
Evaluation of the Advanta Dx SARS-CoV-2 RT-PCR Assay, a High-Throughput Extraction-Free Diagnostic Test for the Detection of SARS-CoV-2 in Saliva: A Diagnostic Accuracy Study

 ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Collection
2.3. Specimen Collection
2.4. Specimen Analysis
2.4.1. Advanta Dx SARS-CoV-2 RT-PCR Assay (Fluidigm)
2.4.2. Reference Standard
2.5. Sample Size Calculation
2.6. Data Analysis
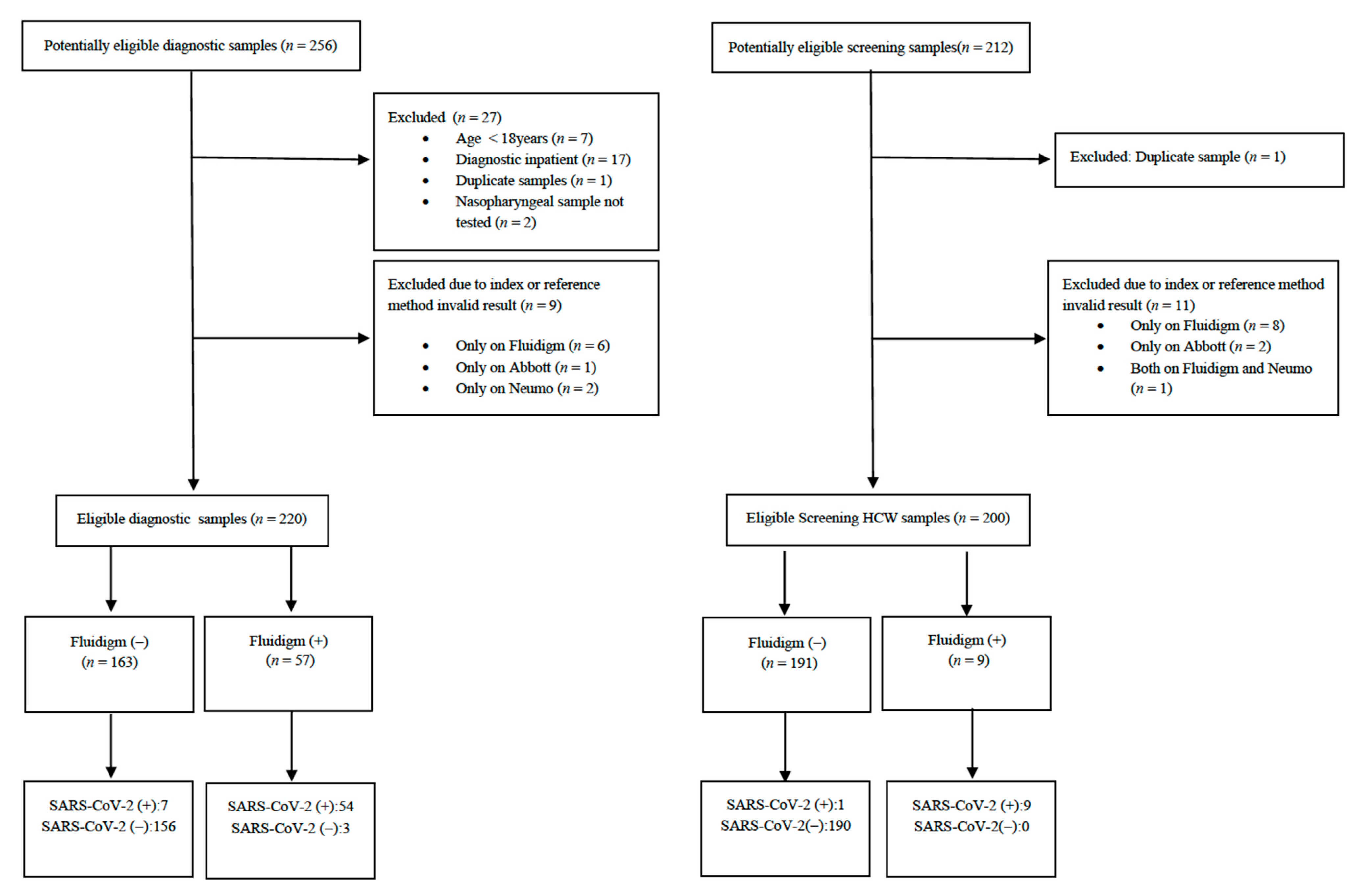
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mercer, T.R.; Salit, M. Testing at scale during the COVID-19 pandemic. Nat. Rev. Genet. 2021, 22, 415–426. [Google Scholar] [CrossRef] [PubMed]
- Interim Guidelines for Collecting and Handling of Clinical Specimens for COVID-19 Testing. Available online: https://www.cdc.gov/coronavirus/2019-ncov/lab/guidelines-clinical-specimens.html (accessed on 24 September 2021).
- Diagnostic Testing and Screening for SARS-CoV-2. Available online: https://www.ecdc.europa.eu/en/covid-19/latest-evidence/diagnostic-testing (accessed on 24 September 2021).
- European Centre for Disease Prevention and Control. Considerations for the Use of Saliva as Sample Material for COVID-19 Testing; ECDC: Stockholm, Sweden, 2021. [Google Scholar]
- Bossuyt, P.M.; Reitsma, J.B.; Bruns, D.E.; Gatsonis, C.A.; Glasziou, P.P.; Irwig, L.; Lijmer, J.G.; Moher, D.; Rennie, D.; de Vet, H.C.W.; et al. STARD 2015: An updated list of essential items for reporting diagnostic accuracy studies. BMJ 2015, 61, 1446–1452. [Google Scholar] [CrossRef] [Green Version]
- Fassy, J.; Lacoux, C.; Leroy, S.; Noussair, L.; Hubac, S.; Degoutte, A.; Vassaux, G.; Leclercq, V.; Rouquié, D.; Marquette, C.-H.; et al. Versatile and flexible microfluidic qPCR test for high-throughput SARS-CoV-2 and cellular response detection in nasopharyngeal swab samples. PLoS ONE 2021, 16, e0243333. [Google Scholar] [CrossRef] [PubMed]
- Nörz, D.; Fischer, N.; Schultze, A.; Kluge, S.; Mayer-Runge, U.; Aepfelbacher, M.; Pfefferle, S.; Lütgehetmann, M. Clinical evaluation of a SARS-CoV-2 RT-PCR assay on a fully automated system for rapid on-demand testing in the hospital setting. J. Clin. Virol. 2020, 128, 104390. [Google Scholar] [CrossRef] [PubMed]
- Harrington, A.; Cox, B.; Snowdon, J.; Bakst, J.; Ley, E.; Grajales, P.; Maggiore, J.; Kahn, S. Comparison of abbott ID now and abbott m2000 methods for the detection of SARS-CoV-2 from nasopharyngeal and nasal swabs from symptomatic patients. J. Clin. Microbiol. 2020, 58, e00798-20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buderer, N.M.F. Statistical methodology: I. incorporating the prevalence of disease into the sample size calculation for sensitivity and specificity. Acad. Emerg. Med. 1996, 3, 895–900. [Google Scholar] [CrossRef] [PubMed]
- Siettos, C.; Anastassopoulou, C.; Tsiamis, C.; Vrioni, G.; Tsakris, A. A bulletin from Greece: A health system under the pressure of the second COVID-19 wave. Pathog. Glob. Health 2021, 115, 133–134. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; R Core Team: Vienna, Austria, 2020. [Google Scholar]
- Dorai-Raj, S. Binom: Binomial Confidence Intervals for Several Parameterizations; R Package Version 1.1-1; R Core Team: Vienna, Austria, 2014. [Google Scholar]
- Revelle, W. psych: Procedures for Psychological, Psychometric, and Personality Research; R Package Version 2.1.9; Northwestern University: Evanston, IL, USA, 2021; Available online: https://CRAN.R-project.org/package=psych (accessed on 24 September 2021).
- Butler-Laporte, G.; Lawandi, A.; Schiller, I.; Yao, M.; Dendukuri, N.; McDonald, E.G.; Lee, T.C. Comparison of saliva and nasopharyngeal swab nucleic acid amplification testing for detection of SARS-CoV-2. JAMA Intern. Med. 2021, 181, 353. [Google Scholar] [CrossRef] [PubMed]
- Krause, P.R.; Fleming, T.R.; Longini, I.M.; Peto, R.; Briand, S.; Heymann, D.L.; Beral, V.; Snape, M.D.; Rees, H.; Ropero, A.-M.; et al. SARS-CoV-2 variants and vaccines. N. Engl. J. Med. 2021, 385, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Wyllie, A.L.; Fournier, J.; Casanovas-Massana, A.; Campbell, M.; Tokuyama, M.; Vijayakumar, P.; Geng, B.; Muenker, M.C.; Moore, A.; Vogels, C.; et al. Saliva is more sensitive for SARS-CoV-2 detection in COVID-19 patients than nasopharyngeal swabs. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Bastos, M.L.; Perlman-Arrow, S.; Menzies, D.; Campbell, J.R. The Sensitivity and Costs of Testing for SARS-CoV-2 Infection With Saliva Versus Nasopharyngeal Swabs: A Systematic Review and Meta-analysis. Ann. Intern. Med. 2021, 174, 501–510. [Google Scholar] [CrossRef] [PubMed]
- Gand, M.; Vanneste, K.; Thomas, I.; Van Gucht, S.; Capron, A.; Herman, P.; Roosens, N.H.C.; De Keersmaecker, S.C.J. Deepening of in silico evaluation of SARS-CoV-2 detection RT-qPCR assays in the context of new variants. Genes 2021, 12, 565. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Overall | NeuMoDx | Abbott | |
|---|---|---|---|
| Sample size | 420 | 133 | 287 |
| Mean Age (SD), years | 44.7 (13) | 43.6 (12.6) | 45.2 (13.2) |
| Gender, n (%) | |||
| Male | 161 (38.3%) | 49 (36.8%) | 112 (39%) |
| Female | 259 (61.7%) | 84 (63.2%) | 175 (61%) |
| Sample type, n (%) | |||
| Diagnostic | 220 (52.4%) | 58 (43.6%) | 162 (56.4%) |
| Screening | 200 (47.6%) | 75 (56.4%) | 125 (43.6%) |
| Patient Group | TP | FP | TN | FN | Sensitivity (95% CI) | Specificity (95% CI) | PPV (95% CI) | NPV (95% CI) |
|---|---|---|---|---|---|---|---|---|
| Diagnostic samples | 54 | 3 | 156 | 7 | 88.5% (77.8–95.3%) | 98.1% (94.6–99.6%) | 94.7% (85.4–98.9%) | 95.7% (91.4–98.3%) |
| Tested on NeuMoDx | 17 | 0 | 40 | 1 | 94.4% (72.7–99.9%) | 100%% (91.2–100%) | 100% (80.5–100%) | 97.6% (87.1–99.9%) |
| Tested on Abbott | 37 | 3 | 116 | 6 | 86% (72.1–94.7%) | 97.5% (92.8–99.5%) | 92.5% (79.6–98.4%) | 95.1% (89.6–98.2%) |
| Screening samples | 9 | 0 | 190 | 1 | 90% (55.5–99.7%) | 100% (98.1–100%) | 100% (66.4–100%) | 99.5% (97.1–100%) |
| Tested on NeuMo | 3 | 0 | 72 | 0 | 100% (29.2–100%) | 100% (95–100%) | 100% (29.2–100%) | 100% (95–100%) |
| Tested on Abbott | 6 | 0 | 118 | 1 | 85.7% (42.1–99.6%) | 100% (96.9–100%) | 100% (54.1–100%) | 99.2% (95.4–100%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Balaska, S.; Pilalas, D.; Takardaki, A.; Koutra, P.; Parasidou, E.; Gkeka, I.; Tychala, A.; Meletis, G.; Fyntanidou, B.; Metallidis, S.; et al. Evaluation of the Advanta Dx SARS-CoV-2 RT-PCR Assay, a High-Throughput Extraction-Free Diagnostic Test for the Detection of SARS-CoV-2 in Saliva: A Diagnostic Accuracy Study. Diagnostics 2021, 11, 1766. https://doi.org/10.3390/diagnostics11101766
Balaska S, Pilalas D, Takardaki A, Koutra P, Parasidou E, Gkeka I, Tychala A, Meletis G, Fyntanidou B, Metallidis S, et al. Evaluation of the Advanta Dx SARS-CoV-2 RT-PCR Assay, a High-Throughput Extraction-Free Diagnostic Test for the Detection of SARS-CoV-2 in Saliva: A Diagnostic Accuracy Study. Diagnostics. 2021; 11(10):1766. https://doi.org/10.3390/diagnostics11101766
Chicago/Turabian StyleBalaska, Sofia, Dimitrios Pilalas, Anna Takardaki, Paraskevoula Koutra, Eleftheria Parasidou, Ioanna Gkeka, Areti Tychala, Georgios Meletis, Barbara Fyntanidou, Simeon Metallidis, and et al. 2021. "Evaluation of the Advanta Dx SARS-CoV-2 RT-PCR Assay, a High-Throughput Extraction-Free Diagnostic Test for the Detection of SARS-CoV-2 in Saliva: A Diagnostic Accuracy Study" Diagnostics 11, no. 10: 1766. https://doi.org/10.3390/diagnostics11101766
APA StyleBalaska, S., Pilalas, D., Takardaki, A., Koutra, P., Parasidou, E., Gkeka, I., Tychala, A., Meletis, G., Fyntanidou, B., Metallidis, S., Protonotariou, E., & Skoura, L. (2021). Evaluation of the Advanta Dx SARS-CoV-2 RT-PCR Assay, a High-Throughput Extraction-Free Diagnostic Test for the Detection of SARS-CoV-2 in Saliva: A Diagnostic Accuracy Study. Diagnostics, 11(10), 1766. https://doi.org/10.3390/diagnostics11101766