
Local Laboratory Testing of Germline BRCA Mutations vs. Myriad: A Single-Institution Experience in Korea

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
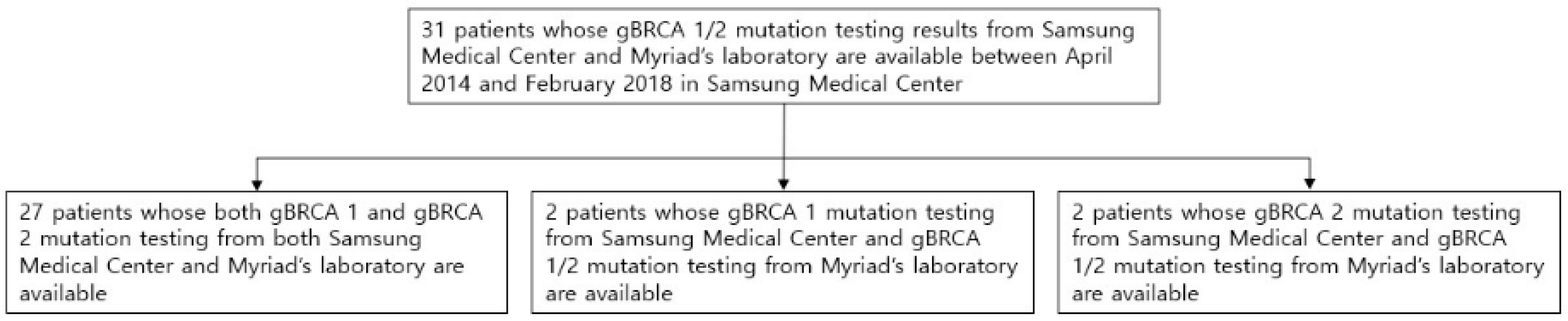
2.1. Study Population
2.2. Data Collection
2.3. Pathology
2.4. BRACAnalysis® CDx
2.5. BRCA 1/2 Gene Mutation Tests from Samsung Medical Center
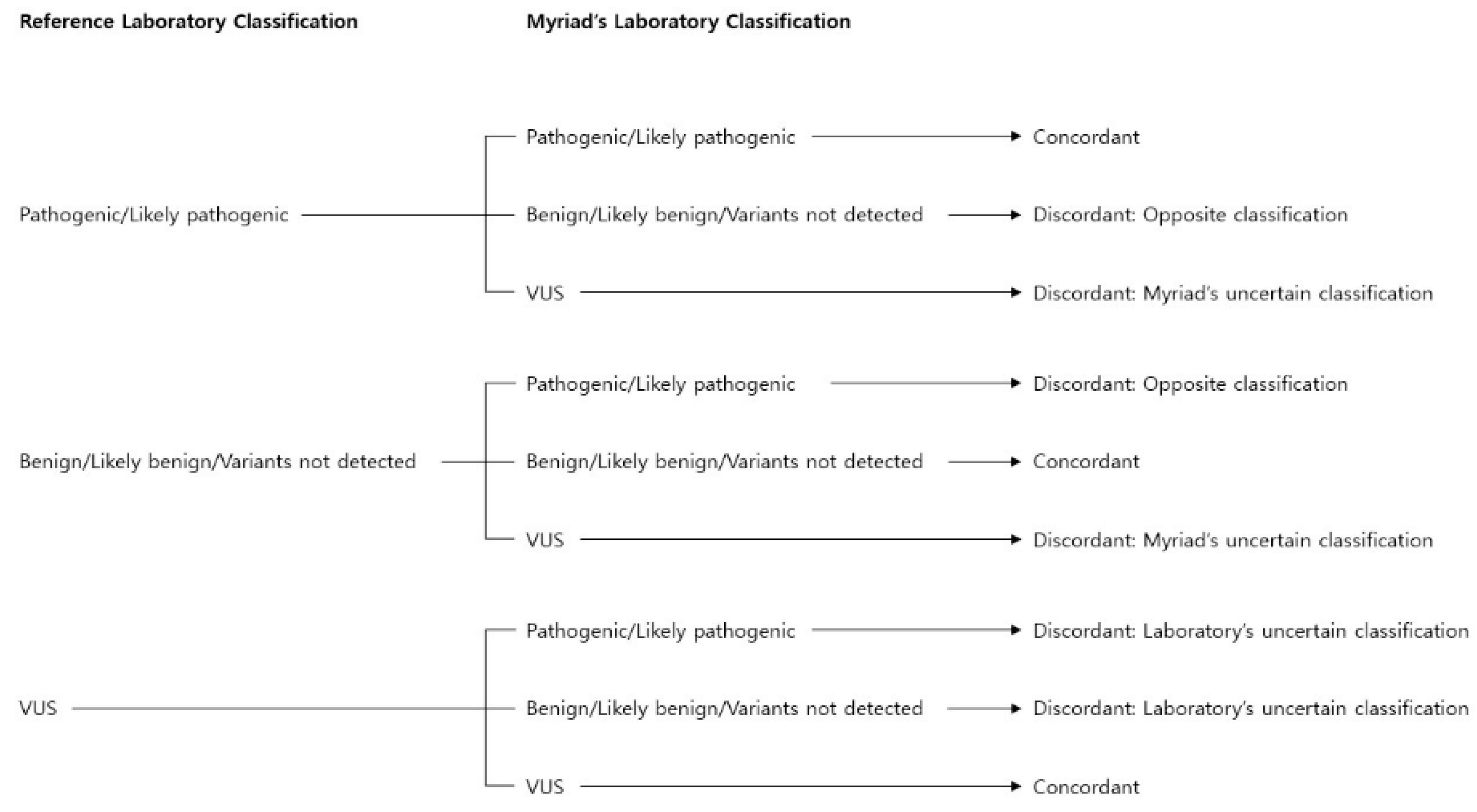
2.6. Comparison of Variant Classifications
2.7. Statistical Analysis
2.8. Ethical Considerations
3. Results
3.1. Patient Characteristics
3.2. gBRCA 1/2 Mutations
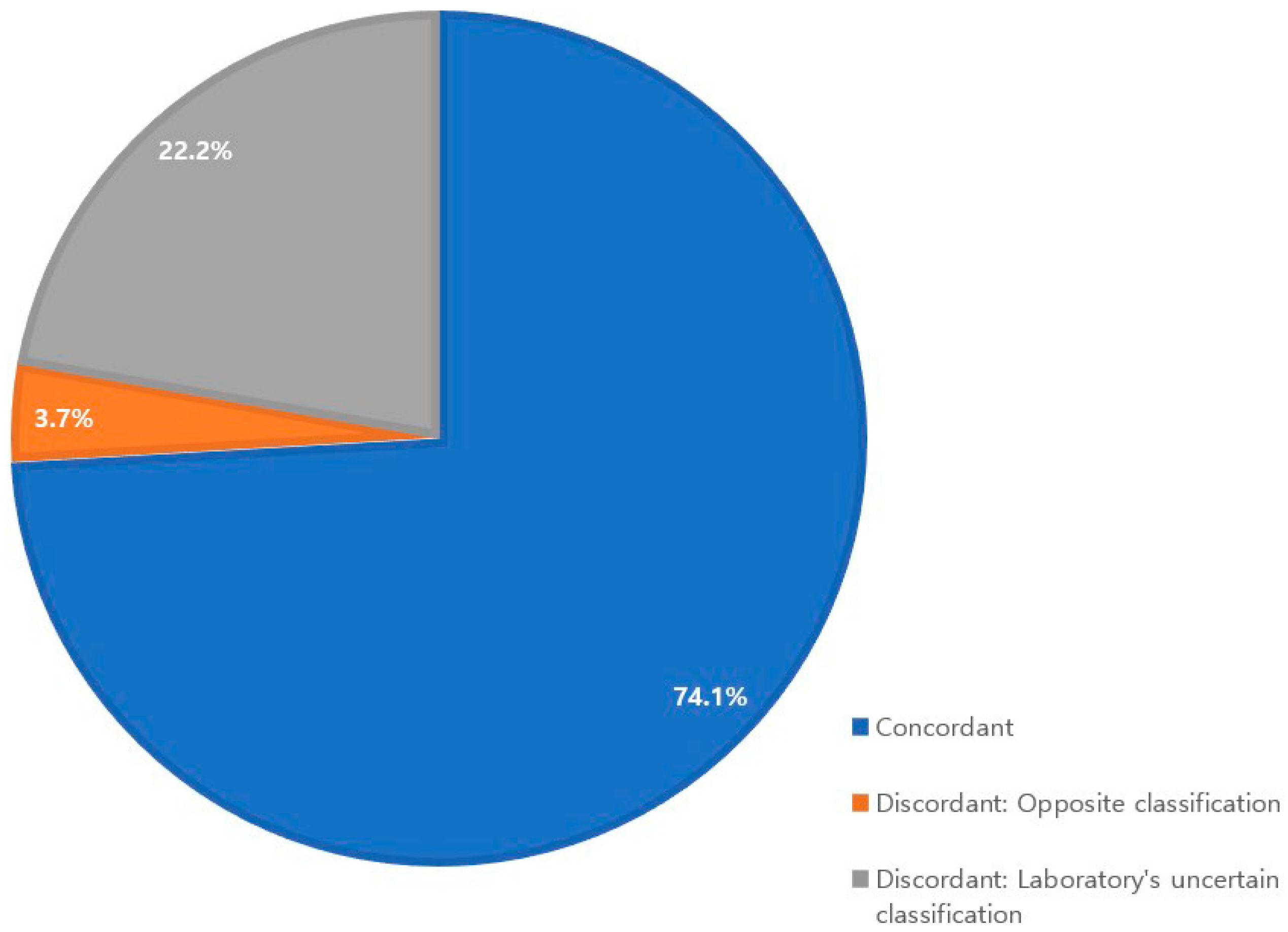
3.3. Concordant Rate
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA A Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Leif, W.; Ellisen, M.; Daniel, A.; Haber, M. Hereditary Breast Cancer. Annu. Rev. Med. 1998, 49, 425–436. [Google Scholar] [CrossRef]
- Yoshida, K.; Miki, Y. Role of BRCA1 and BRCA2 as regulators of DNA repair, transcription, and cell cycle in response to DNA damage. Cancer Sci. 2004, 95, 866–871. [Google Scholar] [CrossRef]
- Antoniou, A.; Pharoah, P.D.P.; Narod, S.; Risch, H.A.; Eyfjord, J.E.; Hopper, J.L.; Loman, N.; Olsson, H.; Johannsson, O.; Borg, Å.; et al. Average Risks of Breast and Ovarian Cancer Associated with BRCA1 or BRCA2 Mutations Detected in Case Series Unselected for Family History: A Combined Analysis of 22 Studies. Am. J. Hum. Genet. 2003, 72, 1117–1130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daly, M.B.; Pilarski, R.; Berry, M.; Buys, S.S.; Farmer, M.; Friedman, S.; Garber, J.E.; Kauff, N.D.; Khan, S.; Klein, C.; et al. NCCN Guidelines Insights: Genetic/Familial High-Risk Assessment: Breast and Ovarian, Version 2.2017. J. Natl. Compr. Cancer Netw. 2017, 15, 9–20. [Google Scholar] [CrossRef]
- Robson, M.; Im, S.-A.; Senkus, E.; Xu, B.; Domchek, S.M.; Masuda, N.; Delaloge, S.; Li, W.; Tung, N.; Armstrong, A.; et al. Olaparib for Metastatic Breast Cancer in Patients with a Germline BRCA Mutation. N. Engl. J. Med. 2017, 377, 523–533. [Google Scholar] [CrossRef]
- Litton, J.K.; Rugo, H.S.; Ettl, J.; Hurvitz, S.A.; Goncalves, A.; Lee, K.H.; Fehrenbacher, L.; Yerushalmi, R.; Mina, L.A.; Martin, M.; et al. Talazoparib in Patients with Advanced Breast Cancer and a Germline BRCA Mutation. N. Engl. J. Med. 2018, 379, 753–763. [Google Scholar] [CrossRef]
- Iglehart, J.D.; Silver, D.P. Synthetic lethality—A new direction in cancer-drug development. N. Engl. J. Med. 2009, 361, 189–191. [Google Scholar] [CrossRef] [Green Version]
- Gunderson, C.C.; Moore, K.N. BRACAnalysis CDx as a companion diagnostic tool for Lynparza. Expert Rev. Mol. Diagn. 2015, 15, 1111–1116. [Google Scholar] [CrossRef]
- Baldwin, A.L.; Cook-Deegan, R. Constructing narratives of heroism and villainy: Case study of Myriad’s BRACAnalysis((R)) compared to Genentech’s Herceptin((R)). Genome Med. 2013, 5, 8. [Google Scholar] [CrossRef] [Green Version]
- Conley, J.M.; Cook-Deegan, R.; Lazaro-Munoz, G. Myriad after MYRIAD: The proprietary data dilemma. North Carol. J. Law Technol. 2014, 15, 597–637. [Google Scholar]
- Balmaña, J.; Digiovanni, L.; Gaddam, P.; Walsh, M.F.; Joseph, V.; Stadler, Z.K.; Nathanson, K.L.; Garber, J.E.; Couch, F.J.; Offit, K.; et al. Conflicting Interpretation of Genetic Variants and Cancer Risk by Commercial Laboratories as Assessed by the Prospective Registry of Multiplex Testing. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2016, 34, 4071–4078. [Google Scholar] [CrossRef] [PubMed]
- Vail, P.J.; Morris, B.; van Kan, A.; Burdett, B.C.; Moyes, K.; Theisen, A.; Kerr, I.D.; Wenstrup, R.J.; Eggington, J.M. Comparison of locus-specific databases for BRCA1 and BRCA2 variants reveals disparity in variant classification within and among databases. J. Community Genet. 2015, 6, 351–359. [Google Scholar] [CrossRef] [Green Version]
- Gradishar, W.; Johnson, K.; Brown, K.; Mundt, E.; Manley, S. Clinical Variant Classification: A Comparison of Public Databases and a Commercial Testing Laboratory. Oncologist 2017, 22, 797–803. [Google Scholar] [CrossRef] [Green Version]
- Hicks, D.G.; Schiffhauer, L. Standardized Assessment of the HER2 Status in Breast Cancer by Immunohistochemistry. Lab. Med. 2011, 42, 459–467. [Google Scholar] [CrossRef] [Green Version]
- Richards, S.; Aziz, N.; Bale, S.; Bick, D.; Das, S.; Gastier-Foster, J.; Grody, W.W.; Hegde, M.; Lyon, E.; Spector, E.; et al. Standards and guidelines for the interpretation of sequence variants: A joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet. Med. Off. J. Am. Coll. Med Genet. 2015, 17, 405–424. [Google Scholar] [CrossRef] [PubMed]
- Eggington, J.M.; Bowles, K.R.; Moyes, K.; Manley, S.; Esterling, L.; Sizemore, S.; Rosenthal, E.; Theisen, A.; Saam, J.; Arnell, C.; et al. A comprehensive laboratory-based program for classification of variants of uncertain significance in hereditary cancer genes. Clin. Genet. 2014, 86, 229–237. [Google Scholar] [CrossRef]
- Lindor, N.M.; Guidugli, L.; Wang, X.; Vallée, M.P.; Monteiro, A.N.A.; Tavtigian, S.; Goldgar, D.E.; Couch, F.J. A review of a multifactorial probability-based model for classification of BRCA1 and BRCA2 variants of uncertain significance (VUS). Hum. Mutat. 2012, 33, 8–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petrucelli, N.; Daly, M.B.; Pal, T. BRCA1- and BRCA2-Associated Hereditary Breast and Ovarian Cancer. 1998 Sep 4 [Updated 2016 Dec 15]. In GeneReviews((R)); University of Washington, Seattle: Seattle, WA, USA, 1993–2021. Available online: https://www.ncbi.nlm.nih.gov/books/NBK1247/ (accessed on 19 January 2021).
- Szabo, C.; Masiello, A.; Ryan, J.F.; Brody, L.C. The breast cancer information core: Database design, structure, and scope. Hum. Mutat. 2000, 16, 123–131. [Google Scholar] [CrossRef]
- Bunyan, D.J.; Eccles, D.M.; Sillibourne, J.; Wilkins, E.; Thomas, N.S.; Shea-Simonds, J.; Duncan, P.J.; Curtis, C.E.; Robinson, D.O.; Harvey, J.F.; et al. Dosage analysis of cancer predisposition genes by multiplex ligation-dependent probe amplification. Br. J. Cancer 2004, 91, 1155. [Google Scholar] [CrossRef] [Green Version]
- Judkins, T.; Rosenthal, E.; Arnell, C.; Burbidge, L.A.; Geary, W.; Barrus, T.; Schoenberger, J.; Trost, J.; Wenstrup, R.J.; Roa, B.B. Clinical significance of large rearrangements in BRCA1 and BRCA2. Cancer 2012, 118, 5210–5216. [Google Scholar] [CrossRef] [Green Version]
- Seong, M.-W.; Cho, S.I.; Kim, K.H.; Chung, I.Y.; Kang, E.; Lee, J.W.; Park, S.K.; Lee, M.H.; Choi, D.H.; Yom, C.K.; et al. A multi-institutional study of the prevalence of BRCA1 and BRCA2 large genomic rearrangements in familial breast cancer patients. BMC Cancer 2014, 14, 645. [Google Scholar] [CrossRef] [Green Version]
- Palma, M.D.; Domchek, S.M.; Stopfer, J.; Erlichman, J.; Siegfried, J.D.; Tigges-Cardwell, J.; Mason, B.A.; Rebbeck, T.R.; Nathanson, K.L. The relative contribution of point mutations and genomic rearrangements in BRCA1 and BRCA2 in high-risk breast cancer families. Cancer Res. 2008, 68, 7006–7014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, K.; Jang, J.-H.; Lee, S.-T.; Yoon, K.-A.; Sook Lee, E.; Kim, J.-W.; Kong, S.-Y. Status of BRCA1/2 Genetic Testing Practices in Korea (2014). Lab Med Online 2018, 8, 107. [Google Scholar] [CrossRef] [Green Version]
- Park, H.S.; Ryu, J.M.; Park, J.S.; Im, S.-A.; Jung, S.-Y.; Kim, E.-K.; Park, W.-C.; Min, J.W.; Lee, J.; You, J.Y.; et al. Clinicopathological Features of Patients with the BRCA1 c.5339T>C (p.Leu1780Pro) Variant. J. Korean Cancer Assoc. 2020, 52, 680. [Google Scholar] [CrossRef] [Green Version]
- Ryu, J.M.; Kang, G.; Nam, S.J.; Kim, S.W.; Yu, J.; Lee, S.K.; Bae, S.Y.; Park, S.; Paik, H.J.; Kim, J.W.; et al. Suggestion of BRCA1 c.5339T>C (p.L1780P) variant confer from ‘unknown significance’ to ‘Likely pathogenic’ based on clinical evidence in Korea. Breast (Edinb. Scotl.) 2017, 33, 109–116. [Google Scholar] [CrossRef]
- Park, K.S.; Cho, E.Y.; Nam, S.J.; Ki, C.-S.; Kim, J.-W. Comparative analysis of BRCA1 and BRCA2 variants of uncertain significance in patients with breast cancer: A multifactorial probability-based model versus ACMG standards and guidelines for interpreting sequence variants. Genet. Med. 2016, 18, 1250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mundt, E.; Nix, P.; Brown, K.; Bowles, K.R.; Manley, S. Complexities of Variant Classification in Clinical Hereditary Cancer Genetic Testing. J. Clin. Oncol. 2017, 35, 3796–3799. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Value |
|---|---|
| Mean age (range), years | 41.8 (31–66) |
| Sex, n (%) | |
| Male | 0 (0.0%) |
| Female | 31 (100.0%) |
| Breast cancer hormone receptor, n (%) | |
| Estrogen receptor (ER) | 14 (45.2%) |
| Progesterone receptor (PR) | 13 (41.9%) |
| Human epidermal growth factor receptor 2 (HER2) | 1 (3.2%) |
| Subtype, n (%) | |
| Triple-negative | 17 (54.8%) |
| ER-positive | 14 (45.2%) |
| HER2-positive | 0 (0.0%) |
| Variable | Value |
|---|---|
| BRCA 1 gene sequencing from Myriad’s laboratory, n (%) | |
| Pathogenic/likely pathogenic variant | 13 (48.1%) |
| VUS | 0 (0.0%) |
| Benign/likely benign/variants not detected | 14 (51.9%) |
| BRCA 1 gene large genomic rearrangement from Myriad’s | |
| laboratory, n (%) | |
| Pathogenic/likely pathogenic variant | 1 (3.7%) |
| Benign/likely benign/variants not detected | 25 (92.6%) |
| Unable to analyze | 1 (3.7%) |
| BRCA 1 gene sequencing from Samsung Medical Center, n (%) | |
| Pathogenic/likely pathogenic variant | 13 (48.1%) |
| VUS | 0 (0.0%) |
| Benign/likely benign/variants not detected | 14 (51.9%) |
| Variable | Value |
|---|---|
| BRCA 2 gene sequencing from Myriad’s laboratory, n (%) | |
| Pathogenic/likely pathogenic variant | 10 (37.0%) |
| VUS | 1 (3.7%) |
| Benign/likely benign/variants not detected | 16 (59.3%) |
| BRCA 2 gene large genomic rearrangement from Myriad’s | |
| laboratory, n (%) | |
| Pathogenic/likely pathogenic variant | 0 (0.0%) |
| Benign/likely benign/variants not detected | 26 (96.3%) |
| Unable to analyze | 1 (3.7%) |
| BRCA 2 gene sequencing from Samsung Medical Center, n (%) | |
| Pathogenic/likely pathogenic variant | 10 (37.0%) |
| VUS | 7 (25.9%) |
| Benign/likely benign/variants not detected | 10 (37.0%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hong, J.; Lee, J.; Kwon, M.; Kim, J.-Y.; Kim, J.-W.; Ahn, J.S.; Im, Y.-H.; Park, Y.H. Local Laboratory Testing of Germline BRCA Mutations vs. Myriad: A Single-Institution Experience in Korea. Diagnostics 2021, 11, 370. https://doi.org/10.3390/diagnostics11020370
Hong J, Lee J, Kwon M, Kim J-Y, Kim J-W, Ahn JS, Im Y-H, Park YH. Local Laboratory Testing of Germline BRCA Mutations vs. Myriad: A Single-Institution Experience in Korea. Diagnostics. 2021; 11(2):370. https://doi.org/10.3390/diagnostics11020370
Chicago/Turabian StyleHong, Joohyun, Jiyun Lee, Minsuk Kwon, Ji-Yeon Kim, Jong-Won Kim, Jin Seok Ahn, Young-Hyuck Im, and Yeon Hee Park. 2021. "Local Laboratory Testing of Germline BRCA Mutations vs. Myriad: A Single-Institution Experience in Korea" Diagnostics 11, no. 2: 370. https://doi.org/10.3390/diagnostics11020370
APA StyleHong, J., Lee, J., Kwon, M., Kim, J. -Y., Kim, J. -W., Ahn, J. S., Im, Y. -H., & Park, Y. H. (2021). Local Laboratory Testing of Germline BRCA Mutations vs. Myriad: A Single-Institution Experience in Korea. Diagnostics, 11(2), 370. https://doi.org/10.3390/diagnostics11020370