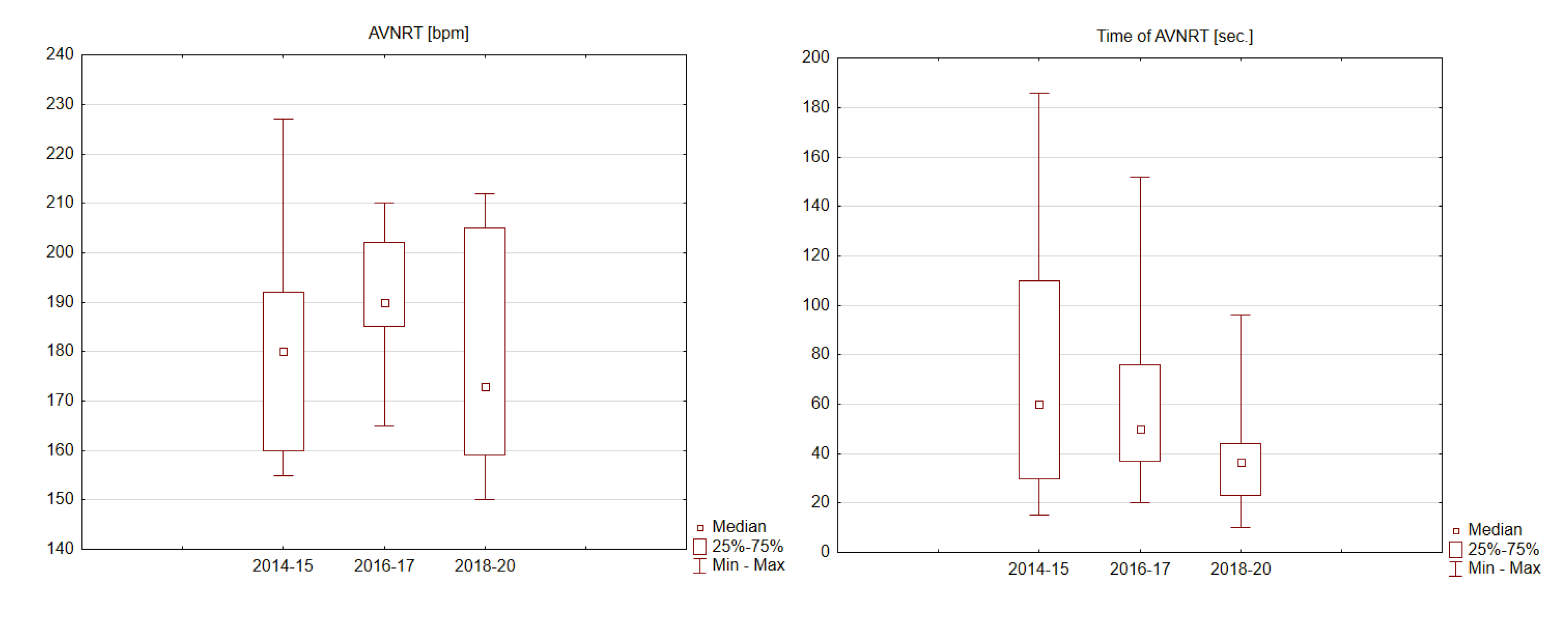
| Analyzed years with tachycardia | 2014–15 N = 15 | Median | 23 | 125 | 120 | 180 | 60 |
| QD | 12.6 | 13.5 | 8.5 | 16.0 | 40.0 | ||
| Min-Max | 4–68 | 90–167 | 90–156 | 155–227 | 15–186 | ||
| 2016–17 N = 11 | Median | 33 | 130 | 115 | 190 | 50 | |
| QD | 18.9 | 13.5 | 14.0 | 8.5 | 19.5 | ||
| Min-Max | 14–110 | 86–153 | 93–139 | 165– 210 | 20–152 | ||
| 2018–IV 20 N = 14 | Median | 32 | 127 | 122 | 173 | 37 | |
| QD | 34.4 | 8.5 | 7.5 | 23.0 | 10.5 | ||
| Min-Max | 2–131 | 100–147 | 98–140 | 150–212 | 10–96 | ||
| p-value (comparing periods) | 0.1778 | 0.1778 | 0.1593 | 0.2657 | 0.1748 | ||
| Features of tachycardia | Primary N = 40 | Median | 29 | 127 | 119 | 187 | 40 |
| QD | 23.7 | 11.5 | 8.8 | 19.0 | 21.8 | ||
| Min-Max | 2–131 | 86–167 | 90–156 | 150–227 | 10–186 | ||
| Repeated N = 5 | Median | 180 | 114 | 109 | 201 | 23 | |
| QD | 82.4 | 5.0 | 2.0 | 11.0 | 13.5 | ||
| Min-Max | 15–191 | 93–130 | 79–118 | 158–217 | 7–56 | ||
| p-value (primary vs. repeated) | 0.2249 | 0.2249 | 0.1056 | 0.2249 | 0.1380 | ||
| Parameters | Units (Normal Values) | Result |
|---|---|---|
| Left ventricle end-diastolic diameter volume | mL (106 ± 22) | 111 |
| Left ventricle end-systolic diameter volume | mL (41 ± 10) | 35 |
| Ejection fraction 2D (%) bi-plane | % (62 ± 5) | 65 |
| Global longitudinal strain | % (−20) | 20.4 |
| Interventricular septum diameter | mm (6–10) | 10 |
| Posterior wall diastolic diameter | mm (6–10) | 10 |
| Right ventricular end-diastolic diameter | mm (20–30) | 30 |
| S’ right ventricle | cm/s (14.1 ± 2.3) | 16 |
| Left atrium | mm (30–40) | 36 |
| Left atrial volume index | mL/m2 (16–34) | 30.0 |
| Right atrial area | cm2 16 ± 5 | 14.4 |
| Mitral valve E-wave | cm/s 73 ± 19 | 80 |
| Mitral valve A-wave | cm/s (69 ± 17) | 50 |
| E’ lateral | cm/s (>10) | 20 |
| E’ septal | cm/s (>7) | 12 |
| E/e’ lateral | ratio(<15) | 4.0 |
| E/e’ septal | ratio (<13) | 6.6 |
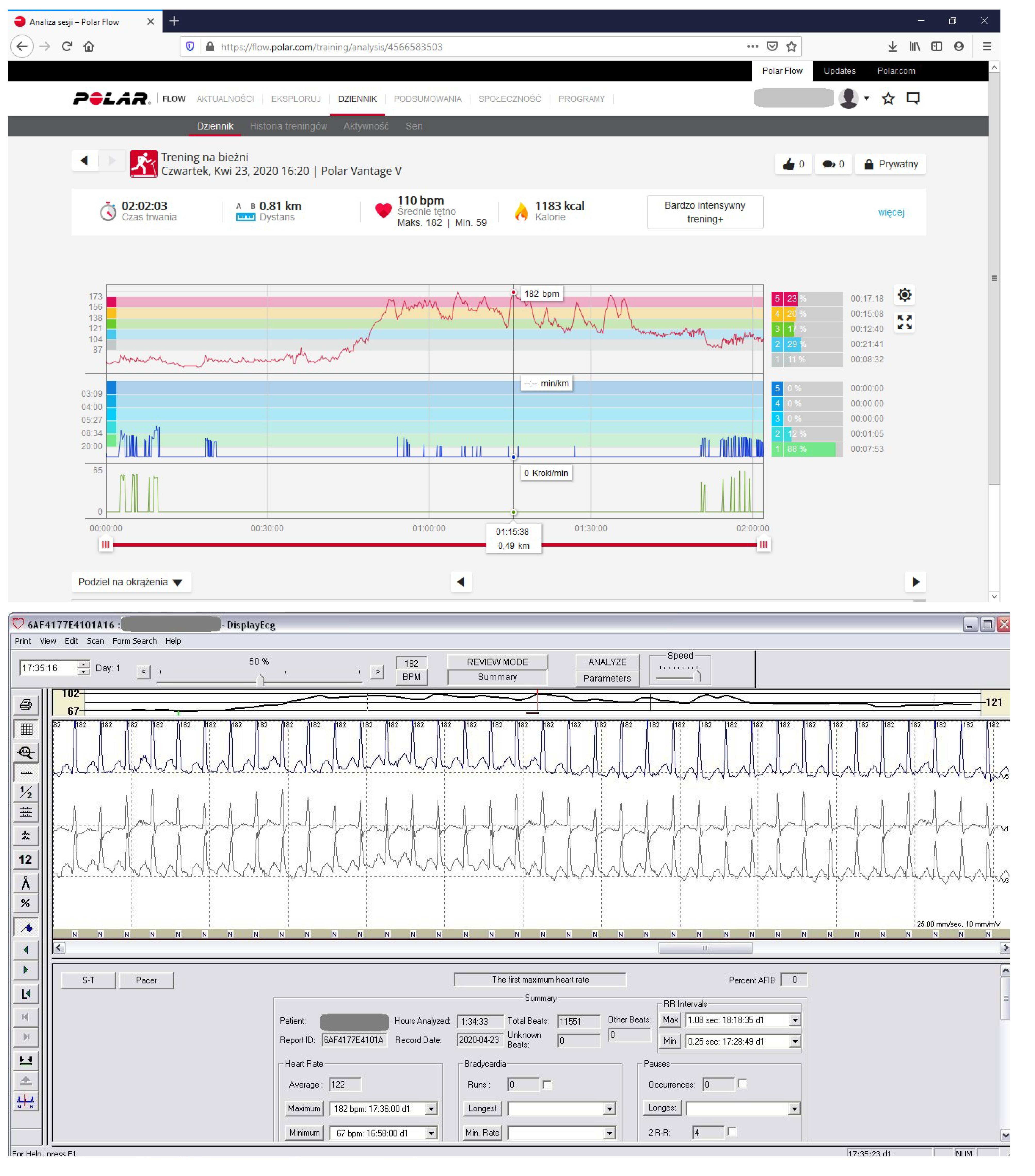
| Measurement Number | Polar Vantage V (Maximum HR Recorded during Training) (bpm) | V800 HR Monitors (Maximum HR Recorded during Training) (bpm) | Forerunner 910 XT GPS Maximum HR Recorded during Training (bpm) | Holter ECG Maximum HR Recorded during Training(bpm) | Difference in bpm Between Devices |
|---|---|---|---|---|---|
| 1 | 227 | 226 AVNRT | 1(App.1 No 7) | ||
| 2 | 179 | 179 SHR | 0 | ||
| 3 | 202 | 203 AVNRT | 1(App.1 No 19) | ||
| 4 | 178 | 178 SHR | 0 | ||
| 5 | 177 | 178 SHR | 1 | ||
| 6 | 205 | 206 AVNRT | 1(App.1 No 36) | ||
| 7 | 174 | 173 SHR | 1 | ||
| 8 | 182 | 182 SHR | 0 (Figure 1, Figure 4) |
© 2020 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gajda, R. Heart Rate Monitor Instead of Ablation? Atrioventricular Nodal Re-Entrant Tachycardia in a Leisure-Time Triathlete: 6-Year Follow-Up. Diagnostics 2020, 10, 391. https://doi.org/10.3390/diagnostics10060391
Gajda R. Heart Rate Monitor Instead of Ablation? Atrioventricular Nodal Re-Entrant Tachycardia in a Leisure-Time Triathlete: 6-Year Follow-Up. Diagnostics. 2020; 10(6):391. https://doi.org/10.3390/diagnostics10060391
Chicago/Turabian StyleGajda, Robert. 2020. "Heart Rate Monitor Instead of Ablation? Atrioventricular Nodal Re-Entrant Tachycardia in a Leisure-Time Triathlete: 6-Year Follow-Up" Diagnostics 10, no. 6: 391. https://doi.org/10.3390/diagnostics10060391
APA StyleGajda, R. (2020). Heart Rate Monitor Instead of Ablation? Atrioventricular Nodal Re-Entrant Tachycardia in a Leisure-Time Triathlete: 6-Year Follow-Up. Diagnostics, 10(6), 391. https://doi.org/10.3390/diagnostics10060391