
Significance of Pelvic Fluid Observed during Ovarian Cancer Screening with Transvaginal Sonogram

 , ,
, ,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Interpretation of TVS Screening Results
2.3. Pelvic Free Fluid Identification
2.4. Statistical Analysis
2.5. Fluid Duration Analysis
3. Results
3.1. Demographics
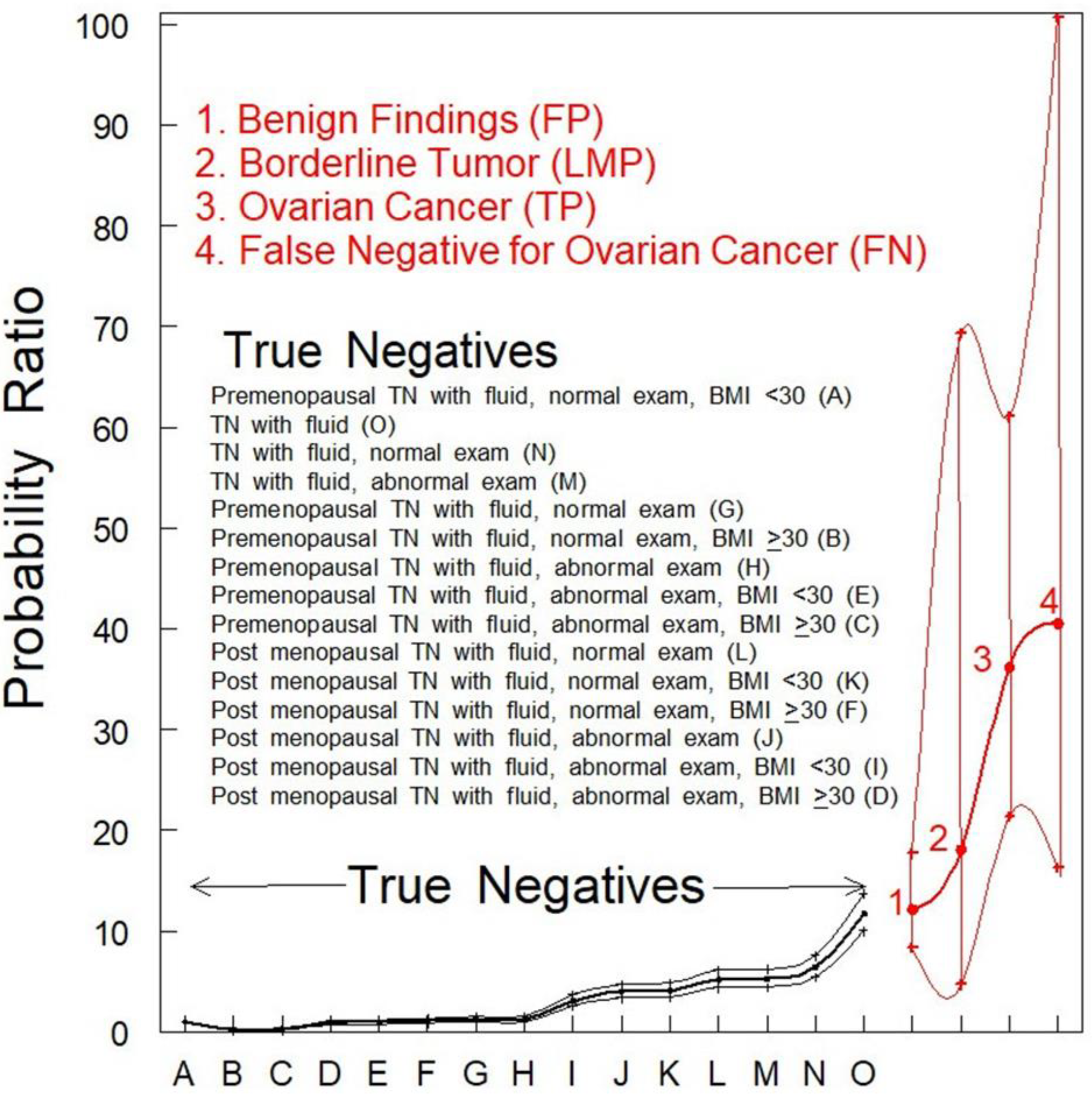
3.2. Probability of Identifying Pelvic Fluid in Each Group
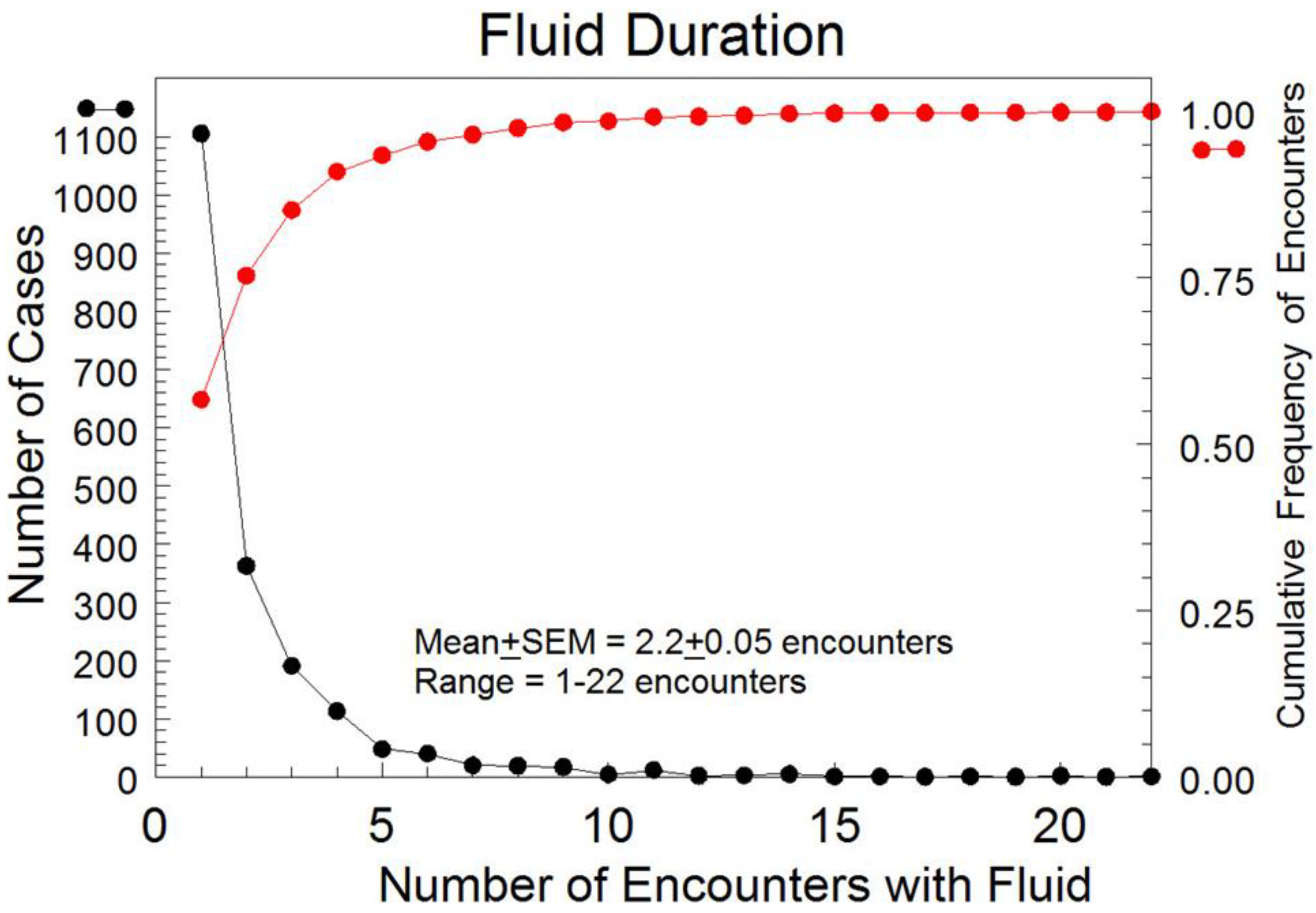
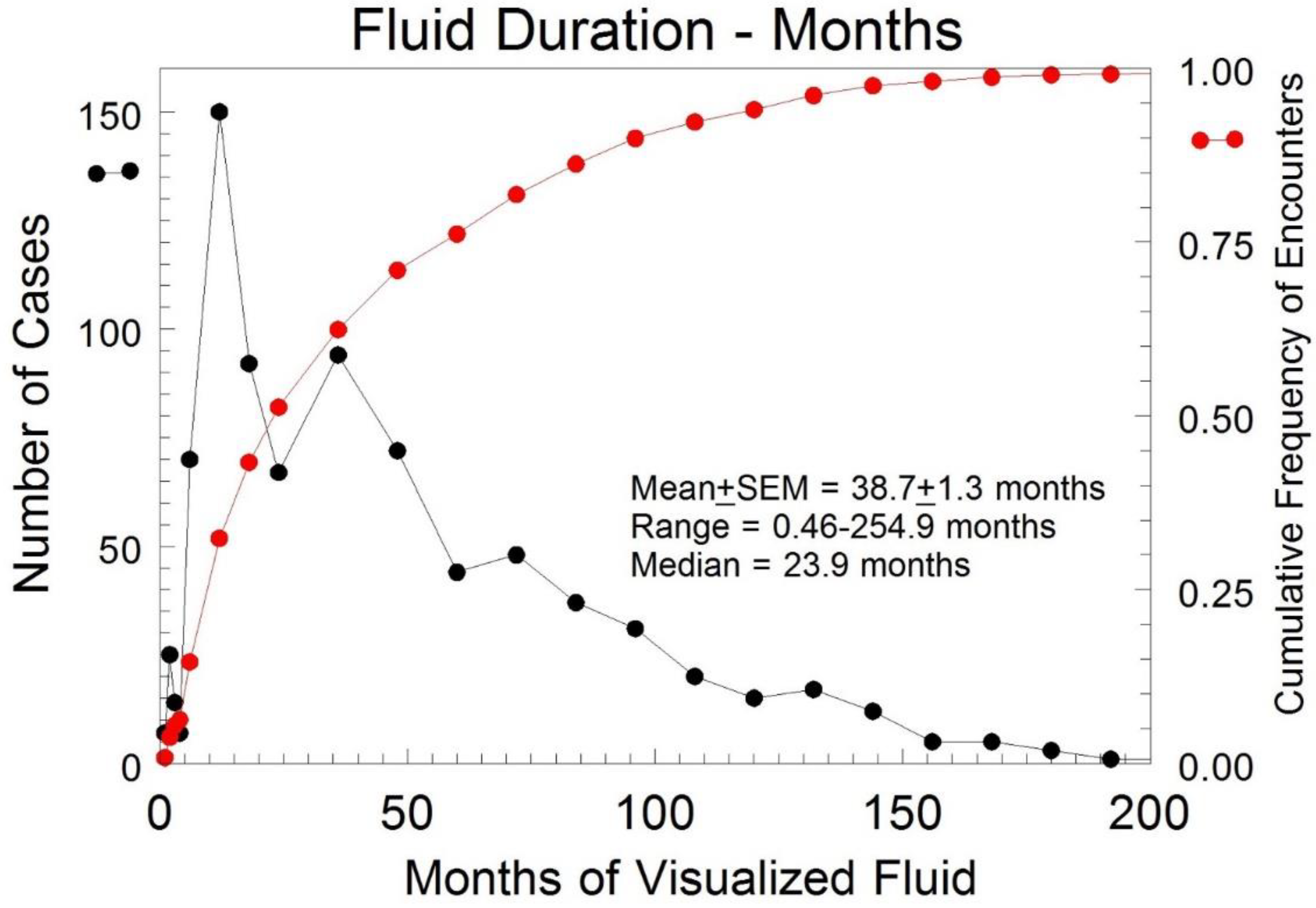
3.3. Duration of Fluid Identified in TN Subjects
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Howlader, N.; Noone, A.M.; Krapcho, M.; Garshell, J.; Miller, D.; Altekruse, S.F.; Kosary, C.L.; Yu, M.; Ruhl, J.; Tatalovich, Z.; et al. Seer Cancer Statistics Review; National Cancer Institute: Bethesda, MD, USA, 2015; pp. 1975–2016. Available online: https://seer.cancer.gov/csr/1975_2016/ (accessed on 14 December 2021).
- Pavlik, E.J.; van Nagell, J.R., Jr. Early detection of ovarian tumors using ultrasound. Womens Health Lond 2013, 9, 39–55. [Google Scholar] [CrossRef] [Green Version]
- Committee on the State of the Science in Ovarian Cancer Research; Board on Health Care Services; Institute of Medicine; National Academies of Sciences, Engineering, and Medicine. Ovarian Cancers: Evolving Paradigms in Research and Care; National Academies Press: Washington, DC, USA, 2016. Available online: https://www.ncbi.nlm.nih.gov/books/NBK367618/ (accessed on 14 December 2021).
- Kurman, R.J.; Shih, I.-M. Molecular pathogenesis and extraovarian origin of epithelial ovarian cancer—Shifting the paradigm. Hum. Pathol. 2001, 42, 918–931. [Google Scholar] [CrossRef] [Green Version]
- Shih, I.-M.; Kurman, R.J. Ovarian tumorigenesis: A proposed model based on morphological and molecular genetic analysis. Am. J. Pathol. 2004, 164, 1511–1518. [Google Scholar] [CrossRef]
- Crum, C.P. Intercepting pelvic cancer in the distal fallopian tube: Theories and realities. Mol. Oncol. 2009, 3, 165–170. [Google Scholar] [CrossRef] [PubMed]
- Gershenson, D.M.; Tortolero-Luna, G.; Malpica, A.; Baker, V.V.; Whittaker, L.; Johnson, E.; Follen, M.M. Ovarian intraepithelial neoplasia and ovarian cancer. Obstet. Gynecol. Clin. N. Am. 1996, 23, 475–543. [Google Scholar]
- Kindelberger, D.W.; Lee, Y.; Miron, A.; Hirsch, M.S.; Feltmate, C.; Medeiros, F.; Callahan, M.J.; Garner, E.O.; Gordon, R.W.; Birch, C.; et al. Intraepithelial carcinoma of the fimbria and pelvic serous carcinoma: Evidence for a causal relationship. Am. J. Surg. Pathol. 2007, 31, 161–169. [Google Scholar] [CrossRef] [Green Version]
- Crum, C.P.; McKeon, F.D.; Xian, W. The oviduct and ovarian cancer: Causality, clinical implications, and “targeted prevention”. Clin. Obstet. Gynecol. 2012, 55, 24–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soong, T.R.; Howitt, B.E.; Horowitz, N.; Nucci, M.R.; Crum, C.P. The fallopian tube, “precursor escape” and narrowing the knowledge gap to the origins of high-grade serous carcinoma. Gynecol. Oncol. 2019, 152, 426–433. [Google Scholar] [CrossRef]
- Menon, U.; Karpinskyjj, C.; Gentry-Maharaj, A. Ovarian cancer prevention and screening. Obstet. Gynecol. 2018, 131, 909–927. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnes, B.M.; Nelson, L.; Tighe, A.; Burghel, G.J.; Lin, H.-I.; Desai, S.; McGrail, J.C.; Morgan, R.D.; Taylor, S.S. Distinct transcriptional programs stratify ovarian cancer cell lines into the five major histological subtypes. Genome Med. 2021, 13, 140. [Google Scholar] [CrossRef]
- Nesic, K.; Kondrashova, O.; Hurley, R.M.; McGehee, C.D.; Vandenberg, V.J.; Ho, G.-Y.; Lieschke, E.; Dall, G.; Bound, N.; Shield-Artin, K.; et al. Acquired RAD51C Promoter Methylation Loss Causes PARP Inhibitor Resistance in High-Grade Serous Ovarian Carcinoma. Cancer Res. 2021, 81, 4709–4722. [Google Scholar] [CrossRef] [PubMed]
- Konstantinopoulos, P.A.; Cannistra, S.A. Immune Checkpoint Inhibitors in Ovarian Cancer: Can We Bridge the Gap Between IMagynation and Reality? J. Clin. Oncol. 2021, 39, 1833–1838. [Google Scholar] [CrossRef] [PubMed]
- Porter, R.L.; Matulonis, U.A. Checkpoint Blockade: Not Yet NINJA Status in Ovarian Cancer. J. Clin. Oncol. 2021, 39, 3651–3655. [Google Scholar] [CrossRef] [PubMed]
- Gu, S.; Lheureux, S.; Sayad, A.; Cybulska, P.; Hogen, L.T.; Vyarvelska, I.; Tu, D.; Parulekar, W.R.; Nankivell, M.; Kehoe, S.; et al. Computational modeling of ovarian cancer dynamics suggests optimal strategies for therapy and screening. Proc. Natl. Acad. Sci. USA 2021, 118, e2026663118. [Google Scholar] [CrossRef]
- Moorthy, R.S. Transvaginal Sonography. Med. J. Armed Forces India 2000, 56, 181–183. [Google Scholar] [CrossRef] [Green Version]
- van Nagell, J.; Burgess, B.; Miller, R.; Baldwin, L.; DeSimone, C.; Ueland, F.; Huang, B.; Chen, Q.; Kryscio, R.J.; Pavlik, E.J. Survival of Women With Type I and II Epithelial Ovarian Cancer Detected by Ultrasound Screening. Obstet. Gynecol. 2018, 132, 1091–1100. [Google Scholar] [CrossRef]
- Gorski, J.W.; Quattrone, M.; van Nagell, J.R.; Pavlik, E.J. Assessing the Costs of Screening for Ovarian Cancer in the United States: An Evolving Analysis. Diagnostics 2020, 10, 67. [Google Scholar] [CrossRef] [Green Version]
- van Nagell, J.R.; Miller, R.W.; DeSimone, C.P.; Ueland, J.R.; Podzielinski, I.; Goodrich, S.T.; Elder, J.W.; Huang, B.; Kryscio, R.J.; Pavlik, E.J. Long-term survival of women with epithelial ovarian cancer detected by ultrasonographic screening. Obstet. Gynecol. 2011, 118, 1212–1221. [Google Scholar] [CrossRef]
- Buys, S.S.; Partridge, E.; Black, A.; Johnson, C.C.; Lamerato, L.; Isaacs, C.; Reding, D.J.; Greenlee, R.T.; Yokachi, L.A.; Kessel, B.; et al. Effect of screening on ovarian cancer mortality: The Prostate, Lung, Colorectal and Ovarian (PLCO) Cancer Screening Randomized Controlled Trial. JAMA 2011, 305, 2295–2303. [Google Scholar] [CrossRef]
- Menon, U.; Gentry-Maharaj, A.; Hallett, R.; Ryan, A.; Burnell, M.; Sharma, A.; Lewis, S.; Davies, S.; Philpott, S.; Lopes, A.; et al. Sensitivity and specificity of multimodal and ultrasound screening for ovarian cancer, and stage distribution of detected cancers: Results of the prevalence screen of the UK Collaborative Trial of Ovarian Cancer Screening (UKCTOCS). Lancet Oncol. 2009, 10, 327–340. [Google Scholar] [CrossRef] [Green Version]
- Menon, U.; Gentry-Maharaj, A.; Burnell, M.; Singh, N.; Ryan, A.; Karpinskyj, C.; Carlino, G.; Taylor, J.; Massingham, S.K.; Raikou, M.; et al. Ovarian cancer population screening and mortality after long-term follow-up in the UK Collaborative Trial of Ovarian Cancer Screening (UKCTOCS): A randomised controlled trial. Lancet 2021, 397, 2182–2193. [Google Scholar] [CrossRef]
- Kobayashi, H.; Yamada, Y.; Sado, T.; Sakata, M.; Yoshida, S.; Kawaguchi, R.; Kanayama, S.; Shigetomi, H.; Haruta, S.; Tsuji, Y.; et al. A randomized study of screening for ovarian cancer: A multicenter study in Japan. Int. J.Gynecol. Cancer 2008, 18, 414–420. [Google Scholar] [CrossRef] [PubMed]
- Grillo, D.; Stienmier, R.H.; Lowell, D.M. Early diagnosis of ovarian carcinoma by culdocentesis. Obstet. Gynecol. 1966, 28, 346–350. [Google Scholar] [CrossRef] [PubMed]
- Vassar Website for Statistical Computations. Available online: http://vassarstats.net/index.html (accessed on 1 June 2020).
- Van Calster, B.; Van Hoorde, K.; Valentin, L.; Testa, A.C.; Fischerova, D.; Van Holsbeke, C.; Savelli, L.; Franchi, D.; Epstein, E.; Kaijser, J.; et al. Evaluating the risk of ovarian cancer before surgery using the ADNEX model to differentiate between benign, borderline, early and advanced stage invasive, and secondary metastatic tumours: Prospective multicentre diagnostic study. Version 2. BMJ 2014, 349, g5920. [Google Scholar] [CrossRef] [Green Version]
- Timmerman, D.; Van Calster, B.; Testa, A.; Savelli, L.; Fischerova, D.; Froyman, W.; Wynants, L.; Van Holsbeke, C.; Epstein, E.; Franchi, D.; et al. Predicting the risk of malignancy in adnexal masses based on the Simple Rules from the International Ovarian Tumor Analysis group. Am. J. Obstet. Gynecol. 2016, 214, 424–437. [Google Scholar] [CrossRef] [Green Version]
- Anton, C.; Carvalho, F.M.; Oliveira, E.I.; Maciel, G.A.R.; Baracat, E.C.; Carvalho, J.P. A comparison of CA125, HE4, risk ovarian malignancy algorithm (ROMA), and risk malignancy index (RMI) for the classification of ovarian masses. Clinics (Sao Paulo) 2012, 67, 437–441. [Google Scholar] [CrossRef]
- Kaijser, J.; Van Gorp, T.; Van Hoorde, K.; Van Holsbeke, C.; Sayasneh, A.; Vergote, I.; Bourne, T.; Timmerman, D.; Van Calster, B. A comparison between an ultrasound based prediction model (LR2) and the risk of ovarian malignancy algorithm (ROMA) to assess the risk of malignancy in women with an adnexal mass. Gynecol. Oncol. 2013, 129, 377–383. [Google Scholar] [CrossRef]
- Kaijser, J.; Sayasneh, A.; Van Hoorde, K.; Ghaem-Maghami, S.; Bourne, T.; Timmerman, D.; van Calster, B. Presurgical diagnosis of adnexal tumours using mathematical models and scoring systems: A systematic review and meta-analysis. Hum. Reprod. Update 2014, 20, 449–462. [Google Scholar] [CrossRef] [Green Version]
- Meys, E.M.J.; Kaijser, J.; Kruitwagen, R.F.P.M.; Slangen, B.F.M.; Van Calster, B.; Aertgeerts, B.; Verbakel, J.Y.; Timmerman, D.; Van Gorp, T. Subjective assessment versus ultrasound models to diagnose ovarian cancer: A systematic review and meta-analysis. Eur. J. Cancer 2016, 58, 17–29. [Google Scholar] [CrossRef] [PubMed]
- Meys, E.M.J.; Jeelof, L.S.; Achten, N.M.J.; Slangen, B.F.M.; Lambrechts, S.; Kruitwagen, R.F.P.M.; Van Gorp, T. Estimating risk of malignancy in adnexal masses: External validation of the ADNEX model and comparison with other frequently used ultrasound methods. Ultrasound Obstet. Gynecol. 2017, 49, 784–792. [Google Scholar] [CrossRef]
- Nunes, N.; Ambler, G.; Foo, X.; Widschwendter, M.; Jurkovic, D. Prospective evaluation of IOTA logistic regression models LR1 and LR2 in comparison with subjective pattern recognition for diagnosis of ovarian cancer in an outpatient setting. Ultrasound Obstet. Gynecol. 2018, 51, 829–835. [Google Scholar] [CrossRef]
- Ueland, F.R.; DePriest, P.D.; Pavlik, E.J.; Kryscio, R.J.; Nagell, J.R., Jr. Preoperative differentiation of malignant from benign ovarian tumors: The efficacy of morphology indexing and Doppler flow sonography. Gynecol. Oncol. 2003, 91, 46–50. [Google Scholar] [CrossRef]
- Elder, J.W.; Pavlik, E.J.; Long, A.; Miller, R.W.; DeSimone, C.P.; Hoff, J.T.; Ueland, W.R.; Kryscio, R.J.; van Nagell, J.R., Jr.; Ueland, F.R. Serial ultrasonographic evaluation of ovarian abnormalities with a morphology index. Gynecol. Oncol. 2014, 135, 8–12. [Google Scholar] [CrossRef] [PubMed]
- Ohel, I.; Sheiner, E.; Aricha-Tamir, B.; Piura, B.; Meirovitz, M.; Silberstein, T.; Hershkovitz, R. Three-dimensional power Doppler ultrasound in ovarian cancer and its correlation with histology. Arch. Gynecol. Obstet. 2010, 281, 919–925. [Google Scholar] [CrossRef]
- Savelli, L.; De Iaco, P.; Ceccaroni, M.; Ghi, T.; Ceccarini, M.; Seracchioli, R.; Cacciatore, B. Transvaginal sonographic features of peritoneal carcinomatosis. Ultrasound Obstet. Gynecol. 2005, 26, 552–557. [Google Scholar] [CrossRef]
- Outwater, E.K.; Siegelman, E.S.; Wilson, K.M.; Mitchell, D.G. Benign and malignant gynecologic disease: Clinical importance of fluid and peritoneal enhancement in the pelvis at MR imaging. Radiology 1996, 200, 483–488. [Google Scholar] [CrossRef] [PubMed]
- Thomassin-Naggara, I.; Aubert, E.; Rockall, A.; Jalaguire-Coudray, A.; Rouzier, R.; Daraï, E.; Bazot, M. Adnexal masses: Development and preliminary validation of an MR imaging scoring system. Radiology 2013, 267, 432–443. [Google Scholar] [CrossRef]
- Thomassin-Naggara, I.; Poncelet, E.; Jalaguier-Coudray, A.; Guerra, A.; Fournier, L.S.; Stojanovic, S.; Millet, I.; Bharwani, N.; Juhan, V.; Cunha, T.M.; et al. Ovarian-Adnexal Reporting Data System Magnetic Resonance Imaging (O-RADS MRI) Score for Risk Stratification of Sonographically Indeterminate Adnexal Masses. JAMA Netw. Open 2020, 3, e1919896. [Google Scholar] [CrossRef]
- Rumack, C.M.; Levine, D. Diagnostic Ultrasound, 5th ed.; Elsevier Health Sciences: Philadelphia, PA, USA, 2017. [Google Scholar]
- Hanbidge, A.; Lynch, D.; Wilson, S. US of the peritoneum. Radiographics 2003, 23, 663–685. [Google Scholar] [CrossRef]
- Rudralingam, V.; Footitt, C.; Layton, B. Ascites matters. Ultrasound 2017, 25, 69–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ultrasound Technology & Innovation: Diagnosing the Cause of and Measuring Cul-de-Sac Fluid. Available online: https://www.volusonclub.net/empowered-womens-health/diagnosing-the-cause-of-and-measuring-cul-de-sac-fluid/ (accessed on 20 April 2020).




{kind=link}
{kind=link}
{kind=link}
| Study | KYOVS | PLCO | SCSOCS | UKCTOCS |
|---|---|---|---|---|
| Study design | Prospective cohort (ongoing) | Intent to treat RCT (closed) | Intent to treat RCT (closed) | Intent to treat RCT (closed) |
| Number screened | 48,925 a | 34,253 b 34,304 * | 41,688 b 40,799 * | 50,625 c 50,623 a 101,314 * |
| Total screens | 326,998 | 150,598 | 156,747 | 345,570 c 327,775 a |
| Invasive ovarian cancers detected | 78 | 212 b | 27 | 522 c 517 a 1016 * |
| Shift to early-stage disease d | Yes (63%) | No | Yes (67%) | Yes (39.2%) |
| Survival benefit | Yes | No | No | No e |
| Demographic Variable | All TN Subjects (n = 48,212) | TN and Fluid-Negative (n = 46,263) | TN and Fluid-Positive (n = 1949) | p |
|---|---|---|---|---|
| Age (y) | 57.0, 57 (24–95) | 57.3, 57 (24–95) | 51.4, 52 (25–91) | <0.0001 |
| Parity | 2.3, 2 (0–19) | 2.3, 2 (0–19) | 2.1, 2 (0–8) | <0.0001 |
| Weight (kg) | 73.4, 70.3 (34–204) | 73.5, 70.3 (34–204) | 70.6, 67.1 (41–153) | <0.0001 |
| Height (cm) | 163.3, 162.6 (119–198) | 163.3, 162.6 (119–198) | 164.3, 165 (135–188) | <0.0001 |
| Family cancer history: | ||||
| Ovary | 11,329 (23.5%) | 10,628 (23.0%) | 701 (38.9%) | <0.0001 |
| Breast | 23,758 (49.6%) | 22,797 (49.2%) | 961 (49.3%) | 0.9790 |
| Colon | 13,433 (27.9%) | 12,819 (27.7%) | 614 (31.5%) | 0.0003 |
| No history of hormone replacement therapy | 17,587 (36.5%) | 16,711 (36.1%) | 876 (44.9%) | <0.0001 |
| Hormone replacement on the last visit | 5830 (12.1%) | 5627 (12.2%) | 203 (10.4%) | 0.0205 |
| Nulliparous | 7020 (14.6%) | 6647 (14.4%) | 373 (19.1%) | <0.0001 |
| Demographic Variable | All TP Subjects (n = 78) | TP and Fluid-Negative (n = 64) | TP and Fluid-Positive (n = 14) | p |
|---|---|---|---|---|
| Age (y) | 65.5, 66 (36–86) | 64.9, 66 (36–82) | 68.4, 71 (45–85) | 0.2285 |
| Parity | 2.0, 2 (0–8) | 2.1, 2 (0–8) | 1.8, 2 (0–5) | 0.4818 |
| Weight (kg) | 71.4, 69 (44–122) | 72.5, 69.7 (44–123) | 67.7, 68.6 (52–82) | 0.1920 |
| Height (cm) | 163.2, 163 (142–179) | 163, 163 (152–178) | 164.4, 165 (142–178) | 0.4329 |
| Family cancer history: | ||||
| Ovary | 17 (21.7%) | 15 (23.4%) | 2 (14.2%) | 0.7223 |
| Breast | 33 (42.3%) | 26 (40.6%) | 7 (50%) | 0.5614 |
| Colon | 20 (25.6%) | 16 (25%) | 4 (28.6%) | 0.7464 |
| No history of hormone replacement therapy | 59 (75.6%) | 48 (75%) | 11 (78.6%) | 1 |
| Hormone replacement on the last visit | 6 (7.7%) | 5 (7.8%) | 1 (7.1%) | 1 |
| Nulliparous | 14 (17.0%) | 9 (14.1%) | 5 (35.7%) | 0.1159 |
| Demographic Variable | All FP Subjects (n = 614) | FP and Fluid-Negative (n = 581) | FP and Fluid-Positive (n = 33) | p |
|---|---|---|---|---|
| Age (y) | 59.2, 59 (29–85) | 59.3, 59 (29–85) | 57.1, 59 (36–81) | 0.2992 |
| Parity | 2.1, 2 (0–10) | 2.1, 2 (0–10) | 1.6, 2 (0–4) | 0.0344 |
| Weight (kg) | 74.8, 72.6 (36–167) | 75.1, 72.6 (36–167) | 70.9, 69.9 (47–98) | 0.1632 |
| Height (cm) | 164.4, 162.6 (139–181) | 164.4, 162.6 (140–181) | 164.8, 165 (152–175) | 0.8202 |
| Family cancer history: | ||||
| Ovary | 182 (29.6%) | 168 (28.9%) | 14 (42.4%) | 0.0983 |
| Breast | 269 (43.8%) | 252 (43.3%) | 17 (51.5%) | 0.3592 |
| Colon | 161 (6.2%) | 148 (25.5%) | 13 (39.4%) | 0.0770 |
| No history of hormone replacement therapy | 60 (9.86%) | 58 (10%) | 2 (6.1%) | 0.7612 |
| Hormone replacement on last visit | 41 (6.7%) | 39 (6.7%) | 2 (6.1%) | 1 |
| Nulliparous | 31 (5%) | 29 (5%) | 2 (6.1%) | 0.6797 |
| Group | Fluid-Positive | Fluid-Negative | PR (95% Confidence Interval (CI)) | OR (95% CI) |
|---|---|---|---|---|
| Premenopausal TN with fluid, a normal exam and a BMI < 30 | 166 | 41,830 | 1 | 1 |
| TN with fluid | 1948 | 40,048 | 11.73 (10.02–13.74) | 12.26 (10.45–14.37) |
| TN with fluid and a normal exam | 1071 | 40,925 | 6.45 (5.48–7.59) | 6.59 (5.60–7.77) |
| TN with fluid and an abnormal exam | 877 | 41,119 | 5.28 (4.48–6.23) | 5.37 (4.55–6.35) |
| Premenopausal TN with fluid and a normal exam | 207 | 41,789 | 1.25 (1.02–1.53) | 1.25 (1.02–1.53) |
| Premenopausal TN with fluid, a normal exam, a BMI ≥ 30 | 40 | 41,956 | 0.24 (0.17–0.34) | 0.24 (0.17–0.34) |
| Premenopausal TN with fluid and an abnormal exam | 211 | 41,785 | 1.27 (1.04–1.56) | 1.27 (1.04–1.56) |
| Premenopausal TN with fluid, an abnormal exam, and a BMI < 30 | 158 | 41,838 | 0.95 (0.77–1.18) | 0.0232 (0.77–1.18) |
| Premenopausal TN with fluid, an abnormal exam, and a BMI ≥ 30 | 47 | 41,949 | 0.28 (0.20–0.39) | 0.28 (0.20–0.39) |
| Postmenopausal TN with fluid and a normal exam | 862 | 41,134 | 5.19 (4.40–6.13) | 5.28 (4.47–6.24) |
| Postmenopausal TN with fluid, a normal exam, and a BMI < 30 | 675 | 41,321 | 4.07 (3.43–4.82) | 4.12 (3.47–4.88) |
| Postmenopausal TN with fluid, a normal exam, and a BMI ≥ 30 | 181 | 41,815 | 1.09 (0.88–1.35) | 1.09 (0.88–1.35) |
| Postmenopausal TN with fluid and an abnormal exam | 666 | 41,330 | 4.01 (3.39–4.75) | 4.06 (3.42–4.82) |
| Postmenopausal TN with fluid, an abnormal exam, and a BMI < 30 | 512 | 41,484 | 3.08 (2.59–3.67) | 3.11 (2.61–3.71) |
| Postmenopausal TN with fluid, an abnormal exam, and a BMI ≥ 30 | 149 | 41,847 | 0.90 (0.72–1.12) | 0.90 (0.72–1.12) |
| Group | Fluid-Positive | Fluid-Negative | PR (95% CI) | OR (95% CI) |
|---|---|---|---|---|
| Premenopausal TN with fluid, a normal exam, and a BMI < 30 | 166 | 41830 | 1 | 1 |
| Benign findings (FPs) | 31 | 614 | 12.16 (8.35–17.70) | 12.72 (8.60–18.82) |
| Borderline tumor (low malignant potential (LMP)) | 2 | 26 | 18.07 (4.71–69.30) | 19.38 (4.56–82.33) |
| Ovarian cancer (TP) | 13 | 78 | 36.14 (21.36–61.14) | 42.00 (22.90–77.03) |
| FN for ovarian cancer | 4 | 21 | 40.48 (16.28–100.65) | 48.00 (16.30–141.35) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gorski, J.W.; Dietrich, C.S., III; Davis, C.; Erol, L.; Dietrich, H.; Per, N.J.; Ferrell, E.L.; McDowell, A.B.; Riggs, M.J.; Hutchcraft, M.L.; et al. Significance of Pelvic Fluid Observed during Ovarian Cancer Screening with Transvaginal Sonogram. Diagnostics 2022, 12, 144. https://doi.org/10.3390/diagnostics12010144
Gorski JW, Dietrich CS III, Davis C, Erol L, Dietrich H, Per NJ, Ferrell EL, McDowell AB, Riggs MJ, Hutchcraft ML, et al. Significance of Pelvic Fluid Observed during Ovarian Cancer Screening with Transvaginal Sonogram. Diagnostics. 2022; 12(1):144. https://doi.org/10.3390/diagnostics12010144
Chicago/Turabian StyleGorski, Justin W., Charles S. Dietrich, III, Caeli Davis, Lindsay Erol, Hayley Dietrich, Nicholas J. Per, Emily Lenk Ferrell, Anthony B. McDowell, McKayla J. Riggs, Megan L. Hutchcraft, and et al. 2022. "Significance of Pelvic Fluid Observed during Ovarian Cancer Screening with Transvaginal Sonogram" Diagnostics 12, no. 1: 144. https://doi.org/10.3390/diagnostics12010144
APA StyleGorski, J. W., Dietrich, C. S., III, Davis, C., Erol, L., Dietrich, H., Per, N. J., Ferrell, E. L., McDowell, A. B., Riggs, M. J., Hutchcraft, M. L., Baldwin-Branch, L. A., Miller, R. W., DeSimone, C. P., Gallion, H. H., Ueland, F. R., van Nagell, J. R., Jr., & Pavlik, E. J. (2022). Significance of Pelvic Fluid Observed during Ovarian Cancer Screening with Transvaginal Sonogram. Diagnostics, 12(1), 144. https://doi.org/10.3390/diagnostics12010144