
Evaluation of Depth of Invasion and Tumor Thickness as a Prognostic Factor for Early-Stage Oral Squamous Cell Carcinoma: A Retrospective Study

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
- (1)
- Absence of positive lymph nodes, lymphovascular invasion, or perineural invasion.
- (2)
- Primary OSCC was limited only to soft tissue (absence of bone invasion).
- (3)
- Tumor size greater than 4 cm was excluded as it was considered a more progressed state.
2.2. Statistical Analysis
3. Results
3.1. Patient Characteristics
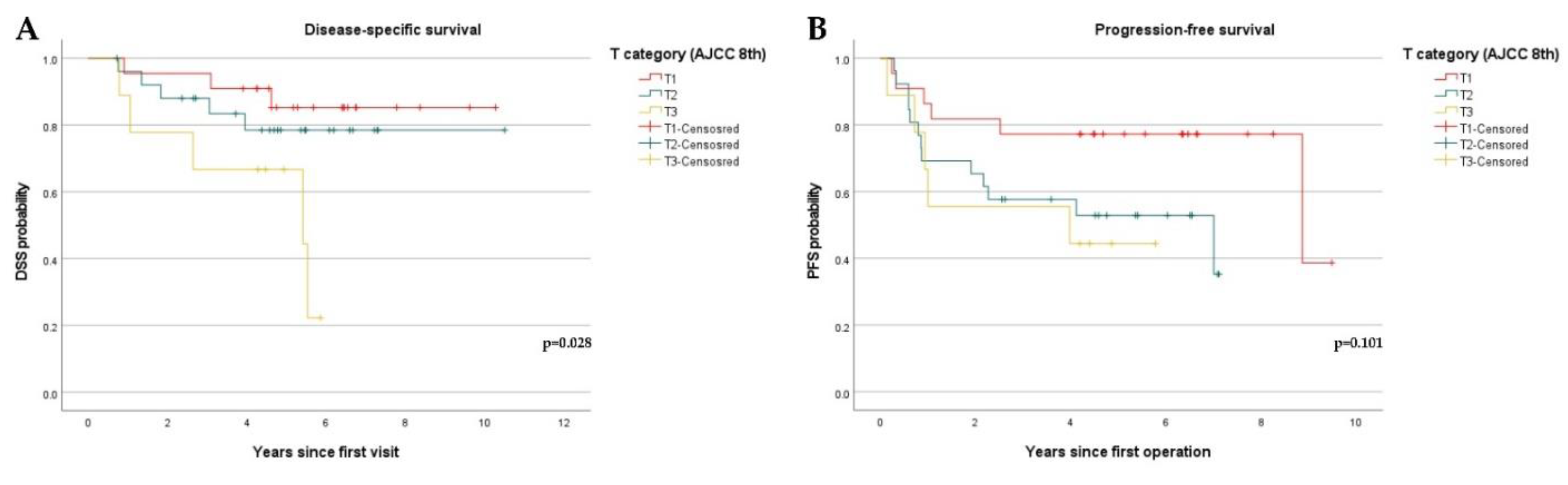
3.2. Disease-Specific Survival and Progression-Free Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kennedy, R.A. WHO is in and WHO is out of the mouth, salivary glands, and jaws sections of the 4th edition of the WHO classification of head and neck tumours. Br. J. Oral Maxillofac. Surg. 2018, 56, 90–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Müller, S. Update from the 4th edition of the World Health Organization of head and neck tumours: Tumours of the oral cavity and mobile tongue. Head Neck Pathol. 2017, 11, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Aslam, F.; Atique, M.; Aslam, M.; Sarfraz, T.; Ayaz, B.A.B.; Alamgir, W. Relation of tumour thickness with lymph node metastasis in oral squamous cell carcinoma. Pak. Armed Forces Med. J. 2012, 62, 529–533. [Google Scholar]
- Pentenero, M.; Gandolfo, S.; Carrozzo, M. Importance of tumor thickness and depth of invasion in nodal involvement and prognosis of oral squamous cell carcinoma: A review of the literature. Head Neck J. Sci. Spec. Head Neck 2005, 27, 1080–1091. [Google Scholar] [CrossRef]
- Ahmed, S.Q.; Junaid, M.; Awan, S.; Choudhary, M.M.; Kazi, M.; Masoom, A.; Khan, H.U. Relationship of tumor thickness with neck node metastasis in buccal squamous cell carcinoma: An experience at a tertiary care hospital. Int. Arch. Otorhinolaryngol. 2017, 21, 265–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berdugo, J.; Thompson, L.D.; Purgina, B.; Sturgis, C.D.; Tuluc, M.; Seethala, R.; Chiosea, S.I. Measuring depth of invasion in early squamous cell carcinoma of the oral tongue: Positive deep margin, extratumoral perineural invasion, and other challenges. Head Neck Pathol. 2019, 13, 154–161. [Google Scholar] [CrossRef]
- Dirven, R.; Ebrahimi, A.; Moeckelmann, N.; Palme, C.E.; Gupta, R.; Clark, J. Tumor thickness versus depth of invasion–Analysis of the 8th edition American Joint Committee on Cancer Staging for oral cancer. Oral Oncol. 2017, 74, 30–33. [Google Scholar] [CrossRef]
- Faisal, M.; Abu Bakar, M.; Sarwar, A.; Adeel, M.; Batool, F.; Malik, K.I.; Jamshed, A.; Hussain, R. Depth of invasion (DOI) as a predictor of cervical nodal metastasis and local recurrence in early stage squamous cell carcinoma of oral tongue (ESSCOT). PLoS ONE 2018, 13, e0202632. [Google Scholar] [CrossRef]
- Liu, B.; Amaratunga, R.; Veness, M.; Wong, E.; Abdul-Razak, M.; Coleman, H.; Gebski, V.; Sundaresan, P. Tumor depth of invasion versus tumor thickness in guiding regional nodal treatment in early oral tongue squamous cell carcinoma. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2020, 129, 45–50. [Google Scholar] [CrossRef]
- Tam, S.; Amit, M.; Zafereo, M.; Bell, D.; Weber, R.S. Depth of invasion as a predictor of nodal disease and survival in patients with oral tongue squamous cell carcinoma. Head Neck 2019, 41, 177–184. [Google Scholar] [CrossRef] [Green Version]
- Lydiatt, W.M.; Patel, S.G.; O’Sullivan, B.; Brandwein, M.S.; Ridge, J.A.; Migliaccim, J.C.; Loomis, A.M.; Shah, J.P. Head and neck cancers—Major changes in the American Joint Committee on cancer eighth edition cancer staging manual. CA A Cancer J. Clin. 2017, 67, 122–137. [Google Scholar] [CrossRef] [PubMed]
- Tan, W.J.; Chia, C.S.; Tan, H.K.; Soo, K.C.; Iyer, N.G. Prognostic significance of invasion depth in oral tongue squamous cell carcinoma. ORL 2012, 74, 264–270. [Google Scholar] [CrossRef]
- Kukreja, P.; Parekh, D.; Roy, P. Practical challenges in measurement of depth of invasion in oral squamous cell carcinoma: Pictographical documentation to improve consistency of reporting per the AJCC 8th edition recommendations. Head Neck Pathol. 2020, 14, 419–427. [Google Scholar] [CrossRef]
- Gonzalez-Moles, M.A.; Esteban, F.; Rodriguez-Archilla, A.; Ruiz-Avila, I.; Gonzalez-Moles, S. Importance of tumour thickness measurement in prognosis of tongue cancer. Oral Oncol. 2002, 38, 394–397. [Google Scholar] [CrossRef]
- Kozak, M.M.; Shah, J.; Chen, M.; Schaberg, K.; von Eyben, R.; Chen, J.J.; Bui, T.; Kong, C.; Kaplan, M.; Divi, V.; et al. Depth of invasion alone as a prognostic factor in low‐risk early‐stage oral cavity carcinoma. Laryngoscope 2019, 129, 2082–2086. [Google Scholar] [CrossRef]
- Almangush, A.; Bello, I.O.; Coletta, R.D.; Mäkitie, A.A.; Mäkinen, L.K.; Kauppila, J.H.; Pukkila, M.; Hagström, J.; Laranne, J.; Soini, Y.; et al. For early-stage oral tongue cancer, depth of invasion and worst pattern of invasion are the strongest pathological predictors for locoregional recurrence and mortality. Virchows Arch. 2015, 467, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Larson, A.R.; Kemmer, J.; Formeister, E.; El-Sayed, I.; Ha, P.; George, J.; Ryan, W.; Chan, E.; Heaton, C. Beyond Depth of Invasion: Adverse Pathologic Tumor Features in Early Oral Tongue Squamous Cell Carcinoma. Laryngoscope 2020, 130, 1715–1720. [Google Scholar] [CrossRef]
- Kano, S.; Sakashita, T.; Tsushima, N.; Mizumachi, T.; Nakazono, A.; Suzuki, T.; Yasukawa, S.; Homma, A. Validation of the 8th edition of the AJCC/UICC TNM staging system for tongue squamous cell carcinoma. Int. J. Clin. Oncol. 2018, 23, 844–850. [Google Scholar] [CrossRef] [Green Version]
- Piazza, C.; Bresciani, L.; Giannini, L. Depth of invasion for prognostic stratification in oral cavity cancer: Do we need further validation? Ann. Transl. Med. 2019, 7 (Suppl. 3), S84. [Google Scholar] [CrossRef] [Green Version]
- Bjerkli, I.H.; Laurvik, H.; Nginamau, E.S.; Søland, T.M.; Costea, D.; Hov, H.; Uhlin-Hansen, L.; Hadler-Olsen, E.; Steigen, S.E. Tumor budding score predicts lymph node status in oral tongue squamous cell carcinoma and should be included in the pathology report. PLoS ONE 2020, 15, e0239783. [Google Scholar] [CrossRef]
- Brockhoff, H.C.; Kim, R.Y.; Braun, T.M.; Skouteris, C.; Helman, J.I.; Ward, B.B. Correlating the depth of invasion at specific anatomic locations with the risk for regional metastatic disease to lymph nodes in the neck for oral squamous cell carcinoma. Head Neck 2017, 39, 974–979. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | N (%) | |
|---|---|---|
| Age (yrs) | 59 (25–85) | |
| Sex | Male | 35 (61.4) |
| Female | 22 (38.6) | |
| Oral subsites | Tongue | 28 (49.1) |
| Palate | 3 (5.3) | |
| Retromolar trigone | 2 (3.5) | |
| Gingiva | 11 (19.3) | |
| Buccal mucosa | 9 (15.8) | |
| Mouth floor | 4 (7.0) | |
| pT (AJCC 7th) | pT1 | 35 (61.4) |
| pT2 | 22 (38.6) | |
| pT (AJCC 8th/DOI) | pT1 | 22 (38.6) |
| pT2 | 26 (45.6) | |
| pT3 | 9 (15.8) | |
| pT (AJCC 8th/TT) | pT1 | 14 (24.6) |
| pT2 | 35 (56.1) | |
| pT3 | 11 (19.3) | |
| Tumor thickness (mm) * | 6.95 (1.00–21.73) | |
| Depth of invasion (mm) * | 4.59 (0.30–23.20) | |
| Neck dissection | No ND | 19 (33.3) |
| Elective ND | 38 (66.7) | |
| Overall treatment | Surgery only | 48 (84.2) |
| Surgery + adjuvant treatment | 9 (15.8) | |
| Recurrence | 22 (38.6) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, Y.-J.; Kwon, T.-G.; Kim, J.-W.; Lee, S.-T.; Hong, S.-H.; Choi, S.-Y. Evaluation of Depth of Invasion and Tumor Thickness as a Prognostic Factor for Early-Stage Oral Squamous Cell Carcinoma: A Retrospective Study. Diagnostics 2022, 12, 20. https://doi.org/10.3390/diagnostics12010020
Lee Y-J, Kwon T-G, Kim J-W, Lee S-T, Hong S-H, Choi S-Y. Evaluation of Depth of Invasion and Tumor Thickness as a Prognostic Factor for Early-Stage Oral Squamous Cell Carcinoma: A Retrospective Study. Diagnostics. 2022; 12(1):20. https://doi.org/10.3390/diagnostics12010020
Chicago/Turabian StyleLee, You-Jung, Tae-Geon Kwon, Jin-Wook Kim, Sung-Tak Lee, Su-Hyung Hong, and So-Young Choi. 2022. "Evaluation of Depth of Invasion and Tumor Thickness as a Prognostic Factor for Early-Stage Oral Squamous Cell Carcinoma: A Retrospective Study" Diagnostics 12, no. 1: 20. https://doi.org/10.3390/diagnostics12010020
APA StyleLee, Y. -J., Kwon, T. -G., Kim, J. -W., Lee, S. -T., Hong, S. -H., & Choi, S. -Y. (2022). Evaluation of Depth of Invasion and Tumor Thickness as a Prognostic Factor for Early-Stage Oral Squamous Cell Carcinoma: A Retrospective Study. Diagnostics, 12(1), 20. https://doi.org/10.3390/diagnostics12010020