
Perivascular Adipose Tissue Attenuation on Computed Tomography beyond the Coronary Arteries. A Systematic Review

 ,
,  ,
, 
 , , ,
, , ,
Abstract
:1. Introduction
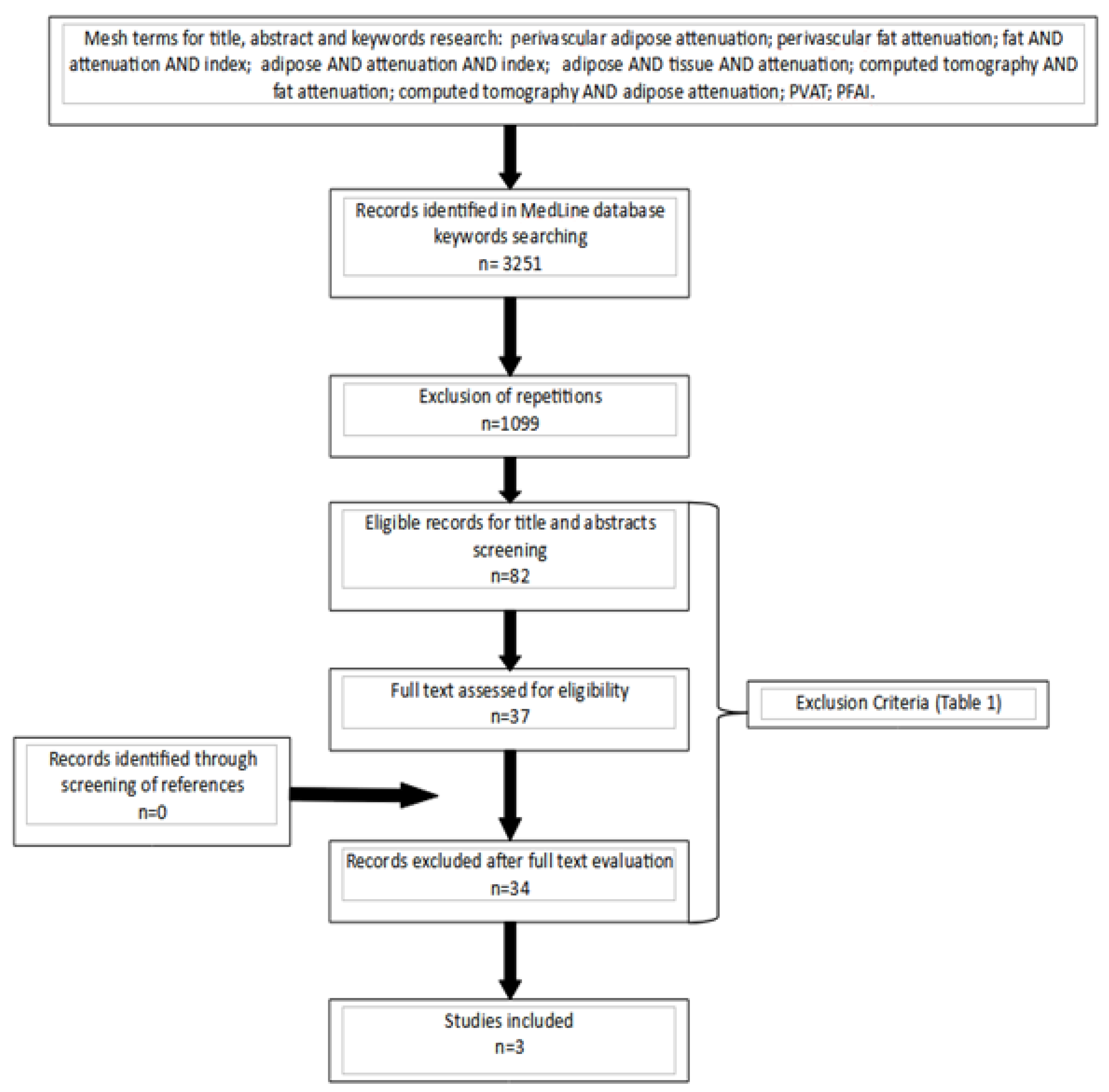
2. Materials and Methods
Data Extraction, Quality Assessment, and Critical Appraisal
3. Results
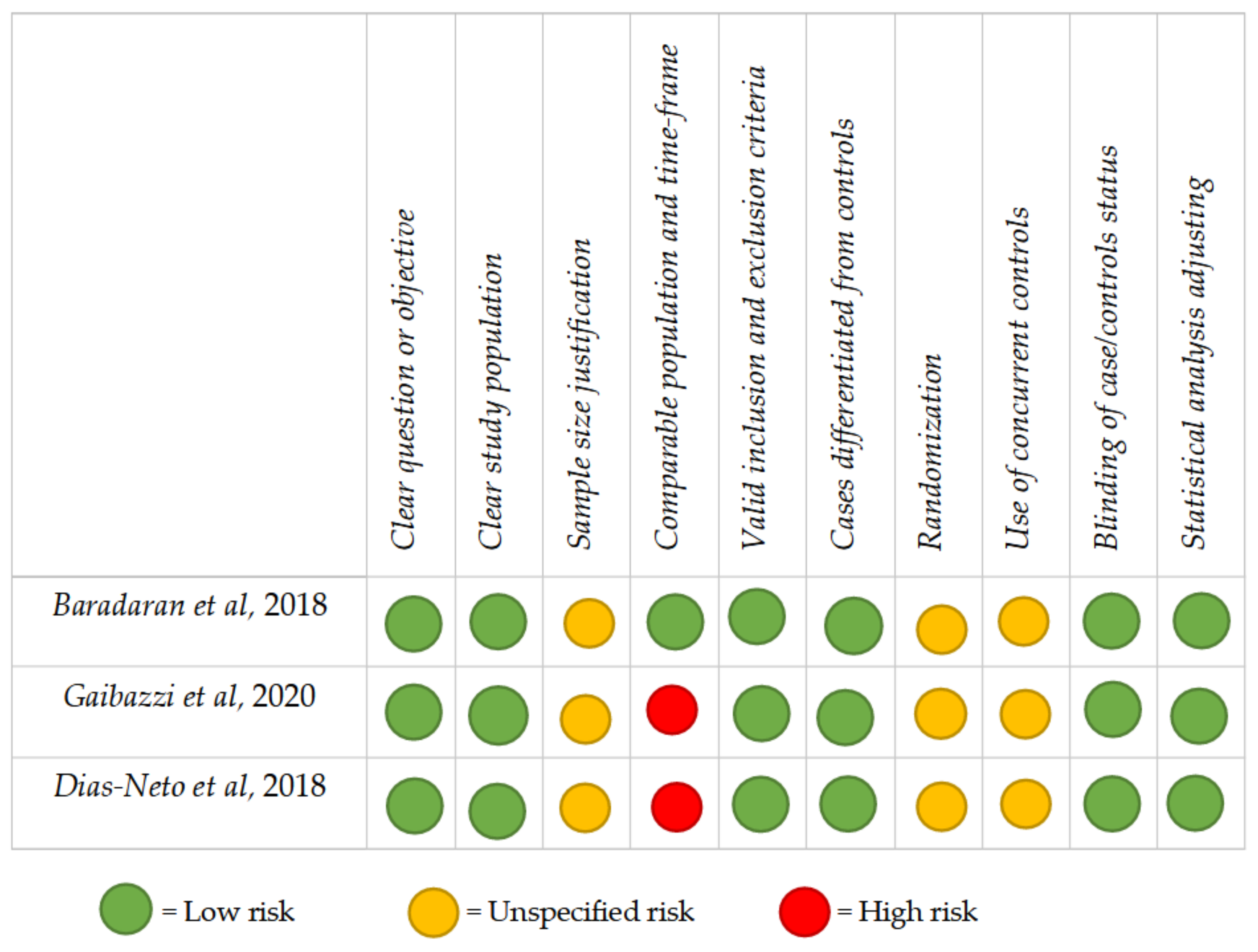
3.1. Quality Assessment
3.2. Level of Evidence
3.3. Perivascular Adipose Tissue Attenuation
3.4. Carotid Artery
3.5. Ascending Thoracic Aorta
3.6. Abdominal Aorta
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availibility Statement
Conflicts of Interest
References
- Meijer, R.I.; Bakker, W.; Alta, C.-L.A.; Sipkema, P.; Yudkin, J.S.; Viollet, B.; Richter, E.A.; Smulders, Y.M.; van Hinsbergh, V.W.; Serné, E.H.; et al. Perivascular adipose tissue control of insulin-induced vasoreactivity in muscle is impaired in db/db mice. Diabetes 2013, 62, 590–598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iozzo, P. Myocardial, perivascular, and epicardial fat. Diabetes Care 2011, 34, S371–S379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ridker, P.M.; Everett, B.M.; Thuren, T.; MacFadyen, J.G.; Chang, W.H.; Ballantyne, C.; Fonseca, F.; Nicolau, J.; Koenig, W.; Anker, S.D.; et al. Antiinflammatory Therapy with Canakinumab for Atherosclerotic Disease. N. Engl. J. Med. 2017, 377, 1119–1131. [Google Scholar] [CrossRef] [PubMed]
- Tardif, J.-C.; Kouz, S.; Waters, D.D.; Bertrand, O.F.; Diaz, R.; Maggioni, A.P.; Pinto, F.J.; Ibrahim, R.; Gamra, H.; Kiwan, G.S.; et al. Efficacy and Safety of Low-Dose Colchicine after Myocardial Infarction. N. Engl. J. Med. 2019, 381, 2497–2505. [Google Scholar] [CrossRef] [PubMed]
- Nidorf, S.M.; Fiolet, A.T.L.; Mosterd, A.; Eikelboom, J.W.; Schut, A.; Opstal, T.S.J.; The, S.H.K.; Xu, X.-F.; Ireland, M.A.; Lenderink, T.; et al. Colchicine in Patients with Chronic Coronary Disease. N. Engl. J. Med. 2020, 383, 1838–1847. [Google Scholar] [CrossRef] [PubMed]
- Oikonomou, E.; Marwan, M.; Desai, M.Y.; Mancio, J.; Alashi, A.; Centeno, E.H.; Thomas, S.; Herdman, L.; Kotanidis, C.; Thomas, K.E.; et al. Non-invasive detection of coronary inflammation using computed tomography and prediction of residual cardiovascular risk (the CRISP CT study): A post-hoc analysis of prospective outcome data. Lancet 2018, 392, 929–939. [Google Scholar] [CrossRef] [Green Version]
- Baradaran, H.; Myneni, P.K.; Patel, P.; Askin, G.; Gialdini, G.; Al-Dasuqi, K.; Kamel, H.; Gupta, A. Association Between Carotid Artery Perivascular Fat Density and Cerebrovascular Ischemic Events. J. Am. Heart Assoc. 2018, 7, e010383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaibazzi, N.; Sartorio, D.; Tuttolomondo, D.; Napolitano, F.; Siniscalchi, C.; Borrello, B.; Palumbo, A.A.; Nicolini, F. Attenuation of peri-vascular fat at computed tomography to measure inflammation in ascending aorta aneurysms. Eur. J. Prev. Cardiol. 2020, 17, 2047487320911846. [Google Scholar] [CrossRef] [PubMed]
- Dias-Neto, M.; Meekel, J.P.; van Schaik, T.G.; Hoozemans, J.; Nunes, F.S.; Henriques-Coelho, T.; Lely, R.J.; Wisselink, W.; Blankensteijn, J.D.; Yeung, K.K. High Density of Periaortic Adipose Tissue in Abdominal Aortic Aneurysm. Eur. J. Vasc. Endovasc. Surg. 2018, 56, 663–671. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rost, N.S.; Wolf, P.A.; Kase, C.S.; Kelly-Hayes, M.; Silbershatz, H.; Massaro, J.; D’Agostino, R.B.; Franzblau, C.; Wilson, P.W. Plasma concentration of C-reactive protein and risk of ischemic stroke and transient ischemic attack: The Framingham study. Stroke 2001, 32, 2575–2579. [Google Scholar] [CrossRef] [PubMed]
- Lombardo, A.; Biasucci, L.M.; Lanza, G.A.; Coli, S.; Silvestri, P.; Cianflone, D.; Liuzzo, G.; Burzotta, F.; Crea, F.; Maseri, A. Inflammation as a possible link between coronary and carotid plaque instability. Circulation 2004, 109, 3158–3163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dinarello, C.A. A clinical perspective of IL-1β as the gatekeeper of inflammation. Eur. J. Immunol. 2011, 41, 1203–1217. [Google Scholar] [CrossRef] [PubMed]
- Johnston, W.F.; Salmon, M.; Pope, N.H.; Meher, A.; Su, G.; Stone, M.L.; Lu, G.; Owens, G.K.; Upchurch, G.R., Jr.; Ailawadi, G. Inhibition of interleukin-1β decreases aneurysm formation and progression in a novel model of thoracic aortic aneurysms. Circulation 2014, 130, S51–S59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Memon, A.; Zarrouk, M.; Ågren-Witteschus, S.; Sundquist, J.; Gottsäter, A.; Sundquist, K. Identification of novel diagnostic and prognostic biomarkers for abdominal aortic aneurysm. Eur. J. Prev. Cardiol. 2020, 27, 132–142. [Google Scholar] [CrossRef] [PubMed]
- Margaritis, M.; Antonopoulos, A.; Digby, J.; Lee, R.; Reilly, S.; Coutinho, P.; Shirodaria, C.; Sayeed, R.; Petrou, M.; De Silva, R.; et al. Interactions between vascular wall and perivascular adipose tissue reveal novel roles for adiponectin in the regulation of endothelial nitric oxide synthase function in human vessels. Circulation 2013, 127, 2209–2221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takaoka, M.; Suzuki, H.; Shioda, S.; Sekikawa, K.; Saito, Y.; Nagai, R.; Sata, M. Endovascular injury induces rapid phenotypic changes in perivascular adipose tissue. Arter. Thromb. Vasc. Biol. 2010, 30, 1576–1582. [Google Scholar] [CrossRef] [PubMed]
- Antonopoulos, A.S.; Sanna, F.; Sabharwal, N.; Thomas, S.; Oikonomou, E.K.; Herdman, L.; Margaritis, M.; Shirodaria, C.; Kampoli, A.-M.; Akoumianakis, I.; et al. Detecting human coronary inflammation by imaging perivascular fat. Sci. Transl. Med. 2017, 9, eaal2658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Konishi, M.; Sugiyama, S.; Sato, Y.; Oshima, S.; Sugamura, K.; Nozaki, T.; Ohba, K.; Matsubara, J.; Sumida, H.; Nagayoshi, Y.; et al. Pericardial fat inflammation correlates with coronary artery disease. Atherosclerosis 2010, 213, 649–655. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Studies published up to November 2020 | Studies different from the case–control setting |
| Studies performed on humans with the execution of perivascular adipose tissue attenuation through computed tomography imaging | Publication type: case reports, conference proceedings, personal communications, letters to the editor, and reviews |
| Studies not written in the English language |
| Authors | Aim | Subjects | Exclusion Criteria | Statistical Significance |
|---|---|---|---|---|
| Baradaran et al. [8] | To evaluate the association between pericarotid inflammation, measured through the density of carotid PVAT on CT, with stroke and TIA. | 94 patients with unilateral ICA stenosis ≥50% to 99%: 42 with stroke or TIA; 52 asymptomatic patients. | Simultaneous bilateral anterior circulation stroke or TIA, bilateral extracranial ICA stenosis. | In the between-subject analysis of stenotic ICAs, symptomatic patients had higher mean pericarotid fat density compared with asymptomatic patients (p = 0.009) without significant difference in non-stenotic ICAs (p = 0.198). Within-subject comparison showed increased density in stenotic ICA versus non-stenotic ICA (p < 0.0001). |
| Gaibazzi et al. [9] | To evaluate differences in periaortic inflammation, measured through ascending aorta PVAT attenuation on CT, among patients with AAA and controls. | 240 subjects: 160 AAA; 80 HC. | Myocardial infarction, heart valvular or ascending aorta surgery, coronary Revascularization, or another type of percutaneous intervention, inflammatory disease, infective disease, or active neoplasia. | In the overall study population, simple linear regression showed a significant positive correlation between the PVAT attenuation and the maximum diameter of the ascending aorta (p < 0.0001). |
| Dias-Neto et al. [10] | To evaluate differences in periaortic inflammation, measured through abdominal aortic PVAT attenuation on CT, among patients with AbAA, AIOD, and patients without aortic disease. | 341 subjects: 140 AbAA; 104 AIOD; 97 HC. | Ruptured AbAA, symptomatic AbAA, inflammatory AbAA, clinical symptoms suggesting aortic inflammation or inflammatory aspects on CT, previous abdominal aortic intervention, active neoplasia, active infection, or incomplete CT scans. | AbAA patients presented higher intra-individual PVAT differences with higher PVAT density around the aneurysm sac than the healthy neck (p < 0.006). |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tuttolomondo, D.; Martini, C.; Nicolini, F.; Formica, F.; Pini, A.; Secchi, F.; Volpi, R.; De Filippo, M.; Gaibazzi, N. Perivascular Adipose Tissue Attenuation on Computed Tomography beyond the Coronary Arteries. A Systematic Review. Diagnostics 2021, 11, 1495. https://doi.org/10.3390/diagnostics11081495
Tuttolomondo D, Martini C, Nicolini F, Formica F, Pini A, Secchi F, Volpi R, De Filippo M, Gaibazzi N. Perivascular Adipose Tissue Attenuation on Computed Tomography beyond the Coronary Arteries. A Systematic Review. Diagnostics. 2021; 11(8):1495. https://doi.org/10.3390/diagnostics11081495
Chicago/Turabian StyleTuttolomondo, Domenico, Chiara Martini, Francesco Nicolini, Francesco Formica, Alessandro Pini, Francesco Secchi, Riccardo Volpi, Massimo De Filippo, and Nicola Gaibazzi. 2021. "Perivascular Adipose Tissue Attenuation on Computed Tomography beyond the Coronary Arteries. A Systematic Review" Diagnostics 11, no. 8: 1495. https://doi.org/10.3390/diagnostics11081495
APA StyleTuttolomondo, D., Martini, C., Nicolini, F., Formica, F., Pini, A., Secchi, F., Volpi, R., De Filippo, M., & Gaibazzi, N. (2021). Perivascular Adipose Tissue Attenuation on Computed Tomography beyond the Coronary Arteries. A Systematic Review. Diagnostics, 11(8), 1495. https://doi.org/10.3390/diagnostics11081495