
Effects of Sex and Age on Fat Fraction, Diffusion-Weighted Image Signal Intensity and Apparent Diffusion Coefficient in the Bone Marrow of Asymptomatic Individuals: A Cross-Sectional Whole-Body MRI Study

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Population
2.2. Acquisition Protocol
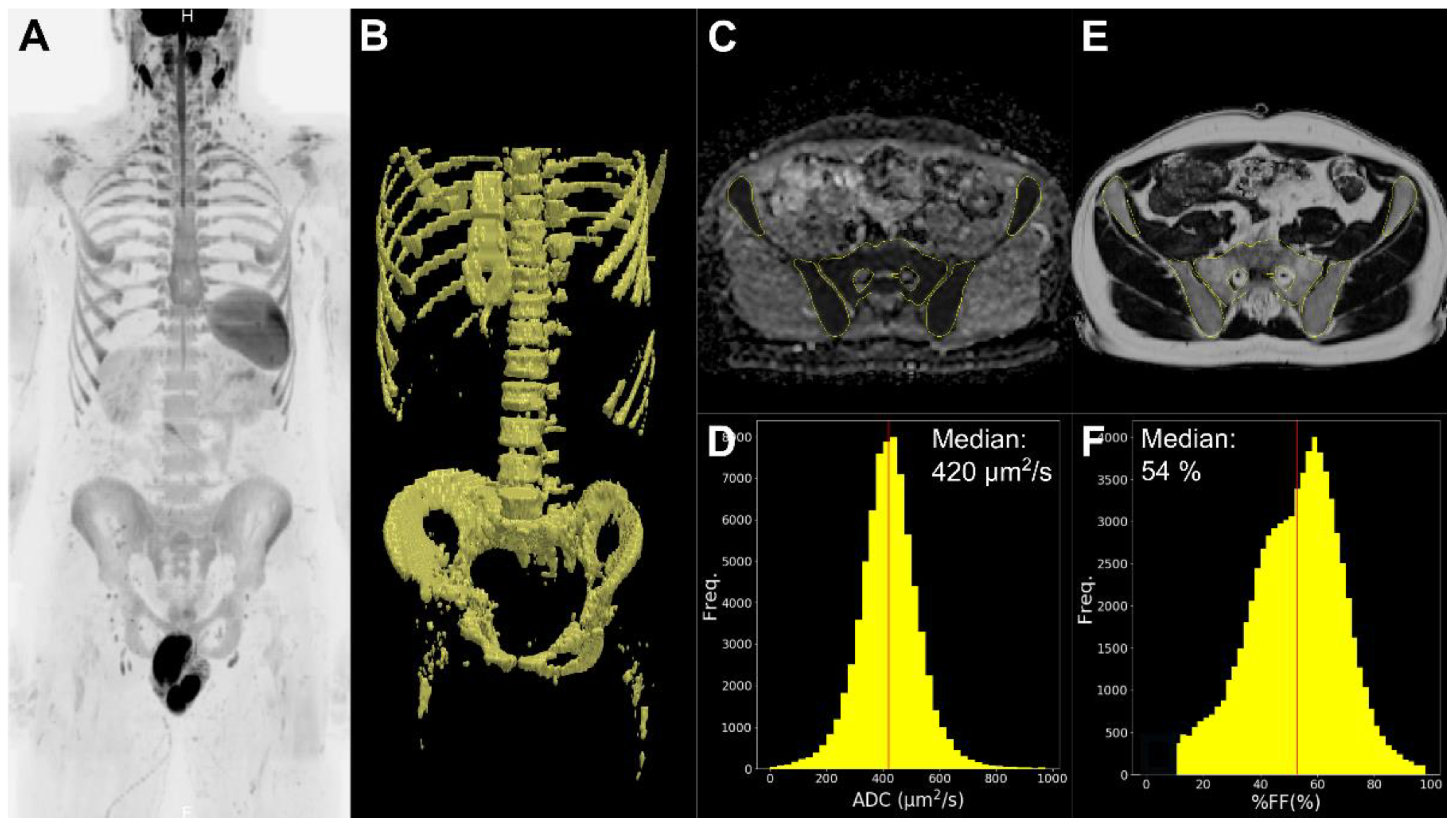
2.3. Image Processing and Analysis
2.4. Statistical Analysis
3. Results
3.1. Population
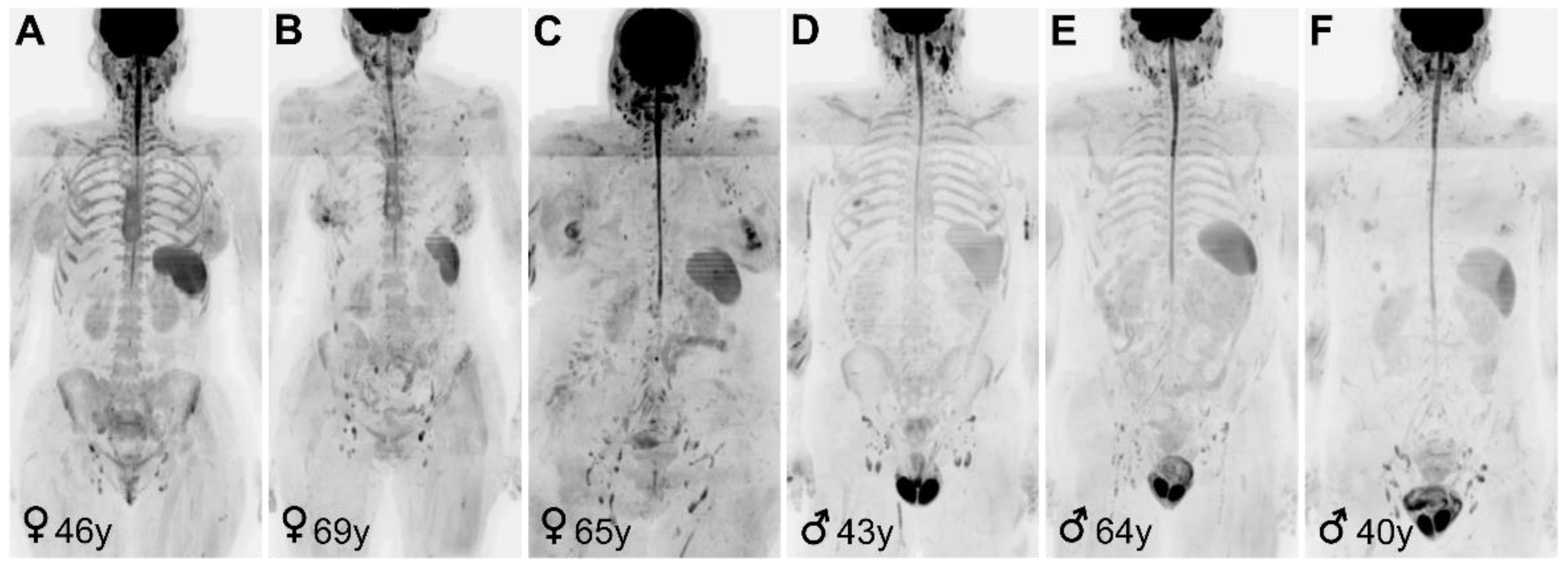
3.2. Overall Distribution of Relative %FF, Signal Intensity in DW Images and ADC and Their Correlation with Age
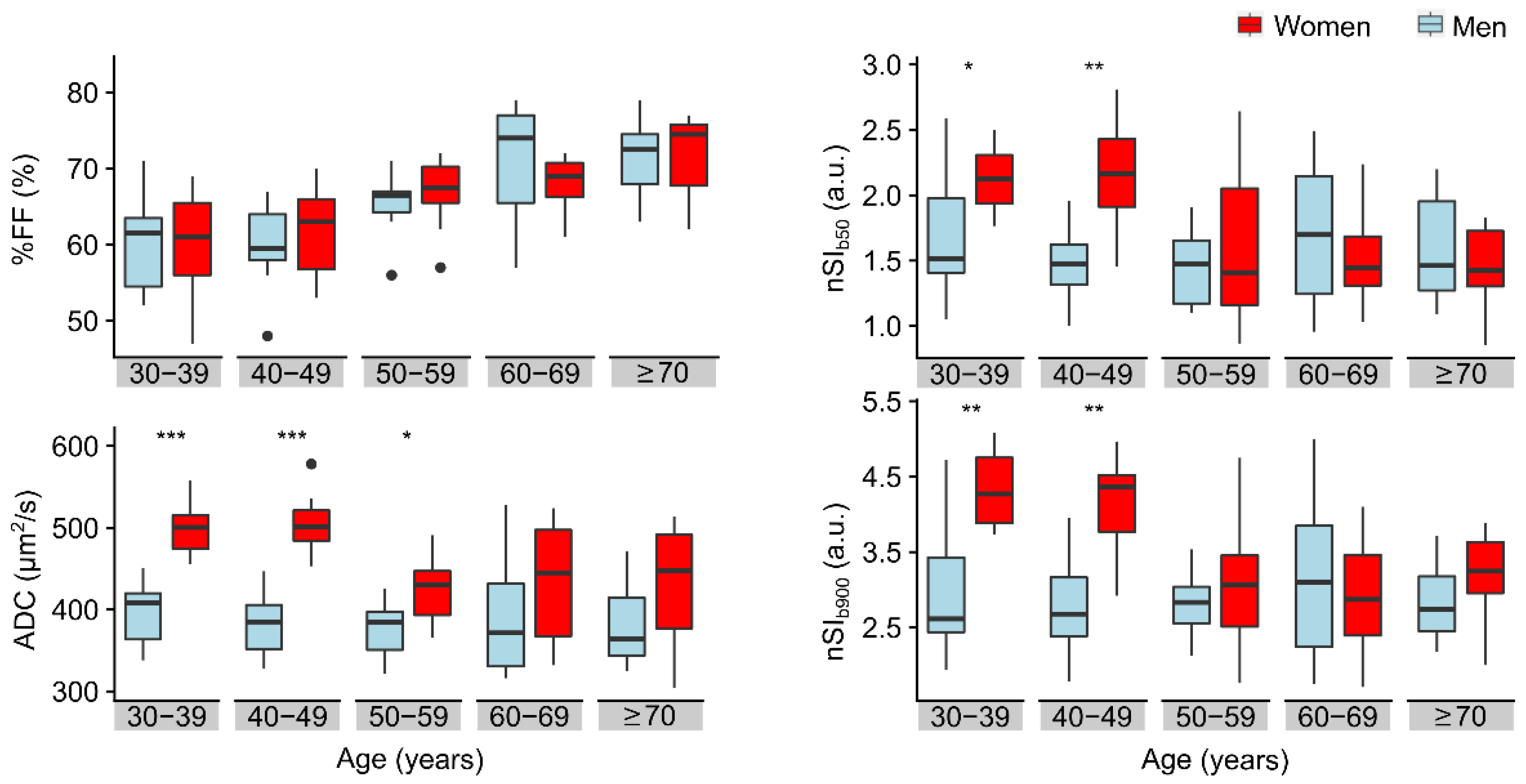
3.3. Effect of Sex and Age on Relative %FF and Signal Intensity in DW Images and ADC
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
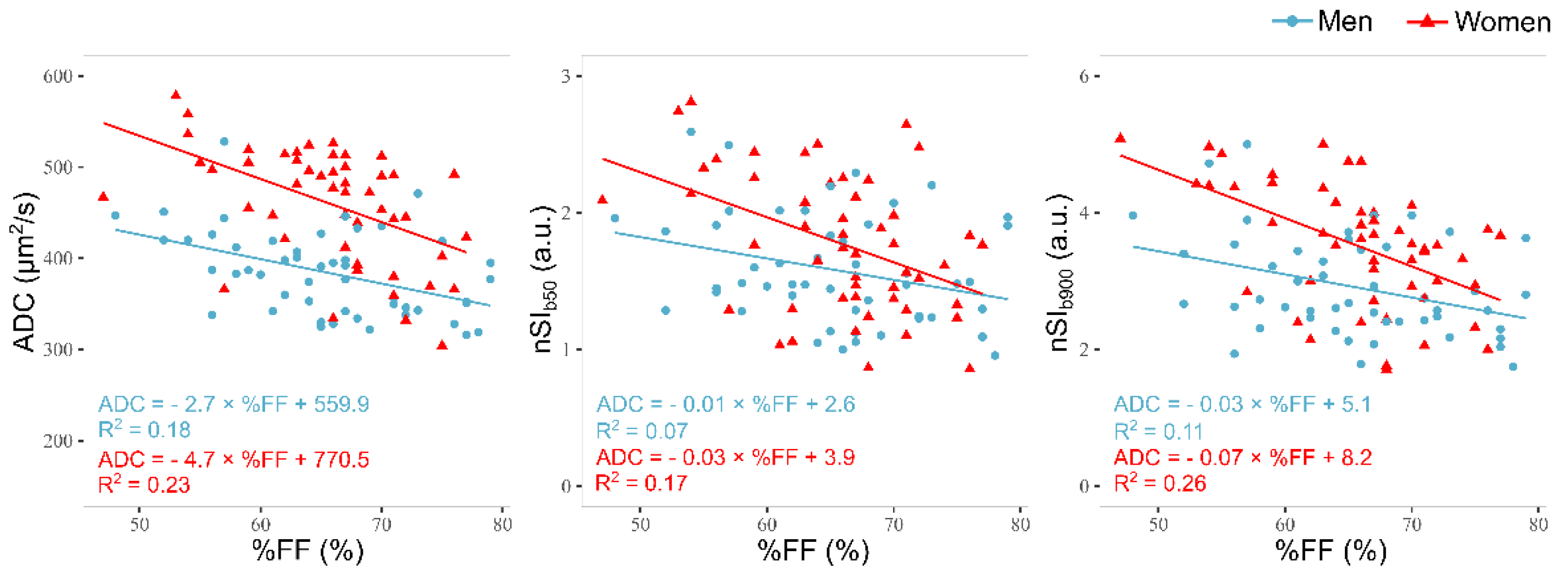
Appendix A.1. Correlation of Relative %FF with Signal Intensity in DW-Images and ADC

Appendix A.2. Post Hoc Analysis
References
- Lecouvet, F.; Larbi, A.; Pasoglou, V.; Omoumi, P.; Tombal, B.; Michoux, N.; Malghem, J.; Lhommel, R.; Berg, B.C.V. MRI for response assessment in metastatic bone disease. Eur. Radiol. 2013, 23, 1986–1997. [Google Scholar] [CrossRef]
- Padhani, A.R.; Makris, A.; Gall, P.; Collins, D.J.; Tunariu, N.; de Bono, J.S. Therapy monitoring of skeletal metastases with whole-body diffusion MRI. J. Magn. Reson. Imaging 2014, 39, 1049–1078. [Google Scholar] [CrossRef] [PubMed]
- Giles, S.L.; Messiou, C.; Collins, D.J.; Morgan, V.A.; Simpkin, C.J.; West, S.; Davies, F.E.; Morgan, G.J.; DeSouza, N.M. Whole-Body Diffusion-weighted MR Imaging for Assessment of Treatment Response in Myeloma. Radiology 2014, 271, 785–794. [Google Scholar] [CrossRef] [Green Version]
- Petralia, G.; Padhani, A.R.; Pricolo, P.; Zugni, F.; Martinetti, M.; Summers, P.E.; Grazioli, L.; Colagrande, S.; Giovagnoni, A.; Bellomi, M.; et al. Whole-body magnetic resonance imaging (WB-MRI) in oncology: Recommendations and key uses. Radiol. Med. 2019, 124, 218–233. [Google Scholar] [CrossRef]
- Zugni, F.; Padhani, A.R.; Koh, D.-M.; Summers, P.E.; Bellomi, M.; Petralia, G. Whole-body magnetic resonance imaging (WB-MRI) for cancer screening in asymptomatic subjects of the general population: Review and recommendations. Cancer Imaging 2020, 20, 34. [Google Scholar] [CrossRef]
- Petralia, G.; Koh, D.-M.; Attariwala, R.; Busch, J.J.; Eeles, R.; Karow, D.; Lo, G.G.; Messiou, C.; Sala, E.; Vargas, H.A.; et al. Oncologically Relevant Findings Reporting and Data System (ONCO-RADS): Guidelines for the Acquisition, Interpretation, and Reporting of Whole-Body MRI for Cancer Screening. Radiology 2021, 201740. [Google Scholar] [CrossRef]
- Kosmin, M.; Padhani, A.R.; Gogbashian, A.; Woolf, D.; Ah-See, M.-L.; Ostler, P.; Sutherland, S.; Miles, D.; Noble, J.; Koh, D.-M.; et al. Comparison of Whole-Body MRI, CT, and Bone Scintigraphy for Response Evaluation of Cancer Therapeutics in Metastatic Breast Cancer to Bone. Radiology 2020, 297, 622–629. [Google Scholar] [CrossRef]
- Zugni, F.; Ruju, F.; Pricolo, P.; Alessi, S.; Iorfida, M.; Colleoni, M.A.; Bellomi, M.; Petralia, G. The added value of whole-body magnetic resonance imaging in the management of patients with advanced breast cancer. PLoS ONE 2018, 13, e0205251. [Google Scholar] [CrossRef] [PubMed]
- Donners, R.; Blackledge, M.; Tunariu, N.; Messiou, C.; Merkle, E.M.; Koh, D.-M. Quantitative Whole-Body Diffusion-Weighted MR Imaging. Magn. Reson. Imaging Clin. N. Am. 2018, 26, 479–494. [Google Scholar] [CrossRef]
- Summers, P.; Saia, G.; Colombo, A.; Pricolo, P.; Zugni, F.; Alessi, S.; Marvaso, G.; Jereczek-Fossa, B.A.; Bellomi, M.; Petralia, G. Whole-body magnetic resonance imaging: Technique, guidelines and key applications. Ecancermedicalscience 2021, 15. [Google Scholar] [CrossRef]
- Coleman, R.E.; Croucher, P.I.; Padhani, A.R.; Clézardin, P.; Chow, E.; Fallon, M.; Guise, T.; Colangeli, S.; Capanna, R.; Costa, L. Bone metastases. Nat. Rev. Dis. Prim. 2020, 6, 1–28. [Google Scholar] [CrossRef]
- Messiou, C.; Hillengass, J.; Delorme, S.; Lecouvet, F.E.; Moulopoulos, L.; Collins, D.J.; Blackledge, M.D.; Abildgaard, N.; Østergaard, B.; Schlemmer, H.-P.; et al. Guidelines for Acquisition, Interpretation, and Reporting of Whole-Body MRI in Myeloma: Myeloma Response Assessment and Diagnosis System (MY-RADS). Radiology 2019, 291, 5–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Padhani, A.R.; Lecouvet, F.E.; Tunariu, N.; Koh, D.-M.; De Keyzer, F.; Collins, D.J.; Sala, E.; Schlemmer, H.P.; Petralia, G.; Vargas, H.A.; et al. METastasis Reporting and Data System for Prostate Cancer: Practical Guidelines for Acquisition, Interpretation, and Reporting of Whole-body Magnetic Resonance Imaging-based Evaluations of Multiorgan Involvement in Advanced Prostate Cancer. Eur. Urol. 2017, 71, 81–92. [Google Scholar] [CrossRef] [Green Version]
- Pricolo, P.; Ancona, E.; Summers, P.; Abreu-Gomez, J.; Alessi, S.; Jereczek-Fossa, B.A.; De Cobelli, O.; Nolè, F.; Renne, G.; Bellomi, M.; et al. Whole-body magnetic resonance imaging (WB-MRI) reporting with the METastasis Reporting and Data System for Prostate Cancer (MET-RADS-P): Inter-observer agreement between readers of different expertise levels. Cancer Imaging 2020, 20, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Hardouin, P.; Pansini, V.; Cortet, B. Bone marrow fat. Jt. Bone Spine 2014, 81, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Veldhuis-Vlug, A.G.; Rosen, C.J. Mechanisms of marrow adiposity and its implications for skeletal health. Metabolism 2017, 67, 106–114. [Google Scholar] [CrossRef] [Green Version]
- Dietrich, O.; Geith, T.; Baur-Melnyk, A.; Reiser, M.F. Diffusion imaging of the vertebral bone marrow. NMR Biomed. 2015, 30, e3333. [Google Scholar] [CrossRef]
- Karampinos, D.C.; Ruschke, S.; Dieckmeyer, M.; Diefenbach, M.; Franz, D.; Gersing, A.S.; Krug, R.; Baum, T. Quantitative MRI and spectroscopy of bone marrow. J. Magn. Reson. Imaging 2018, 47, 332–353. [Google Scholar] [CrossRef] [Green Version]
- Kazerooni, A.F.; Pozo, J.M.; McCloskey, E.V.; Rad, H.S.; Frangi, A.F. Diffusion MRI for Assessment of Bone Quality; A Review of Findings in Healthy Aging and Osteoporosis. J. Magn. Reson. Imaging 2020, 51, 975–992. [Google Scholar] [CrossRef] [Green Version]
- Ueda, Y.; Miyati, T.; Ohno, N.; Motono, Y.; Hara, M.; Shibamoto, Y.; Kasai, H.; Kawamitsu, H.; Matsubara, K. Apparent diffusion coefficient and fractional anisotropy in the vertebral bone marrow. J. Magn. Reson. Imaging 2010, 31, 632–635. [Google Scholar] [CrossRef]
- He, J.; Fang, H.; Na Li, X. Vertebral bone marrow diffusivity in normal adults with varying bone densities at 3T diffusion-weighted imaging. Acta Radiol. 2018, 159, 89–96. [Google Scholar] [CrossRef]
- Chen, L.; Sun, P.; Hao, Q.; Yin, W.; Xu, B.; Ma, C.; Stemmer, A.; Fu, C.; Wang, M.; Lu, J. Diffusion-weighted MRI in the evaluation of the thyroid nodule: Comparison between integrated-shimming EPI and conventional 3D-shimming EPI techniques. Oncotarget 2018, 9, 26209–26216. [Google Scholar] [CrossRef] [Green Version]
- Griffith, J.F.; Yeung, D.K.; Ma, H.T.; Leung, J.C.S.; Kwok, T.C.; Leung, P.C. Bone marrow fat content in the elderly: A reversal of sex difference seen in younger subjects. J. Magn. Reson. Imaging 2012, 36, 225–230. [Google Scholar] [CrossRef]
- Baum, T.; Rohrmeier, A.; Syväri, J.; Diefenbach, M.N.; Franz, D.; Dieckmeyer, M.; Scharr, A.; Hauner, H.; Ruschke, S.; Kirschke, J.S.; et al. Anatomical Variation of Age-Related Changes in Vertebral Bone Marrow Composition Using Chemical Shift Encoding-Based Water–Fat Magnetic Resonance Imaging. Front. Endocrinol. 2018, 9, 141. [Google Scholar] [CrossRef] [Green Version]
- He, J.; Fang, H.; Li, X. Vertebral bone marrow fat content in normal adults with varying bone densities at 3T magnetic resonance imaging. Acta Radiol. 2019, 60, 509–515. [Google Scholar] [CrossRef]
- Lavdas, I.; Rockall, A.G.; Castelli, F.; Sandhu, R.S.; Papadaki, A.; Honeyfield, L.; Waldman, A.D.; Aboagye, E.O. Apparent Diffusion Coefficient of Normal Abdominal Organs and Bone Marrow from Whole-Body DWI at 1.5 T: The Effect of Sex and Age. Am. J. Roentgenol. 2015, 205, 242–250. [Google Scholar] [CrossRef]
- Tsujikawa, T.; Oikawa, H.; Tasaki, T.; Hosono, N.; Tsuyoshi, H.; Yoshida, Y.; Yamauchi, T.; Kimura, H.; Okazawa, H. Whole-body bone marrow DWI correlates with age, anemia, and hematopoietic activity. Eur. J. Radiol. 2019, 118, 223–230. [Google Scholar] [CrossRef]
- Zhang, H.; Xue, H.; Alto, S.; Hui, L.; Kannengiesser, S.; Berthold, K.; Jin, Z. Integrated Shimming Improves Lesion Detection in Whole-Body Diffusion-Weighted Examinations of Patients with Plasma Disorder at 3 T. Investig. Radiol. 2016, 51, 297–305. [Google Scholar] [CrossRef] [Green Version]
- Blackledge, M.D.; Collins, D.J.; Tunariu, N.; Orton, M.R.; Padhani, A.R.; Leach, M.O.; Koh, D.-M. Assessment of Treatment Response by Total Tumor Volume and Global Apparent Diffusion Coefficient Using Diffusion-Weighted MRI in Patients with Metastatic Bone Disease: A Feasibility Study. PLoS ONE 2014, 9, e91779. [Google Scholar] [CrossRef]
- Blackledge, M.D.; Leach, M.O.; Collins, D.J.; Koh, D.-M. Computed Diffusion-weighted MR Imaging May Improve Tumor Detection. Radiology 2011, 261, 573–581. [Google Scholar] [CrossRef]
- Colombo, A.; Saia, G.; Azzena, A.; Rossi, A.; Zugni, F.; Pricolo, P.; Summers, P.; Marvaso, G.; Grimm, R.; Bellomi, M.; et al. Semi-Automated Segmentation of Bone Metastases from Whole-Body MRI: Reproducibility of Apparent Diffusion Coefficient Measurements. Diagnostics 2021, 11, 499. [Google Scholar] [CrossRef] [PubMed]
- Padhani, A.R.; Van Ree, K.; Collins, D.J.; D’Sa, S.; Makris, A. Assessing the Relation Between Bone Marrow Signal Intensity and Apparent Diffusion Coefficient in Diffusion-Weighted MRI. Am. J. Roentgenol. 2013, 200, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Wehrli, F.W. Structural and functional assessment of trabecular and cortical bone by micro magnetic resonance imaging. J. Magn. Reson. Imaging 2007, 25, 390–409. [Google Scholar] [CrossRef]
- Kugel, H.; Jung, C.; Schulte, O.; Heindel, W. Age- and sex-specific differences in the1H-spectrum of vertebral bone marrow. J. Magn. Reson. Imaging 2001, 13, 263–268. [Google Scholar] [CrossRef]
- Le Ster, C.; Lasbleiz, J.; Kannengiesser, S.; Guillin, R.; Gambarota, G.; Saint-Jalmes, H. A fast method for the quantification of fat fraction and relaxation times: Comparison of five sites of bone marrow. Magn. Reson. Imaging 2017, 39, 157–161. [Google Scholar] [CrossRef]
- Borga, M.; Ahlgren, A.; Romu, T.; Widholm, P.; Leinhard, O.D.; West, J. Reproducibility and repeatability of MRI-based body composition analysis. Magn. Reson. Med. 2020, 84, 3146–3156. [Google Scholar] [CrossRef]
- Limonard, E.J.; Veldhuis-Vlug, A.G.; Van Dussen, L.; Runge, J.H.; Tanck, M.W.; Endert, E.; Heijboer, A.C.; Fliers, E.; Hollak, C.E.; Akkerman, E.M.; et al. Short-Term Effect of Estrogen on Human Bone Marrow Fat. J. Bone Miner. Res. 2015, 30, 2058–2066. [Google Scholar] [CrossRef]
- Syed, F.A.; Oursler, M.J.; Hefferan, T.E.; Peterson, J.M.; Riggs, B.L.; Khosla, S. Effects of estrogen therapy on bone marrow adipocytes in postmenopausal osteoporotic women. Osteoporos. Int. 2008, 19, 1323–1330. [Google Scholar] [CrossRef] [Green Version]
- Liney, G.P.; Bernard, C.P.; Manton, D.J.; Turnbull, L.W.; Langton, C.M. Age, gender, and skeletal variation in bone marrow composition: A preliminary study at 3.0Tesla. J. Magn. Reson. Imaging 2007, 26, 787–793. [Google Scholar] [CrossRef]
- Nonomura, Y.; Yasumoto, M.; Yoshimura, R.; Haraguchi, K.; Ito, S.; Akashi, T.; Ohashi, I. Relationship between bone marrow cellularity and apparent diffusion coefficient. J. Magn. Reson. Imaging 2001, 13, 757–760. [Google Scholar] [CrossRef]
- Ruschke, S.; Syväri, J.; Dieckmeyer, M.; Junker, D.; Makowski, M.R.; Baum, T.; Karampinos, D.C. Physiological variation of the vertebral bone marrow water T2 relaxation time. NMR Biomed. 2021, 34, e4439. [Google Scholar] [CrossRef]
- Cui, F.-Z.; Cui, J.-L.; Wang, S.-L.; Yu, H.; Sun, Y.-C.; Zhao, N.; Cui, S.-J. Signal characteristics of normal adult bone marrow in whole-body diffusion-weighted imaging. Acta Radiol. 2016, 57, 1230–1237. [Google Scholar] [CrossRef]
- Ishijima, H.; Ishizaka, H.; Horikoshi, H.; Sakurai, M. Water fraction of lumbar vertebral bone marrow estimated from chemical shift misregistration on MR imaging: Normal variations with age and sex. Am. J. Roentgenol. 1996, 167, 355–358. [Google Scholar] [CrossRef]
- Chen, Y.-Y.; Wu, C.-L.; Shen, S.-H. High Signal in Bone Marrow on Diffusion-Weighted Imaging of Female Pelvis: Correlation With Anemia and Fibroid-Associated Symptoms. J. Magn. Reson. Imaging 2018, 48, 1024–1033. [Google Scholar] [CrossRef]
- De Santis, S.; Rebuzzi, M.; Di Pietro, G.; Fasano, F.; Maraviglia, B.; Capuani, S. In vitroandin vivoMR evaluation of internal gradient to assess trabecular bone density. Phys. Med. Biol. 2010, 55, 5767–5785. [Google Scholar] [CrossRef]
- Ismail, U.N.; Azlan, C.A.; Khairullah, S.; Azman, R.R.; Omar, N.F.; Shah, M.N.M.; Yeong, C.H.; Jackson, N.; Ng, K.H. Marrow Fat Content and Composition in β-Thalassemia: A Study using 1 H-MRS. J. Magn. Reson. Imaging 2021, 53, 190–198. [Google Scholar] [CrossRef]
- Jie, H.; Hao, F.; Na, L.X. Vertebral bone marrow diffusivity in healthy adults at 3T diffusion-weighted imaging. Acta Radiol. 2016, 57, 1238–1243. [Google Scholar] [CrossRef]
- Herrmann, J.; Krstin, N.; Schoennagel, B.P.; Sornsakrin, M.; Derlin, T.; Busch, J.D.; Petersen, K.U.; Graessner, J.; Adam, G.; Habermann, C.R. Age-related distribution of vertebral bone-marrow diffusivity. Eur. J. Radiol. 2012, 81, 4046–4049. [Google Scholar] [CrossRef] [PubMed]
- Messiou, C.; Collins, D.J.; Morgan, V.A.; DeSouza, N.M. Optimising diffusion weighted MRI for imaging metastatic and myeloma bone disease and assessing reproducibility. Eur. Radiol. 2011, 21, 1713–1718. [Google Scholar] [CrossRef]
- Zhang, C.-Y.; Rong, R.; Wang, X.-Y. Age-Related Changes of Bone Marrow of Normal Adult Man on Diffusion Weighted Imaging. Chin. Med. Sci. J. 2008, 23, 162–165. [Google Scholar] [CrossRef]
- Chen, W.-T.; Shih, T.T.-F.; Chen, R.-C.; Lo, S.-Y.; Chou, C.T.; Lee, J.-M.; Tu, H.-Y. Vertebral Bone Marrow Perfusion Evaluated with Dynamic Contrast-enhanced MR Imaging: Significance of Aging and Sex. Radiology 2001, 220, 213–218. [Google Scholar] [CrossRef] [PubMed]
- Bedatsova, L.; Drake, M.T. The skeletal impact of cancer therapies. Br. J. Clin. Pharmacol. 2019, 85, 1161–1168. [Google Scholar] [CrossRef]
- Dieckmeyer, M.; Ruschke, S.; Rohrmeier, A.; Syväri, J.; Einspieler, I.; Seifert-Klauss, V.; Schmidmayr, M.; Metz, S.; Kirschke, J.S.; Rummeny, E.J.; et al. Vertebral bone marrow fat fraction changes in postmenopausal women with breast cancer receiving combined aromatase inhibitor and bisphosphonate therapy. BMC Musculoskelet. Disord. 2019, 20, 515. [Google Scholar] [CrossRef]
- Lee, Y.; Kettinger, A.O.; Wilm, B.J.; Deichmann, R.; Weiskopf, N.; Lambert, C.; Pruessmann, K.P.; Nagy, Z. A comprehensive approach for correcting voxel-wise b-value errors in diffusion MRI. Magn. Reson. Med. 2020, 83, 2173–2184. [Google Scholar] [CrossRef]
- Hu, H.H.; Yokoo, T.; Bashir, M.R.; Sirlin, C.B.; Hernando, D.; Malyarenko, D.; Chenevert, T.L.; Smith, M.A.; Serai, S.D.; Middleton, M.S.; et al. Linearity and Bias of Proton Density Fat Fraction as a Quantitative Imaging Biomarker: A Multicenter, Multiplatform, Multivendor Phantom Study. Radiology 2021, 298, 640–651. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | DWI | T1W | T2W |
|---|---|---|---|
| Sequence type | SS-EPI | GRE Dixon | HASTE |
| FOV (mm) | 430 | 430 | 430 |
| Phase FOV (mm) | 390.9 | 364.0 | 335.9 |
| Matrix (phase × freq.) | 120 × 132 | 209 × 352 | 175 × 320 |
| Voxel (mm) | 1.6 × 1.6 × 5 | 1.2 × 1.2 × 3.5 | 1.3 × 1.3 × 5 |
| n of slices/station | 50 | 72 | 16 |
| n of stations | 4 | 4 | 12/13 |
| Slice thickness (mm) | 5 | 3.5 | 5 |
| Gap between slices (mm) | 0 | 0.7 | 1 |
| TR (ms) | 6550 | 6.65 | 800 |
| TE (ms) | 62 | 2.39/4.77 | 74 |
| TI (ms) | 180 | - | - |
| Flip angle (degrees) | 90 | 20.5 | 149 |
| n of averages | 5 (b50)/15 (b900) | 1 | 1 |
| Fat suppression | STIR | - | - |
| b-values (s/mm2) | 50, 900 | - | - |
| Breathing | Free | Hold | Hold |
| Acquisition time per station (min:s) | 3:46 | 0:16 | 0:16 |
| Image plane | Transversal | Transversal | Transversal |
| Population | Age Range (Years) | Men | Women | ||
|---|---|---|---|---|---|
| n | BMI (kg/m2) | n | BMI (kg/m2) | ||
| Overall | 30–81 | 50 | 25.6 (3.3) | 50 | 23.3 (3.3) |
| 10-years age groups | 30–39 | 10 | 26.7 (4.6) | 10 | 23.5 (3.8) |
| 40–49 | 10 | 24.9 (2.6) | 10 | 22.7 (3.0) | |
| 50–59 | 10 | 25.0 (2.7) | 10 | 24.7 (2.9) | |
| 60–69 | 10 | 25.5 (3.1) | 10 | 23.0 (3.6) | |
| ≥70 | 10 | 25.7 (3.3) | 10 | 22.7 (3.1) | |
| Parameter | Value Descriptors | Full Cohort (N = 100) | Men (N = 50) | Women (N = 50) | p-Value |
|---|---|---|---|---|---|
| %FF (%) | Mean (SD) | 65.6 (7.2) | 65.5 (7.7) | 65.7 (6.6) | 0.767 |
| ±2SD | 51.2–80.0 | 50.1–80.9 | 52.5–78.9 | ||
| nSIb50 (a.u.) | Mean (SD) | 1.7 (0.5) | 1.6 (0.4) | 1.8 (0.5) | 0.049 |
| 5th–95th percentile | 1.0–2.5 | 1.1–2.3 | 1.0–2.6 | ||
| nSIb900 (a.u.) | Mean (SD) | 3.2 (0.9) | 2.9 (0.7) | 3.5 (0.9) | <0.001 |
| 5th–95th percentile | 2.0–4.8 | 2.0–4.0 | 2.0–4.9 | ||
| ADC (µm2/s) | Mean (SD) | 422 (67) | 384 (46) | 460 (63) | <0.001 |
| 5th–95th percentile | 328–524 | 323–449 | 345–532 |
| Parameter | Value Descriptors | Full Cohort (N = 100) | Men (N = 50) | Women (N = 50) |
|---|---|---|---|---|
| %FF (%) | r | 0.63 | 0.63 | 0.64 |
| p-value | <0.001 | <0.001 | <0.001 | |
| nSIb50 (a.u.) | r | −0.3 | −0.01 | −0.54 |
| p-value | 0.003 | 0.949 | <0.001 | |
| nSIb900 (a.u.) | r | −0.27 | 0.01 | −0.57 |
| p-value | 0.006 | 0.955 | <0.001 | |
| ADC (µm2/s) | r | −0.23 | −0.17 | −0.38 |
| p-value | 0.02 | 0.250 | 0.007 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Colombo, A.; Bombelli, L.; Summers, P.E.; Saia, G.; Zugni, F.; Marvaso, G.; Grimm, R.; Jereczek-Fossa, B.A.; Padhani, A.R.; Petralia, G. Effects of Sex and Age on Fat Fraction, Diffusion-Weighted Image Signal Intensity and Apparent Diffusion Coefficient in the Bone Marrow of Asymptomatic Individuals: A Cross-Sectional Whole-Body MRI Study. Diagnostics 2021, 11, 913. https://doi.org/10.3390/diagnostics11050913
Colombo A, Bombelli L, Summers PE, Saia G, Zugni F, Marvaso G, Grimm R, Jereczek-Fossa BA, Padhani AR, Petralia G. Effects of Sex and Age on Fat Fraction, Diffusion-Weighted Image Signal Intensity and Apparent Diffusion Coefficient in the Bone Marrow of Asymptomatic Individuals: A Cross-Sectional Whole-Body MRI Study. Diagnostics. 2021; 11(5):913. https://doi.org/10.3390/diagnostics11050913
Chicago/Turabian StyleColombo, Alberto, Luca Bombelli, Paul E. Summers, Giulia Saia, Fabio Zugni, Giulia Marvaso, Robert Grimm, Barbara A. Jereczek-Fossa, Anwar R. Padhani, and Giuseppe Petralia. 2021. "Effects of Sex and Age on Fat Fraction, Diffusion-Weighted Image Signal Intensity and Apparent Diffusion Coefficient in the Bone Marrow of Asymptomatic Individuals: A Cross-Sectional Whole-Body MRI Study" Diagnostics 11, no. 5: 913. https://doi.org/10.3390/diagnostics11050913
APA StyleColombo, A., Bombelli, L., Summers, P. E., Saia, G., Zugni, F., Marvaso, G., Grimm, R., Jereczek-Fossa, B. A., Padhani, A. R., & Petralia, G. (2021). Effects of Sex and Age on Fat Fraction, Diffusion-Weighted Image Signal Intensity and Apparent Diffusion Coefficient in the Bone Marrow of Asymptomatic Individuals: A Cross-Sectional Whole-Body MRI Study. Diagnostics, 11(5), 913. https://doi.org/10.3390/diagnostics11050913