
Using Blood Eosinophil Count as a Biomarker to Guide Corticosteroid Treatment for Chronic Obstructive Pulmonary Disease




Abstract
:1. Introduction
2. Decreasing Exposure to Corticosteroid Treatment
3. COPD Eosinophil Phenotypes
4. The Eosinophilic COPD Phenotype and Future Risk
5. Blood Eosinophil-Guided Inhaled Corticosteroid Treatment of Patients with Stable COPD
6. Blood Eosinophil-Guided Systemic Corticosteroid Treatment of Patients with COPD
7. Challenges and Further Directions
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wouters, E.F.; Wouters, B.B.; Augustin, I.M.; Houben-Wilke, S.; Vanfleteren, L.E.; Franssen, F.M. Personalised pulmonary rehabilitation in COPD. Eur. Respir. Rev. 2018, 27. [Google Scholar] [CrossRef] [PubMed]
- Singh, D.; Agusti, A.; Anzueto, A.; Barnes, P.J.; Bourbeau, J.; Celli, B.R.; Criner, B.R.; Frith, P.; Halpin, D.M.G.; Han, M.; et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease: The GOLD science committee report 2019. Eur. Respir. J. 2019. [Google Scholar] [CrossRef]
- Barnes, P.J.; Burney, P.G.; Silverman, E.K.; Celli, B.R.; Vestbo, J.; Wedzicha, J.A.; Wouters, E.F. Chronic obstructive pulmonary disease. Nat. Rev. Dis. Primers 2015, 1, 15076. [Google Scholar] [CrossRef]
- Wen, T.; Rothenberg, M.E. The regulatory function of eosinophils. Microbiol. Spectr. 2016, 4. [Google Scholar] [CrossRef]
- O’Sullivan, J.A.; Bochner, B.S. Eosinophils and eosinophil-associated diseases: An update. J. Allergy Clin. Immunol. 2018, 141, 505–517. [Google Scholar] [CrossRef] [Green Version]
- Ko, F.W.; Chan, K.P.; Hui, D.S.; Goddard, J.R.; Shaw, J.G.; Reid, D.W. Acute exacerbation of COPD. Respirology 2016, 21, 1152–1165. [Google Scholar] [CrossRef] [Green Version]
- Pavord, I.D.; Jones, P.W.; Burgel, P.R.; Rabe, K.F. Exacerbations of COPD. Int. J. Chronic Obstr. Pulm. Dis. 2016, 11, 21–30. [Google Scholar]
- 2021 GOLD Report: Global Initiative for Chronic Obstructive Lung Disease. 2020. Available online: goldcopd.org (accessed on 27 January 2021).
- Woods, J.A.; Wheeler, J.S.; Finch, C.K.; Pinner, N.A. Corticosteroids in the treatment of acute exacerbations of chronic obstructive pulmonary disease. Int. J. Chronic Obstr. Pulm. Dis. 2014, 9, 421–430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saeed, M.I.; Eklöf, J.; Achir, I.; Sivapalan, P.; Meteran, H.; Løkke, A.; Biering-Sorensen, T.; Knop, F.K.; Jensen, J.S. Use of inhaled corticosteroids and the risk of developing type 2 diabetes in patients with chronic obstructive pulmonary disease. Diabetes Obes. Metab. 2020, 22, 1348–1356. [Google Scholar] [CrossRef]
- Waljee, A.K.; Rogers, M.A.; Lin, P.; Singal, A.G.; Stein, J.D.; Marks, R.M.; Ayanian, J.Z.; Nallamothu, B.K. Short term use of oral corticosteroids and related harms among adults in the United States: Population based cohort study. BMJ 2017, 357, j1415. [Google Scholar] [CrossRef] [Green Version]
- Broersen, L.H.; Pereira, A.M.; Jørgensen, J.O.L.; Dekkers, O.M. Adrenal insufficiency in corticosteroids use: Systematic review and meta-analysis. J. Clin. Endocrinol. Metab. 2015, 100, 2171–2180. [Google Scholar] [CrossRef] [PubMed]
- Walsh, L.J.; Wong, C.A.; Oborne, J.; Cooper, S.; Lewis, S.A.; Pringle, M.; Hubbard, R.; Tattersfield, A.E. Adverse effects of oral corticosteroids in relation to dose in patients with lung disease. Thorax 2001, 56, 279–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niewoehner, D.E.; Erbland, M.L.; Deupree, R.H.; Collins, D.; Gross, N.J.; Light, R.W.; Anderson, P.; Morgan, N.A. Effect of systemic glucocorticoids on exacerbations of chronic obstructive pulmonary disease. Department of veterans affairs cooperative study group. N. Engl. J. Med. 1999, 340, 1941–1947. [Google Scholar] [CrossRef]
- Baker, J.M.; Pace, H.A.; Ladesich, J.B.; Simon, S.D. Evaluation of the impact of corticosteroid dose on the incidence of hyperglycemia in hospitalized patients with an acute exacerbation of chronic obstructive pulmonary disease. Hosp. Pharm. 2016, 51, 296–304. [Google Scholar] [CrossRef] [Green Version]
- Van Staa, T.P.; Leufkens, H.G.; Cooper, C. The epidemiology of corticosteroid-induced osteoporosis: A meta-analysis. Osteoporos. Int. 2002, 13, 777–787. [Google Scholar] [CrossRef] [Green Version]
- Bafadhel, M.; McKenna, S.; Terry, S.; Mistry, V.; Pancholi, M.; Venge, P.; Lomas, D.A.; Barer, M.R.; Johnston, S.L.; Pavord, I.D.; et al. Blood eosinophils to direct corticosteroid treatment of exacerbations of chronic obstructive pulmonary disease: A randomized placebo-controlled trial. Am. J. Respir. Crit. Care Med. 2012, 186, 48–55. [Google Scholar] [CrossRef] [Green Version]
- Davies, L.; Angus, R.M.; Calverley, P.M. Oral corticosteroids in patients admitted to hospital with exacerbations of chronic obstructive pulmonary disease: A prospective randomised controlled trial. Lancet 1999, 354, 456–460. [Google Scholar] [CrossRef]
- Walters, J.A.; Tan, D.J.; White, C.J.; Gibson, P.G.; Wood-Baker, R.; Walters, E.H. Systemic corticosteroids for acute exacerbations of chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2014. [Google Scholar] [CrossRef] [Green Version]
- Leuppi, J.D.; Schuetz, P.; Bingisser, R.; Bodmer, M.; Briel, M.; Drescher, T.; Deurring, U.; Henzen, C.; Leibbrandt, Y.; Maier, S.; et al. Short-term vs conventional glucocorticoid therapy in acute exacerbations of chronic obstructive pulmonary disease: The REDUCE randomized clinical trial. JAMA 2013, 309, 2223–2231. [Google Scholar] [CrossRef]
- Sivapalan, P.; Ingebrigtsen, T.S.; Rasmussen, D.B.; Sørensen, R.; Rasmussen, C.M.; Jensen, C.B.; Allin, K.H.; Eklof, J.; Seersholm, N.; Vestbo, J.; et al. COPD exacerbations: The impact of long versus short courses of oral corticosteroids on mortality and pneumonia: Nationwide data on 67,000 patients with COPD followed for 12 months. BMJ Open Respir. Res. 2019, 6, e000407. [Google Scholar] [CrossRef]
- Tashkin, D.P.; Wechsler, M.E. Role of eosinophils in airway inflammation of chronic obstructive pulmonary disease. Int. J. Chronic Obstr. Pulm. Dis. 2018, 13, 335–349. [Google Scholar] [CrossRef] [Green Version]
- McDonald, C.F. Eosinophil Biology in COPD. N. Engl. J. Med. 2017, 377, 1680–1682. [Google Scholar] [CrossRef]
- Barnes, P.J. Inflammatory endotypes in COPD. Allergy 2019, 74, 1249–1256. [Google Scholar] [CrossRef] [Green Version]
- Bafadhel, M.; Pavord, I.D.; Russell, R.E.K. Eosinophils in COPD: Just another biomarker? Lancet Respir. Med. 2017, 5, 747–759. [Google Scholar] [CrossRef]
- Rutgers, S.R.; Timens, W.; Kaufmann, H.F.; van der Mark, T.W.; Koeter, G.H.; Postma, D.S. Comparison of induced sputum with bronchial wash, bronchoalveolar lavage and bronchial biopsies in COPD. Eur. Respir. J. 2000, 15, 109–115. [Google Scholar] [CrossRef]
- Bafadhel, M.; McKenna, S.; Terry, S.; Mistry, V.; Reid, C.; Haldar, P.; McCormick, M.; Haldar, K.; Kebadze, T.; Duvoix, A.; et al. Acute exacerbations of chronic obstructive pulmonary disease: Identification of biologic clusters and their biomarkers. Am. J. Respir. Crit. Care Med. 2011, 184, 662–671. [Google Scholar] [CrossRef]
- Saha, S.; Brightling, C.E. Eosinophilic airway inflammation in COPD. Int. J. Chronic Obstr. Pulm. Dis. 2006, 1, 39–47. [Google Scholar] [CrossRef] [Green Version]
- Leigh, R.; Pizzichini, M.M.M.; Morris, M.M.; Maltais, F.; Hargreave, F.E.; Pizzichini, E. Stable COPD: Predicting benefit from high-dose inhaled corticosteroid treatment. Eur. Respir. J. 2006, 27, 964–971. [Google Scholar] [CrossRef] [Green Version]
- Brightling, C.E.; Monteiro, W.; Ward, R.; Parker, D.; Morgan, M.D.; Wardlaw, A.J. Sputum eosinophilia and short-term response to prednisolone in chronic obstructive pulmonary disease: A randomised controlled trial. Lancet 2000, 356, 1480–1485. [Google Scholar] [CrossRef]
- Siva, R.; Green, R.H.; Brightling, C.E.; Shelley, M.; Hargadon, B.; McKenna, S.; Monteiro, W.; Berry, M.; Parker, D.; Wardlaw, A.J.; et al. Eosinophilic airway inflammation and exacerbations of COPD: A randomised controlled trial. Eur. Respir. J. 2007, 29, 906–913. [Google Scholar] [CrossRef] [PubMed]
- Pizzichini, E.; Pizzichini, M.M.; Gibson, P.; Parameswaran, K.; Gleich, G.J.; Berman La, S. Sputum eosinophilia predicts benefit from prednisone in smokers with chronic obstructive bronchitis. Am. J. Respir. Crit. Care Med. 1998, 158, 1511–1517. [Google Scholar] [CrossRef]
- Brightling, C.E.; McKenna, S.; Hargadon, B.; Birring, S.; Green, R.; Siva, R.; Berry, M.; Parker, D.; Monteiro, W.; Pavord, I.D.; et al. Sputum eosinophilia and the short term response to inhaled mometasone in chronic obstructive pulmonary disease. Thorax 2005, 60, 193–198. [Google Scholar] [CrossRef] [Green Version]
- Singh, D. Blood eosinophil counts in chronic obstructive pulmonary disease: A biomarker of inhaled corticosteroid effects. Tuberc. Respir. Dis. 2020, 83, 185–194. [Google Scholar] [CrossRef] [PubMed]
- Negewo, N.A.; McDonald, V.M.; Baines, K.J.; Wark, P.A.; Simpson, J.L.; Jones, P.W. Peripheral blood eosinophils: A surrogate marker for airway eosinophilia in stable COPD. Int. J. Chronic Obstr. Pulm. Dis. 2016, 11, 1495–1504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, D.; Kolsum, U.; Brightling, C.E.; Locantore, N.; Agusti, A.; Tal-Singer, R. Eosinophilic inflammation in COPD: Prevalence and clinical characteristics. Eur. Respir. J. 2014, 44, 1697–1700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pizzichini, M.M.M.; Leigh, R.; Djukanović, R.; Sterk, P.J. Safety of sputum induction. Eur. Respir. J Suppl. 2002, 37, 9s–18s. [Google Scholar] [PubMed] [Green Version]
- Camp, J.; Cane, J.L.; Bafadhel, M. Shall we focus on the eosinophil to guide treatment with systemic corticosteroids during acute exacerbations of COPD? PRO. Med. Sci. 2018, 6, 74. [Google Scholar] [CrossRef] [Green Version]
- Pavord, I.D.; Bafadhel, M. Exhaled nitric oxide and blood eosinophilia: Independent markers of preventable risk. J. Allergy Clin. Immunol. 2013, 132, 828–829. [Google Scholar] [CrossRef]
- Beeh, K.M.; Beier, J.; Kornmann, O.; Mander, A.; Buhl, R. Long-term repeatability of induced sputum cells and inflammatory markers in stable, moderately severe COPD. Chest 2003, 123, 778–783. [Google Scholar] [CrossRef] [Green Version]
- Wagener, A.H.; de Nijs, S.B.; Lutter, R.; Sousa, A.R.; Weersink, E.J.; Bel, E.H. External validation of blood eosinophils, FE(NO) and serum periostin as surrogates for sputum eosinophils in asthma. Thorax 2015, 70, 115–120. [Google Scholar] [CrossRef] [Green Version]
- Ortega, H.; Llanos, J.; Lafeuille, M.; Germain, G.; Duh, M.S.; Bell, C.F.; Sama, S.R.; Hahn, B. Burden of disease associated with a COPD eosinophilic phenotype. Int. J. Chronic Obstr. Pulm. Dis. 2018. [Google Scholar] [CrossRef] [Green Version]
- Casanova, C.; Celli, B.R.; de-Torres, J.P.; Martínez-Gonzalez, C.; Cosio, B.G.; Pinto-Plata, V.; de Lucas-Ramos, P.; Divo, M.; Fuster, A.; Peces-Barba, G.; et al. Prevalence of persistent blood eosinophilia: Relation to outcomes in patients with COPD. Eur. Respir. J. 2017, 50. [Google Scholar] [CrossRef]
- Dinh-Xuan, A.T.; Brusselle, G. FENO as a biomarker guide for inhaled corticosteroid step down in patients with mild-to-moderate well-controlled asthma. Eur. Respir. J. 2020, 55. [Google Scholar] [CrossRef] [PubMed]
- Bikov, A.; Meszaros, M.; Lazar, Z. Exhaled nitric oxide in COPD. Curr. Respir. Med. Rev. 2019, 15, 71–78. [Google Scholar] [CrossRef]
- Colak, Y.; Afzal, S.; Nordestgaard, B.G.; Marott, J.L.; Lange, P. Combined value of exhaled nitric oxide and blood eosinophils in chronic airway disease: The Copenhagen General Population Study. Eur. Respir. J. 2018, 52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karnaushkina, M.A.; Fedosenko, S.V.; Danilov, R.S.; Komarova, I.S. Eosinophilic cationic protein as a non-invasive marker of the nature of inflammatory response in patients with chronic obstructive pulmonary disease. Bull. Sib. Med. 2020, 19, 59–66. [Google Scholar] [CrossRef] [Green Version]
- Aldridge, R.E.; Hancox, R.J.; Cowant, J.O.; Frampton, C.M.; Town, G.I.; Taylor, D.R. Eosinophils and eosinophilic cationic protein in induced sputum and blood: Effects of budesonide and terbutaline treatment. Ann. Allergy Asthma Immunol. 2002, 89, 492–497. [Google Scholar] [CrossRef]
- Gursel, G.; Turktas, H.; Gokcora, N.; Tekin, I.O. Comparison of sputum and serum eosinophil cationic protein (ECP) levels in nonatopic asthma and chronic obstructive pulmonary disease. J. Asthma 1997, 34, 313–319. [Google Scholar] [CrossRef]
- David, B.; Bafadhel, M.; Koenderman, L.; de Soyza, A. Eosinophilic inflammation in COPD: From an inflammatory marker to a treatable trait. Thorax 2020, 76, 188–195. [Google Scholar] [CrossRef] [PubMed]
- Yun, J.H.; Lamb, A.; Chase, R.; Singh, D.; Parker, M.M.; Saferali, A.; Vestbo, J.; Tal-Singer, R.; Castaldi, P.J.; Silverman, E.K.; et al. Blood eosinophil count thresholds and exacerbations in patients with chronic obstructive pulmonary disease. J. Allergy Clin. Immunol. 2018, 141, 2037–2047. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vedel-Krogh, S.; Nielsen, S.F.; Lange, P.; Vestbo, J.; Nordestgaard, B.G. Blood eosinophils and exacerbations in chronic obstructive pulmonary disease. The Copenhagen general population study. Am. J. Respir. Crit. Care Med. 2016, 193, 965–974. [Google Scholar] [CrossRef]
- Prins, H.J.; Duijkers, R.; Lutter, R.; Daniels, J.M.; van der Valk, P.; Schoorl, M. Blood eosinophilia as a marker of early and late treatment failure in severe acute exacerbations of COPD. Respir. Med. 2017, 131, 118–124. [Google Scholar] [CrossRef] [Green Version]
- Couillard, S.; Larivee, P.; Courteau, J.; Vanasse, A. Eosinophils in COPD exacerbations are associated with increased readmissions. Chest 2017, 151, 366–373. [Google Scholar] [CrossRef]
- Li, Q.; Larivee, P.; Courteau, J.; Couillard, S.; Poder, T.G.; Carrier, N. Greater eosinophil counts at first COPD hospitalization are associated with more readmissions and fewer deaths. Int. J. Chronic Obstr. Pulm. Dis. 2019, 14, 331–341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bafadhel, M.; Greening, N.J.; Harvey-Dunstan, T.C.; Williams, J.E.; Morgan, M.D.; Brightling, C.E.; Hussain, S.F.; Pavord, I.D.; Singh, S.J.; Steiner, M.C. Blood eosinophils and outcomes in severe hospitalized exacerbations of COPD. Chest 2016, 150, 320–328. [Google Scholar] [CrossRef] [PubMed]
- Ko, F.W.; Chan, K.P.; Ngai, J.; Ng, S.S.; Yip, W.H.; Ip, A.; Chan, T.O.; Hui, D.S.C. Blood eosinophil count as a predictor of hospital length of stay in COPD exacerbations. Respirology 2020, 25, 259–266. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, S.H.; Guasconi, A.; Vestbo, J.; Jones, P.; Agusti, A.; Paggiaro, P.; Wedzicha, J.A.; Singh, D. Blood eosinophils: A biomarker of response to extrafine beclomethasone/formoterol in chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2015, 192, 523–525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Regan, E.A.; Hokanson, J.E.; Murphy, J.R.; Make, B.; Lynch, D.A.; Beaty, T.H.; Curran-Everett, D.; Silverman, E.K.; Crapo, J.D. Genetic epidemiology of COPD (COPDGene) study design. COPD 2010, 7, 32–43. [Google Scholar] [CrossRef]
- Vestbo, J.; Anderson, W.; Coxson, H.O.; Crim, C.; Dawber, F.; Edwards, L.; Hagan, G.; Knobil, K.; Lomas, D.A.; MacNee, W.; et al. Evaluation of COPD longitudinally to identify predictive surrogate end-points (ECLIPSE). Eur. Respir. J. 2008, 31, 869–873. [Google Scholar] [CrossRef] [Green Version]
- Russell, R.E.K.; Bafadhel, M. Investigating blood eosinophil count thresholds in patients with COPD. Lancet Respir. Med. 2018, 6, 823–824. [Google Scholar] [CrossRef]
- Vedel-Krogh, S.; Nordestgaard, B.G.; Lange, P.; Vestbo, J.; Nielsen, S.F. Blood eosinophil count and risk of pneumonia hospitalisations in individuals with COPD. Eur. Respir. J. 2018, 51. [Google Scholar] [CrossRef]
- Sivapalan, P.; Jensen, J.U. Non-eosinophilic severe exacerbations of COPD: What about antibiotics?—Authors’ reply. Lancet Respir. Med. 2019, 7, e34. [Google Scholar] [CrossRef]
- Turato, G.; Semenzato, U.; Bazzan, E.; Biondini, D.; Tine, M.; Torrecilla, N.; Forner, M.; Marin, J.M.; Cosio, M.G.; Saetta, M. Blood eosinophilia neither reflects tissue eosinophils nor worsens clinical outcomes in chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2018, 197, 1216–1219. [Google Scholar] [CrossRef]
- DiSantostefano, R.L.; Hinds, D.; Le, H.V.; Barnes, N.C. Relationship between blood eosinophils and clinical characteristics in a cross-sectional study of a US population-based COPD cohort. Respir. Med. 2016, 112, 88–96. [Google Scholar] [CrossRef] [Green Version]
- Pavord, I.D.; Lettis, S.; Anzueto, A.; Barnes, N. Blood eosinophil count and pneumonia risk in patients with chronic obstructive pulmonary disease: A patient-level meta-analysis. Lancet Respir. Med. 2016, 4, 731–741. [Google Scholar] [CrossRef]
- Dransfield, M.T.; Singh, D. Predicting pneumonia in chronic obstructive pulmonary disease. Have we unraveled the network of risks? Am. J. Respir. Crit. Care Med. 2020, 201, 1026–1027. [Google Scholar] [CrossRef] [PubMed]
- Kolsum, U.; Donaldson, G.C.; Singh, R.; Barker, B.L.; Gupta, V.; George, L.; Webb, A.J.; Thurston, S.; Brookes, A.J.; McHugh, T.D.; et al. Blood and sputum eosinophils in COPD; relationship with bacterial load. Respir. Res. 2017, 18, 88. [Google Scholar] [CrossRef]
- Lodise, T.P.; Li, J.; Gandhi, H.N.; O’Brien, G.; Sethi, S. Intraclass difference in pneumonia risk with fluticasone and budesonide in COPD: A systematic review of evidence from direct-comparison studies. Int. J. Chronic Obstr. Pulm. Dis. 2020, 15, 2889–2900. [Google Scholar] [CrossRef] [PubMed]
- Bafadhel, M.; Peterson, S.; de Blas, M.A.; Calverley, P.M.; Rennard, S.I.; Richter, K.; Fageras, M. Predictors of exacerbation risk and response to budesonide in patients with chronic obstructive pulmonary disease: A post-hoc analysis of three randomised trials. Lancet Respir. Med. 2018, 6, 117–126. [Google Scholar] [CrossRef]
- Halpin, D.M.G.; Criner, G.J.; Papi, A.; Singh, D.; Anzueto, A.; Martinez, F.J.; Agusti, A.; Vogelmeier, C.F.; Gold Science Committee. Global initiative for the diagnosis, management, and prevention of chronic obstructive lung disease: The 2020 GOLD science committee report on COVID-19 & COPD. Am. J. Respir. Crit. Care Med. 2020. [Google Scholar] [CrossRef]
- Pascoe, S.; Locantore, N.; Dransfield, M.T.; Barnes, N.C.; Pavord, I.D. Blood eosinophil counts, exacerbations, and response to the addition of inhaled fluticasone furoate to vilanterol in patients with chronic obstructive pulmonary disease: A secondary analysis of data from two parallel randomised controlled trials. Lancet Respir. Med. 2015, 3, 435–442. [Google Scholar] [CrossRef]
- Pavord, I.D.; Lettis, S.; Locantore, N.; Pascoe, S.; Jones, P.W.; Wedzicha, J.A.; Barnes, N.C. Blood eosinophils and inhaled corticosteroid/long-acting beta-2 agonist efficacy in COPD. Thorax 2016, 71, 118–125. [Google Scholar] [CrossRef] [Green Version]
- Lipson, D.A.; Barnhart, F.; Brealey, N.; Brooks, J.; Criner, G.J.; Day, N.C.; Dransfield, M.T.; Halpin, D.M.G.; Han, M.K.; Jones, C.E.; et al. Once-daily single-inhaler triple versus dual therapy in patients with COPD. N. Engl. J. Med. 2018, 378, 1671–1680. [Google Scholar] [CrossRef]
- Calverley, P.M.; Tetzlaff, K.; Vogelmeier, C.; Fabbri, L.M.; Magnussen, H.; Wouters, E.F.; Mezzanotte, W.; Disse, B.; Finnigan, H.; Asijee, G.; et al. Eosinophilia, frequent exacerbations, and steroid response in chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2017, 196, 1219–1221. [Google Scholar] [CrossRef]
- Watz, H.; Tetzlaff, K.; Wouters, E.F.; Kirsten, A.; Magnussen, H.; Rodriguez-Roisin, R.; Vogelmeier, C.; Fabbri, L.M.; Chanez, P.; Dahl, R.; et al. Blood eosinophil count and exacerbations in severe chronic obstructive pulmonary disease after withdrawal of inhaled corticosteroids: A post-hoc analysis of the WISDOM trial. Lancet Respir. Med. 2016, 4, 390–398. [Google Scholar] [CrossRef]
- Chapman, K.R.; Hurst, J.R.; Frent, S.M.; Larbig, M.; Fogel, R.; Guerin, T.; Banerji, D.; Patalano, F.; Goyal, P.; Pfister, P.; et al. Long-term triple therapy de-escalation to indacaterol/glycopyrronium in patients with chronic obstructive pulmonary disease (SUNSET): A randomized, double-blind, triple-dummy clinical trial. Am. J. Respir. Crit. Care Med. 2018, 198, 329–339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magnussen, H.; Disse, B.; Rodriguez-Roisin, R.; Kirsten, A.; Watz, H.; Tetzlaff, K.; Towse, L.; Finnigan, H.; Dahl, R.; Decramer, M.; et al. Withdrawal of inhaled glucocorticoids and exacerbations of COPD. N. Engl. J. Med. 2014, 371, 1285–1294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chalmers, J.D.; Laska, I.F.; Franssen, F.M.; Janssens, W.; Pavord, I.; Rigau, D.; McDonnell, M.J.; Roche, N.; Sin, D.D.; Stolz, D.; et al. Withdrawal of inhaled corticosteroids in COPD: A European respiratory society guideline. Eur. Respir. J. 2020, 55. [Google Scholar] [CrossRef] [PubMed]
- Wedzicha, J.A.; Singh, D.; Vestbo, J.; Paggiaro, P.L.; Jones, P.W.; Bonnet-Gonod, F.; Cohuet, G.; Corradi, M.; Vezzoli, S.; Petruzzelli, S.; et al. Extrafine beclomethasone/formoterol in severe COPD patients with history of exacerbations. Respir. Med. 2014, 108, 1153–1162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnes, N.C.; Sharma, R.; Lettis, S.; Calverley, P.M. Blood eosinophils as a marker of response to inhaled corticosteroids in COPD. Eur. Respir. J. 2016, 47, 1374–1382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathioudakis, A.G.; Bikov, A.; Foden, P.; Lahousse, L.; Brusselle, G.; Singh, D.; Vesto, J. Change in blood eosinophils following treatment with inhaled corticosteroids may predict long-term clinical response in COPD. Eur. Respir. J. 2020, 55. [Google Scholar] [CrossRef]
- Wedzicha, J.A.; Banerji, D.; Chapman, K.R.; Vestbo, J.; Roche, N.; Ayers, R.T.; Thach, C.; Fogel, R.; Patalano, F.; Vogelmeier, C.F.; et al. Indacaterol-glycopyrronium versus salmeterol-fluticasone for COPD. N. Engl. J. Med. 2016, 374, 2222–2234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zysman, M.; Deslee, G.; Caillaud, D.; Chanez, P.; Escamilla, R.; Court-Fortune, I.; Nesme-Meyer, P.; Perez, T.; Paillasseur, J.L.; Pinet, C.; et al. Relationship between blood eosinophils, clinical characteristics, and mortality in patients with COPD. Int. J. Chronic Obstr. Pulm. Dis. 2017, 12, 1819–1824. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adir, Y.; Hakrush, O.; Shteinberg, M.; Schneer, S.; Agusti, A. Circulating eosinophil levels do not predict severe exacerbations in COPD: A retrospective study. ERJ Open Res. 2018, 4. [Google Scholar] [CrossRef]
- Bafadhel, M.; Davies, L.; Calverley, P.M.; Aaron, S.D.; Brightling, C.E.; Pavord, I.D. Blood eosinophil guided prednisolone therapy for exacerbations of COPD: A further analysis. Eur. Respir. J. 2014, 44, 789–791. [Google Scholar] [CrossRef] [Green Version]
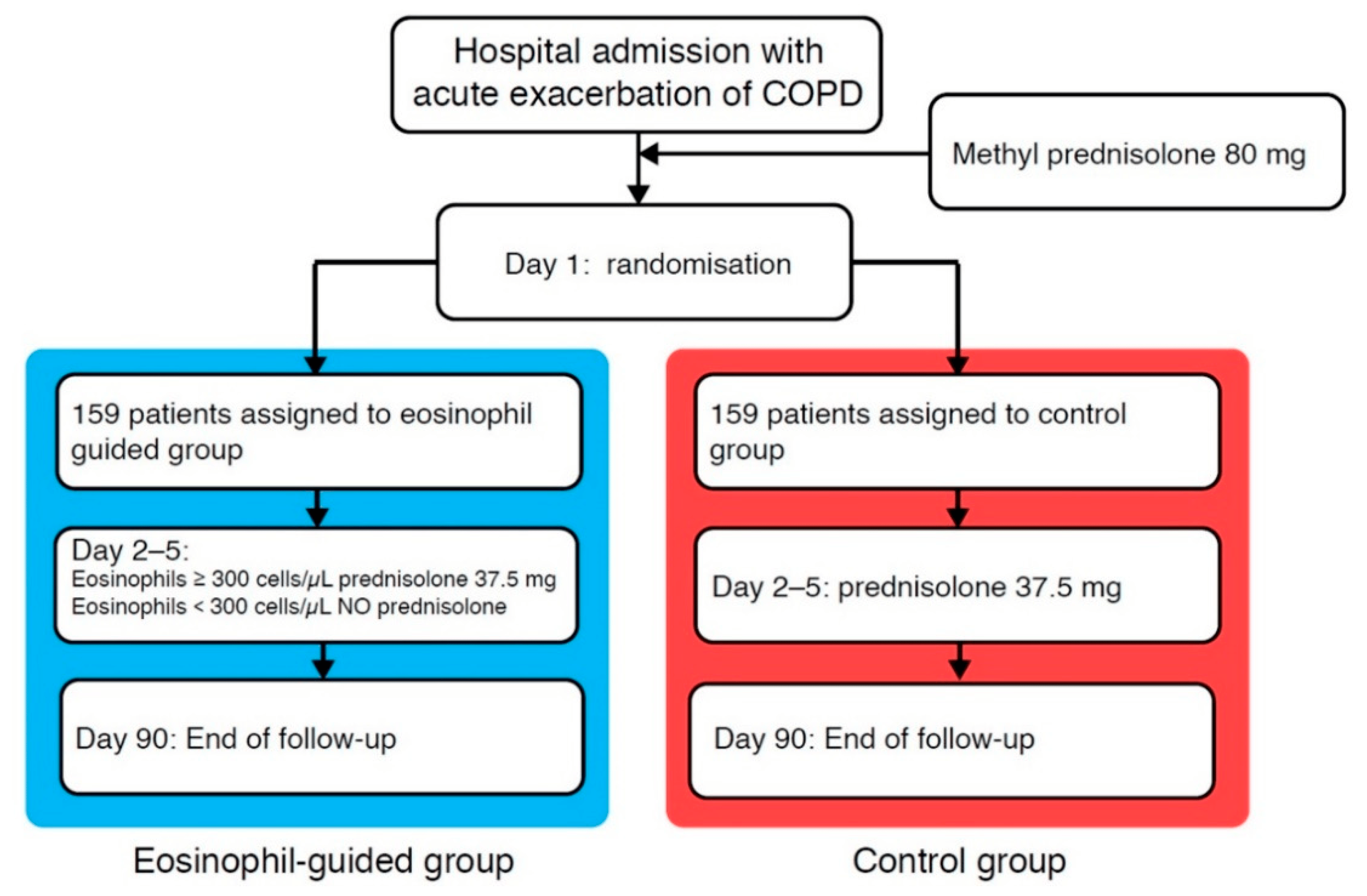
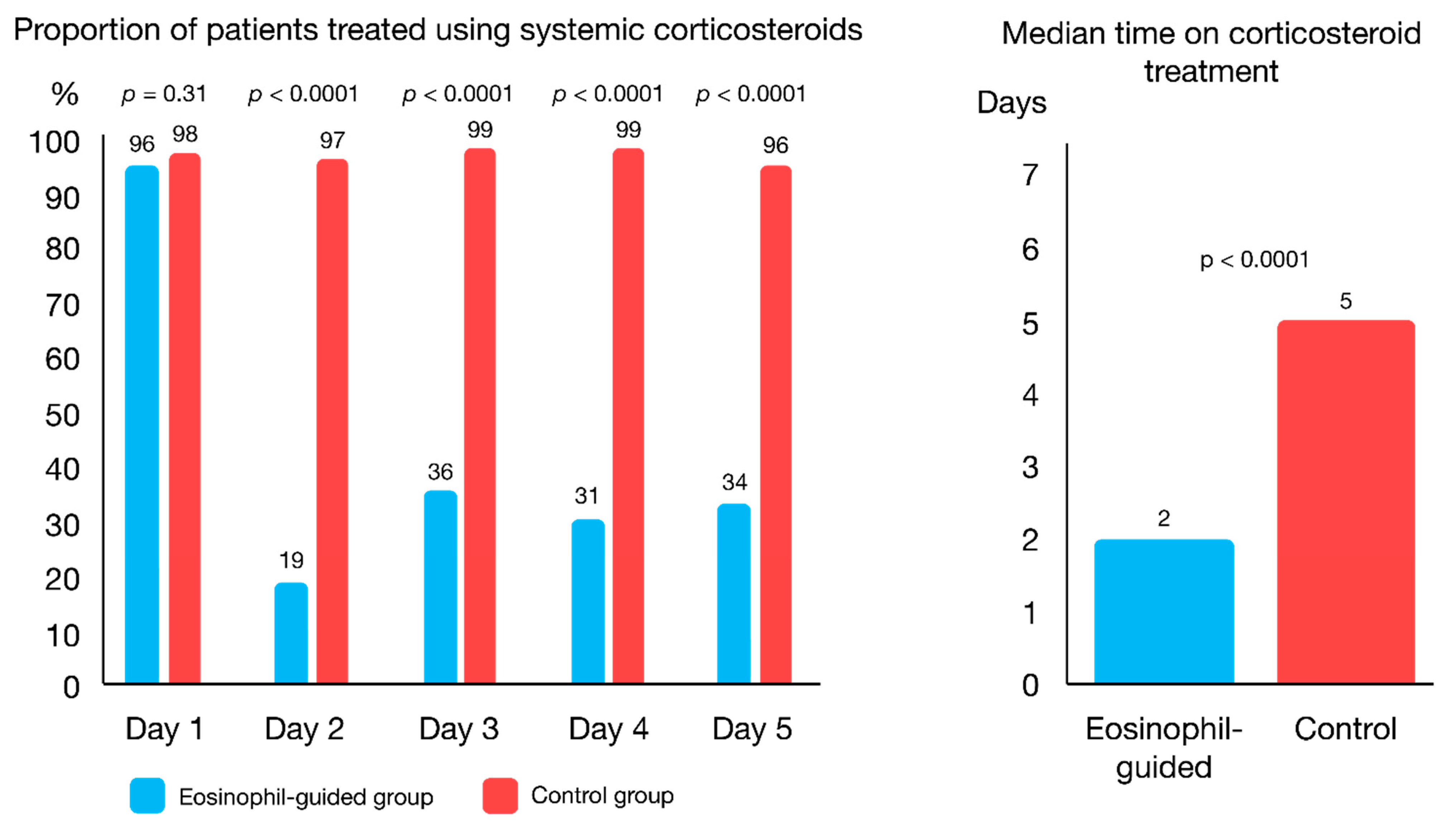
- Sivapalan, P.; Lapperre, T.S.; Janner, J.; Laub, R.R.; Moberg, M.; Bech, C.S.; Eklof, J.; Holm, F.S.; Armbruster, K.; Sivapalan, P.; et al. Eosinophil-guided corticosteroid therapy in patients admitted to hospital with COPD exacerbation (CORTICO-COP): A multicentre, randomised, controlled, open-label, non-inferiority trial. Lancet Respir. Med. 2019, 7, 699–709. [Google Scholar] [CrossRef]
- Anzueto, A.R.; Kostikas, K.; Mezzi, K.; Shen, S.; Larbig, M.; Patalano, F.; Fogel, R.; Banerji, D.; Wedzicha, J.A. Indacaterol/glycopyrronium versus salmeterol/fluticasone in the prevention of clinically important deterioration in COPD: Results from the FLAME study. Respir. Res. 2018, 19, 121. [Google Scholar] [CrossRef]
- Mei, D.; Tan, W.S.D.; Wong, W.S.F. Pharmacological strategies to regain steroid sensitivity in severe asthma and COPD. Curr. Opin. Pharmacol. 2019, 46, 73–81. [Google Scholar] [CrossRef]
- Milara, J.; Cervera, A.; de Diego, A.; Sanz, C.; Juan, G.; Gavaldà, A.; Miralpeix, M.; Morcillo, E.; Cortijo, J. Non-neuronal cholinergic system contributes to corticosteroid resistance in chronic obstructive pulmonary disease patients. Respir. Res. 2016, 17, 145. [Google Scholar] [CrossRef] [Green Version]
- Sun, X.J.; Li, Z.H.; Zhang, Y.; Zhou, G.; Zhang, J.Q.; Deng, J.M.; Bai, J.; Liu, G.N.; Li, M.H.; MacNee, W.; et al. Combination of erythromycin and dexamethasone improves corticosteroid sensitivity induced by CSE through inhibiting PI3K-delta/Akt pathway and increasing GR expression. Am. J. Physiol. Lung Cell. Mol. Physiol. 2015, 309, L139–L146. [Google Scholar] [CrossRef] [PubMed]
- Milara, J.; Morell, A.; Ballester, B.; Sanz, C.; Freire, J.; Qian, X.; Alonso-Garcia, M.; Morcillo, E.; Cortijo, J. Roflumilast improves corticosteroid resistance COPD bronchial epithelial cells stimulated with toll like receptor 3 agonist. Respir. Res. 2015, 16, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, Y.; Yu, P.; Lu, J.J.; Lu, H.Z.; Zhu, L.; Yu, Z.H.; Chen, H.Z.; Cui, Y.Y. A mucoactive drug carbocisteine ameliorates steroid resistance in rat COPD model. Pulm. Pharmacol. Ther. 2016, 39, 38–47. [Google Scholar] [CrossRef] [PubMed]
- Cosio, B.G.; Iglesias, A.; Rios, A.; Noguera, A.; Sala, E.; Ito, K.; Barnes, P.J.; Agusti, A. Low-dose theophylline enhances the anti-inflammatory effects of steroids during exacerbations of COPD. Thorax 2009, 64, 424–429. [Google Scholar] [CrossRef] [Green Version]
- Kadushkin, A.G.; Taganovich, A.D.; Movchan, L.V.; Shman, T.V. Use of the routine complete blood count to predict steroid resistance in patients with chronic obstructive pulmonary disease. Russ. Pulmonol. 2019, 28, 681–692. [Google Scholar] [CrossRef]
- Wedzicha, J.A.; Miravitlles, M.; Hurst, J.R.; Calverley, P.M.; Albert, R.K.; Anzueto, A. Management of COPD exacerbations: A European respiratory society/American thoracic society guideline. Eur. Respir. J. 2017, 49. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Author | N | Treatment | Eosinophil Threshold | Findings |
|---|---|---|---|---|
| IMPACT—Lipson et al., 2018 [74] | 6204 | Fluticasone furoate (ICS)/vilanterol (LABA) vs. umeclidinium (LAMA)/vilanterol (LABA) | ≥150 cells/μL | ICS/LABA/LAMA vs. LABA/LAMA, BEC ≥ 150 cells/μL: 32% reduction in annual exacerbation rate * |
| Bafadhel et al., 2018 [70] | 4528 | BDP/FOR vs. FOR | 200–340 cells/μL | 26–50% decrease in annual exacerbation rate |
| 350–630 cells/μL | 51–60% decrease in annual exacerbation rate | |||
| FORWARD—Siddiqui et al., 2015 [57] | 1199 | BDP/FOR vs. FOR | ≥279.8 cells/μL | BEC ≥ 279.8 cells/μL: 46% reduction in annual exacerbation rate. BEC < 279.8 cells/μL: 28% reduction in annual exacerbation rate. |
| ISOLDE—Barnes et al., 2016 [81] | 456 | fluticasone propionate versus placebo | ≥2% | The reduction in overall exacerbation rate for fluticasone propionate versus placebo was higher in the <2% eosinophil group compared with the ≥2% eosinophil group |
| FLAME—Anzueto et al., 2016 [88] | 3362 | Glycopyrronium (LAMA)/indacaterol (LABA) vs. fluticasone (ICS)/salmeterol (LABA) | ≥2% | 11% reduction (LAMA/LABA vs. ICS/LABA) ** |
| Calverley et al., 2017 [75] | 2420 | ≥300 cells/µL | ICS withdrawal vs. continuation ≥1 exacerbation in prior year AND BEC ≥ 300 cells/μL: 45% increase in annual exacerbation rate * ≥2 exacerbations in prior year AND BEC ≥ 300 cells/μL: 75% increase in annual exacerbation rate *; | |
| WISDOM—Watz et al., 2016 [76] | 2296 | FP/SAL/tiotropium vs. continuation or withdrawal of ICS treatment | ≥300 cells/µL | ICS withdrawal vs. continuation: BEC < 300 cells/μL *: 4% increase *; BEC ≥ 300 cells/μL *: 56% increase in annual exacerbation rate * BEC < 400 cells/μL: 7% increase *; BEC ≥ 400 cells/μL: 73% increase in annual exacerbation rate * |
| SUNSET—Chapman et al., 2018 [77] | 527 | Tiotropium (LAMA)/salmeterol (LABA)/fluticasone (ICS). Two arms: first group continues with triple therapy; second switches to glycopyrronium (LAMA)/indacaterol (LABA) | ≥300 cells/µL | ICS withdrawal vs. continuation: BEC ≥ 300 cells/μL: 86% increase in annual exacerbation rate |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sivapalan, P.; Bikov, A.; Jensen, J.-U. Using Blood Eosinophil Count as a Biomarker to Guide Corticosteroid Treatment for Chronic Obstructive Pulmonary Disease. Diagnostics 2021, 11, 236. https://doi.org/10.3390/diagnostics11020236
Sivapalan P, Bikov A, Jensen J-U. Using Blood Eosinophil Count as a Biomarker to Guide Corticosteroid Treatment for Chronic Obstructive Pulmonary Disease. Diagnostics. 2021; 11(2):236. https://doi.org/10.3390/diagnostics11020236
Chicago/Turabian StyleSivapalan, Pradeesh, András Bikov, and Jens-Ulrik Jensen. 2021. "Using Blood Eosinophil Count as a Biomarker to Guide Corticosteroid Treatment for Chronic Obstructive Pulmonary Disease" Diagnostics 11, no. 2: 236. https://doi.org/10.3390/diagnostics11020236
APA StyleSivapalan, P., Bikov, A., & Jensen, J. -U. (2021). Using Blood Eosinophil Count as a Biomarker to Guide Corticosteroid Treatment for Chronic Obstructive Pulmonary Disease. Diagnostics, 11(2), 236. https://doi.org/10.3390/diagnostics11020236