
Biomarkers in EndoVascular Aneurysm Repair (EVAR) and Abdominal Aortic Aneurysm: Pathophysiology and Clinical Implications



 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
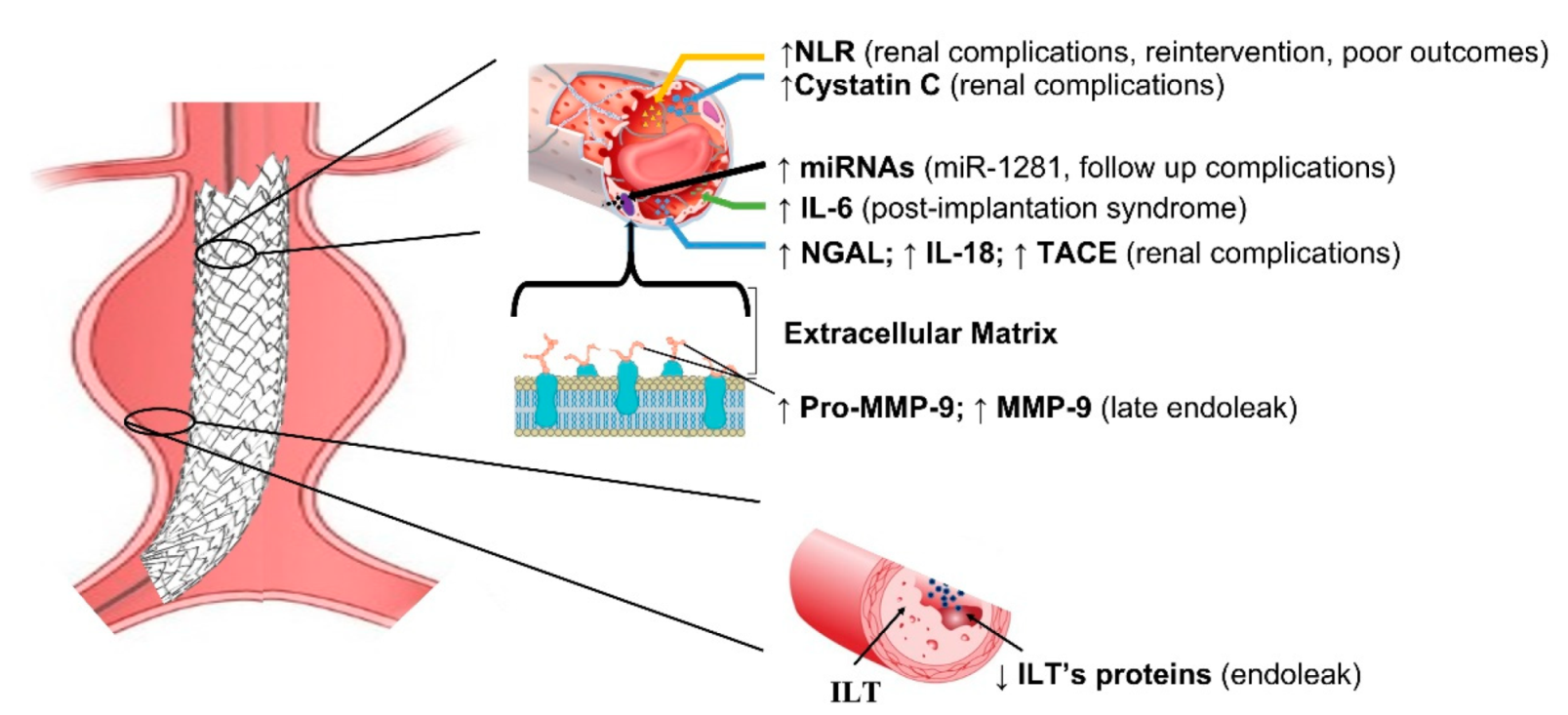
4. Biomarkers and Compounds in EVAR (Treated Disease)
5. Biomarkers and Compounds in Abdominal Aortic Aneurysms (Untreated Disease)
6. The Common Background between EVAR and Untreated AAA: Extracellular Matrix
7. Evidence from Pre-Clinical Studies
8. Future Directions
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ng, E.; Morris, D.R.; Golledge, J. The association between plasma matrix metalloproteinase-9 concentration and endoleak after endovascular aortic aneurysm repair: A meta-analysis. Atherosclerosis 2015, 242, 535–542. [Google Scholar] [CrossRef] [Green Version]
- Karaolanis, G.; Williams, Z.F.; Bakoyiannis, C.; Hadjis, D.; Cox, M.W.; Moris, D. The Clinical Utility and Assessment of Renal Biomarkers in Acute Kidney Injury After Abdominal Endovascular Aneurysm Repair. A Systematic Review. Curr. Pharm. Des. 2019, 25, 4695–4701. [Google Scholar] [CrossRef]
- Tsilimigras, D.I.; Sigala, F.; Karaolanis, G.; Ntanasis-Stathopoulos, I.; Spartalis, E.; Spartalis, M.; Patelis, N.; Papalampros, A.; Long, C.; Moris, D. Cytokines as biomarkers of inflammatory response after open versus endovascular repair of abdominal aortic aneurysms: A systematic review. Acta Pharmacol. Sin. 2018, 39, 1164–1175. [Google Scholar] [CrossRef]
- Antoniou, G.A.; Georgiadis, G.S.; Antoniou, S.A.; Murray, D.; Smyth, J.V.; Serracino-Inglott, F.; Paraskevas, K.I. Plasma matrix metalloproteinase 9 levels may predict endoleaks after endovascular aortic aneurysm repair. Angiology 2013, 64, 49–56. [Google Scholar] [CrossRef]
- Huddle, M.G.; Schlosser, F.J.; Dewan, M.C.; Indes, J.; Muhs, B.E. Can laboratory tests predict the prognosis of patients after endovascular aneurysm repair? Current status and future directions. Vascular 2009, 17, 129–137. [Google Scholar] [CrossRef]
- Kapetanios, D.M.; Karkos, C.D.; Papazoglou, K.O. Changes in circulating markers of coagulation and fibrinolysis after EVAR. Int. Angiol. A J. Int. Union Angiol. 2018, 37, 444–450. [Google Scholar] [CrossRef]
- Davies, R.S.; Abdelhamid, M.; Wall, M.L.; Vohra, R.K.; Bradbury, A.W.; Adam, D.J. Coagulation, fibrinolysis, and platelet activation in patients undergoing open and endovascular repair of abdominal aortic aneurysm. J. Vasc. Surg. 2011, 54, 865–878. [Google Scholar] [CrossRef] [Green Version]
- Missae, L.; Rossoni, B.; Tenorio, E.J.R.; Ribeiro, M.S.; Tirapelli, D.; Joviliano, E.E. Expression of MicroRNA-1281, C-Reactive Protein, and Renal Function in Individuals with Abdominal Aortic Aneurysm and their Clinical Correlation after Endovascular Repair. Braz. J. Cardiovasc. Surg. 2021, 36, 301–307. [Google Scholar] [CrossRef] [PubMed]
- Abdelhamid, M.F.; Davies, R.S.; Vohra, R.K.; Adam, D.J.; Bradbury, A.W. Assessment of renal function by means of cystatin C following standard and fenestrated endovascular aneurysm repair. Ann. Vasc. Surg. 2013, 27, 708–713. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Wang, W.; Chen, Z.; Xu, F.; Zheng, Y. Proteomics applications in biomarker discovery and pathogenesis for abdominal aortic aneurysm. Expert Rev. Proteom. 2021, 18, 305–314. [Google Scholar] [CrossRef] [PubMed]
- Bylund, D.; Henriksson, A.E. Proteomic approaches to identify circulating biomarkers in patients with abdominal aortic aneurysm. Am. J. Cardiovasc. Dis. 2015, 5, 140–145. [Google Scholar] [CrossRef] [Green Version]
- Urbonavicius, S.; Urbonaviciene, G.; Honore, B.; Henneberg, E.W.; Vorum, H.; Lindholt, J.S. Potential circulating biomarkers for abdominal aortic aneurysm expansion and rupture—A systematic review. Eur. J. Vasc. Endovasc. Surg. Off. J. Eur. Soc. Vasc. Surg. 2008, 36, 273–280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stather, P.W.; Sidloff, D.A.; Dattani, N.; Gokani, V.J.; Choke, E.; Sayers, R.D.; Bown, M.J. Meta-analysis and meta-regression analysis of biomarkers for abdominal aortic aneurysm. Br. J. Surg. 2014, 101, 1358–1372. [Google Scholar] [CrossRef]
- Nana, P.; Dakis, K.; Brodis, A.; Spanos, K.; Kouvelos, G. Circulating Biomarkers for the Prediction of Abdominal Aortic Aneurysm Growth. J. Clin. Med. 2021, 10, 1718. [Google Scholar] [CrossRef]
- Moris, D.; Mantonakis, E.; Avgerinos, E.; Makris, M.; Bakoyiannis, C.; Pikoulis, E.; Georgopoulos, S. Novel biomarkers of abdominal aortic aneurysm disease: Identifying gaps and dispelling misperceptions. BioMed Res. Int. 2014, 2014, 925840. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Yang, D.; Zheng, Y. Challenges of applying circulating biomarkers for abdominal aortic aneurysm progression. Exp. Biol. Med. 2021, 246, 1054–1059. [Google Scholar] [CrossRef]
- Groeneveld, M.E.; Meekel, J.P.; Rubinstein, S.M.; Merkestein, L.R.; Tangelder, G.J.; Wisselink, W.; Truijers, M.; Yeung, K.K. Systematic Review of Circulating, Biomechanical, and Genetic Markers for the Prediction of Abdominal Aortic Aneurysm Growth and Rupture. J. Am. Heart Assoc. 2018, 7, e007791. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, F.M.; Rateri, D.L.; Daugherty, A. Abdominal aortic aneurysm: Novel mechanisms and therapies. Curr. Opin. Cardiol. 2015, 30, 566–573. [Google Scholar] [CrossRef] [Green Version]
- Jalalzadeh, H.; Indrakusuma, R.; Planken, R.N.; Legemate, D.A.; Koelemay, M.J.; Balm, R. Inflammation as a Predictor of Abdominal Aortic Aneurysm Growth and Rupture: A Systematic Review of Imaging Biomarkers. Eur. J. Vasc. Endovasc. Surg. Off. J. Eur. Soc. Vasc. Surg. 2016, 52, 333–342. [Google Scholar] [CrossRef] [Green Version]
- Li, T.; Lv, Z.; Jing, J.J.; Yang, J.; Yuan, Y. Matrix metalloproteinase family polymorphisms and the risk of aortic aneurysmal diseases: A systematic review and meta-analysis. Clin. Genet. 2018, 93, 15–32. [Google Scholar] [CrossRef]
- Martin-Ventura, J.L.; Martinez-Lopez, D.; Roldan-Montero, R.; Gomez-Guerrero, C.; Blanco-Colio, L.M. Role of complement system in pathological remodeling of the vascular wall. Mol. Immunol. 2019, 114, 207–215. [Google Scholar] [CrossRef] [PubMed]
- Klopf, J.; Brostjan, C.; Neumayer, C.; Eilenberg, W. Neutrophils as Regulators and Biomarkers of Cardiovascular Inflammation in the Context of Abdominal Aortic Aneurysms. Biomedicines 2021, 9, 1236. [Google Scholar] [CrossRef]
- Araujo, N.N.F.; Lin-Wang, H.T.; Germano, J.F.; Farsky, P.S.; Feldman, A.; Rossi, F.H.; Izukawa, N.M.; Higuchi, M.L.; Savioli Neto, F.; Hirata, M.H.; et al. Dysregulation of microRNAs and target genes networks in human abdominal aortic aneurysm tissues. PLoS ONE 2019, 14, e0222782. [Google Scholar] [CrossRef]
- Butt, H.Z.; Sylvius, N.; Salem, M.K.; Wild, J.B.; Dattani, N.; Sayers, R.D.; Bown, M.J. Microarray-based Gene Expression Profiling of Abdominal Aortic Aneurysm. Eur. J. Vasc. Endovasc. Surg. Off. J. Eur. Soc. Vasc. Surg. 2016, 52, 47–55. [Google Scholar] [CrossRef] [Green Version]
- Plana, E.; Galvez, L.; Medina, P.; Navarro, S.; Fornes-Ferrer, V.; Panadero, J.; Miralles, M. Identification of Novel microRNA Profiles Dysregulated in Plasma and Tissue of Abdominal Aortic Aneurysm Patients. Int. J. Mol. Sci. 2020, 21, 4600. [Google Scholar] [CrossRef]
- Zalewski, D.P.; Ruszel, K.P.; Stepniewski, A.; Galkowski, D.; Bogucki, J.; Kolodziej, P.; Szymanska, J.; Plachno, B.J.; Zubilewicz, T.; Feldo, M.; et al. Identification of Transcriptomic Differences between Lower Extremities Arterial Disease, Abdominal Aortic Aneurysm and Chronic Venous Disease in Peripheral Blood Mononuclear Cells Specimens. Int. J. Mol. Sci. 2021, 22, 3200. [Google Scholar] [CrossRef]
- Zalewski, D.P.; Ruszel, K.P.; Stepniewski, A.; Galkowski, D.; Bogucki, J.; Komsta, L.; Kolodziej, P.; Chmiel, P.; Zubilewicz, T.; Feldo, M.; et al. Dysregulation of microRNA Modulatory Network in Abdominal Aortic Aneurysm. J. Clin. Med. 2020, 9, 1974. [Google Scholar] [CrossRef] [PubMed]
- Blassova, T.; Tonar, Z.; Tomasek, P.; Hosek, P.; Hollan, I.; Treska, V.; Molacek, J. Inflammatory cell infiltrates, hypoxia, vascularization, pentraxin 3 and osteoprotegerin in abdominal aortic aneurysms—A quantitative histological study. PLoS ONE 2019, 14, e0224818. [Google Scholar] [CrossRef]
- Chiang, M.T.; Chen, I.M.; Hsu, F.F.; Chen, Y.H.; Tsai, M.S.; Hsu, Y.W.; Leu, H.B.; Huang, P.H.; Chen, J.W.; Liu, F.T.; et al. Gal-1 (Galectin-1) Upregulation Contributes to Abdominal Aortic Aneurysm Progression by Enhancing Vascular Inflammation. Arterioscler. Thromb. Vasc. Biol. 2021, 41, 331–345. [Google Scholar] [CrossRef]
- Hauzer, W.; Ferenc, S.; Rosinczuk, J.; Gnus, J. The Role of Serum Calprotectin as a New Marker in Abdominal Aortic Aneurysms—A Preliminary Report. Curr. Pharm. Biotechnol. 2021, 22, 508–513. [Google Scholar] [CrossRef] [PubMed]
- Hauzer, W.; Witkiewicz, W.; Gnus, J. Calprotectin and Receptor for Advanced Glycation End Products as a Potential Biomarker in Abdominal Aortic Aneurysm. J. Clin. Med. 2020, 9, 927. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moran, C.S.; Biros, E.; Krishna, S.M.; Morton, S.K.; Sexton, D.J.; Golledge, J. Kallikrein-1 Blockade Inhibits Aortic Expansion in a Mouse Model and Reduces Prostaglandin E2 Secretion From Human Aortic Aneurysm Explants. J. Am. Heart Assoc. 2021, 10, e019372. [Google Scholar] [CrossRef]
- Li, T.; Yang, C.; Jing, J.; Sun, L.; Yuan, Y. Granzyme K—A novel marker to identify the presence and rupture of abdominal aortic aneurysm. Int. J. Cardiol. 2021, 338, 242–247. [Google Scholar] [CrossRef]
- Wu, Z.Y.; Trenner, M.; Boon, R.A.; Spin, J.M.; Maegdefessel, L. Long noncoding RNAs in key cellular processes involved in aortic aneurysms. Atherosclerosis 2020, 292, 112–118. [Google Scholar] [CrossRef] [Green Version]
- Raffort, J.; Lareyre, F.; Clement, M.; Mallat, Z. Micro-RNAs in abdominal aortic aneurysms: Insights from animal models and relevance to human disease. Cardiovasc. Res. 2016, 110, 165–177. [Google Scholar] [CrossRef] [Green Version]
- Kumar, S.; Boon, R.A.; Maegdefessel, L.; Dimmeler, S.; Jo, H. Role of Noncoding RNAs in the Pathogenesis of Abdominal Aortic Aneurysm. Circ. Res. 2019, 124, 619–630. [Google Scholar] [CrossRef]
- Borek, A.; Drzymala, F.; Botor, M.; Augusciak-Duma, A.M.; Sieron, A.L. Roles of microRNAs in abdominal aortic aneurysm pathogenesis and the possibility of their use as biomarkers. Kardiochirurgia I Torakochirurgia Pol. = Pol. J. Cardio-Thorac. Surg. 2019, 16, 124–127. [Google Scholar] [CrossRef] [PubMed]
- Iyer, V.; Rowbotham, S.; Biros, E.; Bingley, J.; Golledge, J. A systematic review investigating the association of microRNAs with human abdominal aortic aneurysms. Atherosclerosis 2017, 261, 78–89. [Google Scholar] [CrossRef]
- Knappich, C.; Spin, J.M.; Eckstein, H.H.; Tsao, P.S.; Maegdefessel, L. Involvement of Myeloid Cells and Noncoding RNA in Abdominal Aortic Aneurysm Disease. Antioxid. Redox Signal. 2020, 33, 602–620. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hovsepian, D.M.; Ziporin, S.J.; Sakurai, M.K.; Lee, J.K.; Curci, J.A.; Thompson, R.W. Elevated plasma levels of matrix metalloproteinase-9 in patients with abdominal aortic aneurysms: A circulating marker of degenerative aneurysm disease. J. Vasc. Interv. Radiol. JVIR 2000, 11, 1345–1352. [Google Scholar] [CrossRef]
- LeMaire, S.A.; Wang, X.; Wilks, J.A.; Carter, S.A.; Wen, S.; Won, T.; Leonardelli, D.; Anand, G.; Conklin, L.D.; Wang, X.L.; et al. Matrix metalloproteinases in ascending aortic aneurysms: Bicuspid versus trileaflet aortic valves. J. Surg. Res. 2005, 123, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Koullias, G.J.; Ravichandran, P.; Korkolis, D.P.; Rimm, D.L.; Elefteriades, J.A. Increased tissue microarray matrix metalloproteinase expression favors proteolysis in thoracic aortic aneurysms and dissections. Ann. Thorac. Surg. 2004, 78, 2106–2110. [Google Scholar] [CrossRef]
- Ramirez, F.; Rifkin, D.B. Extracellular microfibrils: Contextual platforms for TGFbeta and BMP signaling. Curr. Opin. Cell Biol. 2009, 21, 616–622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steffensen, L.B.; Stubbe, J.; Lindholt, J.S.; Beck, H.C.; Overgaard, M.; Bloksgaard, M.; Genovese, F.; Holm Nielsen, S.; Tha, M.L.T.; Bang-Moeller, S.K.; et al. Basement membrane collagen IV deficiency promotes abdominal aortic aneurysm formation. Sci. Rep. 2021, 11, 12903. [Google Scholar] [CrossRef] [PubMed]
- Ostberg, N.P.; Zafar, M.A.; Ziganshin, B.A.; Elefteriades, J.A. The Genetics of Thoracic Aortic Aneurysms and Dissection: A Clinical Perspective. Biomolecules 2020, 10, 182. [Google Scholar] [CrossRef] [Green Version]
- Schwarze, U.; Schievink, W.I.; Petty, E.; Jaff, M.R.; Babovic-Vuksanovic, D.; Cherry, K.J.; Pepin, M.; Byers, P.H. Haploinsufficiency for one COL3A1 allele of type III procollagen results in a phenotype similar to the vascular form of Ehlers-Danlos syndrome, Ehlers-Danlos syndrome type IV. Am. J. Hum. Genet. 2001, 69, 989–1001. [Google Scholar] [CrossRef] [Green Version]
- Neptune, E.R.; Frischmeyer, P.A.; Arking, D.E.; Myers, L.; Bunton, T.E.; Gayraud, B.; Ramirez, F.; Sakai, L.Y.; Dietz, H.C. Dysregulation of TGF-beta activation contributes to pathogenesis in Marfan syndrome. Nat. Genet. 2003, 33, 407–411. [Google Scholar] [CrossRef]
- Didangelos, A.; Yin, X.; Mandal, K.; Baumert, M.; Jahangiri, M.; Mayr, M. Proteomics characterization of extracellular space components in the human aorta. Mol. Cell. Proteom. MCP 2010, 9, 2048–2062. [Google Scholar] [CrossRef] [Green Version]
- Barallobre-Barreiro, J.; Loeys, B.; Mayr, M.; Rienks, M.; Verstraeten, A.; Kovacic, J.C. Extracellular Matrix in Vascular Disease, Part 2/4: JACC Focus Seminar. J. Am. Coll. Cardiol. 2020, 75, 2189–2203. [Google Scholar] [CrossRef]
- Yin, X.; Wanga, S.; Fellows, A.L.; Barallobre-Barreiro, J.; Lu, R.; Davaapil, H.; Franken, R.; Fava, M.; Baig, F.; Skroblin, P.; et al. Glycoproteomic Analysis of the Aortic Extracellular Matrix in Marfan Patients. Arterioscler. Thromb. Vasc. Biol. 2019, 39, 1859–1873. [Google Scholar] [CrossRef] [PubMed]
- Eilenberg, W.; Zagrapan, B.; Bleichert, S.; Ibrahim, N.; Knobl, V.; Brandau, A.; Martelanz, L.; Grasl, M.T.; Hayden, H.; Nawrozi, P.; et al. Histone citrullination as a novel biomarker and target to inhibit progression of abdominal aortic aneurysms. Transl. Res. J. Lab. Clin. Med. 2021, 233, 32–46. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Wang, M.; Zhang, J.; Xu, P.; Wang, H. MicroRNA-29a-3p regulates abdominal aortic aneurysm development and progression via direct interaction with PTEN. J. Cell. Physiol. 2020, 235, 9414–9423. [Google Scholar] [CrossRef]
- Huang, K.; Wang, Y.; Siu, K.L.; Zhang, Y.; Cai, H. Targeting feed-forward signaling of TGFbeta/NOX4/DHFR/eNOS uncoupling/TGFbeta axis with anti-TGFbeta and folic acid attenuates formation of aortic aneurysms: Novel mechanisms and therapeutics. Redox Biol. 2021, 38, 101757. [Google Scholar] [CrossRef]
- Huang, T.; Liu, S.; Liu, R.; Pan, B.; Wang, W. Inhibition of miR-188-5p Suppresses Progression of Experimental Abdominal Aortic Aneurysms. J. Cardiovasc. Pharmacol. 2021, 77, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Ilic, N.S.; Opacic, D.; Mutavdzic, P.; Koncar, I.; Dragas, M.; Jovicic, S.; Markovic, M.; Davidovic, L. Evaluation of the renal function using serum Cystatin C following open and endovascular aortic aneurysm repair. Vascular 2018, 26, 132–141. [Google Scholar] [CrossRef]
- Arnaoutoglou, E.; Kouvelos, G.; Papa, N.; Karamoutsios, A.; Bouris, V.; Vartholomatos, G.; Matsagkas, M. Platelet activation after endovascular repair of abdominal aortic aneurysm. Vascular 2016, 24, 287–294. [Google Scholar] [CrossRef]
- De Haro, J.; Bleda, S.; Acin, F. C-reactive protein predicts aortic aneurysmal disease progression after endovascular repair. Int. J. Cardiol. 2016, 202, 701–706. [Google Scholar] [CrossRef] [PubMed]
- Courtois, A.; Makrygiannis, G.; El Hachemi, M.; Hultgren, R.; Allaire, E.; Namur, G.; Hustinx, R.; Defraigne, J.O.; Sakalihasan, N. Positron Emission Tomography/Computed Tomography Predicts and Detects Complications After Endovascular Repair of Abdominal Aortic Aneurysms. J. Endovasc. Ther. Off. J. Int. Soc. Endovasc. Spec. 2019, 26, 520–528. [Google Scholar] [CrossRef]
- Ascoli Marchetti, A.; Pratesi, G.; Di Giulio, L.; Battistini, M.; Massoud, R.; Ippoliti, A. EVAR and OPEN treatment of abdominal aortic aneurysm: What is the role of MMP-9 in the follow-up? J. Med. Vasc. 2017, 42, 21–28. [Google Scholar] [CrossRef] [Green Version]
- Georgiadis, G.S.; Antoniou, G.A.; Argyriou, C.; Schoretsanitis, N.; Nikolopoulos, E.; Kapoulas, K.; Lazarides, M.K.; Tentes, I. Correlation of Baseline Plasma and Inguinal Connective Tissue Metalloproteinases and Their Inhibitors With Late High-Pressure Endoleak After Endovascular Aneurysm Repair: Long-term Results. J. Endovasc. Ther. Off. J. Int. Soc. Endovasc. Spec. 2019, 26, 826–835. [Google Scholar] [CrossRef] [PubMed]
- Hellenthal, F.A.; Ten Bosch, J.A.; Pulinx, B.; Wodzig, W.K.; de Haan, M.W.; Prins, M.H.; Welten, R.J.; Teijink, J.A.; Schurink, G.W. Plasma levels of matrix metalloproteinase-9: A possible diagnostic marker of successful endovascular aneurysm repair. Eur. J. Vasc. Endovasc. Surg. Off. J. Eur. Soc. Vasc. Surg. 2012, 43, 171–172. [Google Scholar] [CrossRef] [Green Version]
- Moxon, J.V.; Ng, E.; Lazzaroni, S.M.; Boult, M.; Velu, R.; Fitridge, R.A.; Golledge, J. Circulating biomarkers are not associated with endoleaks after endovascular repair of abdominal aortic aneurysms. J. Vasc. Surg. 2018, 67, 770–777. [Google Scholar] [CrossRef] [Green Version]
- Filis, K.; Martinakis, V.; Galyfos, G.; Sigala, F.; Theodorou, D.; Andreadou, I.; Zografos, G. Osteopontin and Osteoprotegerin as Potential Biomarkers in Abdominal Aortic Aneurysm before and after Treatment. Int. Sch. Res. Not. 2014, 2014, 461239. [Google Scholar] [CrossRef]
- Ikoma, A.; Nakai, M.; Sato, M.; Sato, H.; Takeuchi, H.; Tanaka, F.; Sanda, H.; Nakata, K.; Minamiguchi, H.; Sonomura, T.; et al. Changes in inflammatory, coagulopathic, and fibrinolytic responses after endovascular repair of an abdominal aortic aneurysm: Relationship between fibrinogen degradation product levels and endoleaks. Jpn. J. Radiol. 2014, 32, 347–355. [Google Scholar] [CrossRef]
- Inagaki, E.; Farber, A.; Eslami, M.H.; Kalish, J.; Rybin, D.V.; Doros, G.; Peacock, M.R.; Siracuse, J.J. Preoperative hypoalbuminemia is associated with poor clinical outcomes after open and endovascular abdominal aortic aneurysm repair. J. Vasc. Surg. 2017, 66, 53–63.e51. [Google Scholar] [CrossRef] [Green Version]
- Wohlauer, M.; Brier, C.; Kuramochi, Y.; Eagleton, M. Preoperative Hypoalbuminemia is a Risk Factor for Early and Late Mortality in Patients Undergoing Endovascular Juxtarenal and Thoracoabdominal Aortic Aneurysm Repair. Ann. Vasc. Surg. 2017, 42, 198–204. [Google Scholar] [CrossRef]
- Kapetanios, D.; Karkos, C.D.; Pliatsios, I.; Mitka, M.; Giagtzidis, I.T.; Konstantinidis, K.; Papazoglou, K.O. Association Between Perioperative Fibrinogen Levels and the Midterm Outcome in Patients Undergoing Elective Endovascular Repair of Abdominal Aortic Aneurysms. Ann. Vasc. Surg. 2019, 56, 202–208. [Google Scholar] [CrossRef]
- Lecumberri, E.; Ruiz-Carmona, C.; Mateos, E.; Galarza, A.; Subirana, I.; Clara, A. Prognostic Value of Inflammatory Biomarkers in 5-Year Survival After Endovascular Repair of Abdominal Aortic Aneurysms in a Predominantly Male Cohort: Implications for Practice. World J. Surg. 2021, 45, 1949–1955. [Google Scholar] [CrossRef] [PubMed]
- Ntalouka, M.P.; Nana, P.; Kouvelos, G.N.; Stamoulis, K.; Spanos, K.; Giannoukas, A.; Matsagkas, M.; Arnaoutoglou, E. Association of Neutrophil-Lymphocyte and Platelet-Lymphocyte Ratio with Adverse Events in Endovascular Repair for Abdominal Aortic Aneurysm. J. Clin. Med. 2021, 10, 1083. [Google Scholar] [CrossRef] [PubMed]
- Octeau, D.; Faries, C.; Barnes, H.; Nakazawa, K.R.; Rao, A.J.; Ting, W.; Marin, M.L.; Vouyouka, A.G.; Faries, P.L.; Tadros, R.O. Neutrophil-to-Lymphocyte Ratio Associated With Adverse Events After Endovascular Aneurysm Repair (EVAR). Ann. Vasc. Surg. 2021, 75, 45–54. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Choi, J.H.; Kim, E.J. Volume of mural thrombus plays a role in the elevation of inflammatory markers after endovascular aortic repair. J. Cardiothorac. Surg. 2018, 13, 27. [Google Scholar] [CrossRef]
- Lee, R.; Cassimee, I.; Huang, H.; Lapolla, P.; Ngetich, E.; Chandrashekar, A.; Charles, P.; Kessler, B.; Fischer, R.; Handa, A. Integrated Plasma and Tissue Proteomics Reveals Attractin Release by Intraluminal Thrombus of Abdominal Aortic Aneurysms and Improves Aneurysm Growth Prediction in Humans. Ann. Surg. 2020. [Google Scholar] [CrossRef] [PubMed]
- Sartipy, F.; Lindstrom, D.; Gillgren, P.; Ternhag, A. The role of procalcitonin in postimplantation syndrome after EVAR: A pilot study. Ann. Vasc. Surg. 2014, 28, 866–873. [Google Scholar] [CrossRef]
- Nessvi Otterhag, S.; Gottsater, A.; Acosta, S.; Palmqvist, B.; Lindblad, B. Inflammatory mediators after endovascular aortic aneurysm repair. Cytokine 2014, 70, 151–155. [Google Scholar] [CrossRef] [PubMed]
- Noorani, A.; Sadat, U.; Rollins, K.E.; Chowdhury, M.M.; Tang, T.Y.; Harrison, S.C.; Usman, A.; Burling, K.; Nordon, A.; Boyle, J.R. Assessment of Renal Injury in Patients Undergoing Elective EVAR Using Urinary Neutrophil Gelatin-Associated Lipocalin, Interleukin 18, and Retinol-Binding Protein. Angiology 2017, 68, 547–552. [Google Scholar] [CrossRef] [PubMed]
- Rampoldi, B.; Tessarolo, S.; Giubbilini, P.; Gaia, P.; Corino, S.D.; Mazza, S.; Rigolini, R.; Poli, M.D.; Vianello, E.; Romanelli, M.M.C.; et al. Neutrophil gelatinase-associated lipocalin and acute kidney injury in endovascular aneurysm repair or open aortic repair: A pilot study. Biochem. Med. 2018, 28, 010904. [Google Scholar] [CrossRef]
- Obata, Y.; Kamijo-Ikemori, A.; Ichikawa, D.; Sugaya, T.; Kimura, K.; Shibagaki, Y.; Tateda, T. Clinical usefulness of urinary liver-type fatty-acid-binding protein as a perioperative marker of acute kidney injury in patients undergoing endovascular or open-abdominal aortic aneurysm repair. J. Anesth. 2016, 30, 89–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Obata, Y.; Kamijo-Ikemori, A.; Inoue, S. Clinical Utility of Urinary Biomarkers for Prediction of Acute Kidney Injury and Chronic Renal Dysfunction After Open Abdominal Aortic Aneurysm Repair. Int. J. Nephrol. Renov. Dis. 2021, 14, 371–384. [Google Scholar] [CrossRef] [PubMed]
- Ousaka, D.; Fujii, Y.; Oozawa, S.; Nishibori, M.; Kuroko, Y.; Masuda, Z.; Sano, S. Decreased Serum Levels of High Mobility Group Box 1 (HMGB-1) after Graft Replacement or Stenting of Abdominal Aortic Aneurysm. Ann. Vasc. Surg. 2017, 41, 265–270. [Google Scholar] [CrossRef] [Green Version]
- Pirgakis, K.M.; Makris, K.; Dalainas, I.; Lazaris, A.M.; Maltezos, C.K.; Liapis, C.D. Urinary cystatin C as an early biomarker of acute kidney injury after open and endovascular abdominal aortic aneurysm repair. Ann. Vasc. Surg. 2014, 28, 1649–1658. [Google Scholar] [CrossRef]
- Wang, Y.; Ge, W.; Niu, L.; Yu, W.; Li, C.; Wang, H. Combined Detection of Plasma Tumor Necrosis Factor-alpha Converting Enzyme and Notch1 is Valuable in Screening Endoleak After Endovascular Abdominal Aortic Aneurysms Repair. Ann. Vasc. Surg. 2021, 76, 302–308. [Google Scholar] [CrossRef] [PubMed]
- Whaley, Z.L.; Cassimjee, I.; Novak, Z.; Rowland, D.; Lapolla, P.; Chandrashekar, A.; Pearce, B.J.; Beck, A.W.; Handa, A.; Lee, R. The Spatial Morphology of Intraluminal Thrombus Influences Type II Endoleak after Endovascular Repair of Abdominal Aortic Aneurysms. Ann. Vasc. Surg. 2020, 66, 77–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yates, C.M.; Abdelhamid, M.; Adam, D.J.; Nash, G.B.; Bradbury, A.W.; Rainger, G.E. Endovascular aneurysm repair reverses the increased titer and the inflammatory activity of interleukin-1alpha in the serum of patients with abdominal aortic aneurysm. J. Vasc. Surg. 2011, 54, 497–503. [Google Scholar] [CrossRef] [Green Version]
- Zettervall, S.L.; Dansey, K.; Swerdlow, N.J.; Soden, P.; Evenson, A.; Schermerhorn, M.L. Aspartate transaminase to platelet ratio index and Model for End-Stage Liver Disease scores are associated with morbidity and mortality after endovascular aneurysm repair among patients with liver dysfunction. J. Vasc. Surg. 2020, 72, 904–909. [Google Scholar] [CrossRef]
- Zettervall, S.L.; Ultee, K.H.J.; Soden, P.A.; Deery, S.E.; Shean, K.E.; Pothof, A.B.; Wyers, M.; Schermerhorn, M.L. Predictors of renal dysfunction after endovascular and open repair of abdominal aortic aneurysms. J. Vasc. Surg. 2017, 65, 991–996. [Google Scholar] [CrossRef] [Green Version]
- Lesiak, M.; Augusciak-Duma, A.; Stepien, K.L.; Fus-Kujawa, A.; Botor, M.; Sieron, A.L. Searching for new molecular markers for cells obtained from abdominal aortic aneurysm. J. Appl. Genet. 2021, 62, 487–497. [Google Scholar] [CrossRef]
- Xie, X.; Wang, E.C.; Xu, D.; Shu, X.; Zhao, Y.F.; Guo, D.; Fu, W.; Wang, L. Bioinformatics Analysis Reveals the Potential Diagnostic Biomarkers for Abdominal Aortic Aneurysm. Front. Cardiovasc. Med. 2021, 8, 656263. [Google Scholar] [CrossRef]
- Gan, S.; Pan, Y.; Mao, J. miR-30a-GNG2 and miR-15b-ACSS2 Interaction Pairs May Be Potentially Crucial for Development of Abdominal Aortic Aneurysm by Influencing Inflammation. DNA Cell Biol. 2019, 38, 1540–1556. [Google Scholar] [CrossRef]
- Gan, S.; Shi, W.; Tang, J. miRNAs regulating the expressions of NTF3, GNG2 and ITGA7 are involved in the pathogenesis of abdominal aortic aneurysm in mice. Gen. Physiol. Biophys. 2021, 40, 1–16. [Google Scholar] [CrossRef]
- Guo, S.; Li, Y.; Li, R.; Zhang, P.; Wang, Y.; Gopinath, S.C.B.; Gong, K.; Wan, P. High-performance detection of an abdominal aortic aneurysm biomarker by immunosensing. Biotechnol. Appl. Biochem. 2020, 67, 383–388. [Google Scholar] [CrossRef]
- Cersit, S.; Ocal, L.; Keskin, M.; Gursoy, M.O.; Kalcik, M.; Bayam, E.; Karaduman, A.; Uysal, S.; Uslu, A.; Kup, A.; et al. Association of C-Reactive Protein-to-Albumin Ratio With the Presence and Progression of Abdominal Aortic Aneurysm. Angiology 2021, 72, 153–158. [Google Scholar] [CrossRef]
- Lu, H.Y.; Shih, C.M.; Sung, S.H.; Wu, A.T.H.; Cheng, T.M.; Lin, Y.C.; Shih, C.C. Galectin-3 as a Biomarker for Stratifying Abdominal Aortic Aneurysm Size in a Taiwanese Population. Front. Cardiovasc. Med. 2021, 8, 663152. [Google Scholar] [CrossRef]
- Jablonska, A.; Zagrapan, B.; Neumayer, C.; Klinger, M.; Eilenberg, W.; Nanobachvili, J.; Paradowska, E.; Brostjan, C.; Huk, I. TLR2 2029C/T and TLR3 1377C/T and -7C/A Polymorphisms Are Associated with the Occurrence of Abdominal Aortic Aneurysm. J. Immunol. 2020, 204, 2900–2909. [Google Scholar] [CrossRef]
- Jeong, S.J.; Cho, M.J.; Ko, N.Y.; Kim, S.; Jung, I.H.; Min, J.K.; Lee, S.H.; Park, J.G.; Oh, G.T. Deficiency of peroxiredoxin 2 exacerbates angiotensin II-induced abdominal aortic aneurysm. Exp. Mol. Med. 2020, 52, 1587–1601. [Google Scholar] [CrossRef]
- Kim, E.N.; Yu, J.; Lim, J.S.; Jeong, H.; Kim, C.J.; Choi, J.S.; Kim, S.R.; Ahn, H.S.; Kim, K.; Oh, S.J. CRP immunodeposition and proteomic analysis in abdominal aortic aneurysm. PLoS ONE 2021, 16, e0245361. [Google Scholar] [CrossRef]
- Li, L.; Shao, J.; Niu, W.; Che, H.; Song, F.; Liu, G.; Lu, S. Neutrophil Gelatinase-Associated Lipocalin as an Early Predictor of Contrast-Induced Nephropathy Following Endovascular Aortic Repair for Abdominal Aortic Aneurysm. Clin. Appl. Thromb./Hemost. Off. J. Int. Acad. Clin. Appl. Thromb./Hemost. 2021, 27, 10760296211025618. [Google Scholar] [CrossRef]
- Li, T.; Wang, T.; Zhao, X. Profiles of immune infiltration in abdominal aortic aneurysm and their associated marker genes: A gene expression-based study. Braz. J. Med. Biol. Res. = Rev. Bras. De Pesqui. Med. E Biol. 2021, 54, e11372. [Google Scholar] [CrossRef]
- Lieberg, J.; Wanhainen, A.; Ottas, A.; Vahi, M.; Zilmer, M.; Soomets, U.; Bjorck, M.; Kals, J. Metabolomic Profile of Abdominal Aortic Aneurysm. Metabolites 2021, 11, 555. [Google Scholar] [CrossRef]
- Lindquist Liljeqvist, M.; Eriksson, L.; Villard, C.; Lengquist, M.; Kronqvist, M.; Hultgren, R.; Roy, J. Dipeptidyl peptidase-4 is increased in the abdominal aortic aneurysm vessel wall and is associated with aneurysm disease processes. PLoS ONE 2020, 15, e0227889. [Google Scholar] [CrossRef] [Green Version]
- Maitiseyiti, A.; Ci, H.; Fang, Q.; Guan, S.; Shawuti, A.; Wang, H.; Ge, X. Identification of Novel Long Noncoding RNAs and Their Role in Abdominal Aortic Aneurysm. BioMed Res. Int. 2020, 2020, 3502518. [Google Scholar] [CrossRef]
- Memon, A.A.; Zarrouk, M.; Agren-Witteschus, S.; Sundquist, J.; Gottsater, A.; Sundquist, K. Identification of novel diagnostic and prognostic biomarkers for abdominal aortic aneurysm. Eur. J. Prev. Cardiol. 2020, 27, 132–142. [Google Scholar] [CrossRef]
- Shi, F.; Ma, C.; Ji, C.; Li, M.; Liu, X.; Han, Y. Serum Lipid Oxidative Stress Products as Risk Factors Are the Candidate Predictive Biomarkers for Human Abdominal Aortic Aneurysms. Clin. Appl. Thromb. /Hemost. Off. J. Int. Acad. Clin. Appl. Thromb. /Hemost. 2020, 26, 1076029620932226. [Google Scholar] [CrossRef] [PubMed]
- Tran, A.; Pope, A.; Dear, A.E. Point of care ankle pulse waveform: A biomarker for abdominal aortic aneurysm? Vascular 2021, 17085381211013976. [Google Scholar] [CrossRef]
- Xie, T.; Yin, L.; Guo, D.; Zhang, Z.; Chen, Y.; Liu, B.; Wang, W.; Zheng, Y. The potential role of plasma fibroblast growth factor 21 as a diagnostic biomarker for abdominal aortic aneurysm presence and development. Life Sci. 2021, 274, 119346. [Google Scholar] [CrossRef]
- Liu, P.; Sun, Z.; Zhang, Y.; Guo, W. Myeloid related protein 8/14 is a new candidate biomarker and therapeutic target for abdominal aortic aneurysm. Biomed. Pharmacother. = Biomed. Pharmacother. 2019, 118, 109229. [Google Scholar] [CrossRef]
- Xu, W.; Chao, Y.; Liang, M.; Huang, K.; Wang, C. CTRP13 Mitigates Abdominal Aortic Aneurysm Formation via NAMPT1. Mol. Ther. J. Am. Soc. Gene Ther. 2021, 29, 324–337. [Google Scholar] [CrossRef]
- Zhang, H.; Yang, D.; Chen, S.; Li, F.; Cui, L.; Liu, Z.; Shao, J.; Chen, Y.; Liu, B.; Zheng, Y. Identification of potential proteases for abdominal aortic aneurysm by weighted gene coexpression network analysis. Genome 2020, 63, 561–575. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Biomarker/Compound | Biological Effect and Clinical Importance | Reference |
|---|---|---|
| Cystatin C | Early marker of renal failure–significant increase of Cystatin C 24 h after EVAR and for 12 months. | [9] |
| Cystatin C levels in endovascular aneurysm repair patients significantly increased post- operatively and restored to values comparable to baseline at the discharge. | [55] | |
| Platelet count and markers of platelet activation (CD-62P; CD36) | Significant reduction in PLT count and increase in PLT activation at the immediate postoperative period | [56,57] |
| Genetic features (MSN, PSMB10, and STIM1) | Three genes (MSN, PSMB10, and STIM1) are downregulated in AAA compared with controls; EIF3G, SIVA, PUF60, CYC1, FIBP, and CARD8 were downregulated post-EVAR. Those genes are involved in: regulation of apoptosis, proteolysis, the electron transport chain, leukocyte migration, and the humoral immune response | [24] |
| 18F-fluorodeoxyglucose (FDG) detected with PET/CT; D-dimer | Patients who developed endoleak had a significantly higher SUVr compared to patients who did not develop endoleak. The SUVr was significantly higher in the group of patients with sac growth compared to patients with decreased AAA diameter. Quantitative analysis showed that sac growth and SUVr were significantly higher in the presence of endoleak after EVAR. D-dimer was significantly increased in patients with both endoleak and positive PET/CT in the post-EVAR group. | [58] |
| Matrix metalloproteinase and tissue inhibitors: MMP-2, MMP-9 (Pro and activate), TIMP-1, TIMP-2 | Inguinal fascial tissue proMMP-9 significantly predicted late endoleak. | [59,60] |
| ProMMP-9 and active MMP-9 biomarkers are significantly associated with late endoleak. | [61,62] | |
| Osteopontin (OPN) and osteoprotegerin (OPG) | OPN (a calcification inhibitor) values are associated with aneurysm presence (more expressed in AAA group than in the control group, hernia pts); OPN values increase after AAA repair, independently of the type of repair. | [63] |
| Fibrinogen degradation product (FDP) | A change in FDP of 3.1 mg/mL was the optimal cutoff point for predicting the presence of an endoleak after EVAR | [64] |
| Albumin | Preoperative hypoalbuminemia is associated with increased postoperative morbidity and mortality in a severity-dependent manner among patients undergoing OAR or EVAR | [65] |
| Preoperative hypoalbuminemia is associated with increased postoperative mortality in pts after FEVAR | [66] | |
| Fibrinogen | the difference in fibrinogen levels (baseline to 24 h post-procedure) were significantly higher in patients with endoleaks | [6,67] |
| Neutrophil-to-lymphocyte ratio (NLR) | Preop NLR > 3 was independently associated with lower survival rates at 2-years | [68] |
| NLR postoperative value of 9.9 PLR postoperative value of 22.8 were associated with the occurrence of AKI after EVAR | [69] | |
| High preoperative level of NLR (>3.6) was significantly associated with higher rates of death at 5 years as well as higher rates of reinterventions at 30 days, 1 year and 5 years. | [70] | |
| Routine blood tests, white blood cell (WBC), C-reactive protein (CRP), procalcitonin (PCT) | WBC and CRP revealed that inflammatory markers were significantly enhanced as the volume of mural thrombus increased | [71,72] |
| High C-reactive protein, high WBC and low postoperative procalcitonin are associated with post-implantation syndrome | [73] | |
| miRNA | hyperexpression of miRNA-1281 in patients with AAA and a significant reduction of it after EVAR miRNA-1281 presents a significant reduction in patients with no follow-up complications | [8] |
| Urokinase plasminogen activator (suPAR), endothelin (ET)-1, tumour necrosis factor (TNF)-a, interleukin (IL)-6, IgM antibodies against phosphorylcholine (IgM anti-PC) | SuPAR (p < 0.001), ET-1 (p = 0.003) and IL-6 (p = 0.02) increased whereas IgM anti-PC decreased (p < 0.001) after EVAR | [74] |
| Neutrophil gelatin-associated lipocalin (NGAL), interleukin 18 (IL-18), and retinol-binding protein (urine levels) | A significant rise in levels of NGAL and IL-18 precedes the significant rise in Serum creatinine in pts with AKI after EVAR | [75,76] |
| Urinary liver-type fatty-acid-binding pro- tein (L-FABP) | A significant rise in level of urinary L-FABP precedes the rise of serum creatinine in pts with AKI after EVAR | [77,78] |
| High-mobility group box 1 (HMGB-1) | Serum HMGB-1: intracellular regulator of gene transcription and promotes secretion of several inflammatory cytokines. Serum HMGB-1 levels in AAA patients were significantly higher than in healthy controls; the serum HMGB-1 levels in both the EVAR group and the OAR group were significantly decreased from baseline at both 3 months and 1 year after surgery | [79] |
| Urinary Cystatin C (uCysC) | High postoperative level uCysC precedes the rise of serum creatinine in pts with AKI after EVAR or OR | [80] |
| Tumor necrosis factor-α converting enzyme (TACE), Notch-1 | TACE and Notch1 concentrations were higher in patients with endoleak than in those without endoleak, 6 months after EVAR | [81] |
| Intraluminal thrombus (ILT) | Absence of ILT is a significant predictor of type II endoleak | [82] |
| Serum IL-1-α, IL-1β, IL-4, IL-6, IL-8, IL-10, IFN-γ, IP-10, MCP-1, TNF-α, and TNF-β | Significant decrease of IL-1α, 6 months after EVAR | [83] |
| Aspartate transaminase to platelet ratio index (APRI) | Significant increase in morbidity and mortality in pts with liver fibrosis after EVAR | [84,85] |
| Biomarker/Compound | Biological Effect and Clinical Importance | Reference |
|---|---|---|
| Genetic features | Three genes (MSN, PSMB10, and STIM1) are downregulated in AAA compared with controls. Those genes are involved in: regulation of apoptosis, proteolysis, the electron transport chain, leukocyte migration, and the humoral immune response. | [24] |
| ALOX5, PTGIS, CX3CL1 genes are potentially related with diagnosis of AAA. | [23] | |
| Gene expression profiles allowed to select new potential cytometry markers: CNN1, MYH10, MYOCD, ENG, ICAM2, TEK. | [86] | |
| 120 genes were differentially expressed in AAA. In particular genes associated with inflammatory responses and nuclear-transcribed mRNA catabolic process. The expression levels of IL6 correlated positively with RPL7A and negatively with RPL21. The expression of RPL21 and RPL7A was downregulated, whereas that of IL6 was upregulated in AAA. | [87] | |
| miRNAs | miRNAs are small (19–24 nucleotides) and highly conserved non-coding RNAs involved in gene regulation; are involved in several processes, such as cellular differentiation, apoptosis, or tumorigenesis. | [23] |
| miR-193b-3p, 125b-5p, 150-5p are potentially related with diagnosis of AAA hsa-miR-30a-GNG2 and hsa-miR-15b-ACSS2 interaction pairs may represent novel mechanisms for explaining the pathogenesis of AAA | [88,89,90] | |
| In AAA tissue, six miRNAs (miR-1, miR-27b-3p, miR-29b-3p, miR-133a-3p, miR-133b, and miR-195-5p) were underexpressed from 1.6 to 4.8 times and four miRNAs (miR-146a-5p, miR-21-5p, miR-144-3p, and miR-103a-3p) were overexpressed from 1.3 to 7.2 times, suggesting their involvement in a common regulatory mechanism | [25] | |
| A total of 31 miRNAs and 51 genes were selected as the most promising biomarkers of diagnosis of AAA. | [26,27] | |
| Pentraxin 3 (PTX3) | PTX3 was upregulated in AAA and colocalized with inflammatory infiltrates. | [28] |
| C-reactive protein (CRP)-to-albumin ratio (CAR) | Increased serum CAR was found to be an independent predictor of the presence of AAA | [91] |
| Galectin-1 | Gal-1 is highly induced and contributes to AAA by enhancing matrix degradation activity and inflammatory responses in experimental model; The pathological link between Gal-1 and AAA is also observed in human patients | [29] |
| Galectin-3 | Gal-3 regulates chemotaxis and inflammation; has been reported as a prognostic marker for cardiovascular disease as it is linked to myocardial fibrosis, tissue remodeling, and heart failure development. Circulating Gal-3 levels were significantly correlated with aortic diameter in a concentration-dependent manner. Higher plasma Gal-3 concentrations may be a useful biomarker of AAA progression | [92] |
| Serum calprotectin | Serum calprotectin levels in AAA patients were three times higher than in healthy subjects | [30,31] |
| TLR2, TLR3, TLR4, and TLR9 single-nucleotide polymorphisms (SNPs) | TLRs are type I transmembrane proteins expressed on various immune cells, which recognize molecular patterns unique to pathogens or endogenous molecules released from dying or injured cells Heterozygous genotypes of the TLR2 2029C/T and TLR3 1377C/T and 27C/A SNPs may serve as genetic biomarkers of AAA incidence | [93] |
| Peroxiredoxins (PRDX) | PRDX are a ubiquitous family of thiol- specific antioxidant enzymes that control the levels of intracellular peroxide, which is involved in oxidative stress and signal transduction. PRDX2 plays a role as a negative regulator of the pathological process of AAA | [94] |
| Monomeric form of C-reactive protein (mCRP) | mCRP induces an inflammatory response by monocyte activation and reactive oxygen species formation to exacerbate tissue damage. AAA showed a characteristic deposition of mCRP, and multiple potentially pathologic signaling pathways were upregulated in AAA cases with strong CRP immunopositivity (pathways associated with atherosclerosis, acute phase response, complement system, immune system, and coagulation) | [95] |
| Proteins released by intramural thrombus (ILT) | 3 proteins that are present in ILT, released by ILT and differs between fast and slow growth AAAs. Plasma Attractin correlates significantly with future AAA growth | [71,72] |
| Granzyme K (GZMK) | GZMK, a proinflammatory member of granzyme family, was first discovered in human lymphokine-activated killer cells, and mainly expressed by cytotoxic lymphocytes and monocyte/macrophage cells. infiltrated immune cells in AAA tissues and their associated marker genes: GZMK, CCL5, GZMA, CD2, EOMES, CD247, CD2, CD6, RASGRP1, and CD48 elevated GZMK expression both in serum and tissues is correlated with the presence of AAA, and serum GZMK may be a useful non-invasive marker that helps to identify AAA and its rupture risk | [20,33,96,97] |
| Low molecular weight metabolites | four amino acids (histidine, asparagine, leucine, isoleucine) and four phosphatidylcholines (PC.ae.C34.3, PC.aa.C34.2, PC.ae.C38.0, lysoPC.a.C18.2) were found to be significantly lower after adjustment for confounders among the AAA patients compared with the controls | [98] |
| Dipeptidyl peptidase-4 (DPP4)-inhibitors | Dipeptidyl peptidase-4 (DPP4 a.k.a. CD26) is a serine protease that exists as a membrane bound cell surface peptidase, and as a soluble form in the circulation. DPP4 gene expression is correlated with the expression of genes related to typical AAA processes and the protein was expressed by macro- phages, T-cells, B-cells and SMCs in aneurysm tissue | [99] |
| Long noncoding RNAs (lncRNAs) | lncRNAs have the potential to regulate the expression of genes at the epigenetic, transcriptional, and posttranscriptional levels and play an important role in physiological process. Microarray profile analysis and validation of significantly expressed lncRNA between patients with AAA and the control group | [100] |
| Cystatin B | Growth/differentiation factor 15 and cystatin B had the best ability to discriminate AAA from non-AAA. Higher baseline levels of myeloperoxidase were significantly associated with faster abdominal aortic aneurysm growth | [101] |
| Kallikrein-1 | Serine protease that generates bradykinin, promoting inflammation. Kallikrein-1 blocking antibody reduced levels of cyclooxygenase-2 and secretion of prostaglandin E2 and active matrix metalloproteinase 2 and matrix metalloproteinase 9 from human AAA explants and vascular smooth muscle cells exposed to activated neutrophils | [32] |
| Serum lipid peroxidation products: malondialdehyde (MDA), lipid hydroperoxide (LPO), and glutathione peroxidase (GSH-Px) | the serum MDA and LPO among AAA cases were remarkably increased compared with those from the normal patients. Inversely, serum GSH-Px was significantly decreased in patients with AAA compared to the control group. Moreover, serum MDA level was significantly increased in cases with rupture AAA compared to those in selective AAA cases. Serum MDA may serve as the candidate biomarker for diagnosis of AAA and accurate identification of increased risks of AAA rupture. | [102] |
| Ankle brachial index (ABI) | Logistical regression analysis revealed a statistically significant negative association between initial monophasic posterior tibial artery waveform and abdominal aortic aneurysm presence in patients with ABI > 0.9. | [103] |
| Fibroblast growth factor 21 (FGF21) | FGF21 is a peptide hormone maintaining the homeostasis of glucose, lipid, and energy balance, which belongs to the human FGF superfamily that has crucial roles in a myriad of biological processes. FGF21 was statistically higher in patients with AAA than in control subjects. The protein levels of β-klotho (an essential co-receptor of FGF21) in abdominal aorta of AAA were found significantly lower than in control group. | [104] |
| Biomarker/Compound | Study Type | Biological Effect and In-Vivo Implication | Reference |
|---|---|---|---|
| Neutrophil extracellular traps (NETs), citrullinated histone H3 | mice | citH3 represents a promising AAA biomarker and potential therapeutic target. Inhibitor of citH3 block the AAA progression in mice. | [51] |
| miR-188-5p | mice | Expression of miR-188-5p is increased in experimental AAAs. Treatment with miR-188-5p inhibition limits experimental AAA progression, with histologic evidence of reduced neovessels and attenuated mural leukocyte infiltration. | [54] |
| myeloid related protein 8/14 (MRP8/14) | rat | MRPs especially for MRP8/14 increased the levels of MMP-2 and MMP-9 in rat models. RP8/14 was associated with AAA presence and progression | [105] |
| C1q/tumor necrosis factor (TNF)-related protein-13 (CTRP13) | mice | CTRP13 was shown to effectively reduce the incidence and severity of AAA in conjunction with reduced aortic macrophage infiltration, expression of proinflammatory cytokines (interleukin-6 [IL-6], TNF-α, and monocyte chemoattractant protein 1 [MCP-1]), and vascular smooth muscle cell (SMC) apoptosis. Mechanistically, nicotinamide phosphoribosyl-transferase 1 (NAMPT1) was identified as a new target of CTRP13. NAMPT1 knockdown blocked the beneficial effects of CTRP13 on vascular inflammation and SMC apoptosis. CTRP13 management may be an effective treatment for preventing AAA formation | [106] |
| Differentially expressed genes (DEGs) of proteases | mice | 43 DEGs were correlated with the expression of the protease profile, and most were clustered in immune response module. Mmp16 and Mmp17 were significantly downregulated in AAA mice, while Ctsa, Ctsc, and Ctsw were upregulated. that these ectopic genes are potentially crucial to AAA formation and may act as biomarkers for the diagnosis of AAA. | [107] |
| microRNAs (miRNAs) miR-29a-3p, phosphatase and tensin homolog (PTEN) | mice | Increased expression of miRNA-29a-3p found in AAA-mimic cells with increased cellular viability and significant pathological apoptosis. Further, when the expression of miRNA-29a-3p was downregulated, it reduced the cell viability of AAA cells. PTEN was directly targeted by miRNA-29a-3p so as to regulate the AAA progression. Thus, PTEN was found to strengthen the proliferation effect of miRNA-29a-3p in AAA cells. | [52] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stilo, F.; Catanese, V.; Nenna, A.; Montelione, N.; Codispoti, F.A.; Verghi, E.; Gabellini, T.; Jawabra, M.; Chello, M.; Spinelli, F. Biomarkers in EndoVascular Aneurysm Repair (EVAR) and Abdominal Aortic Aneurysm: Pathophysiology and Clinical Implications. Diagnostics 2022, 12, 183. https://doi.org/10.3390/diagnostics12010183
Stilo F, Catanese V, Nenna A, Montelione N, Codispoti FA, Verghi E, Gabellini T, Jawabra M, Chello M, Spinelli F. Biomarkers in EndoVascular Aneurysm Repair (EVAR) and Abdominal Aortic Aneurysm: Pathophysiology and Clinical Implications. Diagnostics. 2022; 12(1):183. https://doi.org/10.3390/diagnostics12010183
Chicago/Turabian StyleStilo, Francesco, Vincenzo Catanese, Antonio Nenna, Nunzio Montelione, Francesco Alberto Codispoti, Emanuele Verghi, Teresa Gabellini, Mohamad Jawabra, Massimo Chello, and Francesco Spinelli. 2022. "Biomarkers in EndoVascular Aneurysm Repair (EVAR) and Abdominal Aortic Aneurysm: Pathophysiology and Clinical Implications" Diagnostics 12, no. 1: 183. https://doi.org/10.3390/diagnostics12010183
APA StyleStilo, F., Catanese, V., Nenna, A., Montelione, N., Codispoti, F. A., Verghi, E., Gabellini, T., Jawabra, M., Chello, M., & Spinelli, F. (2022). Biomarkers in EndoVascular Aneurysm Repair (EVAR) and Abdominal Aortic Aneurysm: Pathophysiology and Clinical Implications. Diagnostics, 12(1), 183. https://doi.org/10.3390/diagnostics12010183