
Whole Body Low Dose Computed Tomography (WBLDCT) Can Be Comparable to Whole-Body Magnetic Resonance Imaging (WBMRI) in the Assessment of Multiple Myeloma

 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. WBLDCT Protocol
2.2. WBMRI Protocol
2.3. Image Analysis
2.4. Statistical Analysis
3. Results
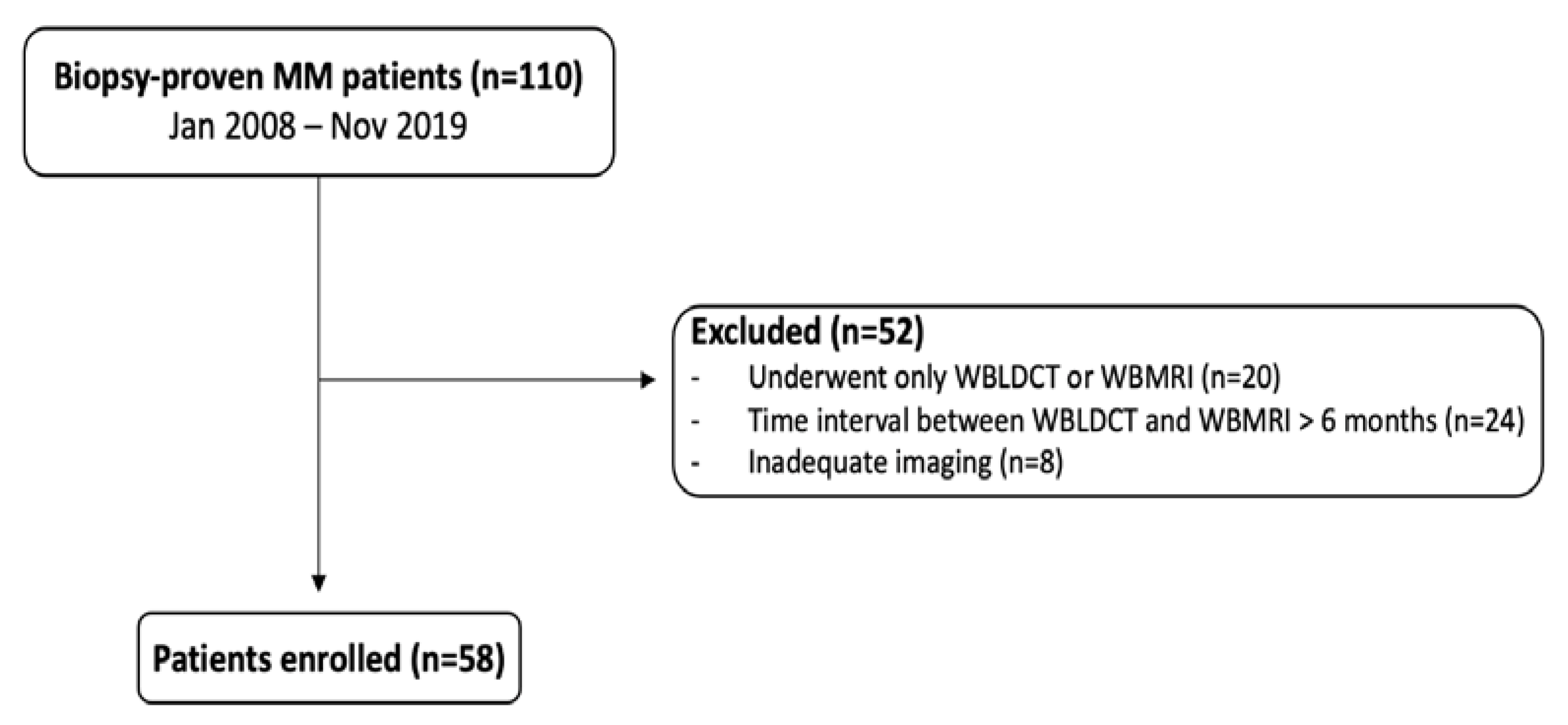
3.1. Patients Population
3.2. CT Findings
3.3. MRI Findings
3.4. Imaging Agreement
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Rajkumar, S.V.; A Dimopoulos, M.; Palumbo, A.; Blade, J.; Merlini, G.; Mateos, M.-V.; Kumar, S.; Hillengass, J.; Kastritis, E.; Richardson, P.; et al. International Myeloma Working Group updated criteria for the diagnosis of multiple myeloma. Lancet Oncol. 2014, 15, e538–e548. [Google Scholar] [CrossRef]
- Mai, E.K.; Hielscher, T.; Kloth, J.K.; Merz, M.; Shah, S.; Raab, M.S.; Hillengass, M.; Wagner, B.; Jauch, A.; Hose, D.; et al. A magnetic resonance imaging-based prognostic scoring system to predict outcome in transplant-eligible patients with multiple myeloma. Haematologica 2015, 100, 818–825. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rasche, L.; Angtuaco, E.J.; Alpe, T.L.; Gershner, G.H.; McDonald, J.E.; Samant, R.S.; Kumar, M.; Van Hemert, R.; Epstein, J.; Deshpande, S.; et al. The presence of large focal lesions is a strong independent prognostic factor in multiple myeloma. Blood 2018, 132, 59–66. [Google Scholar] [CrossRef]
- Nanni, C.; Rubello, D.; Fanti, S.; Farsad, M.; Ambrosini, V.; Rampin, L.; Banti, E.; Carpi, A.; Muzzio, P.; Franchi, R. Role of 18F-FDG-PET and PET/CT imaging in thyroid cancer. Biomed. Pharmacother. 2006, 60, 409–413. [Google Scholar] [CrossRef]
- Rajkumar, S.V. Myeloma today: Disease definitions and treatment advances. Am. J. Hematol. 2016, 91, 90–100. [Google Scholar] [CrossRef] [Green Version]
- Pratt, G.; Bowcock, S.J.; Chantry, A.; Cook, G.; Jackson, G.H.; Lai, M.; Low, E.; Mulholland, N.; Owen, R.G.; Rabin, N.; et al. Time to redefine Myeloma. Br. J. Haematol. 2015, 171, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Ormond Filho, A.G.; Carneiro, B.C.; Pastore, D.; Silva, I.P.; Yamashita, S.R.; Consolo, F.D.; Nico, M.A. Whole-body imaging of multiple myeloma: Diagnostic Criteria. RadioGraphics 2019, 39, 1077–1097. [Google Scholar] [CrossRef] [PubMed]
- Ippolito, D.; Besostri, V.; Bonaffini, P.A.; Rossini, F.; Di Lelio, A.; Sironi, S. Diagnostic value of whole-body low-dose computed tomography (WBLDCT) in bone lesions detection in patients with multiple myeloma (MM). Eur. J. Radiol. 2013, 82, 2322–2327. [Google Scholar] [CrossRef]
- Horger, M.; Claussen, C.D.; Bross-Bach, U.; Vonthein, R.; Trabold, T.; Heuschmid, M.; Pfannenberg, C. Whole-body low-dose multidetector row-CT in the diagnosis of multiple myeloma: An alternative to conventional radiography. Eur. J. Radiol. 2005, 54, 289–297. [Google Scholar] [CrossRef]
- Gleeson, T.G.; Moriarty, J.; Shortt, C.P.; Gleeson, J.P.; Fitzpatrick, P.; Byrne, B.; McHugh, J.; O’Connell, M.; O’Gorman, P.; Eustace, S.J. Accuracy of whole-body low-dose multidetector CT (WBLDCT) versus skeletal survey in the detection of myelomatous lesions, and correlation of disease distribution with whole-body MRI (WBMRI). Skelet. Radiol. 2008, 38, 225–236. [Google Scholar] [CrossRef]
- Lambert, L.; Ourednicek, P.; Meckova, Z.; Gavelli, G.; Straub, J.; Spicka, I. Whole-body low-dose computed tomography in multiple myeloma staging: Superior diagnostic performance in the detection of bone lesions, vertebral compression fractures, rib fractures and extraskeletal findings compared to radiography with similar radiation exposure. Oncol. Lett. 2017, 13, 2490–2494. [Google Scholar] [PubMed] [Green Version]
- Kröpil, P.; Fenk, R.; Fritz, L.B.; Blondin, D.; Kobbe, G.; Mödder, U.; Cohnen, M. Comparison of whole-body 64-slice multidetector computed tomography and conventional radiography in staging of multiple myeloma. Eur. Radiol. 2007, 18, 51–58. [Google Scholar] [CrossRef]
- Cretti, F.; Perugini, G. Patient dose evaluation for the whole-body low-dose multidetector CT (WBLDMDCT) skeleton study in multiple myeloma (MM). La Radiol. Med. 2015, 121, 93–105. [Google Scholar] [CrossRef]
- Hemke, R.; Yang, K.; Husseini, J.; Bredella, M.A.; Simeone, F.J. Organ dose and total effective dose of whole-body CT in multiple myeloma patients. Skelet. Radiol. 2019, 49, 549–554. [Google Scholar] [CrossRef] [Green Version]
- Rajkumar, S.V. Clinical Features, Laboratory Manifestations, and Diagnosis of Multiple Myeloma. UpToDate Website. Available online: http://www.uptodate.com (accessed on 19 February 2018).
- Giles, S.L.; Messiou, C.; Collins, D.J.; Morgan, V.A.; Simpkin, C.J.; West, S.; Davies, F.E.; Morgan, G.J.; DeSouza, N.M. Whole-Body Diffusion-weighted MR Imaging for Assessment of Treatment Response in Myeloma. Radiology 2014, 271, 785–794. [Google Scholar] [CrossRef] [Green Version]
- Bray, T.J.P.; Singh, S.; Latifoltojar, A.; Rajesparan, K.; Rahman, F.; Narayanan, P.; Naaseri, S.; Lopes, A.; Bainbridge, A.; Punwani, S.; et al. Diagnostic utility of whole body Dixon MRI in multiple myeloma: A multi-reader study. PLoS ONE 2017, 12, e0180562. [Google Scholar] [CrossRef] [Green Version]
- Koutoulidis, V.; Papanikolaou, N.; A Moulopoulos, L. Functional and molecular MRI of the bone marrow in multiple myeloma. Br. J. Radiol. 2018, 91, 20170389. [Google Scholar] [CrossRef] [PubMed]
- E Lecouvet, F.; Berg, B.C.V.; E Maldague, B.; Michaux, J.L.; Laterre, E.; Ferrant, A.; Malghem, J. Vertebral compression fractures in multiple myeloma. Part I. Distribution and appearance at MR imaging. Radiology 1997, 204, 195–199. [Google Scholar] [CrossRef]
- Myeloma Diagnosis and Management. NICE (NG35) and Appendices. Available online: https://www.nice.org.uk/guidance/ng35 (accessed on 20 March 2017).
- Petralia, G.; On behalf of the Italian Working Group on Magnetic Resonance; Padhani, A.R.; Pricolo, P.; Zugni, F.; Martinetti, M.; Summers, P.E.; Grazioli, L.; Colagrande, S.; Giovagnoni, A.; et al. Whole-body magnetic resonance imaging (WB-MRI) in oncology: Recommendations and key uses. La Radiol. Med. 2019, 124, 218–233. [Google Scholar] [CrossRef] [PubMed]
- Moulopoulos, L.A.; Koutoulidis, V.; Hillengass, J.; Zamagni, E.; Aquerreta, J.D.; Roche, C.L.; Lentzsch, S.; Moreau, P.; Cavo, M.; Miguel, J.S.; et al. Recommendations for acquisition, interpretation and reporting of whole body low dose CT in patients with multiple myeloma and other plasma cell disorders: A report of the IMWG Bone Working Group. Blood Cancer J. 2018, 8, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Kosmala, A.; Weng, A.M.; Heidemeier, A.; Krauss, B.; Knop, S.; Bley, T.A.; Petritsch, B. Multiple myeloma and dual-energy CT: Diagnostic accuracy of virtual non calcium technique for detection of bone marrow infiltration of the spine and pelvis. Radiology 2018, 286, 205–213. [Google Scholar] [CrossRef]
- Princewill, K.; Kyere, S.; Awan, O.; Mulligan, M. Multiple Myeloma Lesion Detection With Whole Body CT Versus Radiographic Skeletal Survey. Cancer Investig. 2013, 31, 206–211. [Google Scholar] [CrossRef]
- Wolf, M.B.; Murray, F.; Kilk, K.; Hillengass, J.; Delorme, S.; Heiss, C.; Neben, K.; Goldschmidt, H.; Kauczor, H.-U.; Weber, M.-A. Sensitivity of whole-body CT and MRI versus projection radiography in the detection of osteolyses in patients with monoclonal plasma cell disease. Eur. J. Radiol. 2014, 83, 1222–1230. [Google Scholar] [CrossRef] [PubMed]
- Baldi, D.; Tramontano, L.; Alfano, V.; Punzo, B.; Cavaliere, C.; Salvatore, M. Whole Body Low Dose Computed Tomography Using Third-Generation Dual-Source Multidetector With Spectral Shaping: Protocol Optimization and Literature Review. Dose-Response 2020, 18. [Google Scholar] [CrossRef]
- Koutoulidis, V.; Terpos, E.; Klapa, I.; Cheliotis, G.; Ntanasis-Stathopoulos, I.; Boultadaki, A.; Moulopoulos, L.A. Whole-Body Low-Dose CT in Multiple Myeloma: Diagnostic Value of Appendicular Medullary Patterns of Attenuation. Am. J. Roentgenol. 2021, 216, 742–751. [Google Scholar] [CrossRef]
- Terpos, E.; Kleber, M.; Engelhardt, M.; Zweegman, S.; Gay, F.; Kastritis, E.; Van De Donk, N.W.; Bruno, B.; Sezer, O.; Broijl, A.; et al. European Myeloma Network Guidelines for the Management of Multiple Myeloma-related Complications. Haematologica 2015, 100, 1254–1266. [Google Scholar] [CrossRef] [Green Version]
- Moreau, P.; Miguel, J.S.; Sonneveld, P.; Mateos, M.V.; Zamagni, E.; Avet-Loiseau, H.; Hajek, R.; Dimopoulos, M.A.; Ludwig, H.; Einsele, H.; et al. Multiple myeloma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2017, 28, iv52–iv61. [Google Scholar] [CrossRef] [PubMed]
- Terpos, E.; Morgan, G.; Dimopoulos, M.A.; Drake, M.T.; Lentzsch, S.; Raje, N.; Sezer, O.; García-Sanz, R.; Shimizu, K.; Turesson, I.; et al. International Myeloma Working Group Recommendations for the Treatment of Multiple Myeloma–Related Bone Disease. J. Clin. Oncol. 2013, 31, 2347–2357. [Google Scholar] [CrossRef] [Green Version]
- Pianko, M.J.; Terpos, E.; Roodman, G.D.; Divgi, C.R.; Zweegman, S.; Hillengass, J.; Lentzsch, S. Whole-Body Low-Dose Computed Tomography and Advanced Imaging Techniques for Multiple Myeloma Bone Disease. Clin. Cancer Res. 2014, 20, 5888–5897. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amos, B.; Agarwal, A.; Kanekar, S. Imaging of Multiple Myeloma. Hematol. Clin. N. Am. 2016, 30, 843–865. [Google Scholar] [CrossRef]
- Chrzan, R.; Jurczyszyn, A.; Urbanik, A. Whole-Body Low-Dose Computed Tomography (WBLDCT) in Assessment of Patients with Multiple Myeloma–Pilot Study and Standard Imaging Protocol Suggestion. Pol. J. Radiol. 2017, 82, 356–363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hillengas, J.; Landgren, O. Challenges and opportunities of novel imaging techniques in monoclonal plasma cell disorders: Imaging “early myeloma”. Leuk Lymphoma 2013, 54, 1355–1636. [Google Scholar] [CrossRef] [PubMed]
- Chantry, A.; Kazmi, M.; Barrington, S.; Goh, V.; Mulholland, N.; Streetly, M.; Lai, M.; Pratt, G.; Guidelines, T.B.S.F.H. Guidelines for the use of imaging in the management of patients with myeloma. Br. J. Haematol. 2017, 178, 380–393. [Google Scholar] [CrossRef] [PubMed]
- Cascini, G.L.; Falcone, C.; Console, D.; Restuccia, A.; Rossi, M.; Parlati, A.; Tamburrini, O. Whole-body MRI and PET/CT in multiple myeloma patients during staging and after treatment: Personal experience in a longitudinal study. La Radiol. Med. 2013, 118, 930–948. [Google Scholar] [CrossRef]
- Shortt, C.P.; Gleeson, T.G.; Breen, K.A.; McHugh, J.; O’Connell, M.J.; O’Gorman, P.J.; Eustace, S.J. Whole-body MRI versus PET in assessment of multiple myeloma disease activity. AJR Am. J. Roentgenol. 2009, 192, 980–986. [Google Scholar] [CrossRef]
- Pawlyn, C.; Fowkes, L.; Otero, S.; Jones, J.R.; Boyd, K.D.; E Davies, F.; Morgan, G.J.; Collins, D.J.; Sharma, B.; Riddell, A.; et al. Whole-body diffusion-weighted MRI: A new gold standard for assessing disease burden in patients with multiple myeloma? Leukemia 2016, 30, 1446–1448. [Google Scholar] [CrossRef] [Green Version]
- Zamagni, E.; Nanni, C.; Patriarca, F.; Englaro, E.; Castellucci, P.; Geatti, O.; Tosi, P.; Tacchetti, P.; Cangini, D.; Perrone, G.; et al. A prospective comparison of 18F-fluorodeoxyglucose positron emission tomography-computed tomography, magnetic resonance imaging and whole-body planar radiographs in the assessment of bone disease in newly diagnosed multiple myeloma. Haematologica 2007, 92, 50–55. [Google Scholar] [CrossRef]
- Hillengass, J.; Usmani, S.; Rajkumar, S.V.; Durie, B.G.M.; Mateos, M.-V.; Lonial, S.; Joao, C.; Anderson, K.C.; García-Sanz, R.; Riva, E.; et al. International myeloma working group consensus recommendations on imaging in monoclonal plasma cell disorders. Lancet Oncol. 2019, 20, e302–e312. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| WBLDCT Parameter | Measurement |
|---|---|
| Scanner | 256-slice scanner |
| Scan coverage | Cranial vault to the distal tibial metaphysis |
| Tube voltage (kV) | 120 |
| Tube current-time product (mAs) | 40 |
| Collimation (mm) | 128 × 0.65 |
| Pitch | 1 |
| Thickness/Increment of axial slices (mm) | 2/1 |
| Gantry rotation time (ms) | 270 |
| Acquisition time (s) | 10–15 |
| Sequence | Plane | Coverage | TE (ms) | TR (ms) | DFOV (mm) | Voxel Size (mm) | Section Thickness (mm) | SNR |
|---|---|---|---|---|---|---|---|---|
| T1-TSE | Coronal | Vertex to feet | 15 | 922 | 365 | 1.16 × 1.46 | 6 | 1.00 |
| T2-STIR-TSE | Coronal | Vertex to feet | 60 | 8704 | 365 | 1.25 × 1.82 | 6 | 1.00 |
| T1-TSE | Sagittal | Whole spine | 7.4 | 408 | 270 | 0.90 × 1.15 | 3.5 | 1.00 |
| T2-STIR-TSE | Sagittal | Whole spine | 60 | 2533 | 270 | 0.90 × 1.25 | 3.5 | 1.00 |
| DWIBS * | Axial | Vertex to feet | 66 | 6421 | 520 | 5.00 × 4.98 | 6 | 1.00 |
| District (n, %) | Number of Detectable Lesions | |||||
|---|---|---|---|---|---|---|
| CT | MRI | |||||
| <5 | 5–20 | >20 | <5 | 5–20 | >20 | |
| Skull | 13 (22.4) | 4 (6.9) | 1 (1.7) | 4 (6.9) | 1 (1.7) | 0 (0) |
| Sternum and ribs | 5 (8.6) | 6 (10.3) | 0 (0) | 11 (19) | 3 (5.2) | 0 (0) |
| Pelvis | 14 (24.1) | 6 (10.3) | 0 (0) | 13 (22.4) | 4 (6.9) | 0 (0) |
| Spine | 13 (22.4) | 13 (22.4) | 3 (5.2) | 14 (24.1) | 15 (25.9) | 2 (3.4) |
| U/L limbs | 3 (5.2) | 10 (17.2) | 0 (0) | 12 (20.7) | 3 (5.2) | 0 (0) |
| Pattern (n, %) | CT | MRI | Agreement (κ; 95% CI) | p-Value |
|---|---|---|---|---|
| No detectable lesions | 23 (39.7) | 11 (19.0) | 0.459 (0.351–0.699) | <0.0001 |
| Focal involvement | 35 (60.3) | 36 (62.0) | 0.875 (0.783–0.951) | <0.0001 |
| Diffuse | - | 11 (19.0) | ||
| Combined | - | 13 (22.4) | ||
| Durie Salmon Stage (n, %) | ||||
| IA | 9 (15.5) | 11 (19) | 0.759 (0.473.0.949) | <0.0001 |
| IB | 29 (50) | 30 (51.7) | 0.552 (0.345–0.724) | <0.0001 |
| II | 11 (19) | 12 (20.7) | 0.512 (0.186–0.776) | 0.001 |
| III | 9 (15.5) | 5 (8.6) | 0.772 (0.473–1.000) | <0.0001 |
| District | Agreement (κ; 95%CI) | |||
|---|---|---|---|---|
| Overall | <5 Lesions | 5–20 Lesions | >20 Lesions | |
| Skull | 0.283 (0.056–0.510) * | 0.145 (0.010–0.415) ° | 0.028 (−0.069–0.100) ° | § |
| Sternum and ribs | 0.644 (0.405–0.883) * | 0.433 (0.103–0.789) * | 0.642 (0.180–0.990) * | § |
| Pelvis | 0.486 (0.247–0.725) ^ | 0.373 (0.092–0.665) ^ | 0.564 (0.024–0.844) * | § |
| Spine | 0.586 (0.379–0.793) ^ | 0.469 (0.196–0.707) * | 0.624 (0.372–0.834) * | 0.791 (0.122–0.993) * |
| U/L limbs | 0.820 (0.619–0.961) * | 0.776 (0.518–0.949) * | 0.733 (0.710–0.783) * | § |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ippolito, D.; Giandola, T.; Maino, C.; Gandola, D.; Ragusi, M.; Bonaffini, P.A.; Sironi, S. Whole Body Low Dose Computed Tomography (WBLDCT) Can Be Comparable to Whole-Body Magnetic Resonance Imaging (WBMRI) in the Assessment of Multiple Myeloma. Diagnostics 2021, 11, 857. https://doi.org/10.3390/diagnostics11050857
Ippolito D, Giandola T, Maino C, Gandola D, Ragusi M, Bonaffini PA, Sironi S. Whole Body Low Dose Computed Tomography (WBLDCT) Can Be Comparable to Whole-Body Magnetic Resonance Imaging (WBMRI) in the Assessment of Multiple Myeloma. Diagnostics. 2021; 11(5):857. https://doi.org/10.3390/diagnostics11050857
Chicago/Turabian StyleIppolito, Davide, Teresa Giandola, Cesare Maino, Davide Gandola, Maria Ragusi, Pietro Andrea Bonaffini, and Sandro Sironi. 2021. "Whole Body Low Dose Computed Tomography (WBLDCT) Can Be Comparable to Whole-Body Magnetic Resonance Imaging (WBMRI) in the Assessment of Multiple Myeloma" Diagnostics 11, no. 5: 857. https://doi.org/10.3390/diagnostics11050857
APA StyleIppolito, D., Giandola, T., Maino, C., Gandola, D., Ragusi, M., Bonaffini, P. A., & Sironi, S. (2021). Whole Body Low Dose Computed Tomography (WBLDCT) Can Be Comparable to Whole-Body Magnetic Resonance Imaging (WBMRI) in the Assessment of Multiple Myeloma. Diagnostics, 11(5), 857. https://doi.org/10.3390/diagnostics11050857