
Dilated Odontoma Arising in the Mandibular Third Molar Germ: Report of a Case of an Unusual Lesion in an Uncommon Site

 ,
,  ,
,  and
and
Abstract
:1. Introduction
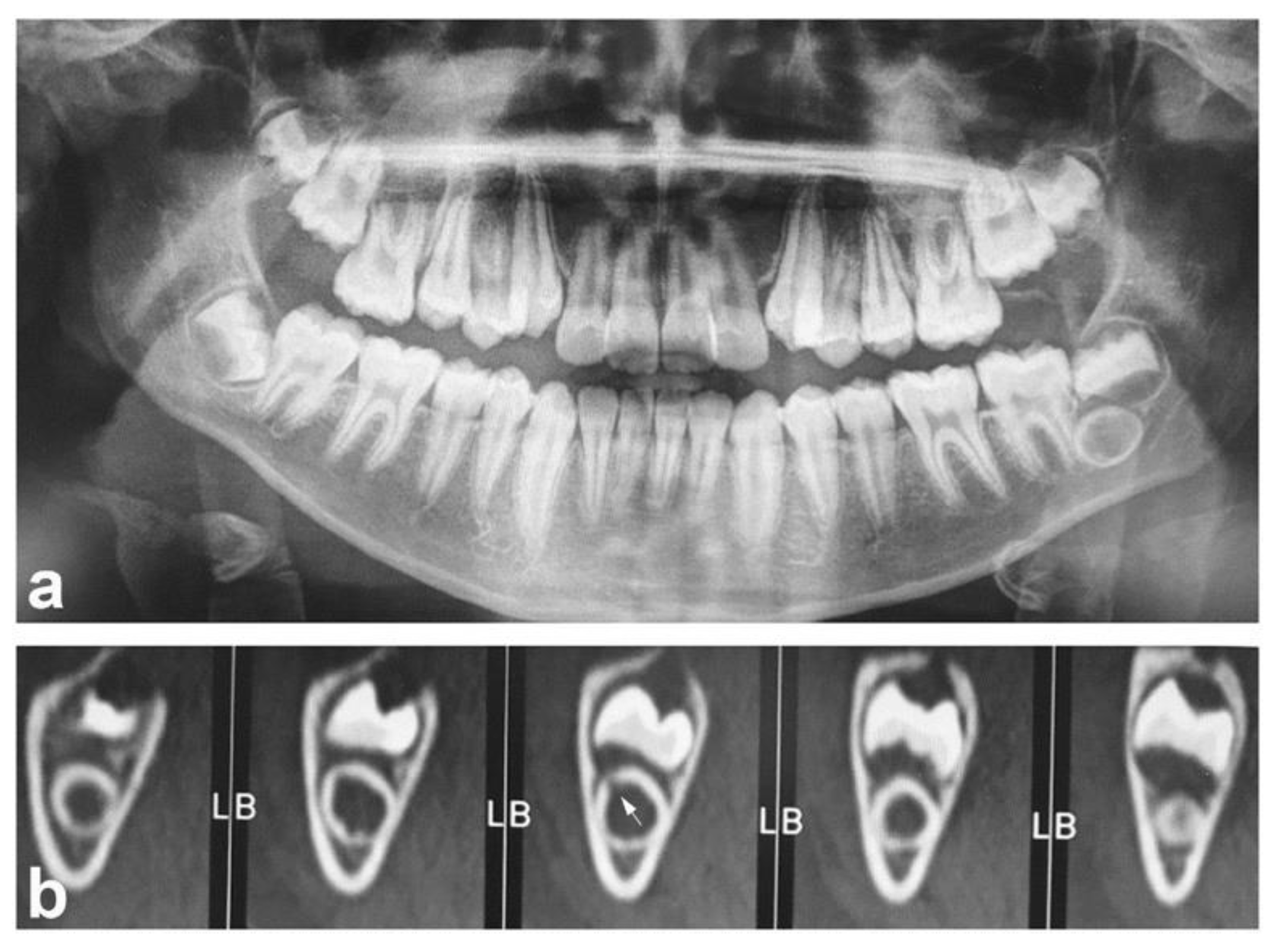
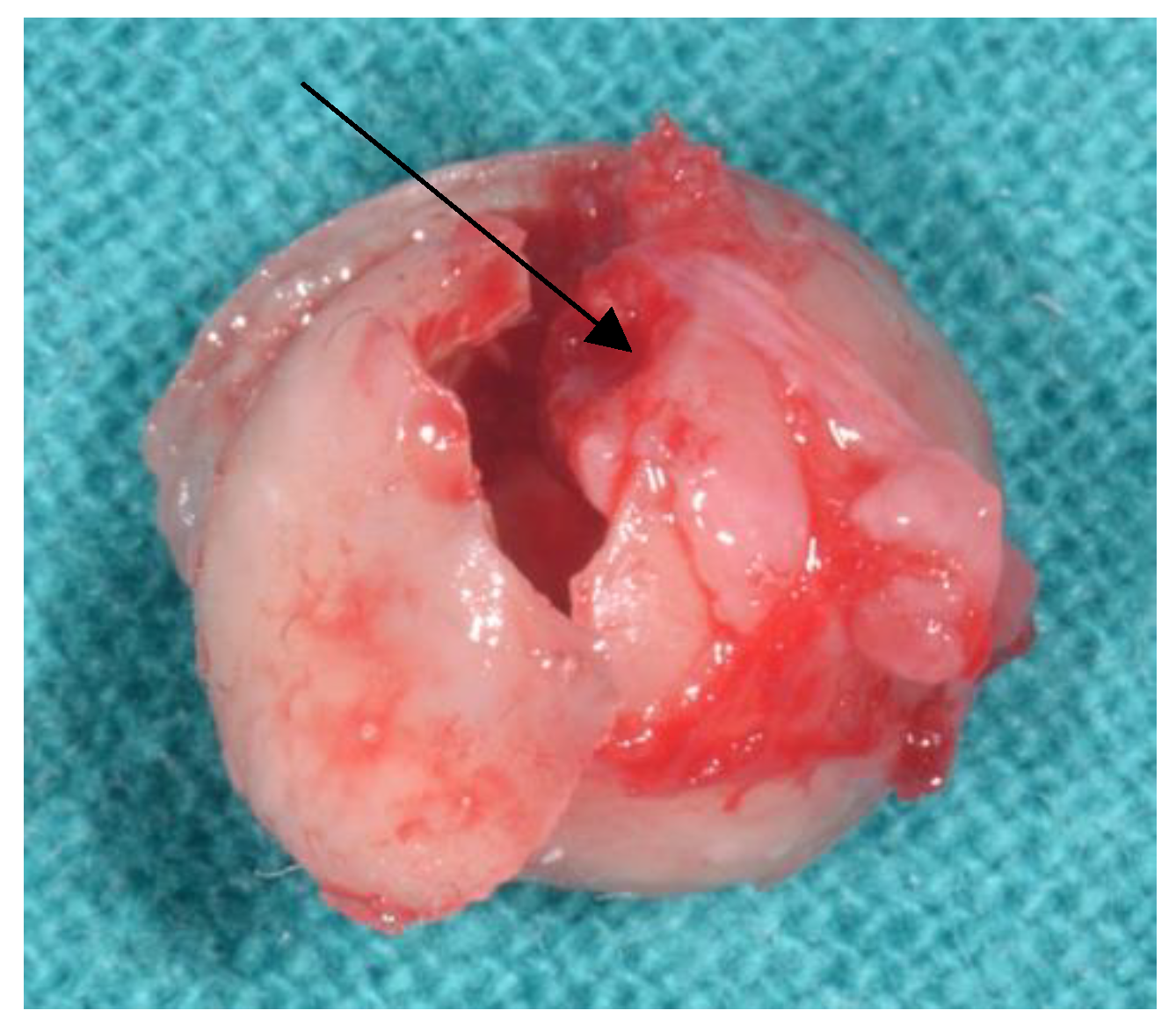
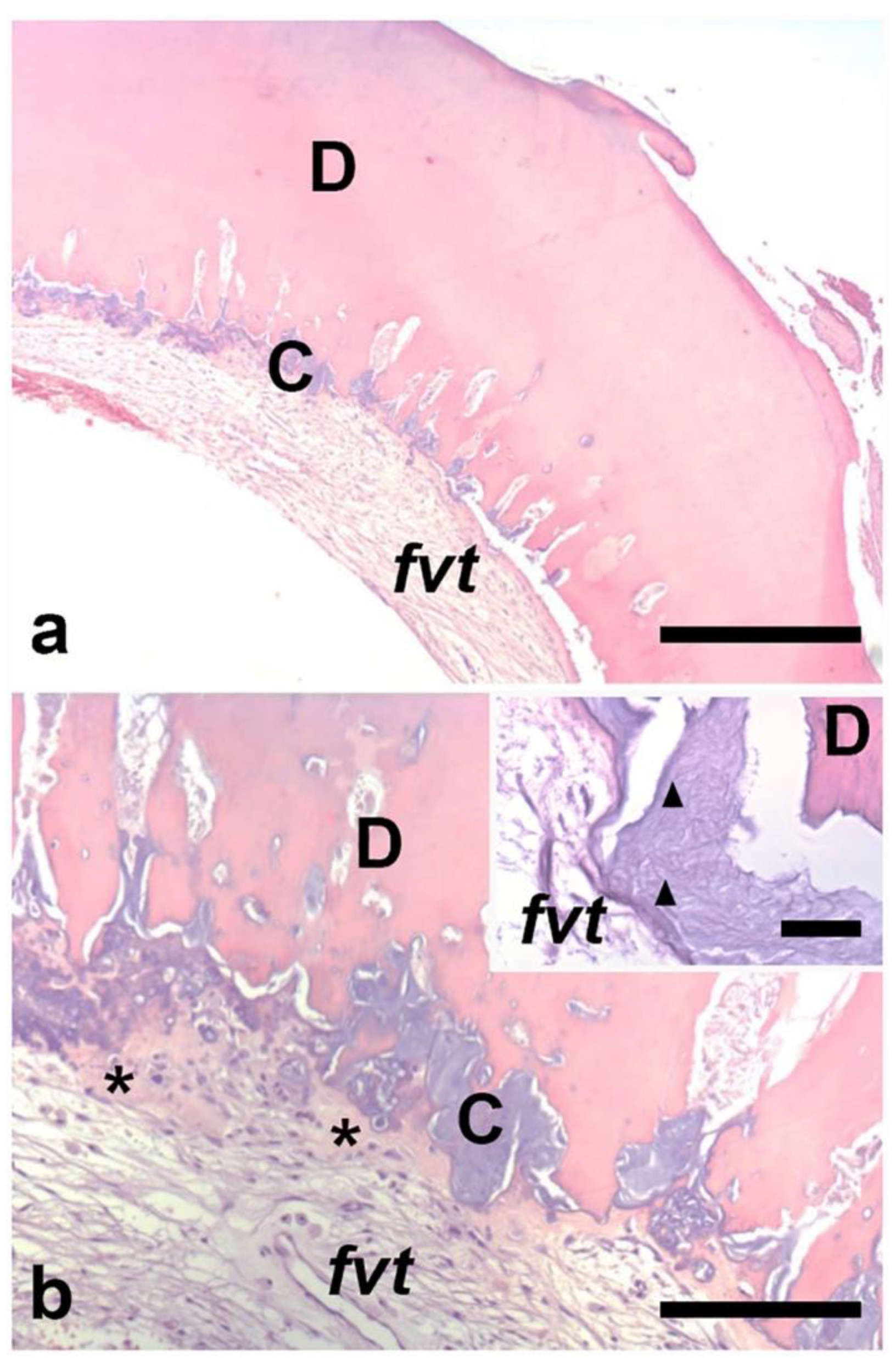
2. Case Report
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jaya, R.; Mohan Kumar, R.S.; Srinivasan, R. A rare case of dilated invaginated odontome with talon cusp in a permanent maxillary central incisor diagnosed by cone beam computed tomography. Imaging Sci. Dent. 2013, 43, 209–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsusue, Y.; Yamamoto, K.; Inagake, K.; Kirita, T. A dilated odontoma in the second molar region of the mandible. Open Dent. J. 2011, 5, 150–153. [Google Scholar] [CrossRef] [PubMed]
- Galvez, P.; Garot, E.; Bres, A.; Crelier, A.; Castain, C.; Catros, S.; Fenelon, M. Dilated odontoma: An unusual case report and literature review. J. Oral Med. Oral Surg. 2021, 27, 24. [Google Scholar] [CrossRef]
- White, S.C.; Pharoah, M.J. Oral Radiology: Principles and Interpretation, 5th ed.; Mosby: St. Louis, MO, USA, 2004. [Google Scholar]
- Oehlers, F.A.C. Dens invaginatus (dilated composite odontome) I. Variations of the invagination process and associated anterior crown forms. Oral Surg. Oral Med. Oral Pathol. 1957, 10, 1204–1218. [Google Scholar] [CrossRef]
- Rushton, M.A. A collection of dilated composite odontomes. Br. Dent. J. 1937, 63, 65–86. [Google Scholar]
- Oehlers, F.A.C. Dens invaginatus (dilated composite odontome). II. Associated posterior crown forms and pathogenesis. Oral Surg. Oral Med. Oral Pathol. 1957, 10, 1302–1316. [Google Scholar] [CrossRef]
- Cuković-Bagić, I.; Macan, D.; Dumancić, J.; Manojlović, S.; Hat, J. Dilated odontome in the mandibular third molar region. Oral Surg. Oral Med. Oral Pathol. Oral Pathol. Endod. 2010, 109, 109–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Almeida, B.; Silva, A.; Pereira, M.; Silva, M.; Nunes, S. Case report of a dilated odontome in the posterior mandible. Int. J. Surg. Case Rep. 2016, 20, 14–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jayachandran, S.; Kayal, L.; Sharma, A.; Priyanka, K. Dilated odontoma: A report of two cases from a radiological perspective. Contemp. Clin. Dent. 2016, 7, 107–110. [Google Scholar] [PubMed]
- Sharma, G.; Nagra, A.; Singh, G.; Nagpal, A.; Soin, A.; Bhardwaj, V. An erupted dilated odontoma: A rare presentation. Case Rep. Dent. 2016, 2016, 9750947. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dental Radiographic Examination: Reccomendations for Patient Selection and Limiting Radiatione Exposure. American Dental Association (Council on Scientific Affairs). Available online: https://www.ada.org/-/media/project/ada-organization/ada/ada-org/ada/ada/publications/ada-news/files/dental_radiographic_examinations_2012.pdf?rev=496a9ceb48a1405f9a8008abc0de745c&hash=7C8A3F99EF8E6DA58E5A2E9DF59B3FD4 (accessed on 6 November 2021).
- Wall, A.; Ng, S.; Djemal, S. The value of cone beam CT in assessing and managing a dilated odontome of a maxillary canine. Dent. Update 2015, 42, 126–128. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, T.; Seto, K. Histopathological Studies of Four Cases of Dilated Odontoma. Oral Med. Pathol. 1996, 1, 56–59. [Google Scholar] [CrossRef] [Green Version]
- Coria-Bello, M.; Morales-González, F.J. Dens invaginatus u odontoma dilatado, a definition controversy. A literature review. Rev. Científica Odontol. 2021, 9, e061. [Google Scholar]
- Patil, S.; Rao, R.S.; Majumdar, B. Hamartomas of the oral cavity. J. Int. Soc. Prev. Community Dent. 2015, 5, 347–353. [Google Scholar] [CrossRef] [PubMed]
- Vared, M.; Fowler, C.B.; Neville, B.W.; Soluk Tekkesin, M. Odontoma. In WHO Classification of Head and Neck Tumours; El-Naggar, A.K., Chan, J.K.C., Grandis, J.R., Takat, T., Slootweg, P.J., Eds.; IARC Press: Lyon, France, 2017; pp. 224–226. [Google Scholar]
- Sedano, H.O.; Ocampo-Acosta, F.; Naranjo-Corona, R.I.; Torres-Arellano, M.E. Multiple dens invaginatus, mulberry molar and conical teeth. Case report and genetic considerations. Med. Oral Patol. Oral Y Cir. Bucal 2009, 14, 69–72. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Age/Gender | Clinical Presentation | Tooth Number | Ref. |
|---|---|---|---|
| 24 years/Male | Pain and swelling | 2.1 | [1] |
| 14 years/Female | Unerupted molar tooth | 3.7 | [2] |
| 7 years/Female | Asymptomatic | 4.2 | [3] |
| 28 years/Female | Asymptomatic | 4.8 | [8] |
| 47 years/Female | Pain and discomfort | 3.8 | [9] |
| 16 years/Male | Swelling | 4.4 bis | [10] |
| 24 years/Male | Pain and swelling | 1.7 | [10] |
| 18 years/Male | Malformed tooth and intermittent mild pain | 2.1 bis | [11] |
| 14 years/Male | Swelling | 2.3 | [13] |
| 60 years/Male | NA | 3.8 | [14] |
| 30years/Male | NA | 4.6 | [14] |
| 49 years/Female | NA | 1.8 | [14] |
| 32 years/Female | NA | right maxillary molar region | [14] |
| 11 years/Male | Asymptomatic | 3.8 (germ tooth) | Present case |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zara, F.; D’Angeli, G.; Corsi, A.; Polimeni, A.; Sfasciotti, G.L. Dilated Odontoma Arising in the Mandibular Third Molar Germ: Report of a Case of an Unusual Lesion in an Uncommon Site. Diagnostics 2021, 11, 2256. https://doi.org/10.3390/diagnostics11122256
Zara F, D’Angeli G, Corsi A, Polimeni A, Sfasciotti GL. Dilated Odontoma Arising in the Mandibular Third Molar Germ: Report of a Case of an Unusual Lesion in an Uncommon Site. Diagnostics. 2021; 11(12):2256. https://doi.org/10.3390/diagnostics11122256
Chicago/Turabian StyleZara, Francesca, Giacomo D’Angeli, Alessandro Corsi, Antonella Polimeni, and Gian Luca Sfasciotti. 2021. "Dilated Odontoma Arising in the Mandibular Third Molar Germ: Report of a Case of an Unusual Lesion in an Uncommon Site" Diagnostics 11, no. 12: 2256. https://doi.org/10.3390/diagnostics11122256
APA StyleZara, F., D’Angeli, G., Corsi, A., Polimeni, A., & Sfasciotti, G. L. (2021). Dilated Odontoma Arising in the Mandibular Third Molar Germ: Report of a Case of an Unusual Lesion in an Uncommon Site. Diagnostics, 11(12), 2256. https://doi.org/10.3390/diagnostics11122256