
Red Cell Distribution Width as a Prognostic Factor and Its Comparison with Lactate in Patients with Sepsis


Abstract
:1. Introduction
2. Materials and Methods
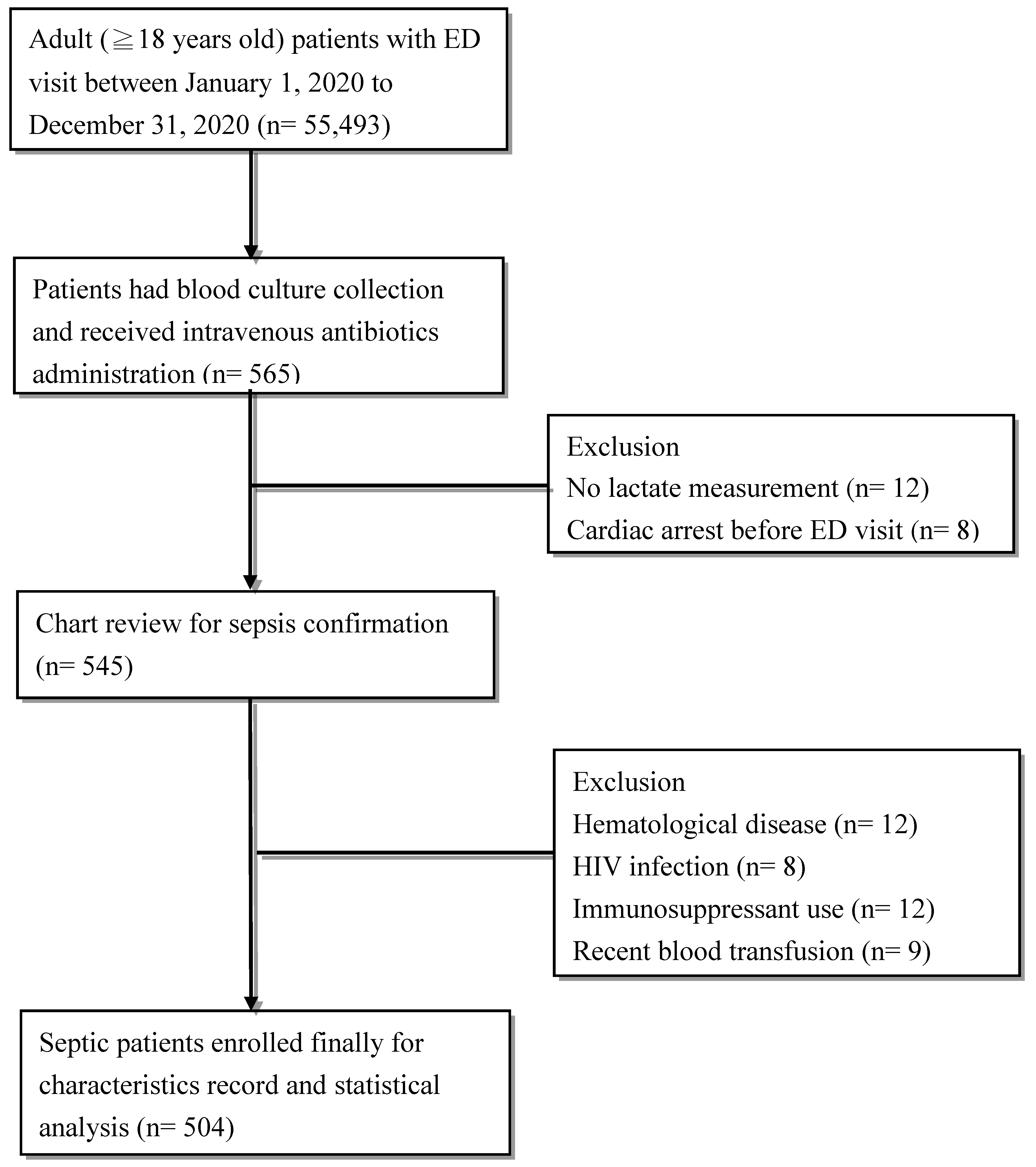
2.1. Study Design
2.2. Data Collection
2.3. Definitions
2.4. Outcomes Measurement
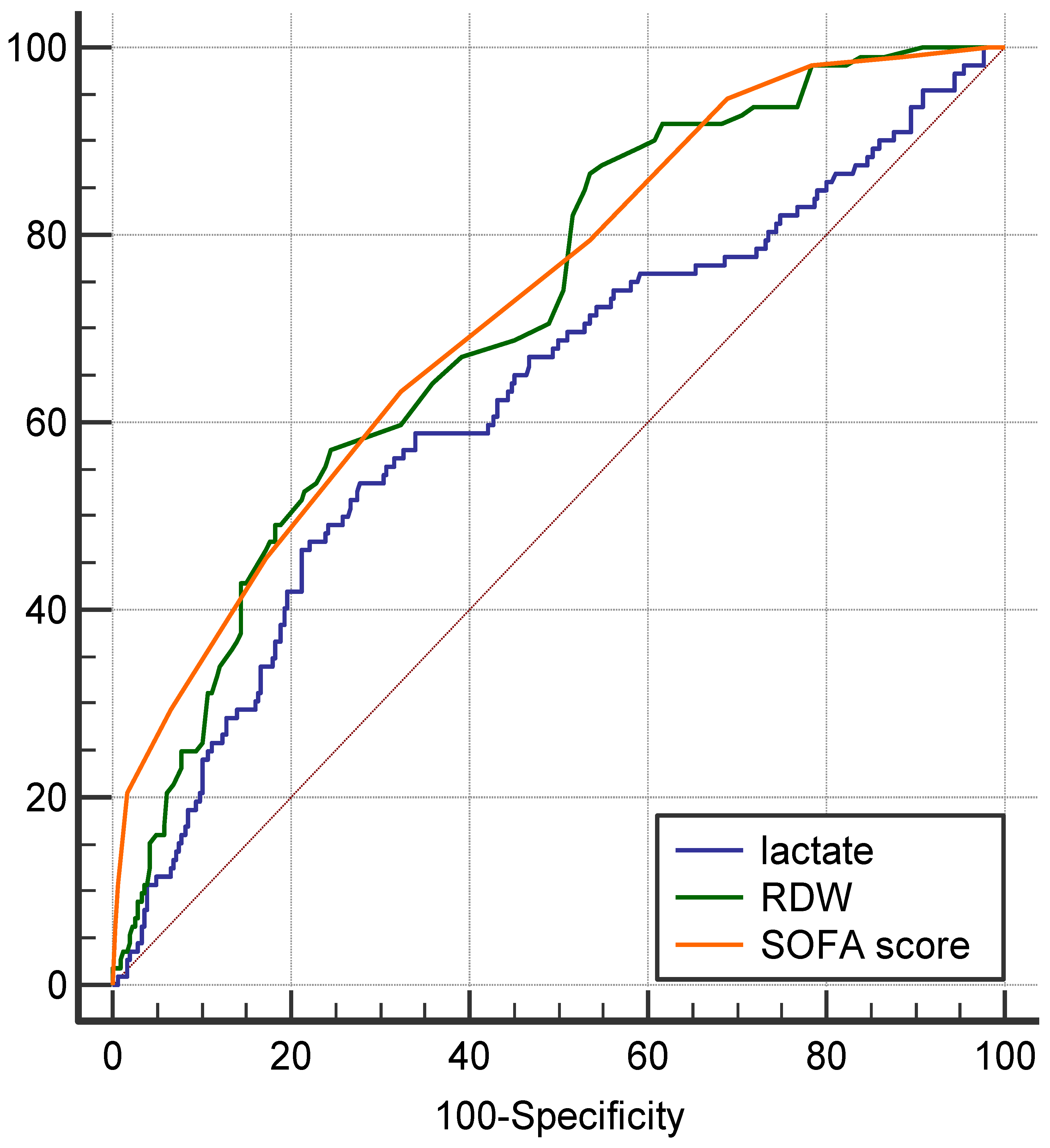
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Outcomes Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Levy, M.M.; Evans, L.E.; Rhodes, A. The surviving sepsis campaign bundle: 2018 update. Intensive Care Med. 2018, 44, 925–928. [Google Scholar] [CrossRef] [Green Version]
- Shapiro, N.I.; Fisher, C.; Donnino, M.; Cataldo, L.; Tang, A.; Trzeciak, S.; Horowitz, G.; Wolfe, R.E. The feasibility and accuracy of point-of-care lactate measurement in emergency department patients with suspected infection. J. Emerg. Med. 2010, 39, 89–94. [Google Scholar] [CrossRef] [Green Version]
- Florkowski, C.; Don-Wauchope, A.; Gimenez, N.; Rodriguez-Capote, K.; Wils, J.; Zemlin, A. Point-of-care testing (POCT) and evidence-based laboratory medicine (EBLM)–Does it leverage any advantage in clinical decision making? Crit. Rev. Clin. Lab. Sci. 2017, 54, 471–494. [Google Scholar] [CrossRef]
- Jo, Y.H.; Kim, K.; Lee, J.H.; Kang, C.; Kim, T.; Park, H.-M.; Kang, K.W.; Kim, J.; Rhee, J.E. Red cell distribution width is a prognostic factor in severe sepsis and septic shock. Am. J. Emerg. Med. 2013, 31, 545–548. [Google Scholar] [CrossRef] [PubMed]
- Wang, A.-Y.; Ma, H.-P.; Kao, W.-F.; Tsai, S.-H.; Chang, C.-K. Red blood cell distribution width is associated with mortality in elderly patients with sepsis. Am. J. Emerg. Med. 2018, 36, 949–953. [Google Scholar] [CrossRef]
- Jandial, A.; Kumar, S.; Bhalla, A.; Sharma, N.; Varma, N.; Varma, S. Elevated red cell distribution width as a prognostic marker in severe sepsis: A prospective observational study. Indian J. Crit. Care Med. 2017, 21, 552. [Google Scholar] [CrossRef]
- Bazick, H.S.; Chang, D.; Mahadevappa, K.; Gibbons, F.K.; Christopher, K.B. Red Cell Distribution Width and all cause mortality in critically ill patients. Crit. Care Med. 2011, 39, 1913. [Google Scholar] [CrossRef] [Green Version]
- Hu, Z.-D.; Lippi, G.; Montagnana, M. Diagnostic and prognostic value of red blood cell distribution width in sepsis: A narrative review. Clin. Biochem. 2020, 77, 1–6. [Google Scholar] [CrossRef]
- Zhang, L.; Yu, C.-H.; Guo, K.-P.; Huang, C.-Z.; Mo, L.-Y. Prognostic role of red blood cell distribution width in patients with sepsis: A systematic review and meta-analysis. BMC Immunol. 2020, 21, 1–8. [Google Scholar] [CrossRef]
- Li, Y.; She, Y.; Fu, L.; Zhou, R.; Xiang, W.; Luo, L. Association Between Red Cell Distribution Width and Hospital Mortality in Patients with Sepsis. J. Int. Med Res. 2021, 49, 03000605211004221. [Google Scholar] [CrossRef]
- Sukewanti, N.M.; Hartawan, I.N.B.; Wati, D.K.; Suparyatha, I.B.G.; Ryalino, C. Correlation of red cell distribution width and serum lactate levels in critically ill pediatric patients. Bali J. Anesthesiol. 2020, 4, 104. [Google Scholar] [CrossRef]
- Vandenbroucke, J.P.; Von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M.; Initiative, S. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. PLoS Med. 2007, 4, e297. [Google Scholar] [CrossRef] [Green Version]
- Bone, R.C.; Balk, R.A.; Cerra, F.B.; Dellinger, R.P.; Fein, A.M.; Knaus, W.A.; Schein, R.M.; Sibbald, W.J. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Chest 1992, 101, 1644–1655. [Google Scholar] [CrossRef] [Green Version]
- Vincent, J.-L.; Moreno, R.; Takala, J.; Willatts, S.; De Mendonça, A.; Bruining, H.; Reinhart, C.; Suter, P.; Thijs, L.G. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. Intensive Care Med. 1996, 22, 707–710. [Google Scholar] [CrossRef]
- Duchnowski, P.; Szymański, P.; Kuśmierczyk, M.; Hryniewiecki, T. Usefulness of FRAIL scale in heart valve diseases. Clin. Interv. Aging 2020, 15, 1071. [Google Scholar] [CrossRef]
- Levey, A.S.; Coresh, J.; Bolton, K.; Culleton, B.; Harvey, K.S.; Ikizler, T.A.; Johnson, C.A.; Kausz, A.; Kimmel, P.L.; Kusek, J. K/DOQI clinical practice guidelines for chronic kidney disease: Evaluation, classification, and stratification. Am. J. Kidney Dis. 2002, 39 (Suppl. 1), i–ii + S1–S266. [Google Scholar]
- Mehta, R.L.; Kellum, J.A.; Shah, S.V.; Molitoris, B.A.; Ronco, C.; Warnock, D.G.; Levin, A. Acute Kidney Injury Network: Report of an initiative to improve outcomes in acute kidney injury. Crit. Care 2007, 11, 1–8. [Google Scholar] [CrossRef] [Green Version]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the areas under two or more correlated receiver operating characteristic curves: A nonparametric approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef]
- Pierce, C.N.; Larson, D.F. Inflammatory cytokine inhibition of erythropoiesis in patients implanted with a mechanical circulatory assist device. Perfusion 2005, 20, 83–90. [Google Scholar] [CrossRef]
- Scharte, M.; Fink, M.P. Red blood cell physiology in critical illness. Crit. Care Med. 2003, 31, S651–S657. [Google Scholar] [CrossRef]
- Subramani, K.; Raju, S.P.; Chu, X.; Warren, M.; Pandya, C.D.; Hoda, N.; Fulzele, S.; Raju, R. Effect of plasma-derived extracellular vesicles on erythrocyte deformability in polymicrobial sepsis. Int. Immunopharmacol. 2018, 65, 244–247. [Google Scholar] [CrossRef]
- Lippi, G.; Targher, G.; Montagnana, M.; Salvagno, G.L.; Zoppini, G.; Guidi, G.C. Relation between red blood cell distribution width and inflammatory biomarkers in a large cohort of unselected outpatients. Arch. Pathol. Lab. Med. 2009, 133, 628–632. [Google Scholar] [CrossRef]
- Evans, T.C.; Jehle, D. The red blood cell distribution width. J. Emerg. Med. 1991, 9, 71–74. [Google Scholar] [CrossRef]
- Duchnowski, P.; Hryniewiecki, T.; Kuśmierczyk, M.; Szymanski, P. Red cell distribution width as a predictor of multiple organ dysfunction syndrome in patients undergoing heart valve surgery. Biol. Open 2018, 7, bio036251. [Google Scholar] [CrossRef] [Green Version]
- Chou, E.H.; Mann, S.; Hsu, T.-C.; Hsu, W.-T.; Liu, C.C.-Y.; Bhakta, T.; Hassani, D.M.; Lee, C.-C. Incidence, trends, and outcomes of infection sites among hospitalizations of sepsis: A nationwide study. PLoS ONE 2020, 15, e0227752. [Google Scholar] [CrossRef] [Green Version]
- Zador, Z.; Landry, A.; Cusimano, M.D.; Geifman, N. Multimorbidity states associated with higher mortality rates in organ dysfunction and sepsis: A data-driven analysis in critical care. Crit. Care 2019, 23, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mansur, A.; Mulwande, E.; Steinau, M.; Bergmann, I.; Popov, A.F.; Ghadimi, M.; Beissbarth, T.; Bauer, M.; Hinz, J. Chronic kidney disease is associated with a higher 90-day mortality than other chronic medical conditions in patients with sepsis. Sci. Rep. 2015, 5, 10539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sadaka, F.; O’Brien, J.; Prakash, S. Red cell distribution width and outcome in patients with septic shock. J. Intensive Care Med. 2013, 28, 307–313. [Google Scholar] [CrossRef] [PubMed]
- Rowe, T.A.; McKoy, J.M. Sepsis in older adults. Infect. Dis. Clin. 2017, 31, 731–742. [Google Scholar] [CrossRef]
- Suetrong, B.; Walley, K.R. Lactic acidosis in sepsis: It’s not all anaerobic: Implications for diagnosis and management. Chest 2016, 149, 252–261. [Google Scholar] [CrossRef] [PubMed]
- Duchnowski, P.; Hryniewiecki, T.; Kuśmierczyk, M.; Szymański, P. The usefulness of perioperative lactate blood levels in patients undergoing heart valve surgery. Kardiochir. Torakochir. Pol. Pol. J. Cardio-Thorac. Surg. 2019, 16, 114. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | All (n = 504) | Normal RDW ≤14.5% (n = 213) | High RDW >14.5% (n = 291) | p Value |
|---|---|---|---|---|
| Age, y, mean ± SD | 68.1 ± 15.8 | 68.3 ± 14.7 | 68.0 ± 16.6 | 0.86 |
| Male, n (%) | 312 (61.9) | 135 (63.4) | 177 (60.8) | 0.56 |
| SIRS, n (%) | 364 (72.2) | 147 (69.0) | 217 (74.6) | 0.19 |
| qSOFA score, n (%) | 0.11 | |||
| 0 | 78 (15.5) | 38 (17.8) | 40 (13.7) | |
| 1 | 164 (32.5) | 75 (35.2) | 89 (30.6) | |
| 2 | 157 (31.2) | 61 (28.6) | 96 (33.0) | |
| 3 | 105 (20.8) | 39 (18.3) | 66 (22.7) | |
| SOFA score, mean ± SD | 8 ± 2 | 7 ± 2 | 9 ± 2 | <0.01 * |
| Frailty syndrome, n (%) | 62 (12.3) | 27 (12.7) | 35 (12.0) | 0.84 |
| Source of sepsis, n (%) | ||||
| Respiratory tract infection | 243 (48.2) | 109 (51.2) | 134 (46.0) | 0.26 |
| Urinary tract infection | 80 (15.9) | 32 (15.0) | 48 (16.5) | 0.66 |
| Intra-abdominal infection | 102 (20.2) | 46 (21.6) | 56 (19.2) | 0.52 |
| Soft tissue infection | 33 (6.5) | 9 (4.2) | 24 (8.2) | 0.10 |
| Other | 46 (9.1) | 17 (8.0) | 29 (10.0) | 0.53 |
| Comorbidities, n (%) | ||||
| Diabetes Mellitus | 239 (47.4) | 94 (44.1) | 145 (49.8) | 0.21 |
| Hypertension | 284 (56.3) | 128 (60.1) | 156 (53.6) | 0.15 |
| Coronary artery disease | 101 (20.0) | 48 (22.5) | 53 (18.2) | 0.23 |
| Chronic kidney disease | 295 (58.5) | 123 (57.7) | 172 (59.1) | 0.76 |
| Cerebrovascular accident | 56 (11.1) | 30 (14.2) | 26 (8.9) | 0.09 |
| Dyslipidemia | 60 (11.9) | 25 (11.7) | 35 (12.0) | 1.00 |
| Laboratory results | ||||
| Hemoglobin, g/dL, mean ± SD | 11.1 ± 2.6 | 12.4 ± 2.3 | 10.3 ± 2.6 | <0.01 * |
| Leukocyte, × 109/L, median (IQR) | 12.7 (7.5–17.8) | 12.2 (7.1–16.9) | 13.1 (8.1–18.8) | 0.18 |
| Creatinine, mg/dL, median (IQR) | 1.8 (1.2–2.8) | 1.7 (1.2–2.6) | 1.9 (1.2–3.0) | 0.14 |
| CRP, mg/dL, median (IQR) | 107.8 (43.7–197.8) | 105.6 (44.2–195.2) | 111.9 (37.9–203.8) | 0.69 |
| Lactate, mmol/L, median (IQR) | 2.3 (1.5–4.2) | 2.2 (1.5–4.0) | 2.4 (1.4–4.5) | 0.57 |
| Variables, n (%) | All (n = 504) | Normal RDW ≤14.5% (n = 213) | High RDW >14.5% (n = 291) | p Value |
|---|---|---|---|---|
| Intensive care unit admission | 211 (41.9) | 69 (32.4) | 142 (48.8) | 0.03 * |
| Endotracheal intubation | 180 (35.7) | 65 (30.5) | 115 (39.5) | 0.19 |
| Septic shock | 164 (32.5) | 50 (23.5) | 114 (39.2) | <0.01 * |
| Acute kidney injury | 175 (34.7) | 69 (32.4) | 106 (36.4) | 0.48 |
| 30-day in-hospital mortality | 137 (27.2) | 44 (20.7) | 93 (32.0) | <0.01 * |
| Variables | Univariate | Multivariate | ||
|---|---|---|---|---|
| HR (95%CI) | p Value | HR (95%CI) | p Value | |
| Age (year) | 1.01 (0.99–1.02) | 0.11 | 1.01 (0.99–1.03) | 0.17 |
| Sex (male) | 1.43 (0.94–2.16) | 0.09 | 1.76 (0.96–3.23) | 0.07 |
| Chronic kidney disease | 1.81 (1.19–2.74) | <0.01 * | ||
| Respiratory tract infection | 1.55 (1.05–2.31) | 0.03 * | 1.21 (0.74–1.90) | 0.98 |
| Urinary tract infection | 0.52 (0.28–0.96) | 0.04 * | 0.64 (0.24–1.34) | 0.39 |
| SOFA score | 3.17 (2.55–3.95) | <0.01 * | 3.21 (2.55–4.03) | <0.01 * |
| RDW (%) | 1.16 (1.08–1.25) | <0.01 * | 1.05 (1.02–1.08) | <0.01 * |
| lactate | 1.08 (1.03–1.14) | <0.01 * | 1.06 (1.02–1.11) | <0.01 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, T.-H.; Hsu, Y.-C. Red Cell Distribution Width as a Prognostic Factor and Its Comparison with Lactate in Patients with Sepsis. Diagnostics 2021, 11, 1474. https://doi.org/10.3390/diagnostics11081474
Wang T-H, Hsu Y-C. Red Cell Distribution Width as a Prognostic Factor and Its Comparison with Lactate in Patients with Sepsis. Diagnostics. 2021; 11(8):1474. https://doi.org/10.3390/diagnostics11081474
Chicago/Turabian StyleWang, Tsung-Han, and Yin-Chou Hsu. 2021. "Red Cell Distribution Width as a Prognostic Factor and Its Comparison with Lactate in Patients with Sepsis" Diagnostics 11, no. 8: 1474. https://doi.org/10.3390/diagnostics11081474
APA StyleWang, T.-H., & Hsu, Y.-C. (2021). Red Cell Distribution Width as a Prognostic Factor and Its Comparison with Lactate in Patients with Sepsis. Diagnostics, 11(8), 1474. https://doi.org/10.3390/diagnostics11081474