
Outcomes of Esophageal Cancer after Esophagectomy in the Era of Early Injection Laryngoplasty

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Principle of Diagnosing and Managing UVFP
2.2. Office-Based Injection Laryngoplasty
2.3. Assessments of Patients with Unilateral Vocal Fold Paralysis
2.4. LEMG Examination
2.5. Glottal Position: Normalized Glottal Gap Area
2.6. Laboratory Voice Analysis
2.7. Quality of Life: Voice Outcome Survey (VOS) and Short-Form 36 (SF-36)
2.8. Statistical Analysis
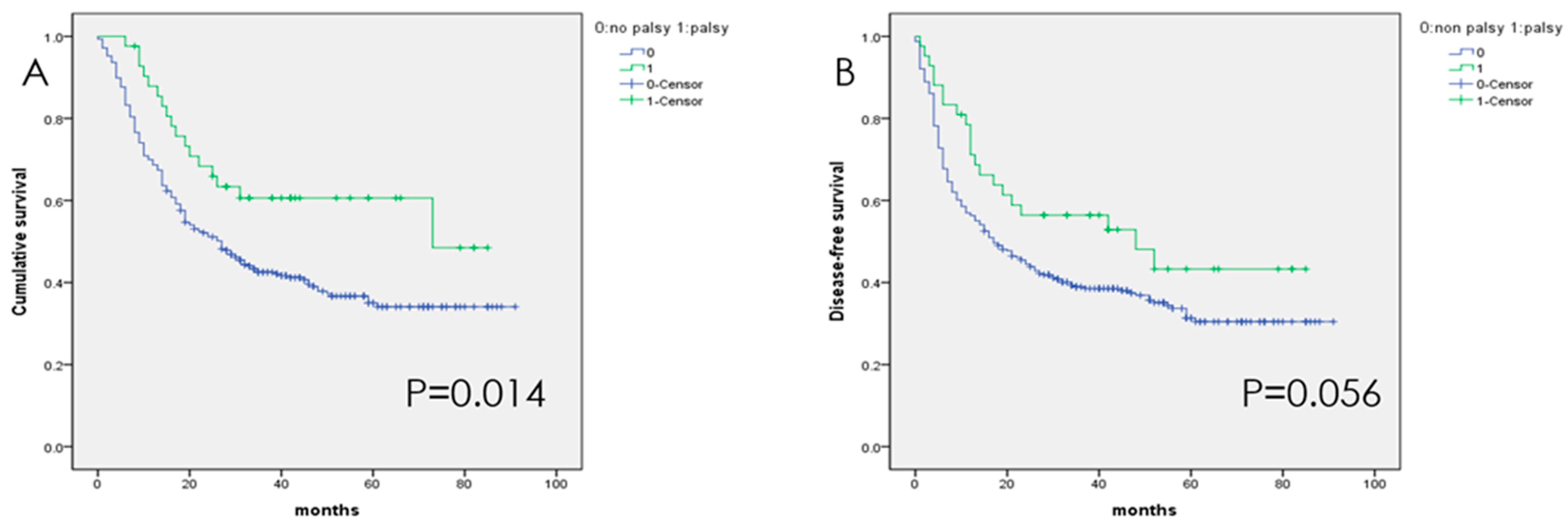
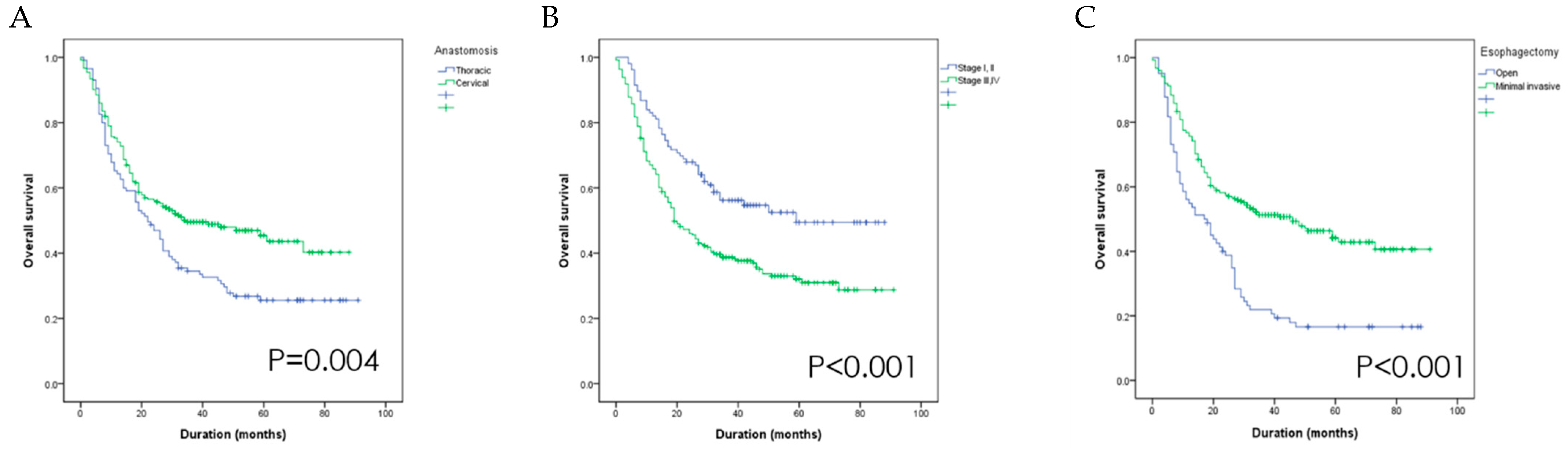
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Koyanagi, K.; Igaki, H.; Iwabu, J.; Ochiai, H.; Tachimori, Y. Recurrent Laryngeal Nerve Paralysis after Esophagectomy: Respiratory Complications and Role of Nerve Reconstruction. Tohoku J. Exp. Med. 2015, 237, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Shimizu, H.; Shiozaki, A.; Fujiwara, H.; Konishi, H.; Kosuga, T.; Komatsu, S.; Ichikawa, D.; Okamoto, K.; Otsuji, E. Short- and Long-term Progress of Recurrent Laryngeal Nerve Paralysis After Subtotal Esophagectomy. Anticancer Res. 2017, 37, 2019–2023. [Google Scholar] [CrossRef]
- Zhong, D.; Zhou, Y.; Li, Y.; Wang, Y.; Zhou, W.; Cheng, Q.; Chen, L.; Zhao, J.; Li, X.; Yan, X. Intraoperative recurrent laryngeal nerve monitoring: A useful method for patients with esophageal cancer. Dis. Esophagus 2014, 27, 444–451. [Google Scholar] [CrossRef] [PubMed]
- Sato, Y.; Kosugi, S.; Aizawa, N.; Ishikawa, T.; Kano, Y.; Ichikawa, H.; Hanyu, T.; Hirashima, K.; Bamba, T.; Wakai, T. Risk Factors and Clinical Outcomes of Recurrent Laryngeal Nerve Paralysis After Esophagectomy for Thoracic Esophageal Carcinoma. World J. Surg. 2016, 40, 129–136. [Google Scholar] [CrossRef]
- Chao, Y.K.; Hsieh, M.J.; Liu, Y.H.; Liu, H.P. Lymph Node Evaluation in Robot-Assisted Versus Video-Assisted Thoracoscopic Esophagectomy for Esophageal Squamous Cell Carcinoma: A Propensity-Matched Analysis. World J. Surg. 2018, 42, 590–598. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Li, Y.; Sun, H.; Zhang, R.; Liu, X.; Liu, S.; Wang, Z.; Zheng, Y.; Yu, Y.; Chen, X.; et al. Analysis of the associated factors for severe weight loss after minimally invasive McKeown esophagectomy. Thorac. Cancer 2019, 10, 209–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, S.Y.; Kim, D.J.; Suh, J.W.; Byun, G.E. Risk Factors for Weight Loss 1 Year After Esophagectomy and Gastric Pull-up for Esophageal Cancer. J. Gastrointest. Surg. 2018, 22, 1137–1143. [Google Scholar] [CrossRef]
- Llaguna, O.H.; Kim, H.J.; Deal, A.M.; Calvo, B.F.; Stitzenberg, K.B.; Meyers, M.O. Utilization and morbidity associated with placement of a feeding jejunostomy at the time of gastroesophageal resection. J. Gastrointest. Surg. 2011, 15, 1663–1669. [Google Scholar] [CrossRef]
- Ryan, A.M.; Rowley, S.P.; Healy, L.A.; Flood, P.M.; Ravi, N.; Reynolds, J.V. Post-oesophagectomy early enteral nutrition via a needle catheter jejunostomy: 8-year experience at a specialist unit. Clin. Nutr. 2006, 25, 386–393. [Google Scholar] [CrossRef]
- Sakatoku, Y.; Fukaya, M.; Miyata, K.; Itatsu, K.; Nagino, M. Clinical value of a prophylactic minitracheostomy after esophagectomy: Analysis in patients at high risk for postoperative pulmonary complications. BMC Surg. 2017, 17, 120. [Google Scholar] [CrossRef] [PubMed]
- Fang, T.J.; Hsin, L.J.; Chung, H.F.; Chiang, H.C.; Li, H.Y.; Wong, A.M.; Pei, Y.C. Office-Based Intracordal Hyaluronate Injections Improve Quality of Life in Thoracic-Surgery-Related Unilateral Vocal Fold Paralysis. Medicine 2015, 94, e1787. [Google Scholar] [CrossRef] [PubMed]
- Pei, Y.C.; Fang, T.J.; Li, H.Y.; Wong, A.M. Cricothyroid muscle dysfunction impairs vocal fold vibration in unilateral vocal fold paralysis. Laryngoscope 2014, 124, 201–206. [Google Scholar] [CrossRef] [PubMed]
- Fang, T.J.; Pei, Y.C.; Hsin, L.J.; Lin, W.N.; Lee, L.A.; Li, H.Y.; Wong, A.M. Quantitative laryngeal electromyography assessment of cricothyroid function in patients with unilateral vocal fold paralysis. Laryngoscope 2015, 125, 2530–2535. [Google Scholar] [CrossRef] [PubMed]
- Omori, K.; Kacker, A.; Slavit, D.H.; Blaugrund, S.M. Quantitative videostroboscopic measurement of glottal gap and vocal function: An analysis of thyroplasty type I. Ann. Otol. Rhinol. Laryngol. 1996, 105, 280–285. [Google Scholar] [CrossRef] [PubMed]
- Gliklich, R.E.; Glovsky, R.M.; Montgomery, W.W. Validation of a voice outcome survey for unilateral vocal cord paralysis. Otolaryngol. Head Neck Surg. 1999, 120, 153–158. [Google Scholar] [PubMed]
- Fang, T.J.; Li, H.Y.; Gliklich, R.E.; Chen, Y.H.; Wang, P.C. Assessment of Chinese-version voice outcome survey in patients with unilateral vocal cord paralysis. Otolaryngol. Head Neck Surg. 2007, 136, 752–756. [Google Scholar] [CrossRef] [PubMed]
- Lu, J.-F.R.; Tseng, H.-M.; Tsai, Y.-J. Assessment of health-related quality of life in Taiwan (I): Development and psychometric testing of SF-36 Taiwan Version. Taiwan J. Pub. Health 2003, 22, 501–511. [Google Scholar]
- Tseng, H.-M.; Lu, J.-F.R.; Tsai, Y.-J. Assessment of health-related quality of life (II): Norming and validation of SF-36 Taiwan Version. Taiwan J. Pub. Health 2003, 22, 512–518. [Google Scholar]
- Deng, J.; Su, Q.; Ren, Z.; Wen, J.; Xue, Z.; Zhang, L.; Chu, X. Comparison of short-term outcomes between minimally invasive McKeown and Ivor Lewis esophagectomy for esophageal or junctional cancer: A systematic review and meta-analysis. Oncotargets Ther. 2018, 11, 6057–6069. [Google Scholar] [CrossRef] [Green Version]
- Zhou, J.; Chen, H.; Lu, J.J.; Xiang, J.; Zhang, Y.; Hu, H.; Zhou, X.; Luo, X.; Yang, F.; Tam, J. Application of a modified McKeown procedure (thoracoscopic esophageal mobilization three-incision esophagectomy) in esophageal cancer surgery: Initial experience with 30 cases. Dis. Esophagus 2009, 22, 687–693. [Google Scholar] [CrossRef]
- Luketich, J.D.; Pennathur, A.; Awais, O.; Levy, R.M.; Keeley, S.; Shende, M.; Christie, N.A.; Weksler, B.; Landreneau, R.J.; Abbas, G.; et al. Outcomes after minimally invasive esophagectomy: Review of over 1000 patients. Ann. Surg. 2012, 256, 95–103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pertl, L.; Zacherl, J.; Mancusi, G.; Gachter, J.N.; Asari, R.; Schoppmann, S.; Bigenzahn, W.; Schneider-Stickler, B. High risk of unilateral recurrent laryngeal nerve paralysis after esophagectomy using cervical anastomosis. Eur. Arch. Oto-Rhino-Laryng. 2011, 268, 1605–1610. [Google Scholar] [CrossRef] [PubMed]
- Akiyama, Y.; Iwaya, T.; Endo, F.; Nikai, H.; Sato, K.; Baba, S.; Chiba, T.; Kimura, T.; Takahara, T.; Nitta, H.; et al. Evaluation of the need for routine feeding jejunostomy for enteral nutrition after esophagectomy. J. Thorac. Dis. 2018, 10, 6854–6862. [Google Scholar] [CrossRef] [PubMed]
- Weijs, T.J.; van Eden, H.W.J.; Ruurda, J.P.; Luyer, M.D.P.; Steenhagen, E.; Nieuwenhuijzen, G.A.P.; van Hillegersberg, R. Routine jejunostomy tube feeding following esophagectomy. J. Thorac. Dis. 2017, 9, S851–S860. [Google Scholar] [CrossRef] [PubMed]
- Scholtemeijer, M.G.; Seesing, M.F.J.; Brenkman, H.J.F.; Janssen, L.M.; van Hillegersberg, R.; Ruurda, J.P. Recurrent laryngeal nerve injury after esophagectomy for esophageal cancer: Incidence, management, and impact on short- and long-term outcomes. J. Thorac. Dis. 2017, 9, S868–S878. [Google Scholar] [CrossRef] [Green Version]
- Pei, Y.C.; Fang, T.J.; Hsin, L.J.; Li, H.Y.; Wong, A.M. Early hyaluronate injection improves quality of life but not neural recovery in unilateral vocal fold paralysis: An open-label randomized controlled study. Restor. Neurol. Neurosci. 2015, 33, 121–130. [Google Scholar] [CrossRef] [Green Version]
- Song, P.C.; Sung, C.K.; Franco, R.A., Jr. Voice outcomes after endoscopic injection laryngoplasty with hyaluronic acid stabilized gel. Laryngoscope 2010, 120 (Suppl. 4), S199. [Google Scholar] [CrossRef]
- Grant, J.R.; Hartemink, D.A.; Patel, N.; Merati, A.L. Acute and subacute awake injection laryngoplasty for thoracic surgery patients. J. Voice 2008, 22, 245–250. [Google Scholar] [CrossRef]
- Graboyes, E.M.; Bradley, J.P.; Meyers, B.F.; Nussenbaum, B. Efficacy and safety of acute injection laryngoplasty for vocal cord paralysis following thoracic surgery. Laryngoscope 2011, 121, 2406–2410. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| All | Non-UVFP * | UVFP | p | |
|---|---|---|---|---|
| Sex (male/female) | 339/19 | 300/16 | 39/3 | 0.459 |
| Age (years) | 55.42 ± 9.41 | 55.50 ± 9.61 | 54.63 ± 7.39 | 0.665 |
| Paralysis | 316 | 42 | ||
| Side (left/right) | 36/6 | |||
| Hyaluronate injection (Y/N) | 31/11 | |||
| Recovery (Y/N) | 4/38 | |||
| Thoracic anastomosis/cervical anastomosis | 115/241 | 112/204 | 3/39 | 0.000 |
| Thoracotomy/MIE ** | 82/274 | 81/235 | 1/41 | |
| Stage | 11 | 9 | 3 | |
| IA | ||||
| IB | 23 | 21 | 2 | |
| IIA | 20 | 16 | 4 | |
| IIB | 54 | 48 | 6 | |
| IIIA | 90 | 80 | 80 | |
| IIIB | 79 | 70 | 70 | |
| IIIC | 63 | 57 | 57 | |
| IV | 14 | 14 | 0 | |
| Unknown | 2 | 1 | 1 | |
| Alive/dead | 147/209 | 123/193 | 25/17 |
| HR | 95% CI | p | ||
|---|---|---|---|---|
| Vocal fold motility | Palsy | 1 | 0.889–2.454 | 0.133 |
| Intact | 1.48 | |||
| Surgical procedure | MIE | 1 | 1.408–3.072 | <0.001 |
| Open | 2.08 | |||
| Stage | I, II | 1 | 1.243–2.375 | 0.001 |
| III, IV | 1.72 | |||
| Anastomosis | Cervical | 0.91 | 0.626–1.311 | 0.600 |
| Thoracic | 1 | |||
| Parameters | n = 29 | n = 13 | |
|---|---|---|---|
| HA Injection | No HA Injection | p Value | |
| Glottal gap | |||
| Closed-phase NGGA | 11.67 ± 12.80 | 3.11 ± 4.09 | 0.037 * |
| 20.55 ± 12.93 | 0.072 | ||
| 8.87 ± 6.21 | 0.705 | ||
| LEMG | |||
| Normal side of TA-LCA (turn/s) | 1112.92 ± 410.48 | 904.39 ± 277.32 | 0.131 |
| Lesion side of TA-LCA (turn/s) | 297.20 ± 227.69 | 582.73 ± 634.41 | 0.173 |
| Turn ratio of TA-LCA | 0.33 ± 0.31 | 0.69 ± 0.72 | 0.034 * |
| 914.05 ± 346.93 | 0.531 | ||
| 704.05 ± 301.44 | 0.814 | ||
| 0.83 ± 0.38 | 0.510 | ||
| Voice laboratory analysis | |||
| Maximum phonation time (s) | 3.93 ± 2.84 | 10.83 ± 7.34 | 0.016 * |
| SZ ratio | 2.05 ± 1.03 | 1.41 ± 0.93 | 0.097 |
| Fundamental frequency (Hz) | 156.97 ± 51.97 | 131.62 ± 37.71 | 0.197 |
| Jitter (%) | 5.18 ± 5.35 | 1.71 ± 1.12 | 0.051 |
| Shimmer (dB) | 0.98 ± 0.65 | 0.48 ± 0.29 | 0.024 * |
| Harmonic-to-noise ratio | 5.15 ± 2.99 | 7.37 ± 5.79 | 0.128 |
| Vos | |||
| Voice outcome survey score | 30.71 ± 12.15 | 58.50 ± 24.04 | 0.005 ** |
| SF-36 | |||
| Physical functioning | 60.36 ± 25.27 | 80.50 ± 13.22 | 0.003 ** |
| Role limitation due to physical health | 16.96 ± 34.06 | 30.00 ± 43.78 | 0.342 |
| Role limitation due to emotional problem | 30.92 ± 40.50 | 70.00 ± 42.89 | 0.014 * |
| Vitality | 47.50 ± 21.54 | 54.50 ± 11.65 | 0.337 |
| Mental health | 63.29 ± 18.60 | 64.80 ± 13.96 | 0.816 |
| Social functioning | 47.45 ± 25.51 | 65.00 ± 26.87 | 0.074 |
| Bodily pain | 63.61 ± 24.91 | 74.75 ± 25.51 | 0.235 |
| General health perceptions | 41.79 ± 22.53 | 55.00 ± 19.72 | 0.110 |
| Parameters | Baseline (a) | 1 Month Post HIL (b) | 3 Month Post HIL (c) | 6 Month Post HIL (d) | p Value | Significant Comparison † |
|---|---|---|---|---|---|---|
| Glottal gap | n =31 | n =28 | n =25 | n =20 | ||
| Closed-phase NGGA | 11.3751 ± 12.4384 | 2.0742 ± 2.1528 | 4.844 ± 4.598 | 2.9502 ± 4.2794 | 0.009 ** | ab, ac, ad |
| Voice laboratory analysis | ||||||
| Maximum phonation time (s) | 3.8067 ± 2.7767 | 7.5948 ± 6.1624 | 7.2396 ± 6.0317 | 7.5043 ± 5.9946 | <0.001 *** | ab, ac, ad |
| SZ ratio | 2.1704 ± 1.1316 | 1.4734 ± 0.9986 | 1.6349 ± 1.0143 | 1.6355 ± 1.2799 | 0.072 | ab |
| Fundamental frequency (Hz) | 154.8151 ± 51.1644 | 142.7253 ± 32.9603 | 144.229 ± 34.116 | 146.8968 ± 38.6546 | 0.774 | |
| Jitter (%) | 5.1929 ± 5.1651 | 1.988 ± 1.043 | 2.8703 ± 1.9116 | 2.2739 ± 1.5287 | 0.050 | ab |
| Shimmer (dB) | 1.008 ± 0.6403 | 0.4184 ± 0.17 | 0.5679 ± 0.3546 | 0.6688 ± 0.7645 | 0.042 * | ab, ac |
| Harmonic-to-noise ratio | 4.9816 ± 3.0341 | 7.3429 ± 2.6551 | 6.3831 ± 1.8776 | 7.2882 ± 2.5396 | 0.004 ** | ab, ac, ad |
| Voice outcome survey | ||||||
| Score of voice outcome survey | 30.3448 ± 12.0957 | 58.0357 ± 18.7251 | 55 ± 21.7945 | 62.1053 ± 25.6209 | <0.001 *** | ab, ac, ad |
| SF-36 | ||||||
| Physical functioning | 60.83 ± 24.88 | 66.03 ± 25.05 | 71.54 ± 20.29 | 68.75 ± 25.64 | 0.053 | ab, ac |
| Role limitation due to physical health problems | 15.83 ± 33.14 | 26.72 ± 38.92 | 36.54 ± 44.85 | 41.25 ± 48.17 | 0.053 | ac, ad |
| Role limitation due to emotional problems | 28.86 ± 39.86 | 48.23 ± 43.28 | 51.22 ± 44.48 | 50 ± 51.3 | 0.034 * | ac |
| Vitality | 47.67 ± 20.79 | 51.03 ± 17.44 | 51.73 ± 19.23 | 57.75 ± 21.12 | 0.001 ** | ac, ad |
| Mental health | 62.13 ± 18.49 | 66.34 ± 13.07 | 66.62 ± 15.76 | 66 ± 19.1 | 0.107 | ac |
| Social functioning | 46.38 ± 25 | 61.76 ± 26.94 | 66.98 ± 26.2 | 71.25 ± 24.03 | <0.001 *** | ab, ac, ad |
| Bodily pain | 62.72 ± 24.72 | 80.02 ± 22.82 | 77.71 ± 21.22 | 79.28 ± 21.59 | 0.003 ** | ab, ac, ad |
| General health perceptions | 41.33 ± 23.19 | 49.83 ± 20.55 | 45.96 ± 20.4 | 50.75 ± 20.41 | 0.360 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fang, T.-J.; Pei, Y.-C.; Lu, Y.-A.; Chung, H.-F.; Chiang, H.-C.; Li, H.-Y.; Wong, A.M.K. Outcomes of Esophageal Cancer after Esophagectomy in the Era of Early Injection Laryngoplasty. Diagnostics 2021, 11, 914. https://doi.org/10.3390/diagnostics11050914
Fang T-J, Pei Y-C, Lu Y-A, Chung H-F, Chiang H-C, Li H-Y, Wong AMK. Outcomes of Esophageal Cancer after Esophagectomy in the Era of Early Injection Laryngoplasty. Diagnostics. 2021; 11(5):914. https://doi.org/10.3390/diagnostics11050914
Chicago/Turabian StyleFang, Tuan-Jen, Yu-Cheng Pei, Yi-An Lu, Hsiu-Feng Chung, Hui-Chen Chiang, Hsueh-Yu Li, and Alice M. K. Wong. 2021. "Outcomes of Esophageal Cancer after Esophagectomy in the Era of Early Injection Laryngoplasty" Diagnostics 11, no. 5: 914. https://doi.org/10.3390/diagnostics11050914
APA StyleFang, T. -J., Pei, Y. -C., Lu, Y. -A., Chung, H. -F., Chiang, H. -C., Li, H. -Y., & Wong, A. M. K. (2021). Outcomes of Esophageal Cancer after Esophagectomy in the Era of Early Injection Laryngoplasty. Diagnostics, 11(5), 914. https://doi.org/10.3390/diagnostics11050914