
Planning the Follow-Up of Patients with Stable Chronic Coronary Artery Disease


Abstract
:1. Introduction
2. Stages in Planning Follow-Up
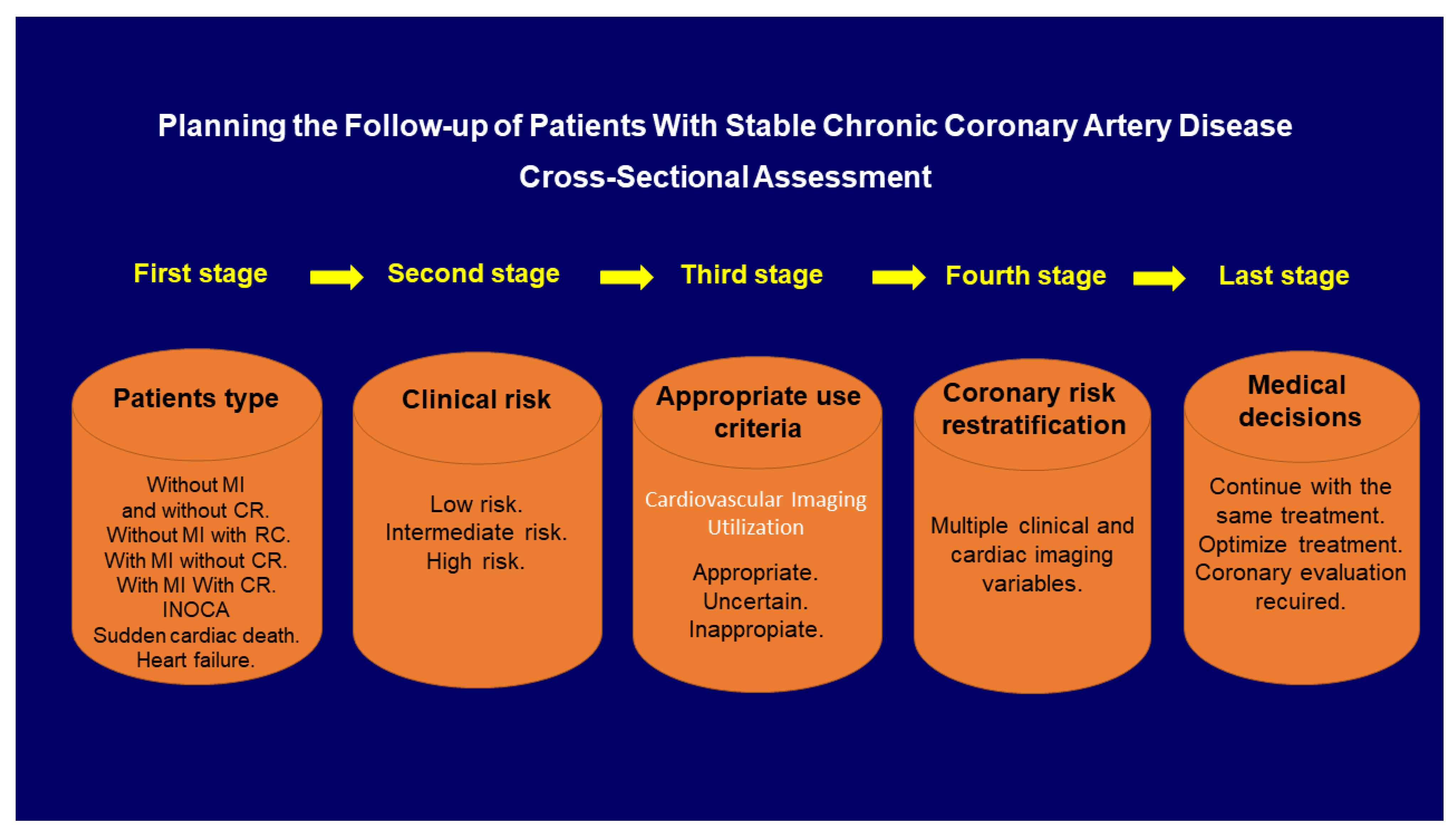
2.1. Cross-Sectional Assessment
2.1.1. First Stage: Type of Patients
2.1.2. Second Stage: Clinical Coronary Risk Stratification
2.1.3. Third Stage: Appropriate Use Criteria in Cardiac Imaging
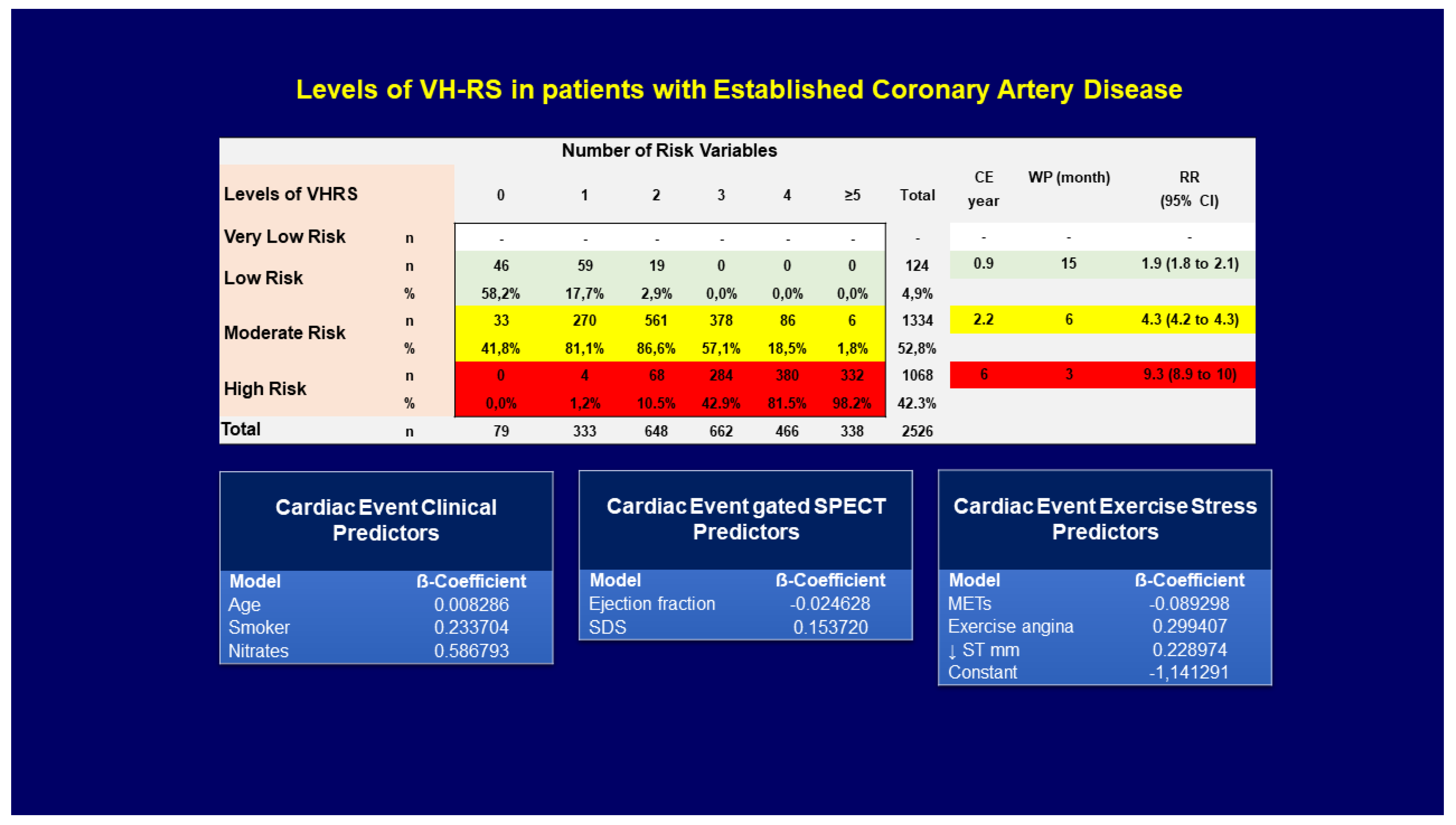
2.1.4. Fourth Stage: Coronary Risk Stratification with Cardiac Imaging
2.1.5. Fifth Stage: Clinical Decision
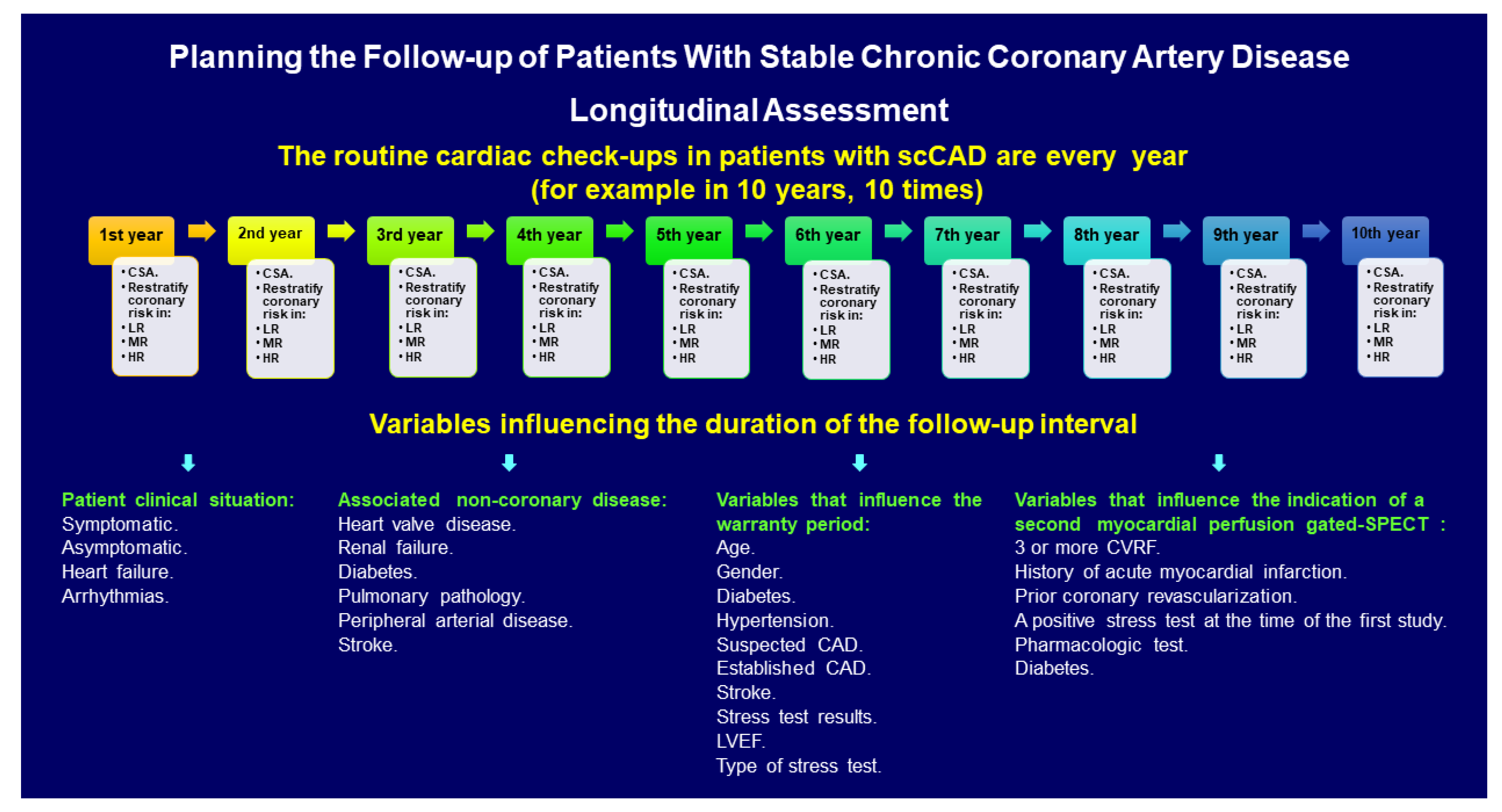
2.2. Longitudinal Assessment
3. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ohman, E.M. Clinical practice. Chronic Stable Angina. N. Engl. J. Med. 2016, 374, 1167–1176. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; De Ferranti, S.; Després, J.P.; Fullerton, H.J.; Howard, V.J.; et al. American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2015 update: A report from the American Heart Association. Circulation 2015, 131, e29–e322. [Google Scholar]
- Nichols, M.; Townsend, N.; Scarborough, P.; Rayner, M. Cardiovascular disease in Europe 2014: Epidemiological update. Eur. Heart J. 2014, 35, 2950–2959. [Google Scholar] [CrossRef] [Green Version]
- Hachamovitch, R.; Hayes, S.W.; Friedman, J.D.; Cohen, I.; Berman, D.S. Stress myocardial perfusion single-photon emission computed tomography is clinically effective and cost effective in risk stratification of patients with a high likelihood of coronary artery disease (CAD) but no known CAD. J. Am. Coll. Cardiol. 2004, 43, 200–208. [Google Scholar] [CrossRef] [Green Version]
- Iskandrian, A.E. The future of nuclear cardiac imaging: Reflection and a vision. J. Nucl. Cardiol. 2018, 25, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Shaw, L.J.; Hachamovitch, R.; Berman, D.S.; Marwick, T.H.; Lauer, M.S.; Heller, G.V.; Iskandrian, A.E.; Kesler, K.L.; Travin, M.I.; Lewin, H.C.; et al. The economic consequences of available diagnostic and prognostic strategies for the evaluation of stable angina patients: An observational assessment of the value of precatheterization ischemia. Economics of Noninvasive Diagnosis (END) Multicenter Study Group. J. Am. Coll. Cardiol. 1999, 33, 661–669. [Google Scholar]
- Taylor, A.J.; Cerqueira, M.; Hodgson, J.M.; Mark, D.; Min, J.; O’Gara, P.; Rubin, G.D.; American College of Cardiology Foundation Appropriate Use Criteria Task Force; Society of Cardiovascular Computed Tomography; American College of Radiology; et al. ACCF/SCCT/ACR/AHA/ASE/ASNC/NASCI/SCAI/SCMR 2010 appropriate use criteria for cardiac computed tomography. A report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, the Society of Cardiovascular Computed Tomography, the American College of Radiology, the American Heart Association, the American Society of Echocardiography, the American Society of Nuclear Cardiology, the North American Society for Cardiovascular Imaging, the Society for Cardiovascular Angiography and Interventions, and the Society for Cardiovascular Magnetic Resonance. J. Am. Coll. Cardiol. 2010, 56, 1864–1894. [Google Scholar] [PubMed]
- Romero-Farina, G.; Montoro-Ronsano, J.; Aguadé-Bruix, S.; Candell-Riera, J. Cost-effectiveness of myocardial perfusion SPECT and stress test according to coronary revascularization therapy, cardiac events and total mortality: Register of 8496 patients. Rev. Española Med. Nuclear Imagen Mol. 2020, 39, 212–219. [Google Scholar] [CrossRef]
- Kunadian, V.; Chieffo, A.; Camici, P.G.; Berry, C.; Escaned, J.; Maas, A.H.E.M.; Prescott, E.; Karam, N.; Appelman, Y.; Fraccaro, C.; et al. An EAPCI Expert Consensus Document on Ischaemia with Non-Obstructive Coronary Arteries in Collaboration with European Society of Cardiology Working Group on Coronary Pathophysiology & Microcirculation Endorsed by Coronary Vasomotor Disorders International Study Group. Eur. Heart J. 2020, 41, 3504–3520. [Google Scholar] [CrossRef]
- Pepine, C.J.; Anderson, R.D.; Sharaf, B.L.; Reis, S.E.; Smith, K.M.; Handberg, E.M.; Johnson, B.D.; Sopko, G.; Bairey Merz, C.N. Coronary microvascular reactivity to adenosine predicts adverse outcome in women evaluated for suspected ischemia results from the National Heart, Lung and Blood Institute WISE (Women’s Ischemia Syndrome Evaluation) study. J. Am. Coll. Cardiol. 2010, 55, 2825–2832. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beltrame, J.F. Assessing patients with myocardial infarction and nonobstructed coronary arteries (MINOCA). J. Intern. Med. 2013, 273, 182–185. [Google Scholar] [CrossRef]
- Safdar, B.; Spatz, E.S.; Dreyer, R.P.; Beltrame, J.F.; Lichtman, J.H.; Spertus, J.A.; Reynolds, H.R.; Geda, M.; Bueno, H.; Dziura, J.D.; et al. Presentation, Clinical Profile, and Prognosis of Young Patients with Myocardial Infarction with Nonobstructive Coronary Arteries (MINOCA): Results from the VIRGO Study. J. Am. Heart Assoc. 2018, 7, 009174. [Google Scholar] [CrossRef] [Green Version]
- Stefanini, G.G.; Alfonso, F.; Barbato, E.; Byrne, R.; Capodanno, D.; Colleran, R.; Escaned, J.; Giacoppo, D.; Kunadian, V.; Lansky, A.; et al. Management of myocardial revascularisation failure: An expert consensus document of the EAPCI. EuroIntervention 2020, 16, e875–e890. [Google Scholar] [CrossRef]
- Lala, A.; Desai, A.S. The Role of Coronary Artery Disease in Heart Failure. Heart Fail. Clin. 2014, 10, 353–365. [Google Scholar] [CrossRef] [PubMed]
- Mohammed, S.F.; Hussain, S.; Mirzoyev, S.A.; Edwards, W.D.; Maleszewski, J.J.; Redfield, M.M. Coronary Microvascular Rarefaction and Myocardial Fibrosis in Heart Failure with Preserved Ejection Fraction. Circulation 2015, 131, 550–559. [Google Scholar] [CrossRef] [Green Version]
- Sara, J.D.; Lennon, R.J.; Gulati, R.; Singh, M.; Holmes, D.R., Jr.; Lerman, L.O.; Lerman, A. Utility of the Framingham Risk Score in predicting secondary events in patients following percutaneous coronary intervention: A time-trend analysis. Am. Heart J. 2015, 172, 115–128. [Google Scholar] [CrossRef] [PubMed]
- Conroy, R.M.; Pyörälä, K.; Fitzgerald, A.P.; Sans, S.; Menotti, A.; De Backer, G.; De Bacquer, D.; Ducimetière, P.; Jousilahti, P.; Keil, U.; et al. Estimation of ten-year risk of fatal cardiovascular disease in Europe: The SCORE project. Eur. Heart J. 2003, 24, 987–1003. [Google Scholar] [CrossRef]
- Biener, M.; Giannitsis, E.; Kuhner, M.; Zelniker, T.; Mueller-Hennessen, M.; Vafaie, M.; Stoyanov, K.M.; Neumann, F.-J.; Katus, H.A.; Hochholzer, W.; et al. Risk prediction in stable cardiovascular disease using a high-sensitivity cardiac troponin T single biomarker strategy compared to the ESC-SCORE. Open Heart 2018, 5, e000710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grundy, S.M.; Cleeman, J.I.; Bairey Merz, C.N.; Brewer, H.B.; Clark, L.T.; Hunninghake, D.B.; Pasternak, R.C.; Smith, S.C.; Stone, N.J. Coordinating Committee of the National Cholesterol Education Program. Implications of recent clinical trials for the National Cholesterol Education Program Adult Treatment Panel III guidelines. Circulation 2004, 110, 227–239. [Google Scholar] [CrossRef] [Green Version]
- Hendel, R.C.; Berman, D.S.; Di Carli, M.F.; Heidenreich, P.A.; Henkin, R.E.; Pellikka, P.A.; Pohost, G.M.; Williams, K.A. ACCF/ASNC/ACR/AHA/ASE/SCCT/SCMR/SNM 2009 appropriate use criteria for cardiac radionuclide imaging: A report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, the American Society of Nuclear Cardiology, the American College of Radiology, the American Heart Association, the American Society of Echocardiography, the Society of Cardiovascular Computed Tomography, the Society for Cardiovascular Magnetic Resonance, and the Society of Nuclear Medicine. Circulation 2009, 119, e561–e587. [Google Scholar]
- Patel, M.R.; Calhoon, J.H.; Dehmer, G.J.; Grantham, J.A.; Maddox, T.M.; Maron, D.J.; Smith, P.K. ACC/AATS/AHA/ASE/ASNC/SCAI/SCCT/STS 2017 Appropriate Use Criteria for Coronary Revascularization in Patients With Stable Ischemic Heart Disease: A Report of the American College of Cardiology Appropriate Use Criteria Task Force, American Association for Thoracic Surgery, American Heart Association, American Society of Echocardiography, American Society of Nuclear Cardiology, Society for Cardiovascular Angiography and Interventions, Society of Cardiovascular Computed Tomography, and Society of Thoracic Surgeons. J. Am. Coll. Cardiol. 2017, 69, 2212–2241. [Google Scholar]
- Trägårdh, E.; Tan, S.S.; Bucerius, J.; Gimelli, A.; Gaemperli, O.; Lindner, O.; Agostini, D.; Übleis, C.; Sciagra, R.; Slart, R.H.; et al. Systematic review of cost-effectiveness of myocardial perfusion scintigraphy in patients with ischaemic heart disease: A report from the cardiovascular committee of the European Association of Nuclear Medicine. Endorsed by the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging. 2017, 18, 825–832. [Google Scholar] [PubMed]
- Hernández, R.; Vale, L. The Value of Myocardial Perfusion Scintigraphy in the Diagnosis and Management of Angina and Myocardial Infarction: A Probabilistic Economic Analysis. Med. Decis. Mak. 2007, 27, 772–788. [Google Scholar] [CrossRef] [Green Version]
- Hayes-Brown, K.; Frogge, N.; Doukky, R. The impact of appropriate use on the cost effectiveness of spect myocardial perfusion imaging in the community setting. J. Am. Coll. Cardiol. 2014, 63, A1222. [Google Scholar] [CrossRef] [Green Version]
- Popescu, B.A.; Stefanidis, A.; Fox, K.F.; Cosyns, B.; Delgado, V.; Di Salvo, G.D.; Donal, E.; Flachskampf, F.A.; Galderisi, M.; Lancellotti, P.; et al. Multimodality imaging in cardiology: A statement on behalf of the Task Force on Multimodality Imaging of the European Association of Cardiovascular Imaging. Eur. Heart J. 2019, 40, 553–558. [Google Scholar]
- Shaw, L.J.; Min, J.K.; Hachamovitch, R.; Hendel, R.C.; Borges-Neto, S.; Berman, D.S. Nomograms for estimating coronary artery disease prognosis with gated stress myocardial perfusion SPECT. J. Nucl. Cardiol. 2011, 19, 43–52. [Google Scholar] [CrossRef] [PubMed]
- McClelland, R.L.; Jorgensen, N.W.; Budoff, M.; Blaha, M.J.; Post, W.S.; Kronmal, R.A.; Bild, D.E.; Shea, S.; Liu, K.; Watson, K.E.; et al. 10-Year Coronary Heart Disease Risk Prediction Using Coronary Artery Calcium and Traditional Risk Factors: Derivation in the MESA (Multi-Ethnic Study of Atherosclerosis) With Validation in the HNR (Heinz Nixdorf Recall) Study and the DHS (Dallas Heart Study). J. Am. Coll. Cardiol. 2015, 66, 1643–1653. [Google Scholar] [PubMed] [Green Version]
- Romero-Farina, G.; Candell-Riera, J.; Aguadé-Bruix, S.; Dorado, D.G. A novel clinical risk prediction model for myocardial infarction, coronary revascularization, and cardiac death according to clinical, exercise, and gated SPECT variables (VH-RS). Eur. Heart J. Cardiovasc. Imaging 2019, 21, 210–221. [Google Scholar] [CrossRef] [PubMed]
- Barbato, E.; Aarnoudse, W.; Aengevaeren, W.R.; Werner, G.; Klauss, V.; Bojara, W.; Herzfeld, I.; Oldroyd, K.G.; Pijls, N.H.; De Bruyne, B. Validation of coronary flow re-serve measurements by thermodilution in clinical practice. Eur. Heart J. 2004, 25, 219–223. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.M.; Jung, J.-H.; Hwang, D.; Park, J.; Fan, Y.; Na, S.-H.; Doh, J.-H.; Nam, C.-W.; Shin, E.-S.; Koo, B.-K. Coronary Flow Reserve and Microcirculatory Resistance in Patients with Intermediate Coronary Stenosis. J. Am. Coll. Cardiol. 2016, 67, 1158–1169. [Google Scholar] [CrossRef]
- Williams, R.P.; de Waard, G.A.; De Silva, K.; Lumley, M.; Asrress, K.; Arri, S.; Ellis, H.; Mir, A.; Clapp, B.; Chiribiri, A.; et al. Doppler Versus Thermodilution-Derived Coronary Microvascular Resistance to Predict Coronary Microvascular Dysfunction in Patients With Acute Myocardial Infarction or Stable Angina Pectoris. Am. J. Cardiol. 2018, 121, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Moody, J.B.; Poitrasson-Riviere, A.; Hagio, T.; Buckley, C.; Weinberg, R.L.; Corbett, J.R.; Murthy, V.L.; Ficaro, E.P. Added value of myocardial blood flow using 18F-flurpiridaz PET to diagnose coronary artery disease: The flurpiridaz 301 trial. J. Nucl. Cardiol. 2020, 30, 1–7. [Google Scholar] [CrossRef]
- Acampa, W.; Zampella, E.; Assante, R.; Genova, A.; De Simini, G.; Mannarino, T.; D’Antonio, A.; Gaudieri, V.; Nappi, C.; Buongiorno, P.; et al. Quantification of myocardial perfusion reserve by CZT-SPECT: A head to head comparison with 82Rubidium PET imaging. J. Nucl. Cardiol. 2020. [Google Scholar] [CrossRef]
- Romero-Farina, G.; Candell-Riera, J.; Aguadé-Bruix, S.; Ferreira-González, I.; Cuberas-Borrós, G.; Pizzi, N.; García-Dorado, D.; Pizzi, M.N. Warranty periods for normal myocardial perfusion stress SPECT. J. Nucl. Cardiol. 2014, 22, 44–54. [Google Scholar] [CrossRef] [PubMed]
- Petretta, M.; Acampa, W.; Assante, R.; Zampella, E.; Nappi, C.; Petretta, A.; Cuocolo, A. My warranty has expired: I need to be retested. J. Nucl. Cardiol. 2019, 26, 998–1006. [Google Scholar] [CrossRef]
- Romero-Farina, G.; Candell-Riera, J.; Aguadé-Bruix, S.; Cuberas-Borros, G.; Pizzi, M.; Santos, A.; De Leon, G.; García-Dorado, D. Variables that influence the indication of a second myocardial perfusion gated-SPECT after a normal stress-rest gated SPECT. Rev. Española Med. Nuclear Imagen Mol. 2014, 33, 72–78. [Google Scholar] [CrossRef] [PubMed]
- Radico, F.; Zimarino, M.; Fulgenzi, F.; Ricci, F.; Di Nicola, M.; Jespersen, L.; Chang, S.M.; Humphries, K.H.; Marzilli, M.; De Caterina, R. Determinants of long-term clinical outcomes in patients with angina but without obstructive coronary artery disease: A systematic review and meta-analysis. Eur. Heart J. 2018, 39, 2135–2146. [Google Scholar] [CrossRef]
- Seitz, A.; Gardezy, J.; Pirozzolo, G.; Probst, S.; Athanasiadis, A.; Hill, S.; Mahrholdt, H.; Bekeredjian, R.; Sechtem, U.; Ong, P. Long-Term Follow-Up in Patients with Stable Angina and Unob-structed Coronary Arteries Undergoing Intracoronary Acetylcholine Testing. JACC Cardiovasc. Interv. 2020, 13, 1865–1876. [Google Scholar] [CrossRef]
- Romero-Farina, G.; Candell-Riera, J.; Aguadé-Bruix, S.; Pizzi, M.N.; García-Dorado, D. Different prognosis according to different clinical, electrocardiographic and scintigraphic ischemia criteria. Int. J. Cardiol. 2016, 219, 240–246. [Google Scholar] [CrossRef] [PubMed]
- Gheorghiade, M.; Sopko, G.; De Luca, L.; Velazquez, E.J.; Parker, J.; Binkley, P.F.; Sadowski, Z.; Golba, K.; Prior, D.L.; Rouleau, J.L.; et al. Navigating the Crossroads of Coronary Artery Disease and Heart Failure. Circulation 2006, 114, 1202–1213. [Google Scholar] [CrossRef] [PubMed]
- Mishra, R.K.; Tison, G.H.; Fang, Q.; Scherzer, R.; Whooley, M.A.; Schiller, N. B Association of Machine Learning-Derived Phenogroupings of Echocardiographic Variables with Heart Failure in Stable Coronary Artery Disease: The Heart and Soul Study. J. Am. Soc. Echocardiogr. 2020, 33, 322–331. [Google Scholar] [CrossRef]
- Romero-Farina, G.; Aguadé-Bruix, S.; Cuellar-Calabria, H.; Pizzi, M.N.; Roque, A.; Candell-Riera, J. Gender differences in outcome in patients with diabetes mellitus. J. Nucl. Cardiol. 2020. [Google Scholar] [CrossRef]
- Peix, A. Choosing between anatomy and function is not always evident for the heart of end-stage renal disease patients. How low can we go? J. Nucl. Cardiol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Kolkailah, A.A.; Iskander, M.; Iskander, F.; Patel, P.P.; Khan, R.; Doukky, R. The prognostic utility of regadenoson SPECT myocardial perfusion imaging in patients with end-stage renal disease: The largest cohort to date. J. Nucl. Cardiol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Wenning, C.; Vrachimis, A.; Pavenstädt, H.-J.; Reuter, S.; Schäfers, M. Coronary artery calcium burden, carotid atherosclerotic plaque burden, and myocardial blood flow in patients with end-stage renal disease: A non-invasive imaging study combining PET/CT and 3D ultrasound. J. Nucl. Cardiol. 2020. [Google Scholar] [CrossRef] [Green Version]
- Bangalore, S.; Maron, D.J.; O’Brien, S.M.; Fleg, J.L.; Kretov, E.I.; Briguori, C.; Kaul, U.; Reynolds, H.; Mazurek, T.; Sidhu, M.S.; et al. Management of Coronary Disease in Patients with Advanced Kidney Disease. N. Engl. J. Med. 2020, 382, 1608–1618. [Google Scholar] [CrossRef] [PubMed]
- Takahara, M.; Iida, O.; Kohsaka, S.; Soga, Y.; Fujihara, M.; Shinke, T.; Amano, T.; Ikari, Y. J-EVT and J-PCI investigators. Diabetes mellitus and other cardiovascular risk factors in low-er-extremity peripheral artery disease versus coronary artery disease: An analysis of 1,121,359 cases from the nationwide databases. Cardiovasc. Diabetol. 2019, 18, 155. [Google Scholar] [CrossRef]
- Curtis, A.B.; Karki, R.; Hattoum, A.; Sharma, U.C. Arrhythmias in Patients ≥80 Years of Age: Pathophysiology, Management, and Outcomes. J. Am. Coll. Cardiol. 2018, 71, 2041–2057. [Google Scholar] [CrossRef]
- Nappi, C.; Gaudieri, V.; Acampa, W.; Arumugam, P.; Assante, R.; Zampella, E.; Mannarino, T.; Mainolfi, C.G.; Imbriaco, M.; Petretta, M.; et al. Coronary vascular age: An alternate means for predicting stress-induced myocardial ischemia in patients with suspected coronary artery disease. J. Nucl. Cardiol. 2018, 26, 1348–1355. [Google Scholar] [CrossRef]
- Fowkes, R.; Byrne, M.; Sinclair, H.; Tang, E.; Kunadian, V. Coronary artery disease in patients with dementia. Coron. Artery Dis. 2016, 27, 511–520. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age |
|---|
| Gender |
| Smoking status |
| Systolic blood pressure |
| Total cholesterol |
| Triglyceride level |
| High-density lipoprotein |
| Low-density lipoprotein |
| Medication for blood pressure |
| Are any of the following present? (Yes or No) |
| 1. Clinical coronary heart disease: |
| Myocardial infarction, |
| Unstable angina or stable angina, |
| Coronary artery procedures (angioplasty or bypass surgery), |
| Evidence of clinically significant myocardial ischemia. |
| 2. Coronary heart disease risk equivalents: includes clinical manifestations of non-coronary forms of atherosclerotic disease: |
| Peripheral arterial disease, |
| Abdominal aortic aneurysm, |
| Carotid artery disease (transient ischemic attacks or stroke of carotid origin or >50% obstruction of a carotid artery), |
| Diabetes, and |
| ≥2 risk factors with 10-year risk for hard coronary heart disease >20%. |
| How many of the following risk factors are present if any? (Score: 1,2,3,4,5) (Note: if high-density lipoprotein ≥60, subtract one from the total count). |
| Cigarette smoking, |
| Hypertension (BP ≥ 140/90 mmHg or on antihypertensive medication), |
| Low high-density lipoprotein cholesterol (<40 mg/dL), |
| Family history of premature coronary heart disease (coronary heart disease in male first-degree relative < 55 years, coronary heart disease in female first-degree relative <65 years), |
| Age (men ≥45 years; women ≥ 55 years). |
| Metabolic syndrome. Are at least three of the following present after 3 months of therapeutic lifestyle changes? (Yes: ≥3 criteria met; or No: <3 criteria met). |
| 1. Abdominal obesity (waist circumference) |
| Women: >88 cm (>35 in). |
| 2. Triglycerides ≥ 150 mg/dL. |
| 3. High-density lipoprotein cholesterol |
| Women: <50 mg/dL. |
| 4. Blood pressure: ≥130/≥85 mmHg. |
| 5. Fasting glucose: ≥110 mg/dL. |
| Microvascular Angina | Vasospastic Angina | Silent Myocardial Ischemia | Heart Failure |
|---|---|---|---|
| Persistent chest pain | Repeated angina episodes | Male | Differentiate cardiopulmonary structural and functional abnormalities |
| Smoking | Non-fata lmyocardial infarction | Diabetes | |
| Diabetes | Repeated angiographies | Pharmacologic stress test | |
| Increased QTc interval | ST segment depression | ||
| Diabetes | Renal Failure | Peripheral Arterial Disease | Advanced Age |
| Gender | Age | Diabetes | Elderly patients |
| Age | Diabetes | End-stage renal disease | Arrhythmias |
| Insulin treatment | End-stage renal disease | Coronary risk factors | Dementia |
| Nitrates | Vascular calcification | Coronary risk factors | |
| Hypercholesterolemia | Carotid plaque burden | ||
| Known coronary artery disease | |||
| Peripheral artery disease | |||
| Dipyridamole stress |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Romero-Farina, G.; Aguadé-Bruix, S. Planning the Follow-Up of Patients with Stable Chronic Coronary Artery Disease. Diagnostics 2021, 11, 1762. https://doi.org/10.3390/diagnostics11101762
Romero-Farina G, Aguadé-Bruix S. Planning the Follow-Up of Patients with Stable Chronic Coronary Artery Disease. Diagnostics. 2021; 11(10):1762. https://doi.org/10.3390/diagnostics11101762
Chicago/Turabian StyleRomero-Farina, Guillermo, and Santiago Aguadé-Bruix. 2021. "Planning the Follow-Up of Patients with Stable Chronic Coronary Artery Disease" Diagnostics 11, no. 10: 1762. https://doi.org/10.3390/diagnostics11101762
APA StyleRomero-Farina, G., & Aguadé-Bruix, S. (2021). Planning the Follow-Up of Patients with Stable Chronic Coronary Artery Disease. Diagnostics, 11(10), 1762. https://doi.org/10.3390/diagnostics11101762