
Deep-Learning Segmentation of Epicardial Adipose Tissue Using Four-Chamber Cardiac Magnetic Resonance Imaging

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
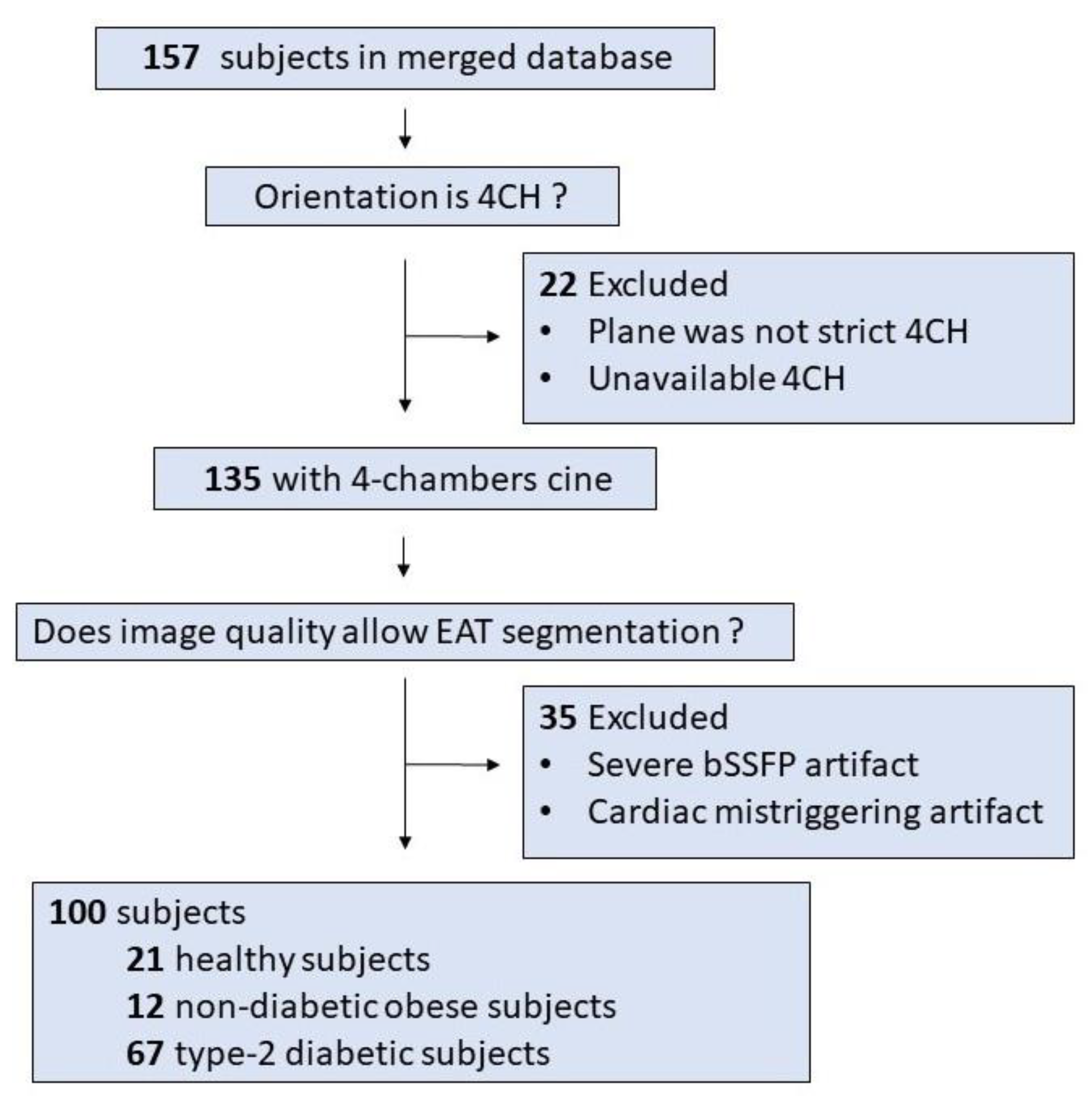
2.1. Study Population
2.2. MRI Acquisition
2.3. EAT Segmentation
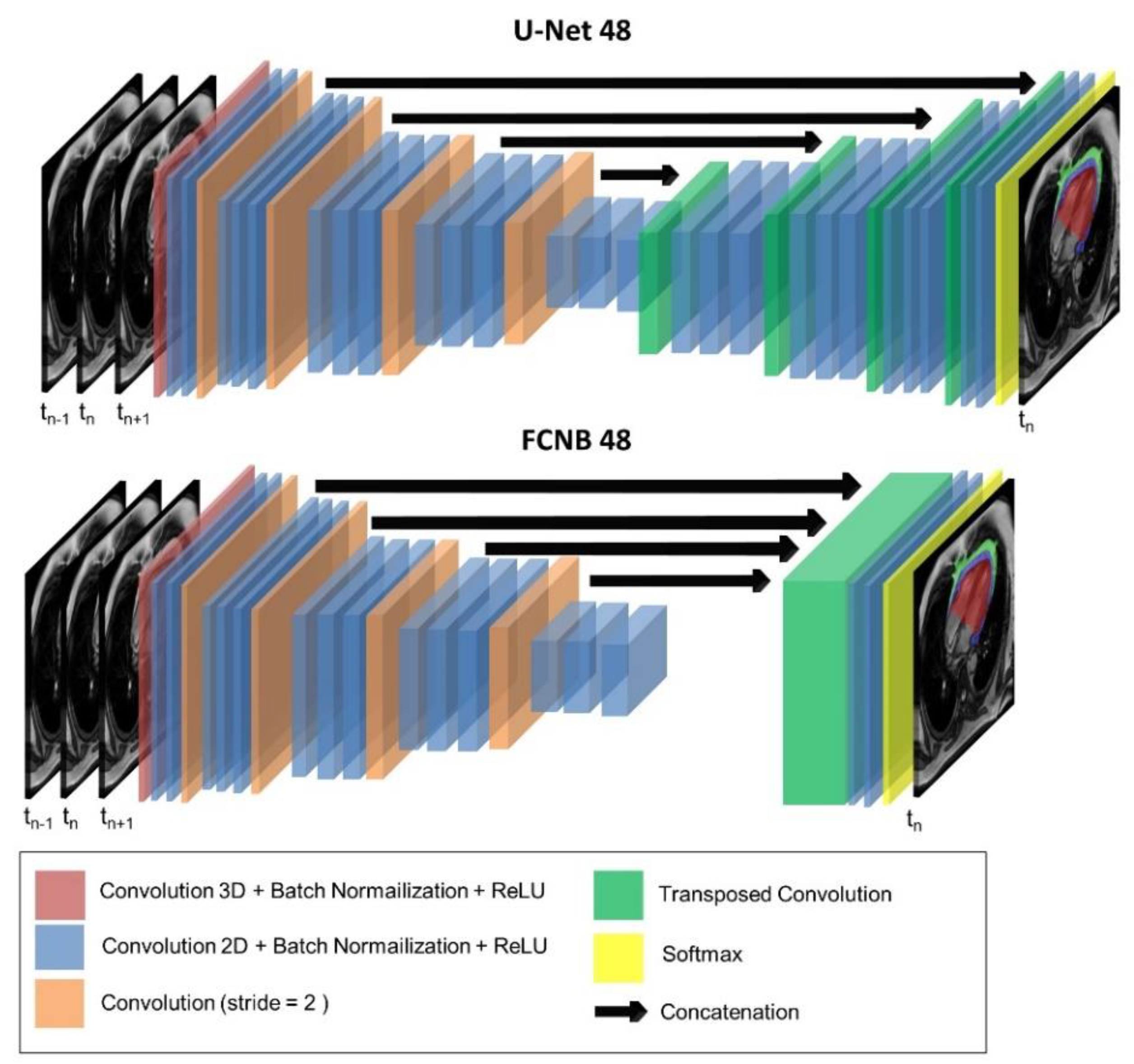
2.4. Network Architecture
2.5. Training
2.6. Evaluation Metrics
2.7. Statistical Analysis
3. Results
4. Discussion
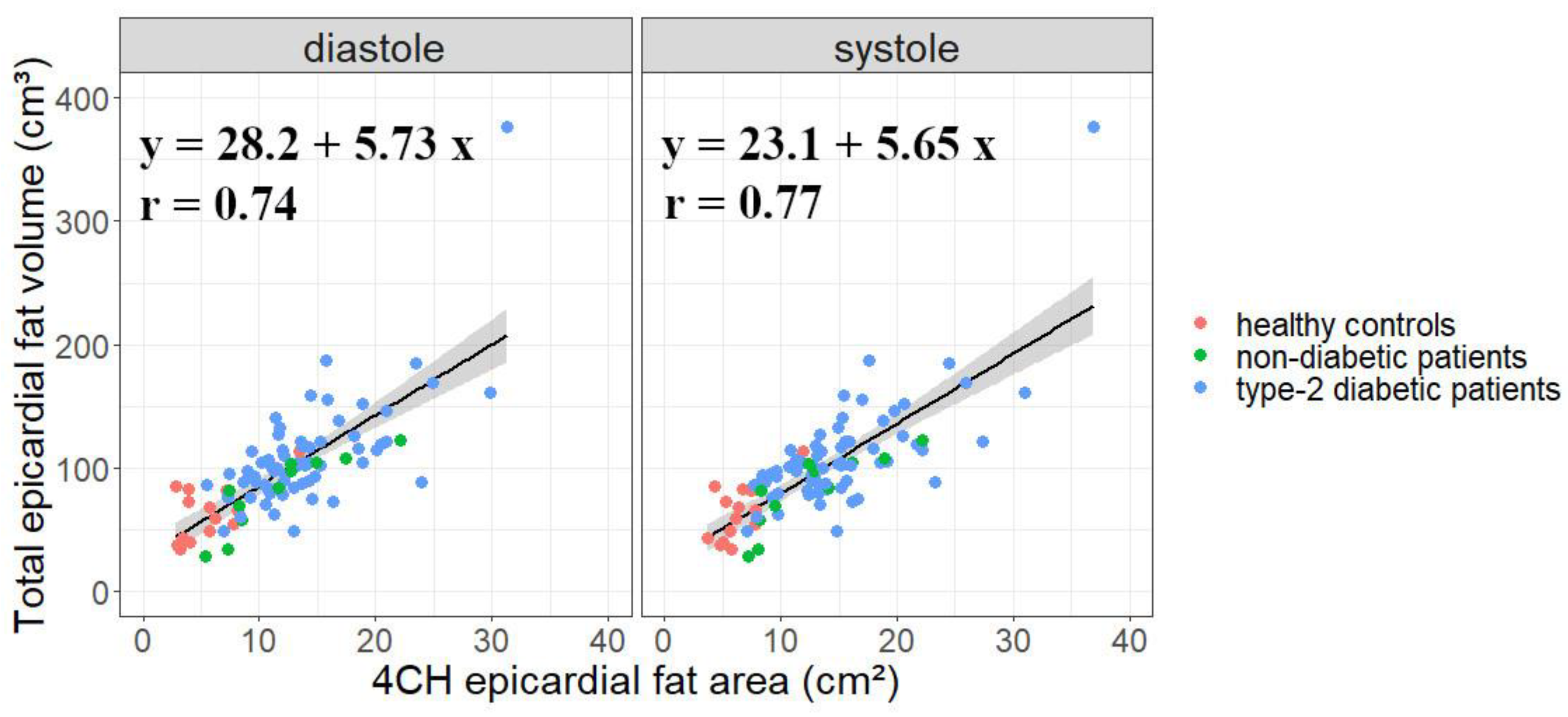
4.1. Four-Chamber-View Intrapericardial Fat Area Is a Relevant Measure of EAT
4.2. A Specific Database with Possible Extensions
4.3. Challenge of EAT Segmentation
4.4. Comparing FCNs Performances
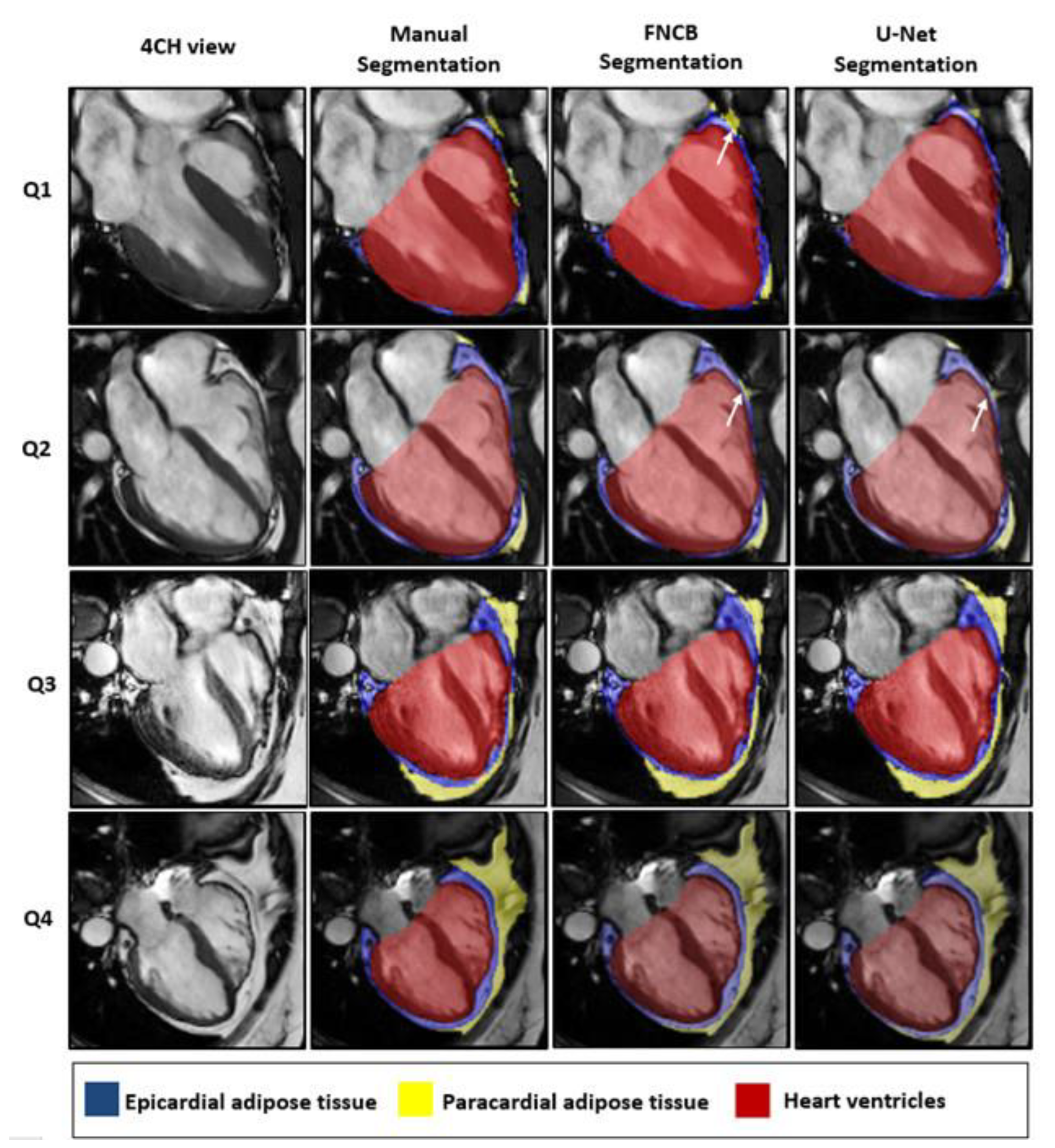
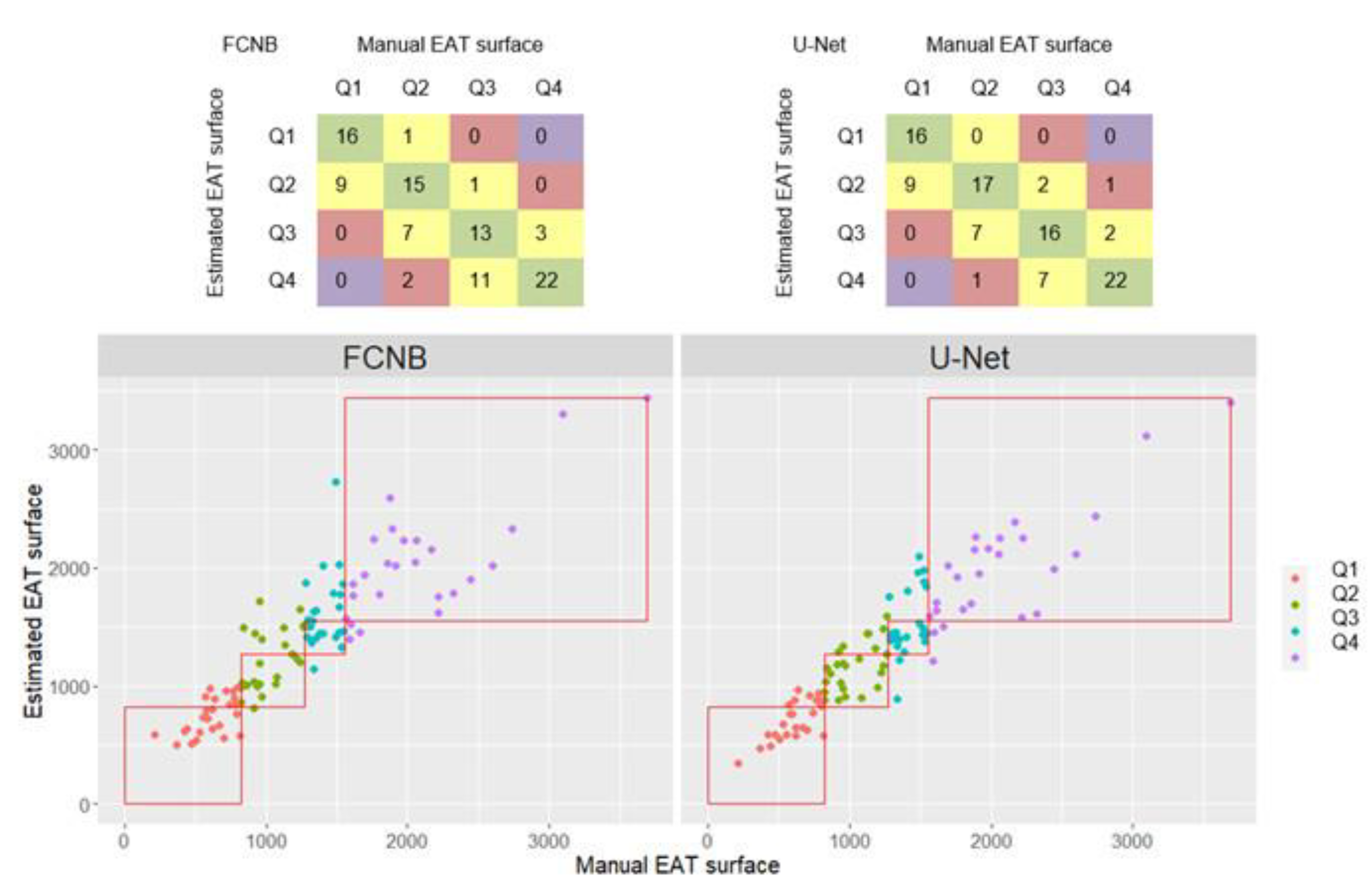
4.5. Performances across Quartiles
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A


References
- Gaborit, B.; Sengenes, C.; Ancel, P.; Jacquier, A.; Dutour, A. Role of Epicardial Adipose Tissue in Health and Disease: A Matter of Fat?. In Comprehensive Physiology; Terjung, R., Ed.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2017; pp. 1051–1082. ISBN 978-0-470-65071-4. [Google Scholar]
- Mahabadi, A.A.; Lehmann, N.; Kälsch, H.; Robens, T.; Bauer, M.; Dykun, I.; Budde, T.; Moebus, S.; Jöckel, K.-H.; Erbel, R.; et al. Association of Epicardial Adipose Tissue with Progression of Coronary Artery Calcification Is More Pronounced in the Early Phase of Atherosclerosis. JACC Cardiovasc. Imaging 2014, 7, 909–916. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ding, J.; Hsu, F.-C.; Harris, T.B.; Liu, Y.; Kritchevsky, S.B.; Szklo, M.; Ouyang, P.; Espeland, M.A.; Lohman, K.K.; Criqui, M.H.; et al. The Association of Pericardial Fat with Incident Coronary Heart Disease: The Multi-Ethnic Study of Atherosclerosis (MESA). Am. J. Clin. Nutr. 2009, 90, 499–504. [Google Scholar] [CrossRef]
- Iacobellis, G. Epicardial and Pericardial Fat: Close, but Very Different. Obesity 2009, 17, 625. [Google Scholar] [CrossRef]
- Nakanishi, K.; Fukuda, S.; Tanaka, A.; Otsuka, K.; Jissho, S.; Taguchi, H.; Yoshikawa, J.; Shimada, K. Persistent Epicardial Adipose Tissue Accumulation Is Associated with Coronary Plaque Vulnerability and Future Acute Coronary Syndrome in Non-Obese Subjects with Coronary Artery Disease. Atherosclerosis 2014, 237, 353–360. [Google Scholar] [CrossRef] [PubMed]
- Rosito, G.A.; Massaro, J.M.; Hoffmann, U.; Ruberg, F.L.; Mahabadi, A.A.; Vasan, R.S.; O’Donnell, C.J.; Fox, C.S. Pericardial Fat, Visceral Abdominal Fat, Cardiovascular Disease Risk Factors, and Vascular Calcification in a Community-Based Sample: The Framingham Heart Study. Circulation 2008, 117, 605–613. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dabbah, S.; Komarov, H.; Marmor, A.; Assy, N. Epicardial Fat, Rather than Pericardial Fat, Is Independently Associated with Diastolic Filling in Subjects without Apparent Heart Disease. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 877–882. [Google Scholar] [CrossRef] [PubMed]
- Antonopoulos, A.S.; Antoniades, C. The Role of Epicardial Adipose Tissue in Cardiac Biology: Classic Concepts and Emerging Roles. J. Physiol. (Lond.) 2017, 595, 3907–3917. [Google Scholar] [CrossRef] [PubMed]
- Iacobellis, G.; Secchi, F.; Capitanio, G.; Basilico, S.; Schiaffino, S.; Boveri, S.; Sardanelli, F.; Corsi Romanelli, M.M.; Malavazos, A.E. Epicardial Fat Inflammation in Severe COVID-19. Obesity 2020, 28, 2260–2262. [Google Scholar] [CrossRef]
- Grodecki, K.; Lin, A.; Razipour, A.; Cadet, S.; McElhinney, P.A.; Chan, C.; Pressman, B.D.; Julien, P.; Maurovich-Horvat, P.; Gaibazzi, N.; et al. Epicardial Adipose Tissue Is Associated with Extent of Pneumonia and Adverse Outcomes in Patients with COVID-19. Metabolism 2021, 115, 154436. [Google Scholar] [CrossRef]
- Mahabadi, A.A.; Rassaf, T. Thoracic Adipose Tissue Density as a Novel Marker of Increased Cardiovascular Risk. Atherosclerosis 2018, 279, 91–92. [Google Scholar] [CrossRef]
- Iacobellis, G.; Assael, F.; Ribaudo, M.C.; Zappaterreno, A.; Alessi, G.; Di Mario, U.; Leonetti, F. Epicardial Fat from Echocardiography: A New Method for Visceral Adipose Tissue Prediction. Obes. Res. 2003, 11, 304–310. [Google Scholar] [CrossRef]
- Dey, D.; Suzuki, Y.; Suzuki, S.; Ohba, M.; Slomka, P.J.; Polk, D.; Shaw, L.J.; Berman, D.S. Automated Quantitation of Pericardiac Fat from Noncontrast CT. Investig. Radiol. 2008, 43, 145–153. [Google Scholar] [CrossRef] [PubMed]
- Nichols, J.H.; Samy, B.; Nasir, K.; Fox, C.S.; Schulze, P.C.; Bamberg, F.; Hoffmann, U. Volumetric Measurement of Pericardial Adipose Tissue from Contrast-Enhanced Coronary Computed Tomography Angiography: A Reproducibility Study. J. Cardiovasc. Comput. Tomogr. 2008, 2, 288–295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Commandeur, F.; Goeller, M.; Razipour, A.; Cadet, S.; Hell, M.M.; Kwiecinski, J.; Chen, X.; Chang, H.-J.; Marwan, M.; Achenbach, S.; et al. Fully Automated CT Quantification of Epicardial Adipose Tissue by Deep Learning: A Multicenter Study. Radiol. Artif. Intell. 2019, 1, e190045. [Google Scholar] [CrossRef]
- Kramer, C.M.; Barkhausen, J.; Bucciarelli-Ducci, C.; Flamm, S.D.; Kim, R.J.; Nagel, E. Standardized Cardiovascular Magnetic Resonance Imaging (CMR) Protocols: 2020 Update. J. Cardiovasc. Magn. Reson. 2020, 22, 17. [Google Scholar] [CrossRef] [PubMed]
- Flüchter, S.; Haghi, D.; Dinter, D.; Heberlein, W.; Kühl, H.P.; Neff, W.; Sueselbeck, T.; Borggrefe, M.; Papavassiliu, T. Volumetric Assessment of Epicardial Adipose Tissue with Cardiovascular Magnetic Resonance Imaging*. Obesity 2007, 15, 870–878. [Google Scholar] [CrossRef] [PubMed]
- Homsi, R.; Meier-Schroers, M.; Gieseke, J.; Dabir, D.; Luetkens, J.A.; Kuetting, D.L.; Naehle, C.P.; Marx, C.; Schild, H.H.; Thomas, D.K.; et al. 3D-Dixon MRI Based Volumetry of Peri- and Epicardial Fat. Int. J. Cardiovasc. Imaging 2016, 32, 291–299. [Google Scholar] [CrossRef]
- Henningsson, M.; Brundin, M.; Scheffel, T.; Edin, C.; Viola, F.; Carlhäll, C.-J. Quantification of Epicardial Fat Using 3D Cine Dixon MRI. BMC Med. Imaging 2020, 20, 80. [Google Scholar] [CrossRef]
- Gaborit, B.; Kober, F.; Jacquier, A.; Moro, P.J.; Cuisset, T.; Boullu, S.; Dadoun, F.; Alessi, M.-C.; Morange, P.; Clément, K.; et al. Assessment of Epicardial Fat Volume and Myocardial Triglyceride Content in Severely Obese Subjects: Relationship to Metabolic Profile, Cardiac Function and Visceral Fat. Int. J. Obes. (Lond.) 2012, 36, 422–430. [Google Scholar] [CrossRef] [Green Version]
- Chetrit, M.; Xu, B.; Kwon, D.H.; Ramchand, J.; Rodriguez, R.E.; Tan, C.D.; Jellis, C.L.; Johnston, D.R.; Renapurkar, R.D.; Cremer, P.C.; et al. Imaging-Guided Therapies for Pericardial Diseases. JACC Cardiovasc. Imaging 2020, 13, 1422–1437. [Google Scholar] [CrossRef]
- Rado, S.D.; Lorbeer, R.; Gatidis, S.; Machann, J.; Storz, C.; Nikolaou, K.; Rathmann, W.; Hoffmann, U.; Peters, A.; Bamberg, F.; et al. MRI-Based Assessment and Characterization of Epicardial and Paracardial Fat Depots in the Context of Impaired Glucose Metabolism and Subclinical Left-Ventricular Alterations. BJR 2019, 92, 20180562. [Google Scholar] [CrossRef] [PubMed]
- Bard, A.; Raisi-Estabragh, Z.; Ardissino, M.; Lee, A.M.; Pugliese, F.; Dey, D.; Sarkar, S.; Munroe, P.B.; Neubauer, S.; Harvey, N.C.; et al. Automated Quality-Controlled Cardiovascular Magnetic Resonance Pericardial Fat Quantification Using a Convolutional Neural Network in the UK Biobank. Front. Cardiovasc. Med. 2021, 8, 677574. [Google Scholar] [CrossRef] [PubMed]
- Nyman, K.; Granér, M.; Pentikäinen, M.O.; Lundbom, J.; Hakkarainen, A.; Sirén, R.; Nieminen, M.S.; Taskinen, M.-R.; Lundbom, N.; Lauerma, K. Cardiac Steatosis and Left Ventricular Function in Men with Metabolic Syndrome. J. Cardiovasc. Magn. Reson. 2013, 15, 103. [Google Scholar] [CrossRef] [Green Version]
- Granér, M.; Siren, R.; Nyman, K.; Lundbom, J.; Hakkarainen, A.; Pentikäinen, M.O.; Lauerma, K.; Lundbom, N.; Adiels, M.; Nieminen, M.S.; et al. Cardiac Steatosis Associates with Visceral Obesity in Nondiabetic Obese Men. J. Clin. Endocrinol. Metab. 2013, 98, 1189–1197. [Google Scholar] [CrossRef] [Green Version]
- Nakanishi, K.; Fukuda, S.; Tanaka, A.; Otsuka, K.; Taguchi, H.; Shimada, K. Relationships Between Periventricular Epicardial Adipose Tissue Accumulation, Coronary Microcirculation, and Left Ventricular Diastolic Dysfunction. Can. J. Cardiol. 2017, 33, 1489–1497. [Google Scholar] [CrossRef] [PubMed]
- Perseghin, G.; Lattuada, G.; De Cobelli, F.; Esposito, A.; Belloni, E.; Ntali, G.; Ragogna, F.; Canu, T.; Scifo, P.; Del Maschio, A.; et al. Increased Mediastinal Fat and Impaired Left Ventricular Energy Metabolism in Young Men with Newly Found Fatty Liver. Hepatology 2007, 47, 51–58. [Google Scholar] [CrossRef]
- Gaborit, B.; Kober, F.; Jacquier, A.; Moro, P.J.; Flavian, A.; Quilici, J.; Cuisset, T.; Simeoni, U.; Cozzone, P.; Alessi, M.-C.; et al. Epicardial Fat Volume Is Associated with Coronary Microvascular Response in Healthy Subjects: A Pilot Study. Obesity 2012, 20, 1200–1205. [Google Scholar] [CrossRef]
- Dutour, A.; Abdesselam, I.; Ancel, P.; Kober, F.; Mrad, G.; Darmon, P.; Ronsin, O.; Pradel, V.; Lesavre, N.; Martin, J.C.; et al. Exenatide Decreases Liver Fat Content and Epicardial Adipose Tissue in Patients with Obesity and Type 2 Diabetes: A Prospective Randomized Clinical Trial Using Magnetic Resonance Imaging and Spectroscopy. Diabetes Obes. Metab. 2016, 18, 882–891. [Google Scholar] [CrossRef]
- Gaborit, B.; Jacquier, A.; Kober, F.; Abdesselam, I.; Cuisset, T.; Boullu-Ciocca, S.; Emungania, O.; Alessi, M.-C.; Clément, K.; Bernard, M.; et al. Effects of Bariatric Surgery on Cardiac Ectopic Fat. J. Am. Coll. Cardiol. 2012, 60, 1381–1389. [Google Scholar] [CrossRef]
- Gaborit, B.; Ancel, P.; Abdullah, A.E.; Maurice, F.; Abdesselam, I.; Calen, A.; Soghomonian, A.; Houssays, M.; Varlet, I.; Eisinger, M.; et al. Effect of Empagliflozin on Ectopic Fat Stores and Myocardial Energetics in Type 2 Diabetes: The EMPACEF Study. Cardiovasc. Diabetol. 2021, 20, 57. [Google Scholar] [CrossRef]
- Tustison, N.J.; Avants, B.B.; Cook, P.A.; Zheng, Y.; Egan, A.; Yushkevich, P.A.; Gee, J.C. N4ITK: Improved N3 Bias Correction. IEEE Trans. Med. Imaging 2010, 29, 1310–1320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCarthy, Paul FSLeyes v.0.31. Available online: https://doi.org/10.5281/zenodo.3403671 (accessed on 2 October 2020).
- Ogier, A.; Sdika, M.; Foure, A.; Le Troter, A.; Bendahan, D. Individual Muscle Segmentation in MR Images: A 3D Propagation through 2D Non-Linear Registration Approaches. In Proceedings of the 2017 39th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Jeju, Korea, 11–15 July 2017; IEEE: Seogwipo, Korea, 2017; pp. 317–320. [Google Scholar]
- Ronneberger, O.; Fischer, P.; Brox, T. U-Net: Convolutional Networks for Biomedical Image Segmentation. In Medical Image Computing and Computer-Assisted Intervention–MICCAI 2015; Navab, N., Hornegger, J., Wells, W.M., Frangi, A.F., Eds.; Lecture Notes in Computer Science; Springer International Publishing: Cham, Switzerland, 2015; Volume 9351, pp. 234–241. ISBN 978-3-319-24573-7. [Google Scholar]
- Bai, W.; Sinclair, M.; Tarroni, G.; Oktay, O.; Rajchl, M.; Vaillant, G.; Lee, A.M.; Aung, N.; Lukaschuk, E.; Sanghvi, M.M.; et al. Automated Cardiovascular Magnetic Resonance Image Analysis with Fully Convolutional Networks. J. Cardiovasc Magn. Reson. 2018, 20, 65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, Q.; Delingette, H.; Duchateau, N.; Ayache, N. 3-D Consistent and Robust Segmentation of Cardiac Images by Deep Learning with Spatial Propagation. IEEE Trans. Med. Imaging 2018, 37, 2137–2148. [Google Scholar] [CrossRef]
- Baumgartner, C.F.; Koch, L.M.; Pollefeys, M.; Konukoglu, E. An Exploration of 2D and 3D Deep Learning Techniques for Cardiac MR Image Segmentation. In Statistical Atlases and Computational Models of the Heart. ACDC and MMWHS Challenges; Pop, M., Sermesant, M., Jodoin, P.-M., Lalande, A., Zhuang, X., Yang, G., Young, A., Bernard, O., Eds.; Lecture Notes in Computer Science; Springer International Publishing: Cham, Switzerland, 2018; Volume 10663, pp. 111–119. ISBN 978-3-319-75540-3. [Google Scholar]
- Isensee, F.; Jaeger, P.F.; Full, P.M.; Wolf, I.; Engelhardt, S.; Maier-Hein, K.H. Automatic Cardiac Disease Assessment on Cine-MRI via Time-Series Segmentation and Domain Specific Features. In Statistical Atlases and Computational Models of the Heart. ACDC and MMWHS Challenges; Pop, M., Sermesant, M., Jodoin, P.-M., Lalande, A., Zhuang, X., Yang, G., Young, A., Bernard, O., Eds.; Lecture Notes in Computer Science; Springer International Publishing: Cham, Switzerland, 2018; Volume 10663, pp. 120–129. ISBN 978-3-319-75540-3. [Google Scholar]
- Sudlow, C.; Gallacher, J.; Allen, N.; Beral, V.; Burton, P.; Danesh, J.; Downey, P.; Elliott, P.; Green, J.; Landray, M.; et al. UK Biobank: An Open Access Resource for Identifying the Causes of a Wide Range of Complex Diseases of Middle and Old Age. PLoS Med. 2015, 12, e1001779. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kingma, D.P.; Ba, J. Adam: A Method for Stochastic Optimization. arXiv 2017, arXiv:1412.6980. [Google Scholar]
- Bai, W. Ukbb_cardiac. Available online: https://github.com/baiwenjia/ukbb_cardiac (accessed on 8 October 2020).
- R Core Team R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020.
- Mahabadi, A.A.; Berg, M.H.; Lehmann, N.; Kälsch, H.; Bauer, M.; Kara, K.; Dragano, N.; Moebus, S.; Jöckel, K.-H.; Erbel, R.; et al. Association of Epicardial Fat with Cardiovascular Risk Factors and Incident Myocardial Infarction in the General Population. J. Am. Coll. Cardiol. 2013, 61, 1388–1395. [Google Scholar] [CrossRef] [Green Version]
- Foldyna, B.; Zeleznik, R.; Eslami, P.; Mayrhofer, T.; Ferencik, M.; Bittner, D.O.; Meyersohn, N.M.; Puchner, S.B.; Emami, H.; Aerts, H.J.W.L.; et al. Epicardial Adipose Tissue in Patients with Stable Chest Pain. JACC Cardiovasc. Imaging 2020, 13, 2273–2275. [Google Scholar] [CrossRef]
- Chaitanya, K.; Karani, N.; Baumgartner, C.F.; Becker, A.; Donati, O.; Konukoglu, E. Semi-Supervised and Task-Driven Data Augmentation. In Information Processing in Medical Imaging; Chung, A.C.S., Gee, J.C., Yushkevich, P.A., Bao, S., Eds.; Lecture Notes in Computer Science; Springer International Publishing: Cham, Switzerland, 2019; Volume 11492, pp. 29–41. ISBN 978-3-030-20350-4. [Google Scholar]
- Bull, R.K.; Edwards, P.D.; Dixon, A.K. CT Dimensions of the Normal Pericardium. BJR 1998, 71, 923–925. [Google Scholar] [CrossRef]
- Bogaert, J.; Francone, M. Cardiovascular Magnetic Resonance in Pericardial Diseases. J. Cardiovasc. Magn. Reson. 2009, 11, 14. [Google Scholar] [CrossRef] [Green Version]
- Poudel, R.P.K.; Lamata, P.; Montana, G. Recurrent Fully Convolutional Neural Networks for Multi-Slice MRI Cardiac Segmentation. In Reconstruction, Segmentation, and Analysis of Medical Images; Zuluaga, M.A., Bhatia, K., Kainz, B., Moghari, M.H., Pace, D.F., Eds.; Lecture Notes in Computer Science; Springer International Publishing: Cham, Switzerland, 2017; Volume 10129, pp. 83–94. ISBN 978-3-319-52279-1. [Google Scholar]
- Huttenlocher, D.P.; Klanderman, G.A.; Rucklidge, W.J. Comparing Images Using the Hausdorff Distance. IEEE Trans. Pattern Anal. Machine Intell. 1993, 15, 850–863. [Google Scholar] [CrossRef] [Green Version]
- Cristobal-Huerta, A.; Torrado-Carvajal, A.; Malpica, N.; Luaces, M.; Hernandez-Tamames, J.A. Automated Quantification of Epicardial Adipose Tissue in Cardiac Magnetic Resonance Imaging. In Proceedings of the 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milan, Italy, 25–29 August 2015; pp. 7308–7311. [Google Scholar]
- Fulton, M.R.; Givan, A.H.; Fernandez-del-Valle, M.; Klingensmith, J.D. Segmentation of Epicardial Adipose Tissue in Cardiac MRI Using Deep Learning. In Proceedings of the Medical Imaging 2020: Biomedical Applications in Molecular, Structural, and Functional Imaging; Gimi, B.S., Krol, A., Eds.; SPIE: Houston, TX, USA, 2020; p. 25. [Google Scholar]
- Daudé, P. Fsleyes-Plugin-Epicseg. Available online: https://github.com/pdaude/fsleyes-plugin-epicseg (accessed on 20 July 2021).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Healthy | Non-Diabetic Obese | Type-2-Diabetic | ||
|---|---|---|---|---|
| Clinical characteristics | ||||
| Number of participants | 21 | 12 | 67 | |
| Age, years | 25 ± 10 | 41 ± 13 | 53 ± 10 | |
| Gender: female, n (%) | 11 (52) | 10 (83) | 41 (61) | |
| BMI, kg/m² | 21.9 ± 2.6 | 40.8 ± 5.9 | 35.6 ± 6.8 | |
| T2D | ||||
| Duration of diabetes, years | 8 ± 6 | |||
| Cardiovascular risk factors, n (%) | ||||
| Hypertension | 6 (29) | 1 (8) | 32 (48) | |
| Dyslipidemia | 2 (10) | 1 (8) | 36 (54) | |
| Current Smoker, n (%) | 3 (14) | 1 (8) | 8 (12) | |
| DSC | MSD (mm) | RSE (%) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Intra | Inter | U-Net | FCNB | Intra | Inter | U-Net | FCNB | Intra | Inter | U-Net | FCNB | |
| Paracardial Fat (PAT) | 0.85 (0.06) | 0.78 (0.09) | 0.80 (0.08) | 0.78 (0.10) | 1.15 (0.63) | 2.08 (1.49) | 2.38 (1.78) | 2.29 (1.47) | 11.78 (8.09) | 20.43 (18.77) | 14.29 (10.44) | 17.43 (17.50) |
| Epicardial Fat (EAT) | 0.83 (0.07) | 0.76 (0.10) | 0.77 (0.07) | 0.76 (0.07) | 1.53 (1.32) | 2.65 (2.98) | 1.71 (1.06) | 2.06 (1.96) | 13.02 (14.59) | 17.67 (15.07) | 20.33 (15.70) | 20.97 (15.66) |
| Pericardial Fat (EAT + PAT) | 0.90 (0.04) | 0.88 (0.05) | 0.88 (0.06) | 0.88 (0.06) | 1.12 (0.66) | 1.55 (0.07) | 1.36 (0.90) | 1.60 (1.28) | 6.92 (7.16) | 9.20 (6.80) | 7.36 (9.40) | 8.92 (12.97) |
| Heart ventricles (HV) | 0.98 (0.01) | 0.96 (0.02) | 0.97 (0.02) | 0.96 (0.03) | 0.96 (0.5) | 1.88 (2.24) | 1.33 (0.79) | 1.42 (0.89) | 2.33 (2.20) | 3.69 (3.18) | 3.88 (4.46) | 4.22 (5.80) |
| Q1 | DSC | MSD (mm) | RSE (%) | |||
| U-Net | FCNB | U-Net | FCNB | U-Net | FCNB | |
| Paracardial Fat (PAT) | 0.55 | 0.53 | 5.82 | 5.69 | 36.21 | 38.54 |
| Epicardial Fat (EAT) | 0.69 | 0.67 | 2.14 | 2.21 | 22.15 | 27.98 |
| Pericardial Fat (EAT + PAT) | 0.78 | 0.77 | 1.60 | 1.78 | 2.08 | 2.65 |
| Heart ventricles (HV) | 0.97 | 0.97 | 1.12 | 1.35 | 12.59 | 16.19 |
| Q2 | DSC | MSD (mm) | RSE (%) | |||
| U-Net | FCNB | U-Net | FCNB | U-Net | FCNB | |
| Paracardial Fat (PAT) | 0.76 | 0.75 | 2.68 | 2.82 | 17.29 | 20.83 |
| Epicardial Fat (EAT) | 0.76 | 0.74 | 1.22 | 1.53 | 17.85 | 21.91 |
| Pericardial Fat (EAT + PAT) | 0.87 | 0.87 | 1.16 | 1.35 | 7.55 | 8.60 |
| Heart ventricles (HV) | 0.97 | 0.97 | 1.11 | 1.65 | 2.57 | 3.04 |
| Q3 | DSC | MSD (mm) | RSE (%) | |||
| U-Net | FCNB | U-Net | FCNB | U-Net | FCNB | |
| Paracardial Fat (PAT) | 0.82 | 0.82 | 2.26 | 1.99 | 12.72 | 12.14 |
| Epicardial Fat (EAT) | 0.80 | 0.79 | 1.30 | 1.47 | 13.49 | 15.87 |
| Pericardial Fat (EAT + PAT) | 0.90 | 0.90 | 1.37 | 1.43 | 5.86 | 5.28 |
| Heart ventricles (HV) | 0.97 | 0.97 | 1.08 | 1.50 | 2.54 | 3.07 |
| Q4 | DSC | MSD (mm) | RSE (%) | |||
| U-Net | FCNB | U-Net | FCNB | U-Net | FCNB | |
| Paracardial Fat (PAT) | 0.80 | 0.78 | 2.46 | 3.12 | 13.65 | 16.72 |
| Epicardial Fat (EAT) | 0.83 | 0.79 | 1.40 | 2.06 | 11.72 | 15.60 |
| Pericardial Fat (EAT + PAT) | 0.91 | 0.90 | 1.40 | 1.84 | 5.64 | 6.43 |
| Heart ventricles (HV) | 0.97 | 0.96 | 1.31 | 2.60 | 3.20 | 4.52 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Daudé, P.; Ancel, P.; Confort Gouny, S.; Jacquier, A.; Kober, F.; Dutour, A.; Bernard, M.; Gaborit, B.; Rapacchi, S. Deep-Learning Segmentation of Epicardial Adipose Tissue Using Four-Chamber Cardiac Magnetic Resonance Imaging. Diagnostics 2022, 12, 126. https://doi.org/10.3390/diagnostics12010126
Daudé P, Ancel P, Confort Gouny S, Jacquier A, Kober F, Dutour A, Bernard M, Gaborit B, Rapacchi S. Deep-Learning Segmentation of Epicardial Adipose Tissue Using Four-Chamber Cardiac Magnetic Resonance Imaging. Diagnostics. 2022; 12(1):126. https://doi.org/10.3390/diagnostics12010126
Chicago/Turabian StyleDaudé, Pierre, Patricia Ancel, Sylviane Confort Gouny, Alexis Jacquier, Frank Kober, Anne Dutour, Monique Bernard, Bénédicte Gaborit, and Stanislas Rapacchi. 2022. "Deep-Learning Segmentation of Epicardial Adipose Tissue Using Four-Chamber Cardiac Magnetic Resonance Imaging" Diagnostics 12, no. 1: 126. https://doi.org/10.3390/diagnostics12010126
APA StyleDaudé, P., Ancel, P., Confort Gouny, S., Jacquier, A., Kober, F., Dutour, A., Bernard, M., Gaborit, B., & Rapacchi, S. (2022). Deep-Learning Segmentation of Epicardial Adipose Tissue Using Four-Chamber Cardiac Magnetic Resonance Imaging. Diagnostics, 12(1), 126. https://doi.org/10.3390/diagnostics12010126