
End-Tidal Carbon Dioxide Pressure Measurement after Prolonged Inspiratory Time Gives a Good Estimation of the Arterial Carbon Dioxide Pressure in Mechanically Ventilated Patients

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Protocol
2.3. Other Collected Data
2.4. Statistical Analysis
3. Results
3.1. Population
3.2. Student’s t-Tests
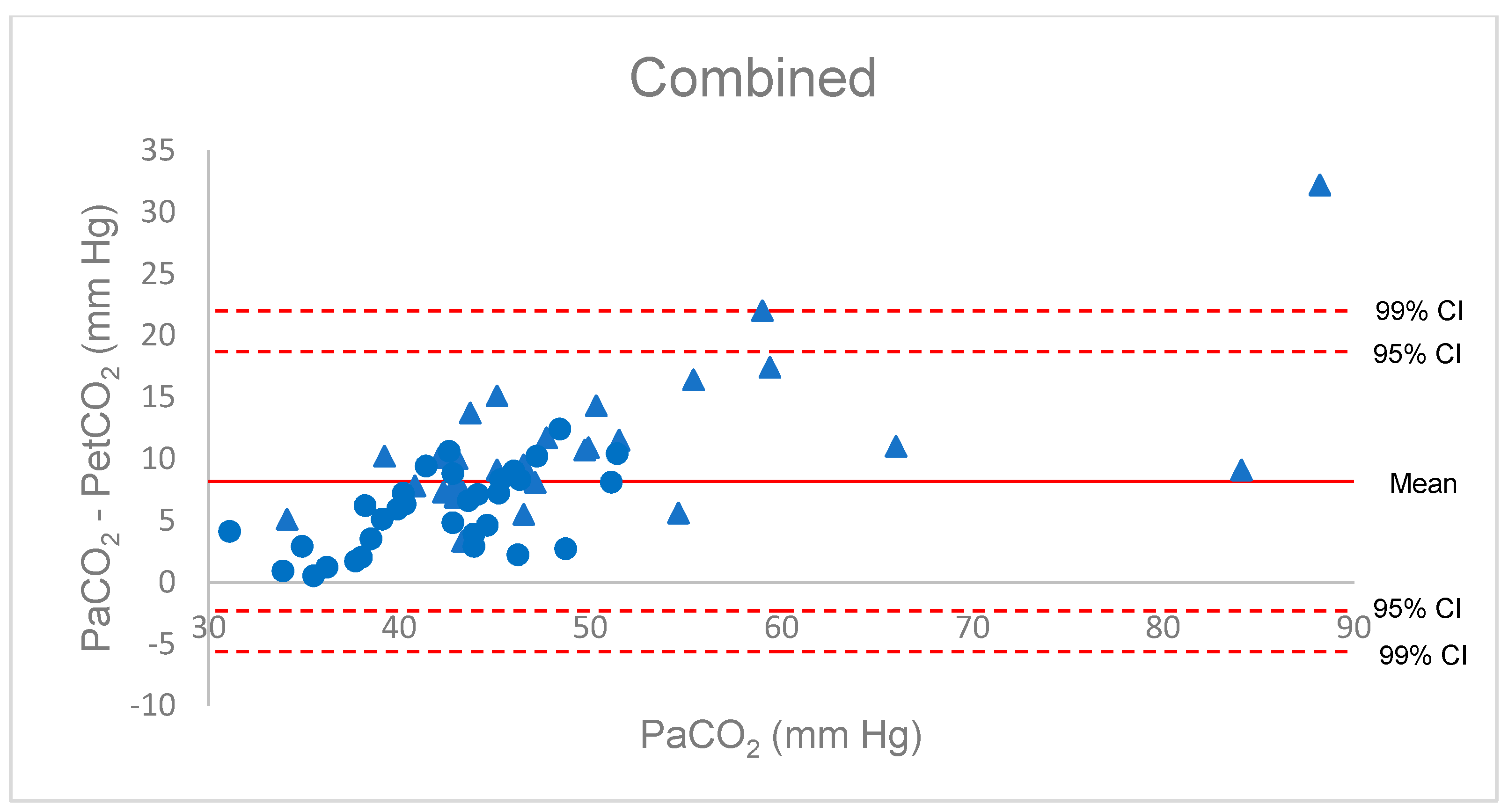
3.3. Bland–Altman Dispersion
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Maiese, A.; Manetti, A.C.; La Russa, R.; Di Paolo, M.; Turillazzi, E.; Frati, P.; Fineschi, V. Autopsy findings in COVID-19-related deaths: A literature review. Forensic Sci. Med. Pathol. 2021, 17, 279–296. [Google Scholar] [CrossRef] [PubMed]
- Raemer, D.B.; Francis, D.; Philip, J.H.; Gabel, R.A. Variation in PCO2 between arterial blood and peak expired gas during anesthesia. Anesth. Analg. 1983, 62, 1065–1069. [Google Scholar] [CrossRef]
- Belpomme, V.; Ricard-Hibon, A.; Devoir, C.; Dileseigres, S.; Devaud, M.L.; Chollet, C.; Marty, J. Correlation of arterial PCO2 and PETCO2 in prehospital controlled ventilation. Am. J. Emerg. Med. 2005, 23, 852–859. [Google Scholar] [CrossRef]
- Strang, C.M.; Hachenberg, T.; Fredén, F.; Hedenstierna, G. Development of atelectasis and arterial to end-tidal PCO2-difference in a porcine model of pneumoperitoneum. Br. J. Anaesth. 2009, 103, 298–303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Law, G.T.S.; Wong, C.Y.; Kwan, C.W.; Wong, K.Y.; Wong, F.P.; Tse, H.N. Concordance between side-stream end-tidal carbon dioxide and arterial carbon dioxide partial pressure in respiratory service setting. Hong Kong Med. J. 2009, 15, 440–446. [Google Scholar]
- Defilippis, V.; D’Antini, D.; Cinnella, G.; Dambrosio, M.; Schiraldi, F.; Procacci, V. End-tidal arterial CO2 partial pressure gradient in patients with severe hypercapnia undergoing noninvasive ventilation. Open Access Emerg. Med. 2013, 5, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hardman, J.G.; Aitkenhead, A.R. Estimating alveolar dead space from the arterial to end-tidal CO2 gradient: A modeling analysis. Anesth. Analg. 2003, 97, 1846–1851. [Google Scholar] [CrossRef] [PubMed]
- Long, B.; Koyfman, A.; Vivirito, M.A. Capnography in the Emergency Department: A Review of Uses, Waveforms, and Limitations. J. Emerg. Med. 2017, 53, 829–842. [Google Scholar] [CrossRef]
- Tavernier, B.; Rey, D.; Thevenin, D.; Triboulet, J.P.; Scherpereel, P. Can prolonged expiration manoeuvres improve the prediction of arterial PCO2 from end-tidal PCO2? Br. J. Anaesth. 1997, 78, 536–540. [Google Scholar] [CrossRef]
- ARDS Definition Task Force; Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. Acute respiratory distress syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar] [CrossRef]
- Losa-Reyna, J.; Torres-Peralta, R.; Henriquez, J.J.G.; Calbet, J.A.L. Arterial to end-tidal Pco2 difference during exercise in normoxia and severe acute hypoxia: Importance of blood temperature correction. Physiol. Rep. 2015, 3, e12512. [Google Scholar] [CrossRef]
- Fineschi, V.; Aprile, A.; Aquila, I.; Arcangeli, M.; Asmundo, A.; Bacci, M.; Cingolani, M.; Cipolloni, L.; D’Errico, S.; De Casamassimi, I.; et al. Management of the corpse with suspect, probable or confirmed COVID-19 respiratory infection—Italian interim recommendations for personnel potentially exposed to material from corpses, including body fluids, in morgue structures and during autopsy practice. Pathologica 2020, 112, 64–77. [Google Scholar] [CrossRef]
- Liu, S.Y.; Lee, T.S.; Bongard, F. Accuracy of capnography in nonintubated surgical patients. Chest 1992, 102, 1512–1515. [Google Scholar] [CrossRef] [PubMed]
- Casati, A.; Salvo, I.; Torri, G.; Calderini, E. Arterial to end-tidal carbon dioxide gradient and physiological dead space monitoring during general anaesthesia: Effects of patients’ position. Minerva Anestesiol. 1997, 63, 177–182. [Google Scholar]
- Yousuf, T.; Brinton, T.; Murtaza, G.; Wozniczka, D.; Ahmad, K.; Iskandar, J.; Mehta, R.; Keshmiri, H.; Hanif, T. Establishing a gradient between partial pressure of arterial carbon dioxide and end-tidal carbon dioxide in patients with acute respiratory distress syndrome. J. Investig. Med. 2017, 65, 338–341. [Google Scholar] [CrossRef]
- Hinkelbein, J.; Floss, F.; Denz, C.; Krieter, H. Accuracy and precision of three different methods to determine Pco2 (Paco2 vs. Petco2 vs. Ptcco2) during interhospital ground transport of critically ill and ventilated adults. J. Trauma Acute Care Surg. 2008, 65, 10–18. [Google Scholar] [CrossRef]
- Nassar, B.S.; Schmidt, G.A. Estimating Arterial Partial Pressure of Carbon Dioxide in Ventilated Patients: How Valid Are Surrogate Measures? Ann. Am. Thorac. Soc. 2017, 14, 1005–1014. [Google Scholar] [CrossRef]
- Fox, B.D.; Joyal, D.; Schlesinger, R.D.; Eisenberg, M.J.; Langleben, D. Evaluation of the MicrostatTM sublingual PCO2 monitor in ambulatory patients. J. Clin. Monit. Comput. 2016, 30, 77–80. [Google Scholar] [CrossRef] [PubMed]
- Robbins, P.A.; Conway, J.; Cunningham, D.A.; Khamnei, S.; Paterson, D.J. A comparison of indirect methods for continuous estimation of arterial PCO2 in men. J. Appl. Physiol. 1990, 68, 1727–1731. [Google Scholar] [CrossRef] [PubMed]
- Fierstra, J.; Machina, M.; Battisti-Charbonney, A.; Duffin, J.; Fisher, J.A.; Minkovich, L. End-inspiratory rebreathing reduces the end-tidal to arterial PCO2 gradient in mechanically ventilated pigs. Intensive Care Med. 2011, 37, 1543–1550. [Google Scholar] [CrossRef]
- Chan, K.L.; Chan, M.T.V.; Gin, T. Mainstream vs. sidestream capnometry for prediction of arterial carbon dioxide tension during supine craniotomy. Anaesthesia 2003, 58, 149–155. [Google Scholar] [CrossRef]
- Kasuya, Y.; Akça, O.; Sessler, D.I.; Ozaki, M.; Komatsu, R. Accuracy of postoperative end-tidal Pco2 measurements with mainstream and sidestream capnography in non-obese patients and in obese patients with and without obstructive sleep apnea. Anesthesiology 2009, 111, 609–615. [Google Scholar] [CrossRef] [Green Version]
- Duyu, M.; Çağlar, Y.M.; Karakaya, Z.; Aslan, M.U.; Yılmaz, S.; Leblebici, A.N.; Bektaş, A.D.; Bahar, M.; Yersel, M.N. Comparison of arterial CO2 estimation by end-tidal and transcutaneous CO2 measurements in intubated children and variability with subject related factors. J. Clin. Monit. Comput. 2021, 35, 101–111. [Google Scholar] [CrossRef]
- From, R.P.; Scamman, F.L. Ventilatory frequency influences accuracy of end-tidal CO2 measurements. Analysis of seven capnometers. Anesth. Analg. 1988, 67, 884–886. [Google Scholar] [CrossRef] [PubMed]
- Sturesson, L.W.; Malmkvist, G.; Allvin, S.; Collryd, M.; Bodelsson, M.; Jonson, B. An appropriate inspiratory flow pattern can enhance CO2 exchange, facilitating protective ventilation of healthy lungs. Br. J. Anaesth. 2016, 117, 243–249. [Google Scholar] [CrossRef] [Green Version]
- Bhavani-Shankar, K. Negative arterial to end-tidal CO2 gradients in children. Can. J. Anaesth. 1994, 41, 1125–1126. [Google Scholar] [CrossRef] [Green Version]
- Campbell, F.A.; McLeod, M.E.; Bissonnette, B.; Swartz, J.S. End-tidal carbon dioxide measurement in infants and children during and after general anaesthesia. Can. J. Anaesth. 1994, 41, 107–110. [Google Scholar] [CrossRef] [Green Version]
- Fletcher, R.; Jonson, B. Deadspace and the single breath test for carbon dioxide during anaesthesia and artificial ventilation. Effects of tidal volume and frequency of respiration. Br. J. Anaesth. 1984, 56, 109–119. [Google Scholar] [CrossRef] [PubMed]
- Jaffe, M.B. Respiratory Gas Analysis-Technical Aspects. Anesth. Analg. 2018, 126, 839–845. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| COVID | Anaesthesia | |
|---|---|---|
| Measure (n) | 35 | 32 |
| % male (M/F ratio) | 0.29 (2/5) | 0.41 (11/16) |
| Mean Age (years) (range) | 65 (59–73) | 59 (23–78) |
| Ventilator (n) | ||
| Evita | 20 (5) | 0 |
| Perseus | 12 (2) | 30 (24) |
| Zeus | 0 | 5 (3) |
| Type of manoeuvre (n) | ||
| Increased inspiratory pause | 35 | 27 |
| Recruitment | 0 | 5 |
| Heart rate (bpm) (SD) | 82 (13) | 78 (13) |
| MAP (mm Hg) (SD) | 81 (13) | 78 (14) |
| Norepinephrine (mg h−1) | 0.21 (0.46) | 0.24 (0.88) |
| Temperature (°C) (SD) | 37 (0.69) | 36 (0.71) |
| PaCO2 (mm Hg) (SD) | 49.3 (11) | 42.2 (5.0) * |
| PaCO2 (n) | ||
| ≤35 mm Hg | 1 | 3 |
| 35 to ≤45 mm Hg | 13 | 19 |
| ≥45 mm Hg | 21 | 10 |
| Compliance (mL cm H2O−1) | 24 (9.8) | 72 (86) * |
| PaO2/FiO2 (mm Hg) (SD) | 224 (53) | 367 (110) * |
| Gradient | COVID | Anaesthesia | Combined | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | p-Value | Mean | SD | p-Value | Mean | SD | p-Value | |
| PaCO2 | 49 | 11 | 42 | 5.0 | 46 | 5.1 | |||
| PetCO2 | 39 | 9 | 37 | 4.0 | 38 | 7.3 | |||
| PACO2 | 51 | 11 | 44 | 4.7 | 46 | 4.6 | |||
| D(a-et)CO2 | +11 | 5.7 | <0.001 | +5.7 | 3.4 | <0.001 | +8.2 | 5.4 | <0.001 |
| D(a-A)CO2 | −1.2 | 3.3 | 0.043 | −1.9 | 3.3 | <0.003 | −1.5 | 3.3 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salomé, A.; Stoclin, A.; Motamed, C.; Sitbon, P.; Bourgain, J.-L. End-Tidal Carbon Dioxide Pressure Measurement after Prolonged Inspiratory Time Gives a Good Estimation of the Arterial Carbon Dioxide Pressure in Mechanically Ventilated Patients. Diagnostics 2021, 11, 2219. https://doi.org/10.3390/diagnostics11122219
Salomé A, Stoclin A, Motamed C, Sitbon P, Bourgain J-L. End-Tidal Carbon Dioxide Pressure Measurement after Prolonged Inspiratory Time Gives a Good Estimation of the Arterial Carbon Dioxide Pressure in Mechanically Ventilated Patients. Diagnostics. 2021; 11(12):2219. https://doi.org/10.3390/diagnostics11122219
Chicago/Turabian StyleSalomé, Arthur, Annabelle Stoclin, Cyrus Motamed, Philippe Sitbon, and Jean-Louis Bourgain. 2021. "End-Tidal Carbon Dioxide Pressure Measurement after Prolonged Inspiratory Time Gives a Good Estimation of the Arterial Carbon Dioxide Pressure in Mechanically Ventilated Patients" Diagnostics 11, no. 12: 2219. https://doi.org/10.3390/diagnostics11122219
APA StyleSalomé, A., Stoclin, A., Motamed, C., Sitbon, P., & Bourgain, J. -L. (2021). End-Tidal Carbon Dioxide Pressure Measurement after Prolonged Inspiratory Time Gives a Good Estimation of the Arterial Carbon Dioxide Pressure in Mechanically Ventilated Patients. Diagnostics, 11(12), 2219. https://doi.org/10.3390/diagnostics11122219