
Preliminary Clinical Experience with a Novel Optical–Ultrasound Imaging Device on Various Skin Lesions


 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
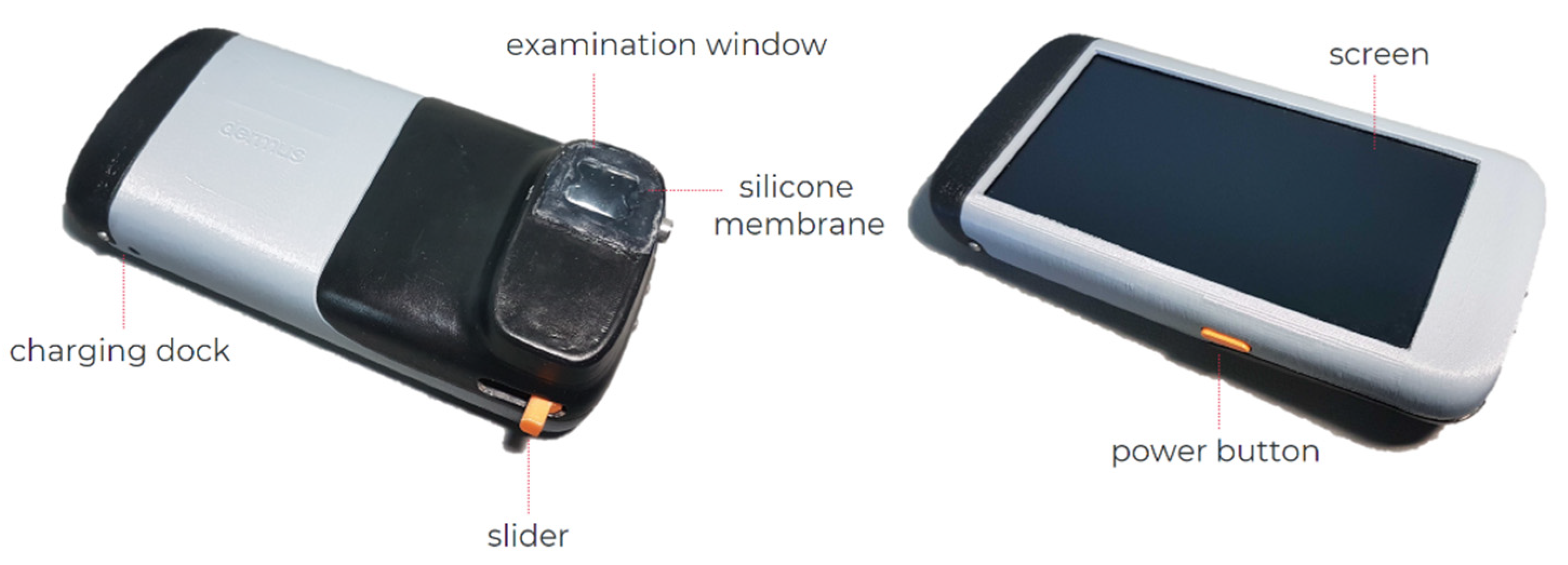
2.1. The Dermus SkinScanner Device
2.2. Study Design
2.2.1. Study Population
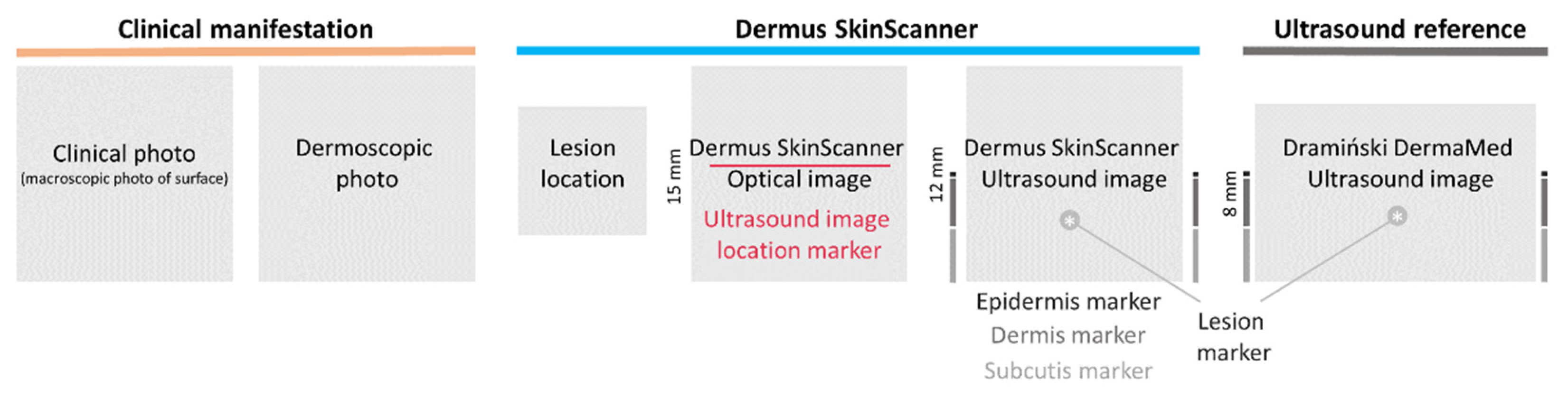
2.2.2. Data Acquisition
2.2.3. Evaluation of Skin Structure Detectability
3. Results
3.1. Skin Structure Detectability
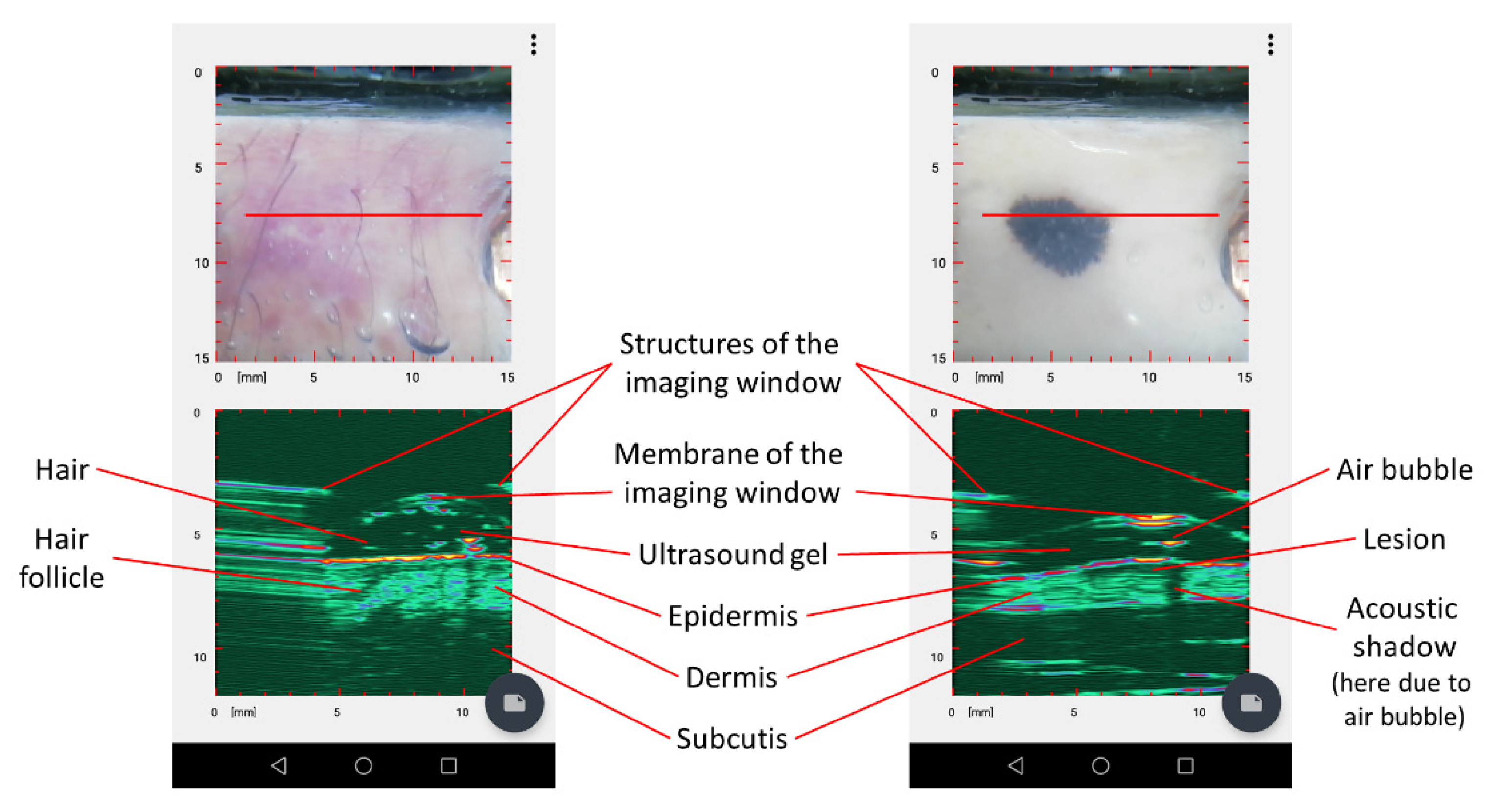
3.2. Dermus SkinScanner Ultrasound Image Interpretation
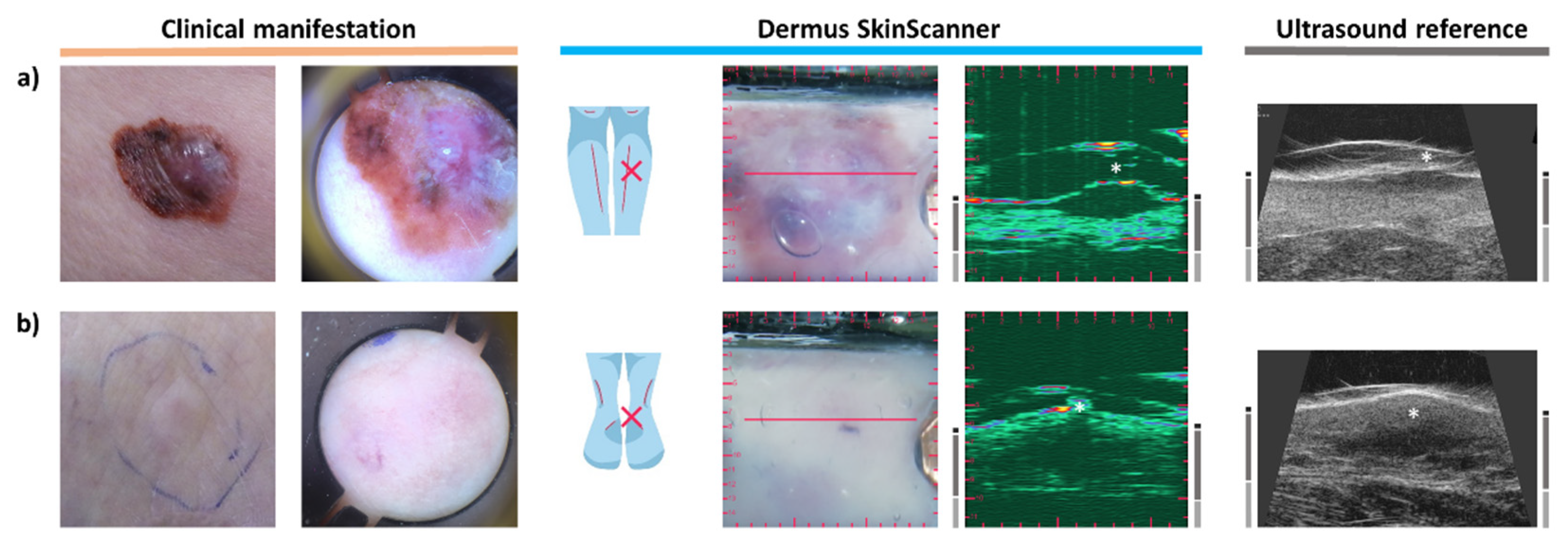
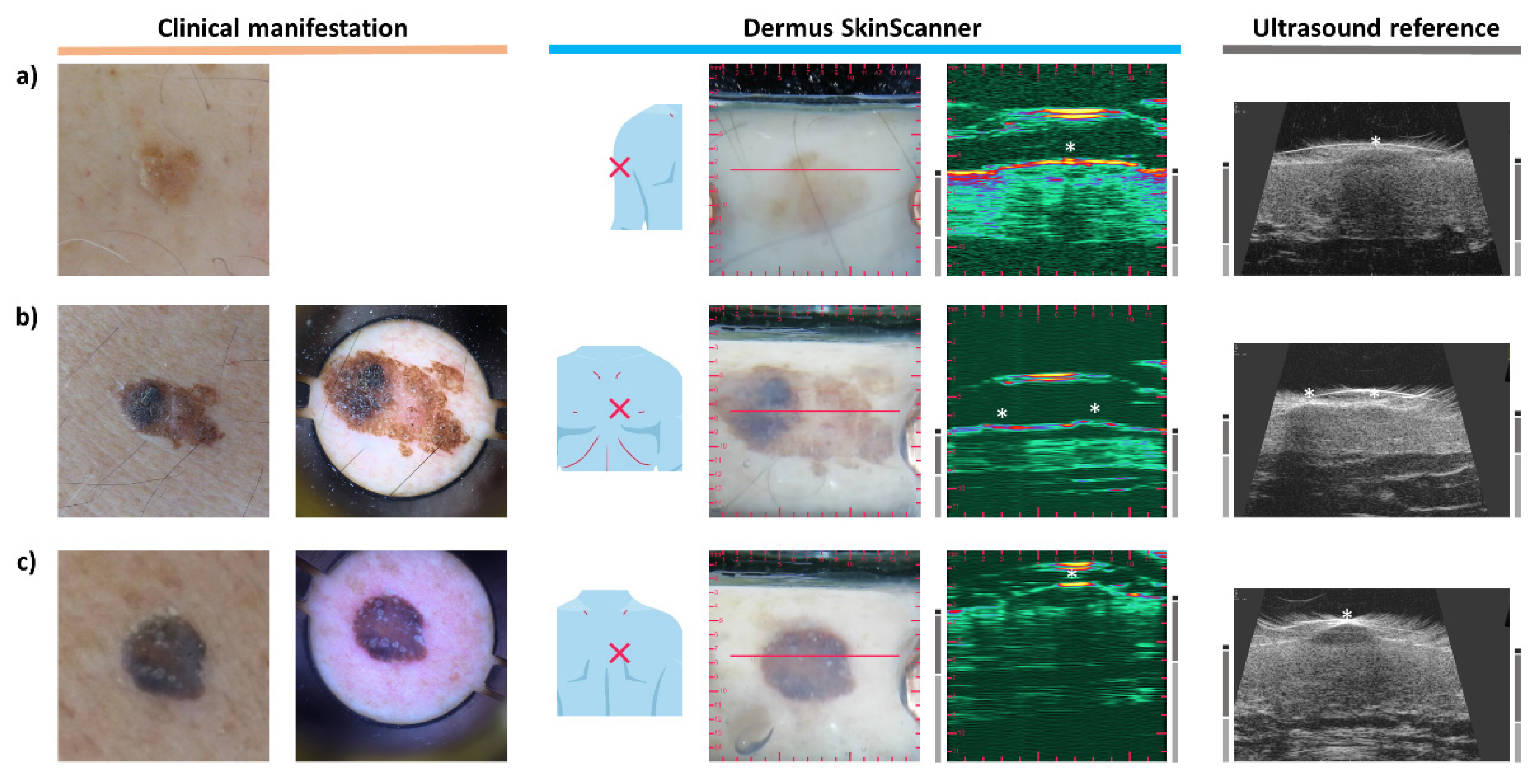
3.3. Melanoma
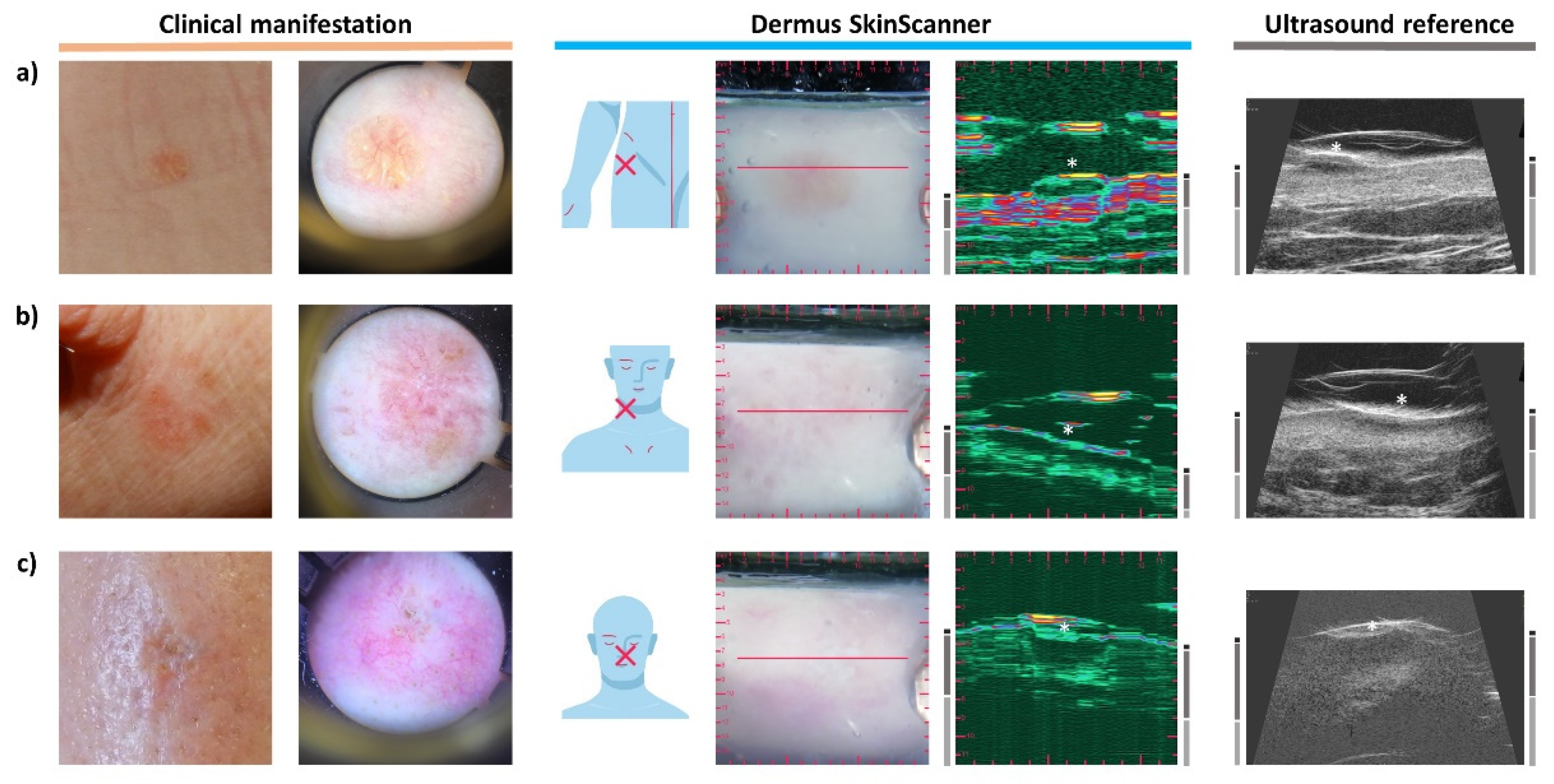
3.4. Basal Cell Carcinoma
3.5. Seborrheic Keratosis
3.6. Dermatofibroma
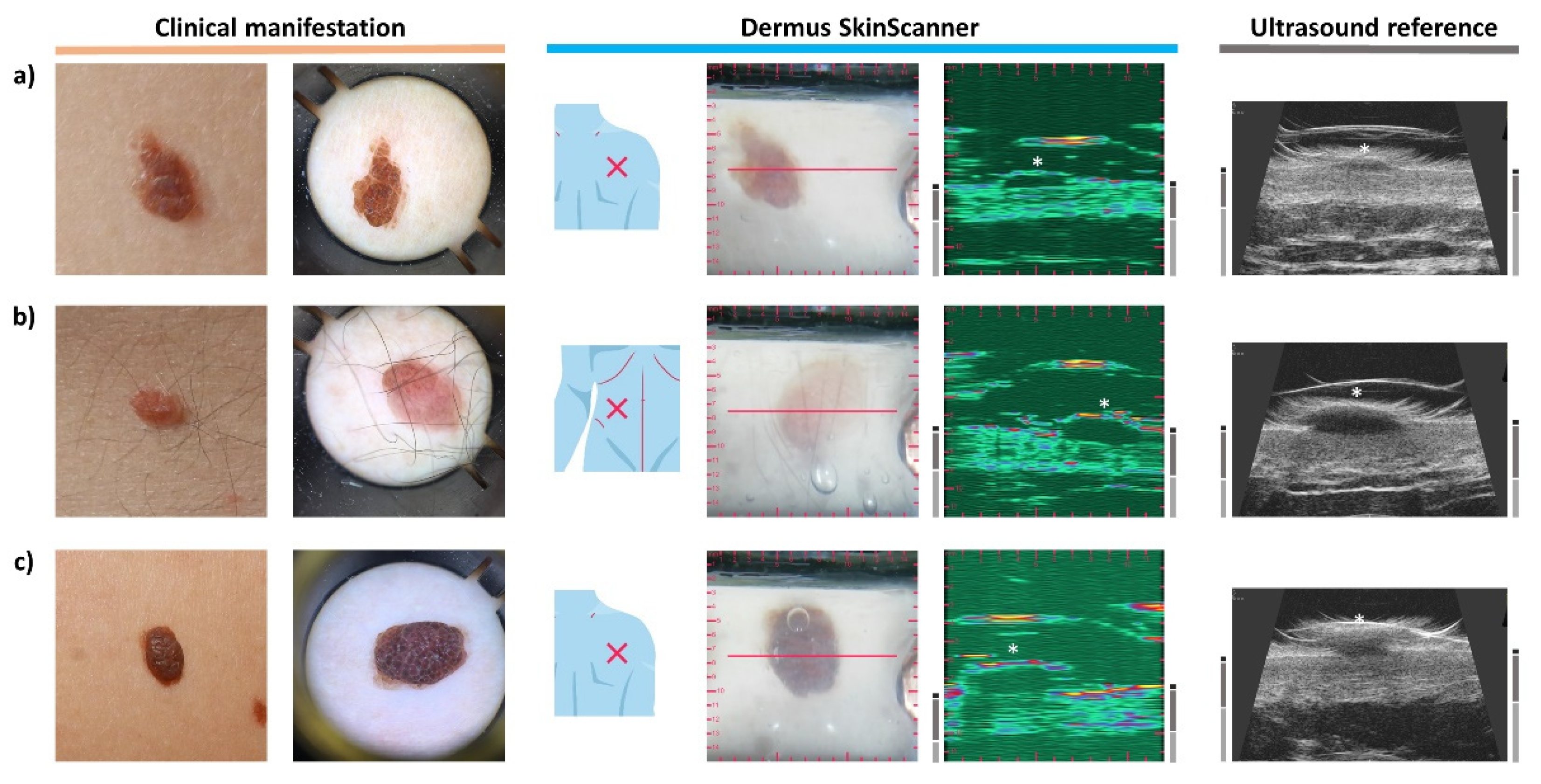
3.7. Naevus
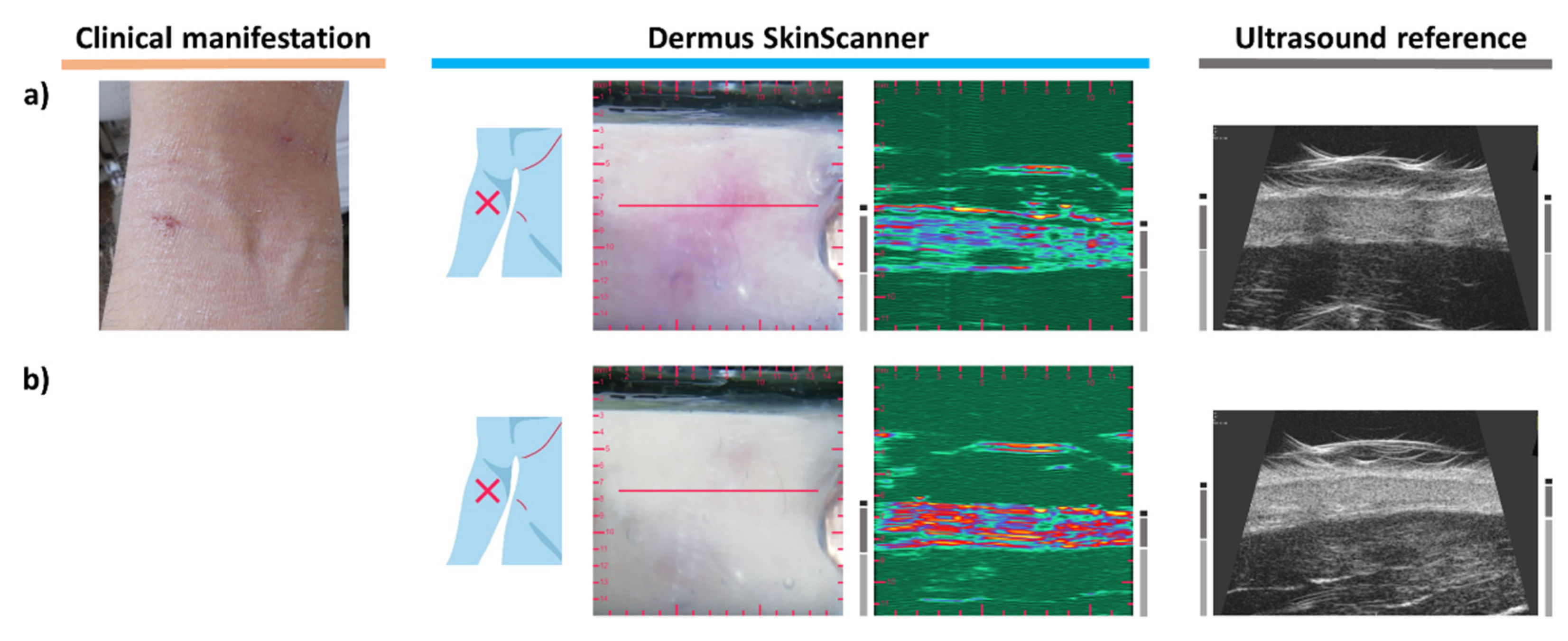
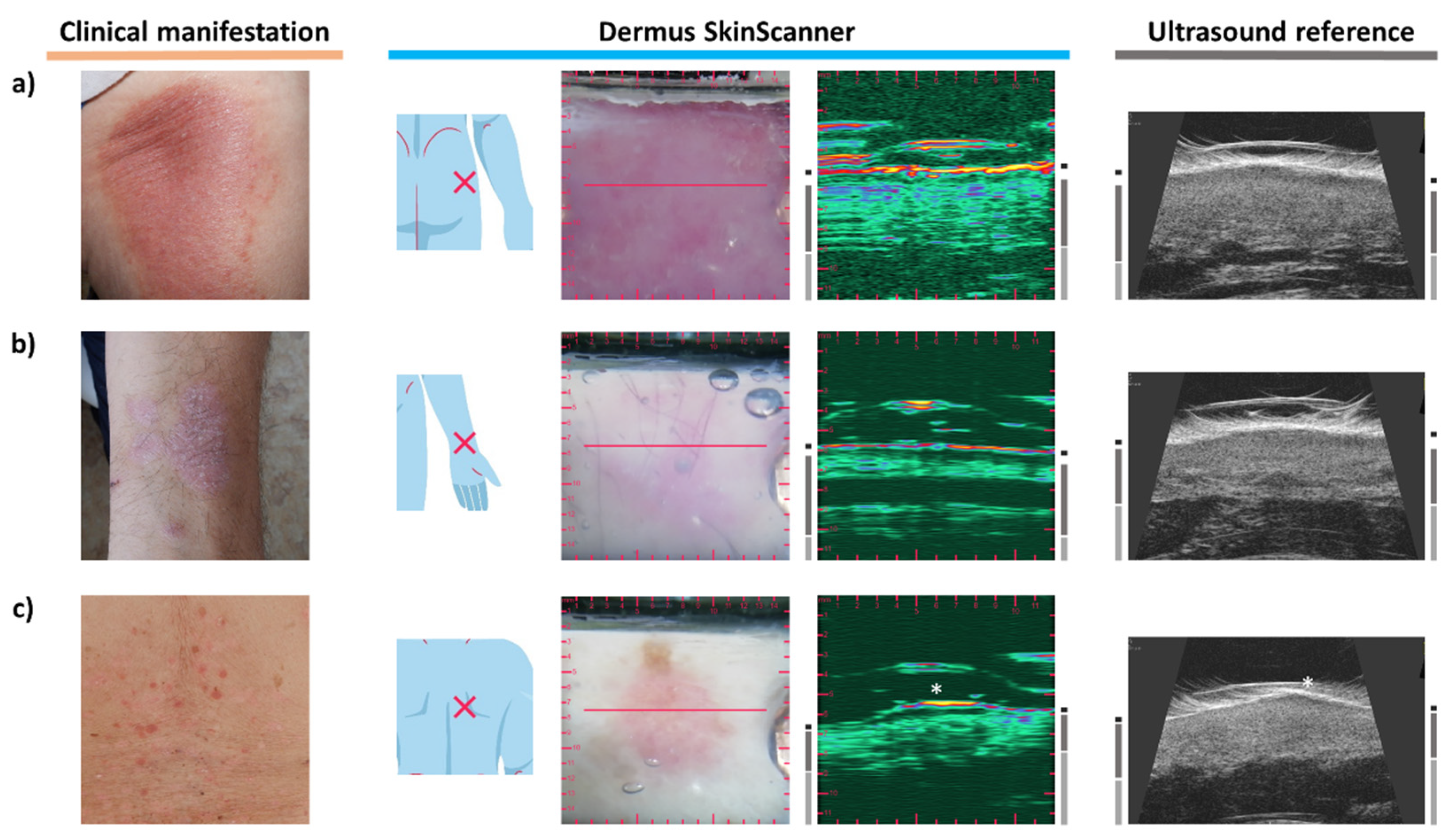
3.8. Dermatitis
3.9. Psoriasis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wilhelm, K.P.; Elsner, P.; Berardesca, E.; Maibach, H.I. (Eds.) Bioengineering of the Skin: Skin Imaging & Analysis, 2nd ed.; CRC Press: Boca Raton, FL, USA, 2006. [Google Scholar]
- Wortsman, X.; Jemec, G. (Eds.) Dermatologic Ultrasound with Clinical and Histologic Correlations; Springer Science & Business Media: New York, NY, USA, 2013; pp. 39–586. [Google Scholar]
- Skin Cancer Foundation: Skin Cancer Facts & Statistics. Available online: https://www.skincancer.org/skin-cancer-information/skin-cancer-facts/ (accessed on 16 June 2021).
- Rigel, D.S.; Carucci, J.A. Malignant melanoma: Prevention, early detection, and treatment in the 21st century. CA Cancer J. Clin. 2000, 50, 215–236. [Google Scholar] [CrossRef] [PubMed]
- Hanifin, J.M.; Reed, M.L.; Prevalence, E.; Impact Working Group. A population-based survey of eczema prevalence in the United States. Dermatitis 2007, 18, 82–91. [Google Scholar] [CrossRef]
- Abuabara, K.; Magyari, A.; McCulloch, C.E.; Linos, E.; Margolis, D.J.; Langan, S.M. Prevalence of atopic eczema among patients seen in primary care: Data from the Health Improvement Network. Ann. Intern. Med. 2019, 170, 354–356. [Google Scholar] [CrossRef]
- Fuxench, Z.C.; Block, J.K.; Boguniewicz, M.; Boyle, J.; Fonacier, L.; Gelfand, J.M.; Grayson, M.H.; Margolis, D.J.; Mitchell, L.; Silverberg, J.I.; et al. Atopic Dermatitis in America Study: A cross-sectional study examining the prevalence and disease burden of atopic dermatitis in the US adult population. J. Investig. Dermatol. 2019, 139, 583–590. [Google Scholar] [CrossRef] [Green Version]
- Kardynal, A.; Olszewska, M. Modern non-invasive diagnostic techniques in the detection of early cutaneous melanoma. J. Dermatol. Case Rep. 2014, 8, 1. [Google Scholar] [CrossRef] [Green Version]
- Botar-Jid, C.M.; Cosgarea, R.; Bolboacă, S.D.; Şenilă, S.C.; Lenghel, L.M.; Rogojan, L.; Dudea, S.M. Assessment of cutaneous melanoma by use of very-high-frequency ultrasound and real-time elastography. Am. J. Roentgenol. 2016, 206, 699–704. [Google Scholar] [CrossRef]
- Polańska, A.; Dańczak-Pazdrowska, A.; Silny, W.; Woźniak, A.; Maksin, K.; Jenerowicz, D.; Janicka-Jedyńska, M. Comparison between high-frequency ultrasonography (Dermascan C, version 3) and histopathology in atopic dermatitis. Ski. Res. Technol. 2013, 19, 432–437. [Google Scholar] [CrossRef]
- Dańczak-Pazdrowska, A.; Polańska, A.; Silny, W.; Sadowska, A.; Osmola-Mańkowska, A.; Czarnecka-Operacz, M.; Żaba, R.; Jenerowicz, D. Seemingly healthy skin in atopic dermatitis: Observations with the use of high-frequency ultrasonography, preliminary study. Ski. Res. Technol. 2012, 18, 162–167. [Google Scholar] [CrossRef] [PubMed]
- Polańska, A.; Silny, W.; Jenerowicz, D.; Knioła, K.; Molińska-Glura, M.; Dańczak-Pazdrowska, A. Monitoring of therapy in atopic dermatitis–observations with the use of high-frequency ultrasonography. Ski. Res. Technol. 2015, 21, 35–40. [Google Scholar] [CrossRef]
- Grajdeanu, I.A.; Statescu, L.; Vata, D.; Popescu, I.A.; Porumb-Andrese, E.; Patrascu, A.I.; Taranu, T.; Crisan, M.; Solovastru, L.G. Imaging techniques in the diagnosis and monitoring of psoriasis. Exp. Ther. Med. 2019, 18, 4974–4980. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tiwari, K.A.; Raišutis, R.; Liutkus, J.; Valiukevičienė, S. Diagnostics of melanocytic skin tumours by a combination of ultrasonic, dermatoscopic and spectrophotometric image parameters. Diagnostics 2020, 10, 632. [Google Scholar] [CrossRef] [PubMed]
- Dinnes, J.; Bamber, J.; Chuchu, N.; Bayliss, S.E.; Takwoingi, Y.; Davenport, C.; Godfrey, K.; O’Sullivan, C.; Matin, R.N.; Deeks, J.J.; et al. High-frequency ultrasound for diagnosing skin cancer in adults. Cochrane Database Syst. Rev. 2018, 12, 1–96. [Google Scholar] [CrossRef]
- Schneider, S.L.; Kohli, I.; Hamzavi, I.H.; Council, M.L.; Rossi, A.M.; Ozog, D.M. Emerging imaging technologies in dermatology: Part I: Basic principles. J. Am. Acad. Dermatol. 2019, 80, 1114–1120. [Google Scholar] [CrossRef]
- Rigel, D.S.; Russak, J.; Friedman, R. The evolution of melanoma diagnosis: 25 years beyond the ABCDs. CA Cancer J. Clin. 2010, 60, 301–316. [Google Scholar] [CrossRef]
- Schneider, S.L.; Kohli, I.; Hamzavi, I.H.; Council, M.L.; Rossi, A.M.; Ozog, D.M. Emerging imaging technologies in dermatology: Part II: Applications and limitations. J. Am. Acad. Dermatol. 2019, 80, 1121–1131. [Google Scholar] [CrossRef]
- Szalai, K.; Hatvani, Z.; Hársing, J.; Somlai, B.; Kárpáti, S. CO07. High frequency ultrasonography in the diagnosis of cutaneous pigmented lesions and melanoma reduce the possibilities of diagnostic pitfalls. Melanoma Res. 2011, 21, e4–e5. [Google Scholar] [CrossRef]
- Hernandez-Ibanez, C.; Blazquez-Sanchez, N.; Aguilar-Bernier, M.; Fúnez-Liébana, R.; Rivas-Ruiz, F.; de Troya-Martin, M. Usefulness of high-frequency ultrasound in the classification of histologic subtypes of primary basal cell carcinoma. Actas Dermo-Sifiliográficas 2017, 108, 42–51. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira Barcaui, E.; Carvalho, A.C.; Valiante, P.M.; Barcaui, C.B. High-frequency ultrasound associated with dermoscopy in pre-operative evaluation of basal cell carcinoma. An. Bras. Dermatol. 2014, 89, 828. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alfageme, F.; Wortsman, X.; Catalano, O.; Roustan, G.; Crisan, M.; Crisan, D.; Gaitini, D.E.; Cerezo, E.; Badea, R. European Federation of Societies for Ultrasound in Medicine and Biology (EFSUMB) position statement on dermatologic ultrasound. Ultraschall Der Med. Eur. J. Ultrasound 2021, 42, 39–47. [Google Scholar] [CrossRef]
- Kimball, A.B.; Resneck, J.S., Jr. The US dermatology workforce: A specialty remains in shortage. J. Am. Acad. Dermatol. 2008, 59, 741–745. [Google Scholar] [CrossRef]
- Csány, G.; Szalai, K.; Füzesi, K.; Gyöngy, M. A low-cost portable ultrasound system for skin diagnosis. In Proceedings of Meetings on Acoustics 6ICU; Acoustical Society of America: Melville, NY, USA, 2017; Volume 32, p. 020002. [Google Scholar]
- Mlosek, R.K.; Migda, B.; Migda, M. High-frequency ultrasound in the 21st century. J. Ultrason. 2021, 20, e233. [Google Scholar] [CrossRef]
- Sciolla, B.; Le Digabel, J.; Josse, G.; Dambry, T.; Guibert, B.; Delachartre, P. Joint segmentation and characterization of the dermis in 50 MHz ultrasound 2D and 3D images of the skin. Comput. Biol. Med. 2018, 103, 277–286. [Google Scholar] [CrossRef]
- Stephens, K. Clarius Introduces First Ultra-High-Frequency Handheld Ultrasound Scanner; AXIS Imaging News: Overland Park, KS, USA, 2020. [Google Scholar]
- Przybysz, P.; Jackowska, T.; Wilińska, M.; Malinowska, S.; Wójtowicz, J.; Mlosek, R.K. Ultrasound image of healthy skin in newborns in the first 24 hours of life. J. Ultrason. 2021, 20, e242. [Google Scholar] [CrossRef]
- Chirikhina, E.; Chirikhin, A.; Dewsbury-Ennis, S.; Bianconi, F.; Xiao, P. Skin Characterizations by Using Contact Capacitive Imaging and High-Resolution Ultrasound Imaging with Machine Learning Algorithms. Appl. Sci. 2021, 11, 8714. [Google Scholar] [CrossRef]
- Chirikhina, E.; Chirikhin, A.; Xiao, P.; Dewsbury-Ennis, S.; Bianconi, F. In Vivo Assessment of Water Content, Trans-Epidermial Water Loss and Thickness in Human Facial Skin. Appl. Sci. 2020, 10, 6139. [Google Scholar] [CrossRef]
- Reginelli, A.; Belfiore, M.P.; Russo, A.; Turriziani, F.; Moscarella, E.; Troiani, T.; Brancaccio, G.; Ronchi, A.; Giunta, E.; Sica, A.; et al. A preliminary study for quantitative assessment with HFUS (High-Frequency Ultrasound) of nodular skin melanoma breslow thickness in adults before surgery: Interdisciplinary team experience. Curr. Radiopharm. 2020, 13, 48–55. [Google Scholar] [CrossRef]
- Gyöngy, M.; Csány, G. Method for Generating Ultrasound Image and Computer Readable Medium. U.S. Patent No. 10,928,515, 23 February 2021. [Google Scholar]
- Csány, G.; Szalai, K.; Gyöngy, M. A real-time data-based scan conversion method for single element ultrasound transducers. Ultrasonics 2019, 93, 26–36. [Google Scholar] [CrossRef] [PubMed]
- Ahn, S.; Park, S.H.; Lee, K.H. How to demonstrate similarity by using noninferiority and equivalence statistical testing in radiology research. Radiology 2013, 267, 328–338. [Google Scholar] [CrossRef] [PubMed]
- Gambichler, T.; Moussa, G.; Bahrenberg, K.; Vogt, M.; Ermert, H.; Weyhe, D.; Altmeyer, P.; Hoffmann, K. Preoperative ultrasonic assessment of thin melanocytic skin lesions using a 100-MHz ultrasound transducer: A comparative study. Dermatol. Surg. 2007, 33, 818–824. [Google Scholar]
- Grajdeanu, I.A.; Vata, D.; Statescu, L.; Popescu, I.A.; Porumb-Andrese, E.; Patrascu, A.I.; Stincanu, A.; Taranu, T.; Crisan, M.; Solovastru, L.G. Use of imaging techniques for melanocytic naevi and basal cell carcinoma in integrative analysis. Exp. Ther. Med. 2020, 20, 78–86. [Google Scholar] [CrossRef] [PubMed]
- Szalai, K.; Hatvani, Z.; Artner, A.; Toth, K.; Harsing, J.; Karpati, S. Significance of ultrasound morphologic evaluation of basocellular cancers from the viewpoint of the therapeutic modalities and followup procedures. J. Investig. Dermatol. 2012, 132, S54. [Google Scholar]
- Wortsman, X.; Bouer, M. Common benign non-vascular skin tumors. In Dermatologic Ultrasound with Clinical and Histologic Correlations; Wortsman, X., Jemec, G., Eds.; Springer Science & Business Media: New York, NY, USA, 2013; pp. 119–175. [Google Scholar]
- Sorokina, E.; Mikailova, D.; Krakhaleva, J.; Krinitsyna, J.; Yakubovich, A.; Sergeeva, I. Ultrasonography patterns of atopic dermatitis in children. Ski. Res. Technol. 2020, 26, 482–488. [Google Scholar] [CrossRef] [PubMed]
- Lacarrubba, F.; Pellacani, G.; Gurgone, S.; Verzì, A.E.; Micali, G. Advances in non-invasive techniques as aids to the diagnosis and monitoring of therapeutic response in plaque psoriasis: A review. Int. J. Dermatol. 2015, 54, 626–634. [Google Scholar] [CrossRef] [PubMed]
- Șomlea, M.C.; Boca, A.N.; Pop, A.D.; Ilieș, R.F.; Vesa, S.C.; Buzoianu, A.D.; Tătaru, A. High-frequency ultrasonography of psoriatic skin: A non-invasive technique in the evaluation of the entire skin of patients with psoriasis: A pilot study. Exp. Ther. Med. 2019, 18, 4981–4986. [Google Scholar] [CrossRef] [PubMed]
- Catalano, O.; Roldán, F.A.; Varelli, C.; Bard, R.; Corvino, A.; Wortsman, X. Skin cancer: Findings and role of high-resolution ultrasound. J. Ultrasound 2019, 22, 423–431. [Google Scholar] [CrossRef] [PubMed]
- Einstien, A.; Rangari, A.P.; Kumar, M.J.; Einstien, D. High Resolution Ultrasound in Cutaneous and Subcutaneous Lesions. Int. J. Contemp. Med. Surg. Radiol. 2018, 3, D66–D70. [Google Scholar] [CrossRef]
- Wortsman, X. Sonography of the primary cutaneous melanoma: A review. Radiol. Res. Pract. 2012, 2012, 814396. [Google Scholar] [CrossRef] [Green Version]
- Wortsman, X.; Carreño, L.; Morales, C. Skin cancer: The primary tumors. In Dermatologic Ultrasound with Clinical and Histologic Correlations; Wortsman, X., Jemec, G., Eds.; Springer Science & Business Media: New York, NY, USA, 2013; pp. 249–282. [Google Scholar]
- Bard, R.L. (Ed.) Image Guided Dermatologic Treatments; Springer Nature: New York, NY, USA, 2019. [Google Scholar]
- Polańska, A.; Dańczak-Pazdrowska, A.; Jałowska, M.; Żaba, R.; Adamski, Z. Current applications of high-frequency ultrasonography in dermatology. Adv. Dermatol. Allergol. Postȩpy Dermatol. I Alergol. 2017, 34, 535. [Google Scholar] [CrossRef]
- Goyal, U.; Pan, J.; Cui, H.; Stea, B. Does ultrasound measurement improve the accuracy of electronic brachytherapy in the treatment of superficial non-melanomatous skin cancer? J. Contemp. Brachyther. 2017, 9, 14. [Google Scholar] [CrossRef] [Green Version]
- Harland, C.C.; Kale, S.G.; Jackson, P.; Mortimer, P.S.; Bamber, J.C. Differentiation of common benign pigmented skin lesions from melanoma by high-resolution ultrasound. Br. J. Dermatol. 2000, 143, 281–289. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez, M.; Wortsman, X.; Filippucci, E.; De Angelis, R.; Filosa, G.; Grassi, W. High-frequency sonography in the evaluation of psoriasis: Nail and skin involvement. J. Ultrasound Med. 2009, 28, 1569–1574. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez, M.; Filippucci, E.; Bertolazzi, C.; Grassi, W. Sonographic monitoring of psoriatic plaque. J. Rheumatol. 2009, 36, 850–851. [Google Scholar] [CrossRef] [PubMed] [Green Version]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dermus SkinScanner | Reference Device (Dramiński DermaMed) | |||||
|---|---|---|---|---|---|---|
| A 1 | B 2 | C 3 | A 1 | B 2 | C 3 | |
| Lesion | 95% | 91% | 91% | 94% | 87% | 94% |
| Epidermis | 96% | 98% | 92% | 96% | 100% | 97% |
| Dermis | 96% | 91% | 96% | 94% | 96% | 96% |
| Subcutis | 94% | 85% | 91% | 94% | 92% | 96% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Csány, G.; Gergely, L.H.; Kiss, N.; Szalai, K.; Lőrincz, K.; Strobel, L.; Csabai, D.; Hegedüs, I.; Marosán-Vilimszky, P.; Füzesi, K.; et al. Preliminary Clinical Experience with a Novel Optical–Ultrasound Imaging Device on Various Skin Lesions. Diagnostics 2022, 12, 204. https://doi.org/10.3390/diagnostics12010204
Csány G, Gergely LH, Kiss N, Szalai K, Lőrincz K, Strobel L, Csabai D, Hegedüs I, Marosán-Vilimszky P, Füzesi K, et al. Preliminary Clinical Experience with a Novel Optical–Ultrasound Imaging Device on Various Skin Lesions. Diagnostics. 2022; 12(1):204. https://doi.org/10.3390/diagnostics12010204
Chicago/Turabian StyleCsány, Gergely, László Hunor Gergely, Norbert Kiss, Klára Szalai, Kende Lőrincz, Lilla Strobel, Domonkos Csabai, István Hegedüs, Péter Marosán-Vilimszky, Krisztián Füzesi, and et al. 2022. "Preliminary Clinical Experience with a Novel Optical–Ultrasound Imaging Device on Various Skin Lesions" Diagnostics 12, no. 1: 204. https://doi.org/10.3390/diagnostics12010204
APA StyleCsány, G., Gergely, L. H., Kiss, N., Szalai, K., Lőrincz, K., Strobel, L., Csabai, D., Hegedüs, I., Marosán-Vilimszky, P., Füzesi, K., Sárdy, M., & Gyöngy, M. (2022). Preliminary Clinical Experience with a Novel Optical–Ultrasound Imaging Device on Various Skin Lesions. Diagnostics, 12(1), 204. https://doi.org/10.3390/diagnostics12010204