
Association between Intraoperative Hyperlactatemia and Myocardial Injury after Noncardiac Surgery

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Approval
2.2. Study Population and Data Collection
2.3. Study Outcome and Definitions
2.4. Perioperative cTn I Measurement
2.5. Intraoperative Lactate Measurement
2.6. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Clinical Outcomes
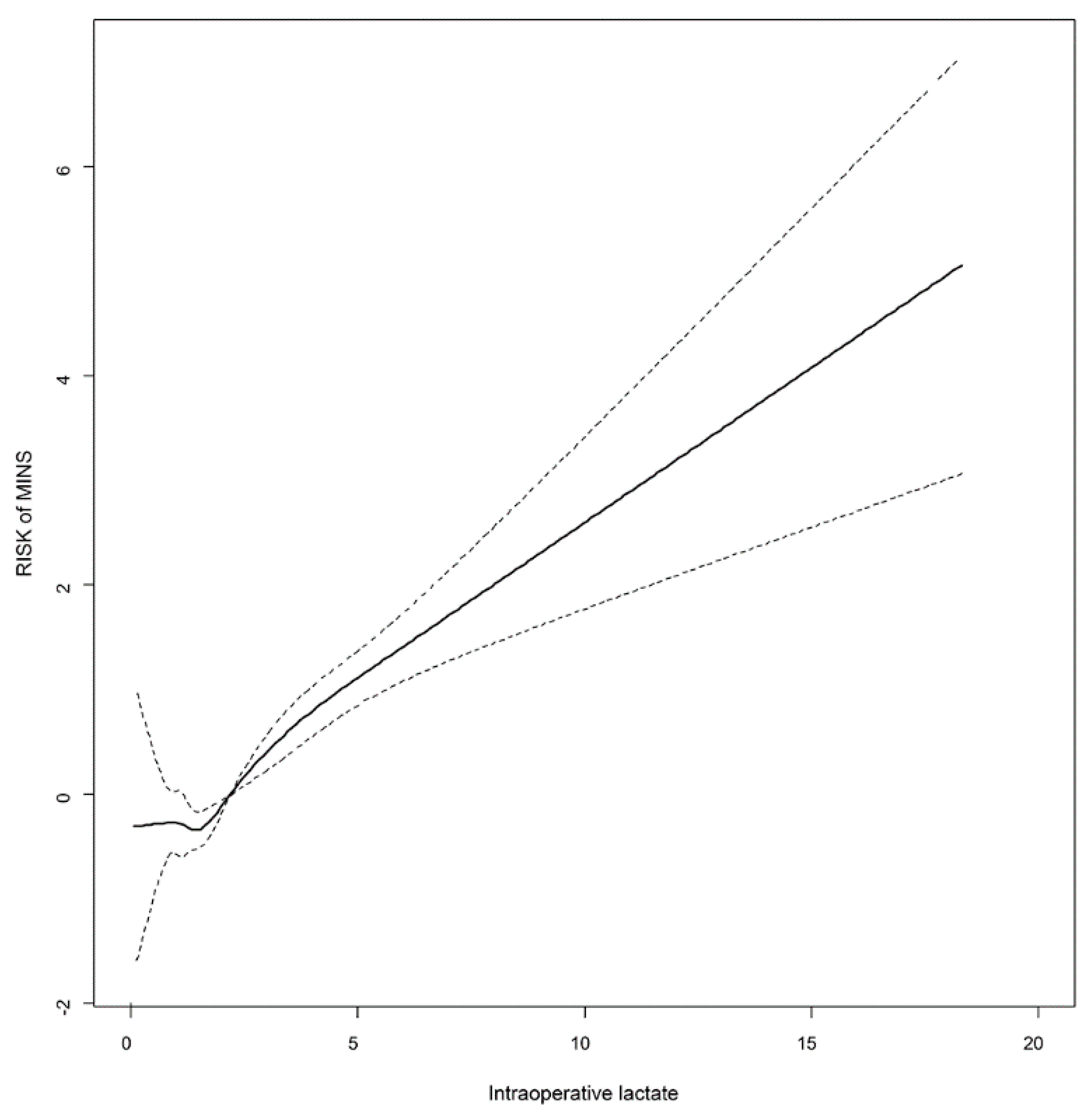
3.3. Threshold
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Devereaux, P.J.; Szczeklik, W. Myocardial injury after non-cardiac surgery: Diagnosis and management. Eur. Heart J. 2020, 41, 3083–3091. [Google Scholar] [CrossRef]
- Botto, F.; Alonso-Coello, P.; Chan, M.T.; Villar, J.C.; Xavier, D.; Srinathan, S.; Guyatt, G.; Cruz, P.; Graham, M.; Wang, C.Y.; et al. Myocardial injury after noncardiac surgery: A large, international, prospective cohort study establishing diagnostic criteria, characteristics, predictors, and 30-day outcomes. Anesthesiology 2014, 120, 564–578. [Google Scholar] [CrossRef]
- Writing Committee for the Vision Study Investigators; Devereaux, P.J.; Biccard, B.M.; Sigamani, A.; Xavier, D.; Chan, M.T.V.; Srinathan, S.K.; Walsh, M.; Abraham, V.; Pearse, R.; et al. Association of Postoperative High-Sensitivity Troponin Levels with Myocardial Injury and 30-Day Mortality Among Patients Undergoing Noncardiac Surgery. JAMA 2017, 317, 1642–1651. [Google Scholar] [CrossRef] [PubMed]
- Smilowitz, N.R.; Redel-Traub, G.; Hausvater, A.; Armanious, A.; Nicholson, J.; Puelacher, C.; Berger, J.S. Myocardial injury after non-cardiac surgery: A systematic review and meta-analysis. Cardiol. Rev. 2019, 27, 267. [Google Scholar] [CrossRef] [PubMed]
- Nagele, P.; Brown, F.; Gage, B.F.; Gibson, D.W.; Miller, J.P.; Jaffe, A.S.; Apple, F.S.; Scott, M.G. High-sensitivity cardiac troponin T in prediction and diagnosis of myocardial infarction and long-term mortality after noncardiac surgery. Am. Heart J. 2013, 166, 325–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Husain, F.A.; Martin, M.J.; Mullenix, P.S.; Steele, S.R.; Elliott, D.C. Serum lactate and base deficit as predictors of mortality and morbidity. Am. J. Surg. 2003, 185, 485–491. [Google Scholar] [CrossRef]
- Bar, S.; Nguyen, M.; de Broca, B.; Bernard, E.; Dupont, H.; Guinot, P.-G. Risk factors and determinants of intraoperative hyperlactatemia in major non-cardiac surgery. J. Clin. Anesth. 2021, 110359. [Google Scholar] [CrossRef] [PubMed]
- Gulmez, S.; Uzun, O.; Senger, A.S.; Keklikkiran, Z.Z.; Bozkurt, H.; Omeroglu, S.; Bozdag, E.; Avan, D.; Polat, E.; Duman, M. Risk factors for persistent elevation of perioperative lactate levels in gastric cancer surgery. Asian J. Med. Sci. 2020, 11, 24–28. [Google Scholar] [CrossRef]
- Valenza, F.; Aletti, G.; Fossali, T.; Chevallard, G.; Sacconi, F.; Irace, M.; Gattinoni, L. Lactate as a marker of energy failure in critically ill patients: Hypothesis. Crit. Care 2005, 9, 588–593. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saugel, B.; Trepte, C.J.; Heckel, K.; Wagner, J.Y.; Reuter, D.A. Hemodynamic management of septic shock: Is it time for “individualized goal-directed hemodynamic therapy” and for specifically targeting the microcirculation? Shock 2015, 43, 522–529. [Google Scholar] [CrossRef]
- Kristensen, S.D.; Knuuti, J. New ESC/ESA Guidelines on non-cardiac surgery: Cardiovascular assessment and management. Eur. Heart J. 2014, 35, 2344–2345. [Google Scholar] [CrossRef] [PubMed]
- Lee, T.H.; Marcantonio, E.R.; Mangione, C.M.; Thomas, E.J.; Polanczyk, C.A.; Cook, E.F.; Sugarbaker, D.J.; Donaldson, M.C.; Poss, R.; Ho, K.K.; et al. Derivation and prospective validation of a simple index for prediction of cardiac risk of major noncardiac surgery. Circulation 1999, 100, 1043–1049. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Latouche, A.; Porcher, R.; Chevret, S. Sample size formula for proportional hazards modelling of competing risks. Stat. Med. 2004, 23, 3263–3274. [Google Scholar] [CrossRef] [PubMed]
- Groenwold, R.H.; Nelson, D.B.; Nichol, K.L.; Hoes, A.W.; Hak, E. Sensitivity analyses to estimate the potential impact of unmeasured confounding in causal research. Int. J. Epidemiol. 2010, 39, 107–117. [Google Scholar] [CrossRef] [PubMed]
- Hajjar, L.A.; Almeida, J.P.; Fukushima, J.T.; Rhodes, A.; Vincent, J.-L.; Osawa, E.A.; Galas, F.R. High lactate levels are predictors of major complications after cardiac surgery. J. Thorac. Cardiovasc. Surg. 2013, 146, 455–460. [Google Scholar] [CrossRef] [Green Version]
- Kogan, A.; Preisman, S.; Bar, A.; Sternik, L.; Lavee, J.; Malachy, A.; Spiegelstein, D.; Berkenstadt, H.; Raanani, E. The impact of hyperlactatemia on postoperative outcome after adult cardiac surgery. J. Anesth. 2012, 26, 174–178. [Google Scholar] [CrossRef]
- Khosravani, H.; Shahpori, R.; Stelfox, H.T.; Kirkpatrick, A.W.; Laupland, K.B. Occurrence and adverse effect on outcome of hyperlactatemia in the critically ill. Crit. Care 2009, 13, R90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Attana, P.; Lazzeri, C.; Picariello, C.; Dini, C.S.; Gensini, G.F.; Valente, S. Lactate and lactate clearance in acute cardiac care patients. Eur. Heart J. Acute Cardiovasc. Care 2012, 1, 115–121. [Google Scholar] [CrossRef] [Green Version]
- Cady, L.D., Jr.; Weil, M.H.; Afifi, A.A.; Michaels, S.F.; Liu, V.Y.; Shubin, H. Quantitation of severity of critical illness with special reference to blood lactate. Crit. Care Med. 1973, 1, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Cecconi, M.; De Backer, D.; Antonelli, M.; Beale, R.; Bakker, J.; Hofer, C.; Jaeschke, R.; Mebazaa, A.; Pinsky, M.R.; Teboul, J.L.; et al. Consensus on circulatory shock and hemodynamic monitoring. Task force of the European Society of Intensive Care Medicine. Intensive Care Med. 2014, 40, 1795–1815. [Google Scholar] [CrossRef]
- Juneja, D.; Singh, O.; Dang, R. Admission hyperlactatemia: Causes, incidence, and impact on outcome of patients admitted in a general medical intensive care unit. J. Crit. Care 2011, 26, 316–320. [Google Scholar] [CrossRef] [PubMed]
- Kraut, J.A.; Madias, N.E. Lactic acidosis. N. Engl. J. Med. 2014, 371, 2309–2319. [Google Scholar] [CrossRef] [PubMed]
- Karlander, L.-E.; Henriksson, J.; Sjöberg, F. Acidosis in muscle tissue distal to vascular contusion despite unchanged global blood flow in rats: An uncoupling of microvascular blood flow and metabolism? Microvasc. Res. 2005, 70, 111–115. [Google Scholar] [CrossRef]
- Lalau, J.-D. Lactic acidosis induced by metformin. Drug Saf. 2010, 33, 727–740. [Google Scholar] [CrossRef]
- Sheth, T.; Natarajan, M.K.; Hsieh, V.; Valettas, N.; Rokoss, M.; Mehta, S.; Jolly, S.; Tandon, V.; Bezerra, H.; Devereaux, P.J. Incidence of thrombosis in perioperative and non-operative myocardial infarction. Br. J. Anaesth. 2018, 120, 725–733. [Google Scholar] [CrossRef] [Green Version]
- Di Vito, L.; Yoon, J.H.; Kato, K.; Yonetsu, T.; Vergallo, R.; Costa, M.; Bezerra, H.G.; Arbustini, E.; Narula, J.; Crea, F.; et al. Comprehensive overview of definitions for optical coherence tomography-based plaque and stent analyses. Coron. Artery Dis. 2014, 25, 172–185. [Google Scholar] [CrossRef]
- Devereaux, P.J.; Xavier, D.; Pogue, J.; Guyatt, G.; Sigamani, A.; Garutti, I.; Leslie, K.; Rao-Melacini, P.; Chrolavicius, S.; Yang, H.; et al. Characteristics and short-term prognosis of perioperative myocardial infarction in patients undergoing noncardiac surgery: A cohort study. Ann. Intern. Med. 2011, 154, 523–528. [Google Scholar] [CrossRef]
- Smilowitz, N.R.; Gupta, N.; Guo, Y.; Berger, J.S.; Bangalore, S. Perioperative acute myocardial infarction associated with non-cardiac surgery. Eur. Heart J. 2017, 38, 2409–2417. [Google Scholar] [CrossRef]
- Guagliumi, G.; Capodanno, D.; Saia, F.; Musumeci, G.; Tarantini, G.; Garbo, R.; Tumminello, G.; Sirbu, V.; Coccato, M.; Fineschi, M.; et al. Mechanisms of atherothrombosis and vascular response to primary percutaneous coronary intervention in women versus men with acute myocardial infarction: Results of the OCTAVIA study. JACC Cardiovasc. Interv. 2014, 7, 958–968. [Google Scholar] [CrossRef] [PubMed]
- Veličković, J.; Palibrk, I.; Miličić, B.; Veličković, D.; Jovanović, B.; Rakić, G.; Petrović, M.; Bumbaširević, V. The association of early postoperative lactate levels with morbidity after elective major abdominal surgery. Bosn. J. Basic Med. Sci. 2019, 19, 72. [Google Scholar] [CrossRef] [Green Version]
- Meyer, Z.C.; Schreinemakers, J.M.; Mulder, P.G.; de Waal, R.A.; Ermens, A.A.; van der Laan, L. Determining the clinical value of lactate in surgical patients on the intensive care unit. J. Surg. Res. 2013, 183, 814–820. [Google Scholar] [CrossRef] [PubMed]
- Vibert, E.; Boleslawski, E.; Cosse, C.; Adam, R.; Castaing, D.; Cherqui, D.; Naili, S.; Régimbeau, J.-M.; Cunha, A.S.; Truant, S. Arterial lactate concentration at the end of an elective hepatectomy is an early predictor of the postoperative course and a potential surrogate of intraoperative events. Ann. Surg. 2015, 262, 787–793. [Google Scholar] [CrossRef]
- Abe, T.; Uchino, S.; Sasabuchi, Y.; Takinami, M. The incidence and outcome of hyperlactatemia in patients admitted to the intensive care unit after elective surgery. Am. J. Surg. 2018, 216, 886–892. [Google Scholar] [CrossRef]
- Meregalli, A.; Oliveira, R.P.; Friedman, G. Occult hypoperfusion is associated with increased mortality in hemodynamically stable, high-risk, surgical patients. Crit. Care 2004, 8, R60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romano, D.; Deiner, S.; Cherukuri, A.; Boateng, B.; Shrivastava, R.; Mocco, J.; Hadjipanayis, C.; Yong, R.; Kellner, C.; Yaeger, K. Clinical impact of intraoperative hyperlactatemia during craniotomy. PLoS ONE 2019, 14, e0224016. [Google Scholar] [CrossRef] [PubMed]
- Maillet, J.-M.; Le Besnerais, P.; Cantoni, M.; Nataf, P.; Ruffenach, A.; Lessana, A.; Brodaty, D. Frequency, risk factors, and outcome of hyperlactatemia after cardiac surgery. Chest 2003, 123, 1361–1366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jansen, T.C.; van Bommel, J.; Schoonderbeek, F.J.; Sleeswijk Visser, S.J.; van der Klooster, J.M.; Lima, A.P.; Willemsen, S.P.; Bakker, J.; LACTATE Study Group. Early lactate-guided therapy in intensive care unit patients: A multicenter, open-label, randomized controlled trial. Am. J. Respir. Crit. Care Med. 2010, 182, 752–761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polonen, P.; Ruokonen, E.; Hippelainen, M.; Poyhonen, M.; Takala, J. A prospective, randomized study of goal-oriented hemodynamic therapy in cardiac surgical patients. Anesth. Analg. 2000, 90, 1052–1059. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Entire Population | Propensity Score Matched Population | |||||
|---|---|---|---|---|---|---|
| Normal (N = 1444) | Hyperlactatemia (N = 461) | p Value | Normal (N = 365) | Hyperlactatemia (N = 365) | SMD | |
| Peak cardiac troponin level, ng/L | 910 (±15,508) | 650 (±3646) | 0.72 | 327 (±2642) | 552 (±3177) | 7.7 |
| * Days to peak cardiac troponin | 0.53 (0.08–1.60) | 0.3 (0.06–1.53) | 0.13 | 0.20 (0.06–0.94) | 0.39 (0.07–1.71) | 10.2 |
| Male | 903 (62.5) | 297 (64.4) | 0.5 | 236 (64.7) | 234 (64.1) | 1.1 |
| Age | 63.7 (±12.8) | 60.4 (±13.1) | <0.001 | 61.6 (±13.5) | 61.9 (±13.3) | 1.7 |
| Diabetes | 846 (58.6) | 362 (78.5) | <0.001 | 260 (71.2) | 275 (75.3) | 9.3 |
| Hypertension | 904 (62.6) | 270 (58.6) | 0.14 | 230 (63.0) | 219 (60.0) | 6.2 |
| Current smoking | 102 (7.1) | 52 (11.3) | 0.01 | 34 (9.3) | 40 (11.0) | 5.4 |
| Current alcohol | 231 (16.0) | 91 (19.7) | 0.07 | 74 (20.3) | 77 (21.1) | 2 |
| Chronic kidney disease | 143 (9.9) | 45 (9.8) | 1 | 33 (9.0) | 33 (9.0) | <0.1 |
| Active cancer | 761 (52.7) | 198 (43.0) | <0.001 | 174 (47.7) | 178 (48.8) | 2.2 |
| Previous disease | ||||||
| History of ischemic heart disease | 257 (17.8) | 64 (13.9) | 0.06 | 53 (14.5) | 55 (15.1) | 1.5 |
| History of heart failure | 23 (1.6) | 7 (1.5) | 1 | 6 (1.6) | 6 (1.6) | <0.1 |
| History of stroke | 111 (7.7) | 30 (6.5) | 0.46 | 28 (7.7) | 26 (7.1) | 2.1 |
| History of arrhythmia | 108 (7.5) | 30 (6.5) | 0.55 | 24 (6.6) | 23 (6.3) | 1.1 |
| History of heart valve disease | 19 (1.3) | 3 (0.7) | 0.36 | 5 (1.4) | 3 (0.8) | 5.3 |
| Preoperative care | ||||||
| * Intensive care unit | 31 (2.1) | 58 (12.6) | <0.001 | 16 (4.4) | 32 (8.8) | 17.8 |
| ECMO | 0 (0.0) | 0 (0.0) | >0.99 | 0 (0.0) | 0 (0.0) | <0.1 |
| * Continuous renal replacement therapy | 2 (0.1) | 19 (4.1) | <0.001 | 2 (0.5) | 10 (2.7) | 17.3 |
| Ventilator | 5 (0.3) | 11 (2.4) | <0.001 | 4 (1.1) | 2 (0.5) | 6.1 |
| Operative variables | ||||||
| ESC/ESA surgical high risk | 394 (27.3) | 286 (62.0) | <0.001 | 183 (50.1) | 191 (52.3) | 4.4 |
| Emergency operation | 139 (9.6) | 117 (25.4) | <0.001 | 80 (21.9) | 84 (23.0) | 2.6 |
| General anesthesia | 1439 (99.7) | 455 (98.7) | 0.045 | 362 (99.2) | 359 (98.4) | 7.5 |
| Operation duration, hours | 3.53 (±1.88) | 5.02 (±2.58) | <0.001 | 4.33 (±2.38) | 4.55 (±2.44) | 9.2 |
| Continuous infusion of inotropics | 419 (29.0) | 267 (57.9) | <0.001 | 181 (49.6) | 184 (50.4) | 1.6 |
| Intraoperative RBC transfusion | 422 (29.2) | 224 (48.6) | <0.001 | 136 (37.3) | 149 (40.8) | 7.3 |
| Normal | Hyperlactatemia | Unadjusted OR/HR (95% CI) | p Value | * Adjusted OR/HR (95% CI) | p Value | |
|---|---|---|---|---|---|---|
| Entire population | (N = 1444) | (N = 461) | ||||
| MINS | 255 (17.7) | 174 (37.7) | 2.83 (2.24–3.56) | <0.001 | 2.03 (1.53–2.69) | <0.001 |
| 30-day mortality | 12 (0.8) | 22 (4.8) | 5.86 (2.90–11.84) | <0.001 | 2.61 (1.13–6.03) | 0.02 |
| Propensity-score-matched population | (N = 365) | (N = 365) | ||||
| MINS | 79 (21.6) | 116 (31.8) | 1.69 (1.21–2.36) | 0.002 | ||
| 30-day mortality | 4 (1.1) | 14 (3.8) | 3.55 (1.17–10.79) | 0.03 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.; Park, J.; Kwon, J.-H.; Kim, S.; Oh, A.R.; Jang, J.N.; Choi, J.-H.; Sung, J.; Yang, K.; Kim, K.; et al. Association between Intraoperative Hyperlactatemia and Myocardial Injury after Noncardiac Surgery. Diagnostics 2021, 11, 1656. https://doi.org/10.3390/diagnostics11091656
Kim J, Park J, Kwon J-H, Kim S, Oh AR, Jang JN, Choi J-H, Sung J, Yang K, Kim K, et al. Association between Intraoperative Hyperlactatemia and Myocardial Injury after Noncardiac Surgery. Diagnostics. 2021; 11(9):1656. https://doi.org/10.3390/diagnostics11091656
Chicago/Turabian StyleKim, Jeayoun, Jungchan Park, Ji-Hye Kwon, Sojin Kim, Ah Ran Oh, Jae Ni Jang, Jin-Ho Choi, Jidong Sung, Kwangmo Yang, Kyunga Kim, and et al. 2021. "Association between Intraoperative Hyperlactatemia and Myocardial Injury after Noncardiac Surgery" Diagnostics 11, no. 9: 1656. https://doi.org/10.3390/diagnostics11091656
APA StyleKim, J., Park, J., Kwon, J. -H., Kim, S., Oh, A. R., Jang, J. N., Choi, J. -H., Sung, J., Yang, K., Kim, K., Ahn, J., & Lee, S. -H. (2021). Association between Intraoperative Hyperlactatemia and Myocardial Injury after Noncardiac Surgery. Diagnostics, 11(9), 1656. https://doi.org/10.3390/diagnostics11091656