
Morphological Characteristics of the Nasopalatine Canal and the Relationship with the Anterior Maxillary Bone—A Cone Beam Computed Tomography Study

 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Characteristics of Imaging Device and Software for Evaluation of Images
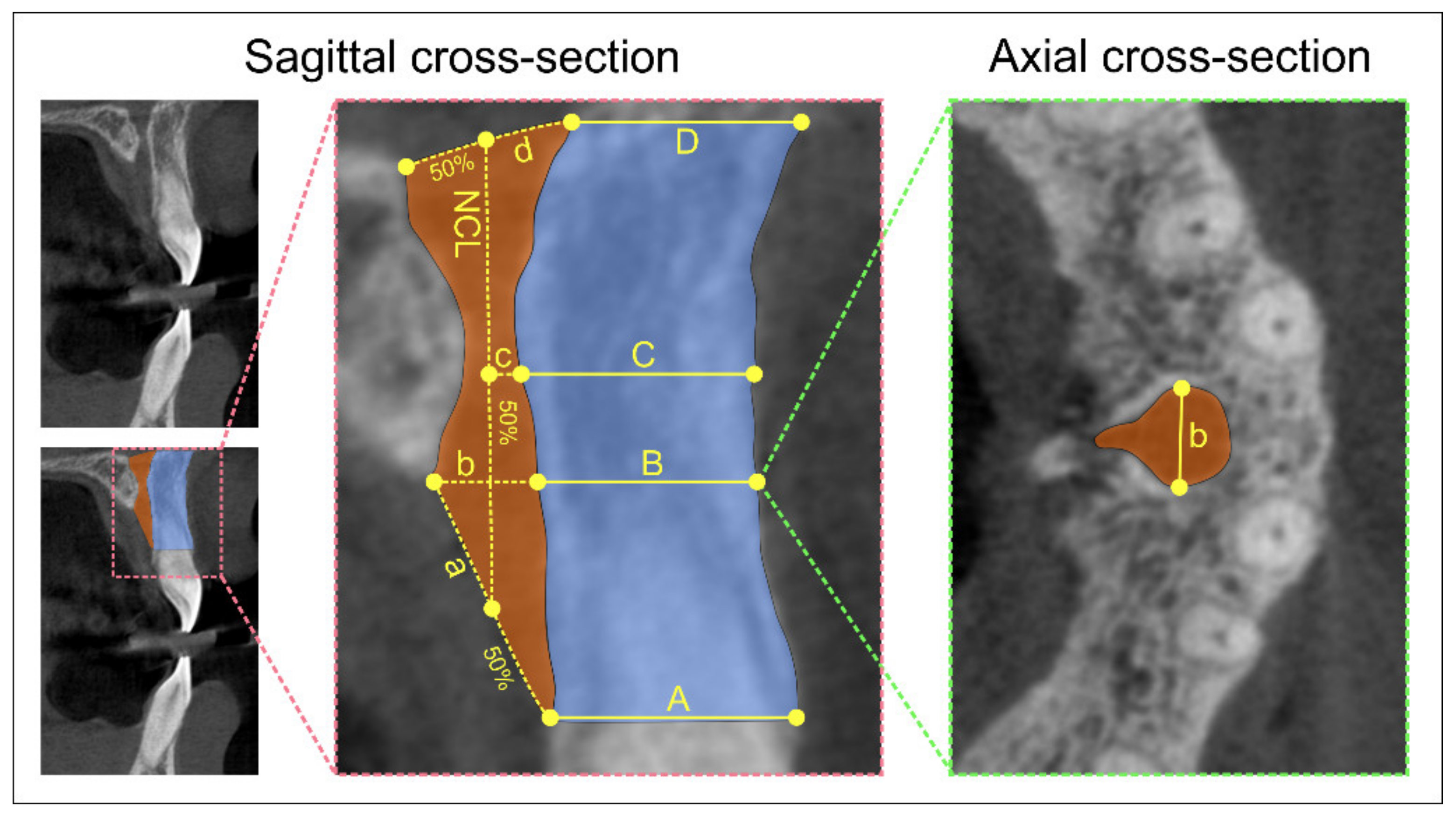
2.3. Nasopalatine Canal Morphology and Dimensions of Different Sections at Predefined Levels of the Nasopalatine Canal
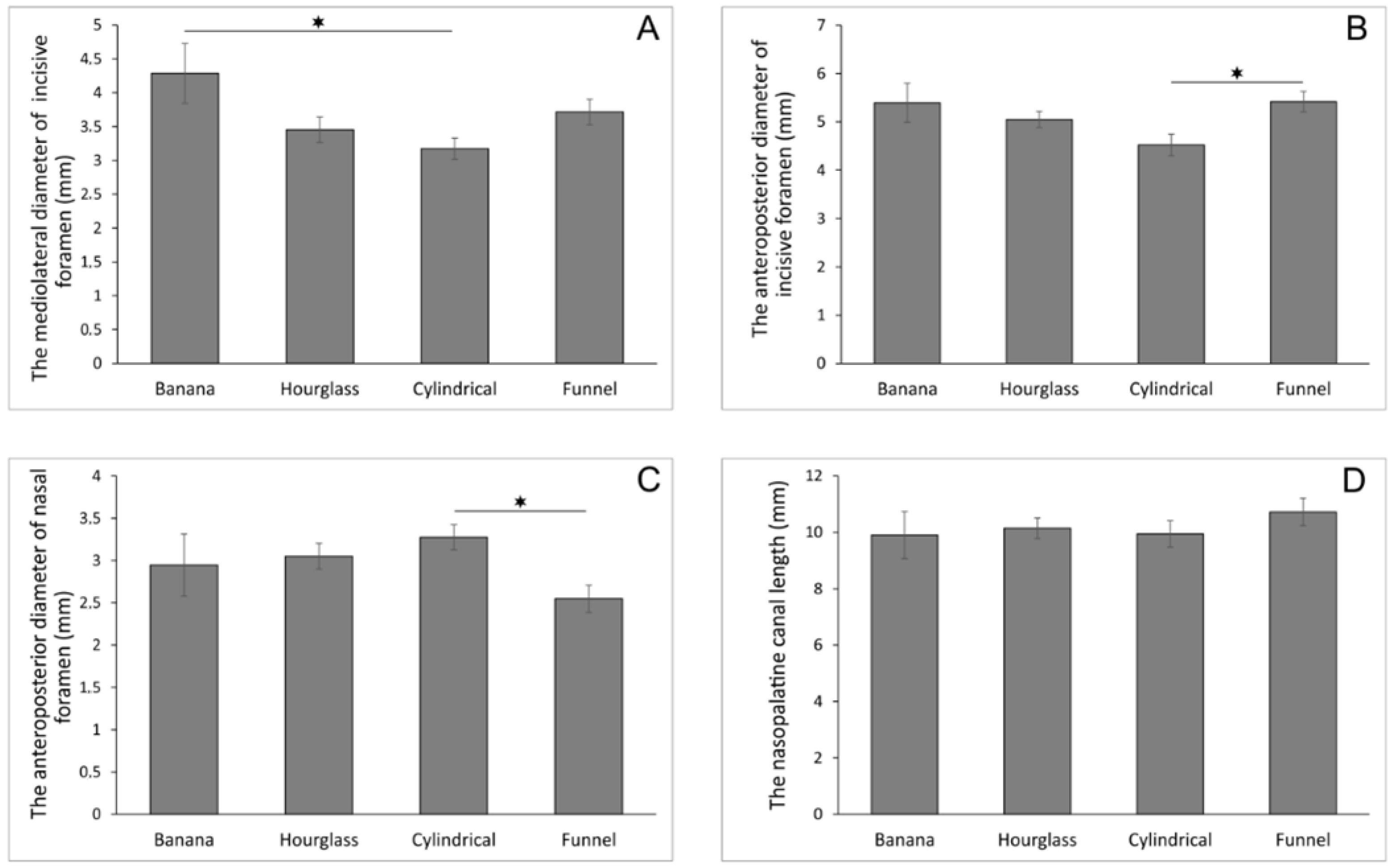
- Antero-posterior diameter (A-P) of nasal foramen (sagittal cross-section)
- Canal length (sagittal cross-section)
- Antero-posterior diameter (A-P) of incisive foramen (sagittal cross-section)
- Mediolateral diameter (M-L) of incisive foramen (axial cross-section).
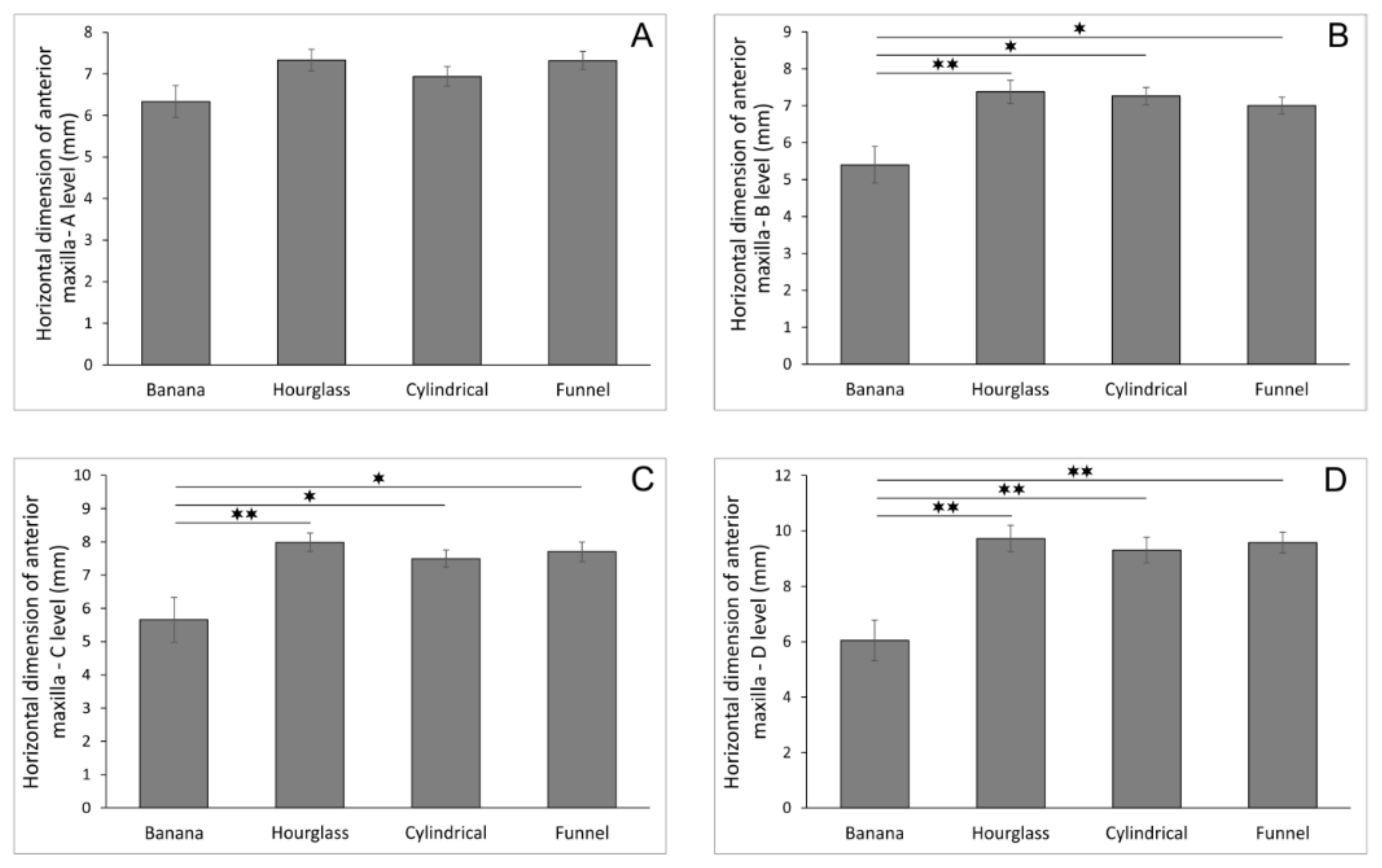
2.4. Horizontal Dimension of Anterior Maxilla
- A level: distance between the buccal border of incisive foramen and the cortical layer
- B level: distance between the buccal wall of the nasopalatine canal and the cortical layer using a horizontal line from the palatal border of the incisive foramen
- C level: distance between the buccal border at the midpoint level of NCL and the cortical layer
- D level: distance between the buccal border of nasal foramen and the cortical layer.
2.5. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jia, X.; Hu, W.; Meng, H. Relationship of central incisor implant placement to the ridge configuration anterior to the nasopalatine canal in dentate and partially edentulous individuals: A comparative study. PeerJ 2015, 3, e1315. [Google Scholar] [CrossRef] [Green Version]
- Liang, X.; Jacobs, R.; Martens, W.; Hu, Y.; Adriaensens, P.; Quirynen, M.; Lambrichts, I. Macro- and micro-anatomical, histological and computed tomography scan characterization of the nasopalatine canal. J. Clin. Periodontol. 2009, 36, 598–603. [Google Scholar] [CrossRef] [Green Version]
- Al-Ghurabi, Z.H.; Al-Bahrani, Z.M. Radiographic Assessment of Nasopalatine Canal Using Cone Beam Computed Tomography. J. Craniofac. Surg. 2020, 31, e4–e6. [Google Scholar] [CrossRef] [PubMed]
- Mardinger, O.; Namani-Sadan, N.; Chaushu, G.; Schwartz-Arad, D. Morphologic Changes of the Nasopalatine Canal Related to Dental Implantation: A Radiologic Study in Different Degrees of Absorbed Maxillae. J. Periodontol. 2008, 79, 1659–1662. [Google Scholar] [CrossRef] [PubMed]
- Güncü, G.N.; Yıldırım, Y.D.; Yılmaz, H.G.; Galindo-Moreno, P.; Velasco-Torres, M.; Al-Hezaimi, K.; Al-Shawaf, R.; Karabulut, E.; Wang, H.L.; Tözüm, T.F. Is there a gender difference in anatomic features of incisive canal and maxillary environmental bone? Clin. Oral Implants Res. 2013, 24, 1023–1026. [Google Scholar] [CrossRef] [Green Version]
- Etoz, M.; Sisman, Y. Evaluation of the nasopalatine canal and variations with cone-beam computed tomography. Surg. Radiol. Anat. 2014, 36, 805–812. [Google Scholar] [CrossRef] [PubMed]
- Safi, Y.; Moshfeghi, M.; Rahimian, S.; Kheirkhahi, M.; Manouchehri, M.E. Assessment of Nasopalatine Canal Anatomic Variations Using Cone Beam Computed Tomography in a Group of Iranian Population. Iran. J. Radiol. 2017, 14, e13480. [Google Scholar] [CrossRef]
- Bornstein, M.M.; Balsiger, R.; Sendi, P.; von Arx, T. Morphology of the nasopalatine canal and dental implant surgery: A radiographic analysis of 100 consecutive patients using limited cone-beam computed tomography. Clin. Oral Implants Res. 2011, 22, 295–301. [Google Scholar] [CrossRef]
- Gil-Marques, B.; Sanchis-Gimeno, J.A.; Brizuela-Velasco, A.; Perez-Bermejo, M.; Larrazábal-Morón, C. Differences in the shape and direction-course of the nasopalatine canal among dentate, partially edentulous and completely edentulous subjects. Anat. Sci. Int. 2019, 95, 76–84. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.-T.; Lee, J.-H.; Jeong, S.-N. Three-dimensional observations of the incisive foramen on cone-beam computed tomography image analysis. J. Periodontal Implant Sci. 2020, 50, 48–55. [Google Scholar] [CrossRef]
- Nikkerdar, N.; Khavid, A.; Golshah, A.; Karimi, A.; Ahmadi, M.M. Anatomical variations of the nasopalatine canal using cone beam computed tomography in a subpopulation residing in west of Iran. Ann. Dent. Spec. 2018, 6, 311–316. [Google Scholar]
- Soumya, P.; Koppolu, P.; Pathakota, K.R.; Chappidi, V. Maxillary Incisive Canal Characteristics: A Radiographic Study Using Cone Beam Computerized Tomography. Radiol. Res. Pract. 2019, 2019, 6151253. [Google Scholar] [CrossRef] [Green Version]
- Jayasinghe, R.M.; Hettiarachchi, P.V.K.S.; Fonseka, M.C.N.; Nanayakkara, D.; Jayasighe, R.D. Morphometric analysis of nasopalatine foramen in Sri Lankan population using CBCT. J. Oral Biol. Craniofac. Res. 2020, 10, 238–240. [Google Scholar] [CrossRef] [PubMed]
- Peñarrocha, M.; Carrillo, C.; Boronat, A.; Peñarrocha, M. Maximum use of the anterior maxillary buttress in severe maxillary atrophy with tilted, palatally positioned implants: A preliminary study. Int. J. Oral Maxillofac. Implants 2010, 25, 813–820. [Google Scholar] [PubMed]
- Peñarrocha, M.; Carrillo, C.; Boronat, A.; Peñarrocha, M. Retrospective study of 68 implants placed in the pterygomaxillary region using drills and osteotomes. Int. J. Oral Maxillofac. Implants 2009, 24, 720–726. [Google Scholar]
- Peñarrocha, D.; Candel, E.; Guirado, J.L.C.; Canullo, L.; Peñarrocha, M. Implants Placed in the Nasopalatine Canal to Rehabilitate Severely Atrophic Maxillae: A Retrospective Study with Long Follow-up. J. Oral Implantol. 2014, 40, 699–706. [Google Scholar] [CrossRef]
- Suter, V.G.A.; Jacobs, R.; Brücker, M.R.; Furher, A.; Frank, J.; Von Arx, T.; Bornstein, M.M. Evaluation of a possible association between a history of dentoalveolar injury and the shape and size of the nasopalatine canal. Clin. Oral Investig. 2015, 20, 553–561. [Google Scholar] [CrossRef]
- Buser, D.; Chappuis, V.; Belser, U.C.; Chen, S. Implant placement post extraction in esthetic single tooth sites: When immediate, when early, when late? Periodontology 2000 2016, 73, 84–102. [Google Scholar] [CrossRef]
- Khojastepour, L.; Haghnegahdar, A.; Keshtkar, M. Morphology and Dimensions of Nasopalatine Canal: A Radiographic Analysis Using Cone Beam Computed Tomography. J. Dent. (Shiraz) 2017, 18, 244–250. [Google Scholar]
- Kan, J.Y.K.; Rungcharassaeng, K.; Deflorian, M.; Weinstein, T.; Wang, H.-L.; Testori, T. Immediate implant placement and provisionalization of maxillary anterior single implants. Periodontology 2000 2018, 77, 197–212. [Google Scholar] [CrossRef]
- Bahşi, I.; Orhan, M.; Kervancıoğlu, P.; Yalçın, E.D.; Aktan, A.M. Anatomical evaluation of nasopalatine canal on cone beam computed tomography images. Folia Morphol. 2019, 78, 153–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Amery, S.M.; Nambiar, P.; Jamaludin, M.; John, J.; Ngeow, W.C. Cone Beam Computed Tomography Assessment of the Maxillary Incisive Canal and Foramen: Considerations of Anatomical Variations When Placing Immediate Implants. PLoS ONE 2015, 10, e0117251. [Google Scholar] [CrossRef] [PubMed]
- Tyndall, D.A.; Price, J.B.; Tetradis, S.; Ganz, S.D.; Hildebolt, C.; Scarfe, W.C. Position statement of the American Academy of Oral and Maxillofacial Radiology on selection criteria for the use of radiology in dental implantology with emphasis on cone beam computed tomography. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2012, 113, 817–826. [Google Scholar] [CrossRef]
- Alkanderi, A.; Al Sakka, Y.; Koticha, T.; Li, J.; Masood, F.; Suárez-López Del Amo, F. Incidence of nasopalatine canal perforation in relation to virtual implant placement: A cone beam computed tomography study. Clin. Implant Dent. Relat. Res. 2020, 22, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Peñarrocha, M.; Carrillo, C.; Uribe, R.; García, B. The nasopalatine canal as an anatomic buttress for implant placement in the severely atrophic maxilla: A pilot study. Int. J. Oral Maxillofac. Implants 2009, 24, 936–942. [Google Scholar] [PubMed]
- McCrea, S.J.J. Aberrations Causing Neurovascular Damage in the Anterior Maxilla during Dental Implant Placement. Case Rep. Dent. 2017, 2017, 5969643. [Google Scholar] [CrossRef] [Green Version]
- Kraut, R.A.; Boyden, D.K. Location of Incisive Canal in Relation to Central Incisor Implants. Implant Dent. 1998, 7, 221–225. [Google Scholar] [CrossRef]
- Fukuda, M.; Matsunaga, S.; Odaka, K.; Oomine, Y.; Kasahara, M.; Yamamoto, M.; Abe, S. Three-dimensional analysis of incisive canals in human dentulous and edentulous maxillary bones. Int. J. Implant Dent. 2015, 1, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hakbilen, S.; Mağat, G. Evaluation of anatomical and morphological characteristics of the nasopalatine canal in a Turkish population by cone beam computed tomography. Folia Morphol. 2018, 77, 527–535. [Google Scholar] [CrossRef] [Green Version]
- Tözüm, T.F.; Güncü, G.N.; Yıldırım, Y.D.; Yılmaz, H.G.; Galindo-Moreno, P.; Velasco-Torres, M.; Al-Hezaimi, K.; Al-Sadhan, R.; Karabulut, E.; Wang, H.L.; et al. Evaluation of Maxillary Incisive Canal Characteristics Related to Dental Implant Treatment With Computerized Tomography: A Clinical Multicenter Study. J. Periodontol. 2012, 83, 337–343. [Google Scholar] [CrossRef]
- Şekerci, A.E.; Buyuk, S.K.; Cantekin, K. Cone-beam computed tomographic analysis of the morphological characterization of the nasopalatine canal in a pediatric population. Surg. Radiol. Anat. 2014, 36, 925–932. [Google Scholar] [CrossRef] [PubMed]
- Thakur, A.R.; Burde, K.; Guttal, K.; Naikmasur, V.G. Anatomy and morphology of the nasopalatine canal using cone-beam computed tomography. Imaging Sci. Dent. 2013, 43, 273–281. [Google Scholar] [CrossRef] [Green Version]
- Mraiwa, N.; Jacobs, R.; Van Cleynenbreugel, J.; Sanderink, G.; Schutyser, F.; Suetens, P.; Van Steenberghe, D.; Quirynen, M. The nasopalatine canal revisited using 2D and 3D CT imaging. Dentomaxillofac. Radiol. 2004, 33, 396–402. [Google Scholar] [CrossRef] [PubMed]
- Görürgöz, C.; Öztaş, B. Anatomıc characterıstıcs and dimensions of the nasopalatine canal: A radiographic study using cone-beam computed tomography. Folia Morphol. 2020, 1–21. [Google Scholar] [CrossRef]
- Gönül, Y.; Bucak, A.; Atalay, Y.; Beker-Acay, M.; Çalişkan, A.; Sakarya, G.; Soysal, N.; Cimbar, M.; Özbek, M. MDCT evalu-ation of nasopalatine canal morphometry and variations: An analysis of 100 patients. Diagn. Interv. Imaging 2016, 97, 1165–1172. [Google Scholar] [CrossRef] [PubMed]
- Salemi, F.; Moghadam, F.A.; Shakibai, Z.; Farhadian, M. Three-dimensional Assessment of the Nasopalatine Canal and the Surrounding Bone Using Cone-beam Computed Tomography. J. Periodontol. Implant Dent. 2016, 8, 1–7. [Google Scholar] [CrossRef]
- Nasseh, I.; Aoun, G.; Sokhn, S. Assessment of the Nasopalatine Canal: An Anatomical Study. Acta Inform. Med. 2017, 25, 34–38. [Google Scholar] [CrossRef] [Green Version]
- Mounir, M.; Beheiri, G.; El-Beialy, W. Assessment of marginal bone loss using full thickness versus partial thickness flaps for alveolar ridge splitting and immediate implant placement in the anterior maxilla. Int. J. Oral Maxillofac. Surg. 2014, 43, 1373–1380. [Google Scholar] [CrossRef]
- Jornet, P.L.; Boix, P.P.; Perez, A.S.; Boracchia, A. Morphological Characterization of the Anterior Palatine Region Using Cone Beam Computed Tomography. Clin. Implant Dent. Relat. Res. 2014, 17, 459–464. [Google Scholar] [CrossRef]
- Panda, M.; Shankar, T.; Raut, A.; Dev, S.; Kar, A.K.; Hota, S. Cone beam computerized tomography evaluation of incisive canal and anterior maxillary bone thickness for placement of immediate implants. J. Indian Prosthodont. Soc. 2018, 18, 356–363. [Google Scholar] [CrossRef]
- Schropp, L.; Wenzel, A.; Kostopoulos, L.; Karring, T. Bone healing and soft tissue contour changes following single-tooth ex-traction: A clinical and radiographic 12-month prospective study. Int. J. Periodontics Restor. Dent. 2003, 23, 313–323. [Google Scholar]
- Chan, H.L.; Garaicoa, P.C.; Suarez, F.; Monje, A.; Benavides, E.; Oh, T.J.; Wang, H.L. Incidence of implant buccal plate fenestration in the esthetic zone: A cone beam computed tomography study. Int. J. Oral Maxillofac. Implants 2014, 29, 171–177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, H.C.; Kang, D.U.; Baek, H.; Hong, J.Y.; Shin, S.Y.; Chung, J.H.; Herr, Y.; Shin, S.I. Cone-beam computed tomographic analysis of the alveolar ridge profile and virtual implant placement for the anterior maxilla. J. Periodontal Implant Sci. 2019, 49, 299–309. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| The Sections of the NPC | Mean ± SEM | The Horizontal Dimension of Anterior Maxilla | Mean ± SEM |
|---|---|---|---|
| The M-L diameter of incisive foramen | 3.53 ± 0.11 | A level | 7.11 ± 0.13 |
| The A-P diameter of incisive foramen | 5.04 ± 0.12 | B level | 7.03 ± 0.15 |
| The A-P diameter of nasal foramen | 2.93 ± 0.01 | C level | 7.52 ± 0.17 |
| The NPC length | 10.26 ± 0.25 | D level | 9.22 ± 0.25 |
| The Sections of the NPC | The Levels of Anterior Maxilla Horizontal Dimension | |||
|---|---|---|---|---|
| A Level | B Level | C Level | D Level | |
| The M-L diameter of incisive foramen | y = −0.2679x + 5.4396 R2 = 0.1103 p = 0.0003 | y = −0.5650x + 8.4428 R2 = 0.1941 p = 1.04 × 10−6 | y = −0.3020x + 5.8057 R2 = 0.2319 p = 6.67 × 10−8 | y = −0.1070x + 4.5191 R2 = 0.0650 p = 0.0064 |
| The A-P diameter of incisive foramen | y = −0.0344x + 7.2914 R2 = 0.0010 p = 0.7408 | y = −0.1272x + 7.6751 R2 = 0.0106 p = 0.2784 | y = −0.0508x + 7.7840 R2 = 0.0013 p = 0.7041 | y = −0.0150x + 9.2974 R2 = 5 × 10−5 p = 0.9402 |
| The A-P diameter of nasal foramen | y = −0.3100x + 8.0271 R2 = 0.0473 p = 0.0207 | y = −0.3233x + 7.9812 R2 = 0.0401 p = 0.0333 | y = −0.6940x + 9.5630 R2 = 0.1431 p = 3.61 × 10−5 | y = −0.8513x + 11.718 R2 = 0.0965 p = 0.0008 |
| The NPC length | y = 0.0063x + 7.0533 R2 = 0.0001 p = 0.8991 | y = 0.0041x + 6.9908 R2 = 5 × 10−5 p = 0.9415 | y = 0.0010x + 7.5173 R2 = 2 × 10−6 p = 0.9872 | y = 0.2360x + 6.7993 R2 = 0.0554 p = 0.0120 |
| The Correlation between the M-L Diameter of the Incisive Foramen and Anterior Maxilla Dimensions on Different Levels | The NPC Shape at the Sagittal Cross-Section | |||
|---|---|---|---|---|
| Banana | Hourglass | Cylindrical | Funnel | |
| The M-L diameter of incisive foramen vs. A level | y = −0.5544x + 8.7112 R2 = 0.4044 p = 0.0481 | y = −0.7374x + 9.8784 R2 = 0.2845 p = 0.0034 | y = 0.0428x + 6.8023 R2 = 0.0008 p = 0.8721 | y = −0.4862x + 9.1267 R2 = 0.1759 p = 0.0070 |
| The M-L diameter of incisive foramen vs. B level | y = −0.8315x + 8.9629 R2 = 0.5505 p = 0.0140 | y = −0.8146x + 10.1860 R2 = 0.2389 p = 0.0083 | y = 0.1325x + 6.8406 R2 = 0.0079 p = 0.6106 | y = −0.6788x + 9.5250 R2 = 0.3035 p = 0.0002 |
| The M-L diameter of incisive foramen vs. C level | y = −1.0048x + 9.9655 R2 = 0.4335 p = 0.0385 | y = −0.7770x + 10.6700 R2 = 0.2767 p = 0.0040 | y = −0.3666x + 8.6585 R2 = 0.0479 p = 0.2065 | y = −0.7856x + 10.6210 R2 = 0.2541 p = 0.0009 |
| The M-L diameter of incisive foramen vs. D level | y = 0.0223x + 5.9534 R2 = 0.0002 p = 0.9704 | y = −0.6056x + 11.8200 R2 = 0.0579 p = 0.2172 | y = −1.1468x + 12.9510 R2 = 0.1498 p = 0.0216 | y = −0.2214x + 10.4040 R2 = 0.0128 p = 0.4871 |
| The Correlation between the A-P Diameter of the Incisive Foramen and Anterior Maxilla Dimensions on Different Levels | The NPC Shape at the Sagittal Cross-Section | |||
|---|---|---|---|---|
| Banana | Hourglass | Cylindrical | Funnel | |
| The A-P diameter of incisive foramen vs. A level | y = 0.0561x + 6.0321 R2 = 0.0034 p = 0.8720 | y = −0.2439x + 8.5649 R2 = 0.0242 p = 0.4288 | y = −0.0008x + 6.9415 R2 = 5 × 10−7 p = 0.9966 | y = −0.0770x + 7.7374 R2 = 0.0056 p = 0.6454 |
| The A-P diameter of incisive foramen vs. B level | y = −0.2531x + 6.7647 R2 = 0.0424 p = 0.5681 | y = −0.7213x + 11.0180 R2 = 0.1459 p = 0.0448 | y = 0.2314x + 6.2150 R2 = 0.0486 p = 0.2032 | y = −0.1054x + 7.5743 R2 = 0.0093 p = 0.5528 |
| The A-P diameter of incisive foramen vs. C level | y = 0.1953x + 4.6053 R2 = 0.0136 p = 0.7482 | y = −0.4346x + 10.1830 R2 = 0.0674 p = 0.1820 | y = 0.1094x + 7.0005 R2 = 0.0086 p = 0.5971 | y = −0.0848x + 8.1612 R2 = 0.0038 p = 0.7062 |
| The A-P diameter of incisive foramen vs. D level | y = 1.0952x + 0.1390 R2 = 0.3653 p = 0.0642 | y = −0.2964x + 11.2260 R2 = 0.0108 p = 0.5985 | y = −0.1947x + 10.1920 R2 = 0.0087 p = 0.5948 | y = 0.0883x + 9.1033 R2 = 0.0026 p = 0.7548 |
| The Correlation between the A-P Diameter of Nasal Foramen and Anterior Maxilla Dimensions on Different Levels | The NPC Shape at the Sagittal Cross-Section | |||
|---|---|---|---|---|
| Banana | Hourglass | Cylindrical | Funnel | |
| The A-P diameter of nasal foramen vs. A level | y = −0.6705x + 8.3104 R2 = 0.4050 p = 0.0479 | y = −0.0976x + 7.6306 R2 = 0.0033 p = 0.7718 | y = 0.0802x + 6.6754 R2 = 0.0025 p = 0.7751 | y = −0.5043x + 8.6054 R2 = 0.1371 p = 0.0186 |
| The A-P diameter of nasal foramen vs. B level | y = −0.9056x + 8.0668 R2 = 0.4470 p = 0.0345 | y = −0.4522x + 8.7537 R2 = 0.0486 p = 0.2596 | y = 0.1208x + 6.8657 R2 = 0.0059 p = 0.6607 | y = −0.5650x + 8.4428 R2 = 0.1523 p = 0.0128 |
| The A-P diameter of nasal foramen vs. C level | y = −1.3293x + 9.5751 R2 = 0.5194 p = 0.0187 | y = −0.8444x + 10.5630 R2 = 0.2157 p = 0.0127 | y = −0.2501x + 8.3141 R2 = 0.0200 p = 0.4181 | y = −0.8599x + 9.8926 R2 = 0.2204 p = 0.0022 |
| The A-P diameter of nasal foramen vs. D level | y = −0.2573x + 6.8070 R2 = 0.0166 p = 0.7228 | y = −0.9414x + 12.6010 R2 = 0.0924 p = 0.1157 | y = −1.4884x + 14.1850 R2 = 0.2259 p = 0.0039 | y = −0.7158x + 11.4050 R2 = 0.0968 p = 0.0507 |
| The Correlation between the NPC Length and Anterior Maxilla Dimensions on Different Levels | The NPC Shape at the Sagittal Cross-Section | |||
|---|---|---|---|---|
| Banana | Hourglass | Cylindrical | Funnel | |
| The NPC length vs. A level | y = 0.2198x + 4.1584 R2 = 0.2267 p = 0.1642 | y = 0.1037x + 6.2811 R2 = 0.0208 p = 0.4641 | y = 0.0689x + 6.2531 R2 = 0.0180 p = 0.4420 | y = −0.1210x + 8.6179 R2 = 0.0717 p = 0.0947 |
| The NPC length vs. B level | y = 0.3059x + 2.3691 R2 = 0.2658 p = 0.1271 | y = 0.0901x + 6.4601 R2 = 0.0108 p = 0.5986 | y = 0.0921x + 6.3458 R2 = 0.0334 p = 0.2930 | y = −0.1359x + 8.4604 R2 = 0.0801 p = 0.0768 |
| The NPC length vs. C level | y = 0.1986x + 3.6923 R2 = 0.0604 p = 0.4937 | y = 0.1174x + 6.7960 R2 = 0.0234 p = 0.4373 | y = 0.0300x + 7.1967 R2 = 0.0028 p = 0.7627 | y = −0.1082x + 8.8615 R2 = 0.0317 p = 0.2717 |
| The NPC length vs. D level | y = −0.0657x + 6.6996 R2 = 0.0056 p = 0.8366 | y = 0.3583x + 6.0940 R2 = 0.0750 p = 0.1585 | y = 0.2601x + 6.7251 R2 = 0.0672 p = 0.1325 | y = 0.2045x + 7.3890 R2 = 0.0718 p = 0.0946 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Milanovic, P.; Selakovic, D.; Vasiljevic, M.; Jovicic, N.U.; Milovanović, D.; Vasovic, M.; Rosic, G. Morphological Characteristics of the Nasopalatine Canal and the Relationship with the Anterior Maxillary Bone—A Cone Beam Computed Tomography Study. Diagnostics 2021, 11, 915. https://doi.org/10.3390/diagnostics11050915
Milanovic P, Selakovic D, Vasiljevic M, Jovicic NU, Milovanović D, Vasovic M, Rosic G. Morphological Characteristics of the Nasopalatine Canal and the Relationship with the Anterior Maxillary Bone—A Cone Beam Computed Tomography Study. Diagnostics. 2021; 11(5):915. https://doi.org/10.3390/diagnostics11050915
Chicago/Turabian StyleMilanovic, Pavle, Dragica Selakovic, Milica Vasiljevic, Nemanja U. Jovicic, Dragan Milovanović, Miroslav Vasovic, and Gvozden Rosic. 2021. "Morphological Characteristics of the Nasopalatine Canal and the Relationship with the Anterior Maxillary Bone—A Cone Beam Computed Tomography Study" Diagnostics 11, no. 5: 915. https://doi.org/10.3390/diagnostics11050915
APA StyleMilanovic, P., Selakovic, D., Vasiljevic, M., Jovicic, N. U., Milovanović, D., Vasovic, M., & Rosic, G. (2021). Morphological Characteristics of the Nasopalatine Canal and the Relationship with the Anterior Maxillary Bone—A Cone Beam Computed Tomography Study. Diagnostics, 11(5), 915. https://doi.org/10.3390/diagnostics11050915