
Performance of a Surrogate SARS-CoV-2-Neutralizing Antibody Assay in Natural Infection and Vaccination Samples

 , , , ,
, , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Collection and Ethical Approval
2.2. Chemiluminescent Microparticle Immunoassay
2.3. Live Virus Microneutralization
2.4. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Coronavirus disease (COVID-19) Pandemic. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019?adgroupsurvey={adgroupsurvey}&gclid=CjwKCAjw0qOIBhBhEiwAyvVcf6iRNGo9p7bc5u7WGTCMJ7-Ca7W0PGNGSZXRmT-bkkBQlPknYd8vlxoCb9QQAvD_BwE (accessed on 31 July 2021).
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.-H.; Nitsche, A.; et al. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell 2020, 181, 271–280.e8. [Google Scholar] [CrossRef] [PubMed]
- Tay, M.Z.; Poh, C.M.; Rénia, L.; Macary, P.A.; Ng, L.F.P. The trinity of COVID-19: Immunity, inflammation and intervention. Nat. Rev. Immunol. 2020, 20, 363–374. [Google Scholar] [CrossRef] [PubMed]
- The Government of the Hong Kong Special Administrative Region. COVID-19 Vaccination Program Officially Launched. Available online: https://www.info.gov.hk/gia/general/202102/26/P2021022600815.htm (accessed on 7 August 2021).
- Wu, Z.; Hu, Y.; Xu, M.; Chen, Z.; Yang, W.; Jiang, Z.; Li, M.; Jin, H.; Cui, G.; Chen, P.; et al. Safety, tolerability, and immunogenicity of an inactivated SARS-CoV-2 vaccine (CoronaVac) in healthy adults aged 60 years and older: A randomised, double-blind, placebo-controlled, phase 1/2 clinical trial. Lancet Infect. Dis. 2021, 21, 803–812. [Google Scholar] [CrossRef]
- Xia, S.; Duan, K.; Zhang, Y.; Zhao, D.; Zhang, H.; Xie, Z.; Li, X.; Peng, C.; Zhang, Y.; Zhang, W.; et al. Effect of an Inactivated Vaccine Against SARS-CoV-2 on Safety and Immunogenicity Outcomes: Interim Analysis of 2 Randomized Clinical Trials. JAMA 2020, 324, 951–960. [Google Scholar] [CrossRef] [PubMed]
- Alberer, M.; Gnad-Vogt, U.; Hong, H.S.; Mehr, K.T.; Backert, L.; Finak, G.; Gottardo, R.; Bica, M.A.; Garofano, A.; Koch, S.D.; et al. Safety and immunogenicity of a mRNA rabies vaccine in healthy adults: An open-label, non-randomised, prospective, first-in-human phase 1 clinical trial. Lancet 2017, 390, 1511–1520. [Google Scholar] [CrossRef]
- Feng, L.; Wang, Q.; Shan, C.; Yang, C.; Feng, Y.; Wu, J.; Liu, X.; Zhou, Y.; Jiang, R.; Hu, P.; et al. An adenovirus-vectored COVID-19 vaccine confers protection from SARS-CoV-2 challenge in rhesus macaques. Nat. Commun. 2020, 11, 4207. [Google Scholar] [CrossRef] [PubMed]
- Browning, S.L.; Gormally, M.; Briggs, N.; Li, M.; Zakko, A.; Laurent-Rolle, M.; Ladines-Lim, J.; Morrison, B.A.; Kandel, P.; Khan, M.; et al. Use of Convalescent Plasma Therapy in Severe Coronavirus Disease 2019: The Yale-New Haven Health System Experience. Blood 2020, 136, 39–40. [Google Scholar] [CrossRef]
- Perera, R.A.P.M.; Ko, R.; Tsang, O.T.Y.; Hui, D.S.C.; Kwan, M.Y.M.; Brackman, C.J.; To, E.M.W.; Yen, H.-L.; Leung, K.; Cheng, S.M.S.; et al. Evaluation of a SARS-CoV-2 Surrogate Virus Neutralization Test for Detection of Antibody in Human, Canine, Cat, and Hamster Sera. J. Clin. Microbiol. 2021, 59, 02504–02520. [Google Scholar] [CrossRef] [PubMed]
- Pan, Y.; Jiang, X.; Yang, L.; Chen, L.; Zeng, X.; Liu, G.; Tang, Y.; Qian, C.; Wang, X.; Cheng, F.; et al. SARS-CoV-2-specific immune response in COVID-19 convalescent individuals. Signal Transduct. Target. Ther. 2021, 6, 1–10. [Google Scholar] [CrossRef]
- Favresse, J.; Gillot, C.; Di Chiaro, L.; Eucher, C.; Elsen, M.; Van Eeckhoudt, S.; David, C.; Morimont, L.; Dogné, J.-M.; Douxfils, J. Neutralizing Antibodies in COVID-19 Patients and Vaccine Recipients after Two Doses of BNT162b2. Viruses 2021, 13, 1364. [Google Scholar] [CrossRef] [PubMed]
- To, K.K.-W.; Tsang, O.T.-Y.; Leung, W.-S.; Tam, A.R.; Wu, T.-C.; Lung, D.C.; Yip, C.C.-Y.; Cai, J.-P.; Chan, J.M.-C.; Chik, T.S.-H.; et al. Temporal profiles of viral load in posterior oropharyngeal saliva samples and serum antibody responses during infection by SARS-CoV-2: An observational cohort study. Lancet Infect. Dis. 2020, 20, 565–574. [Google Scholar] [CrossRef] [Green Version]
- Kristiansen, P.A.; Page, M.; Bernasconi, V.; Mattiuzzo, G.; Dull, P.; Makar, K.; Plotkin, S.; Knezevic, I. WHO International Standard for anti-SARS-CoV-2 immunoglobulin. Lancet 2021, 397, 1347–1348. [Google Scholar] [CrossRef]
- National Center for Biotechnology Information. Gene: ACE2, Angiotensin I Converting Enzyme 2. U.S. National Library of Medicine. Updated on 28 February 2020. Available online: https://www.ncbi.nlm.nih.gov/gene?Db=gene&Cmd=DetailsSearch&Term=59272 (accessed on 9 August 2021).
- Lim, W.W.; Mak, L.; Leung, G.M.; Cowling, B.J.; Peiris, M. Comparative immunogenicity of mRNA and inactivated vaccines against COVID-19. Lancet Microbe 2021. [Google Scholar] [CrossRef]



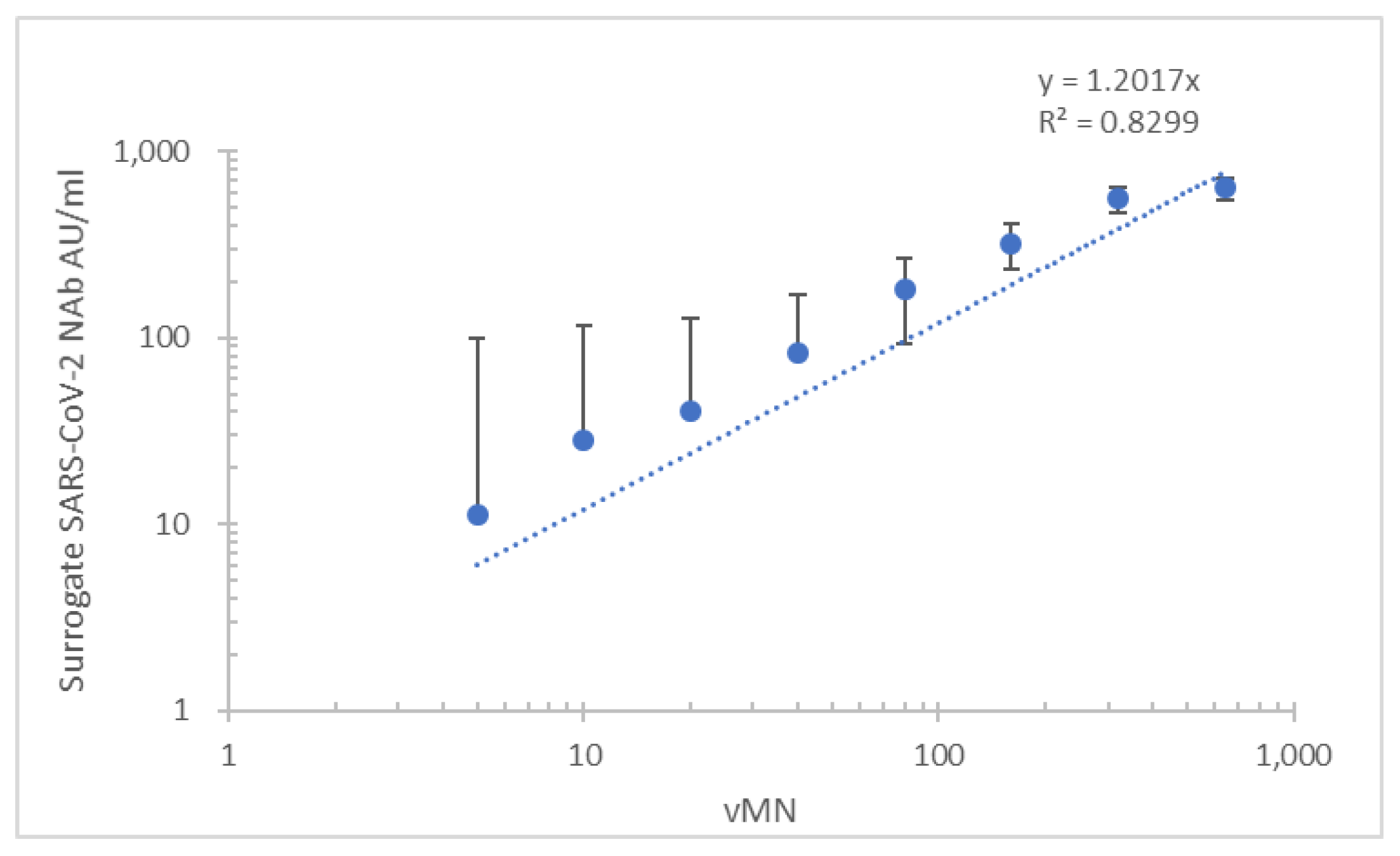{kind=link}
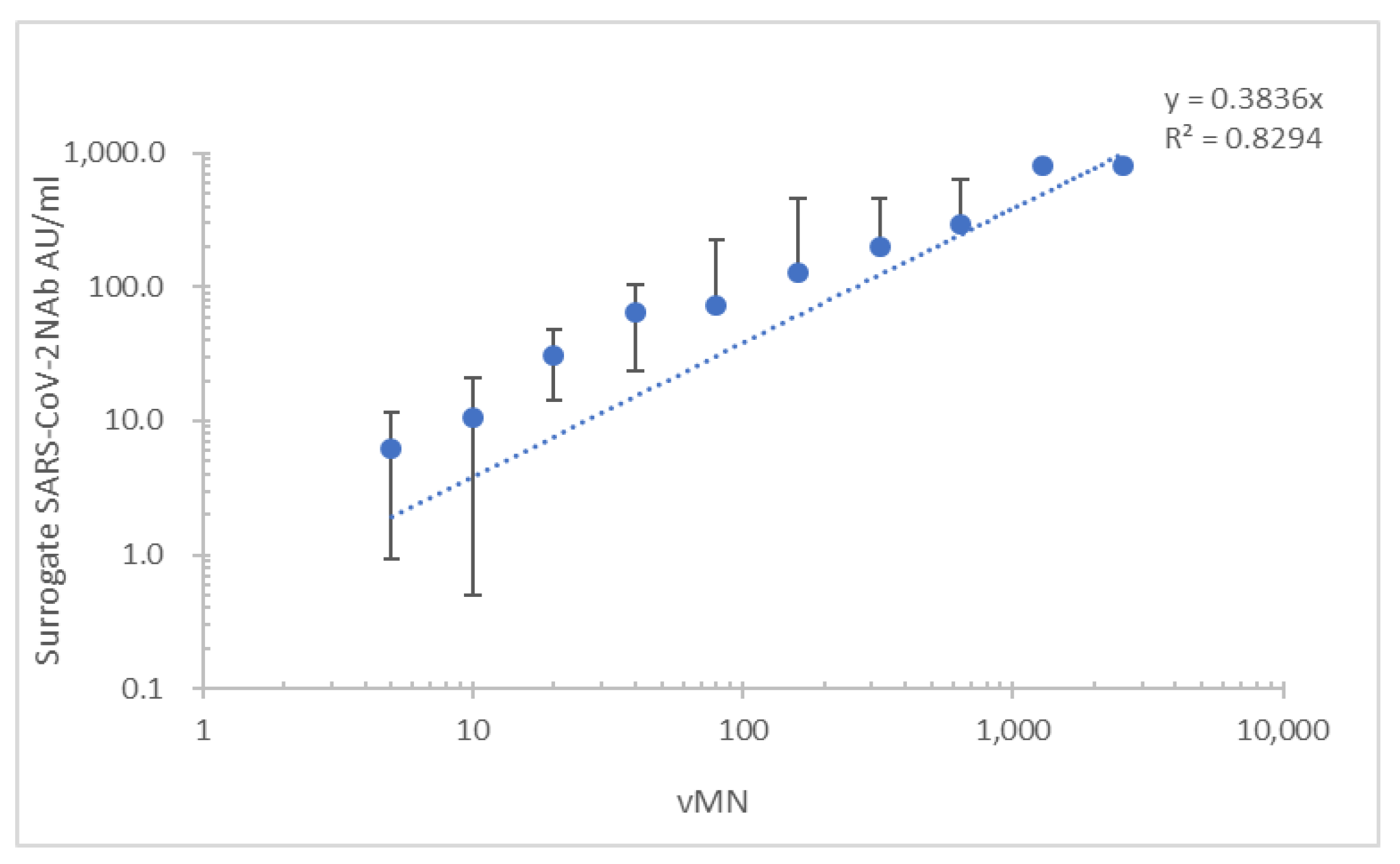{kind=link}
| Sensitivity | Specificity | Positive Predictive Value | Negative Predictive Value | |
|---|---|---|---|---|
| Surrogate NAb | 97.9% | 94.9% | 98.2% | 93.8% |
| (95% CI, Lower-Upper limit) | (0.95–0.99) | (0.88–0.98) | (0.96–0.99) | (0.87–0.97) |
| Vaccine | Number | Mean of sNAb (AU/mL) | SD | GM of vMN (Titers) | SD |
|---|---|---|---|---|---|
| BNT162b2 | 49 | 643.1 | 244.1 | 248.1 | 3.2 |
| Sinovac | 15 | 47.7 | 37.1 | 28.9 | 2.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chan, K.-H.; Leung, K.-Y.; Zhang, R.-R.; Liu, D.; Fan, Y.; Chen, H.; Yuen, K.-Y.; Hung, I.F.-N. Performance of a Surrogate SARS-CoV-2-Neutralizing Antibody Assay in Natural Infection and Vaccination Samples. Diagnostics 2021, 11, 1757. https://doi.org/10.3390/diagnostics11101757
Chan K-H, Leung K-Y, Zhang R-R, Liu D, Fan Y, Chen H, Yuen K-Y, Hung IF-N. Performance of a Surrogate SARS-CoV-2-Neutralizing Antibody Assay in Natural Infection and Vaccination Samples. Diagnostics. 2021; 11(10):1757. https://doi.org/10.3390/diagnostics11101757
Chicago/Turabian StyleChan, Kwok-Hung, Ka-Yi Leung, Ricky-Ruiqi Zhang, Danlei Liu, Yujing Fan, Honglin Chen, Kwok-Yung Yuen, and Ivan Fan-Ngai Hung. 2021. "Performance of a Surrogate SARS-CoV-2-Neutralizing Antibody Assay in Natural Infection and Vaccination Samples" Diagnostics 11, no. 10: 1757. https://doi.org/10.3390/diagnostics11101757
APA StyleChan, K. -H., Leung, K. -Y., Zhang, R. -R., Liu, D., Fan, Y., Chen, H., Yuen, K. -Y., & Hung, I. F. -N. (2021). Performance of a Surrogate SARS-CoV-2-Neutralizing Antibody Assay in Natural Infection and Vaccination Samples. Diagnostics, 11(10), 1757. https://doi.org/10.3390/diagnostics11101757