
Applying Compressed Sensing Volumetric Interpolated Breath-Hold Examination and Spiral Ultrashort Echo Time Sequences for Lung Nodule Detection in MRI

 ,
,
Abstract
:1. Introduction
- The pulmonary nodules detected by the imaging modalities, including CT and MRI, were scheduled for VATS resection, and pathology correlation (malignant vs. non-malignant) of the nodules was performed.
- Both UTE and CS-VIBE sequences provide radiation-free pulmonary nodule detection, which is suitable for young people, pregnant women, patients requiring serial and longitudinal follow-up, or people unwilling to undergo radiation exposure.
- Variable respiratory motion management (breath-hold for CS-VIBE with scanning durations of 13 s vs. free-breathing for spiral UTE with scanning durations of 3.5–5 min) was investigated.
2. Materials and Methods
2.1. Study Design
2.2. MRI Acquisition
2.3. CT Examinations
2.4. Image Analysis
2.5. Statistical Analysis
3. Results
3.1. Patient and Nodule Characteristics
3.2. Qualitative Assessment of Normal Structures and Nodules
3.3. Quantitative Assessment by SNR and CNR
3.4. Evaluation of Nodule Detection Sensitivity
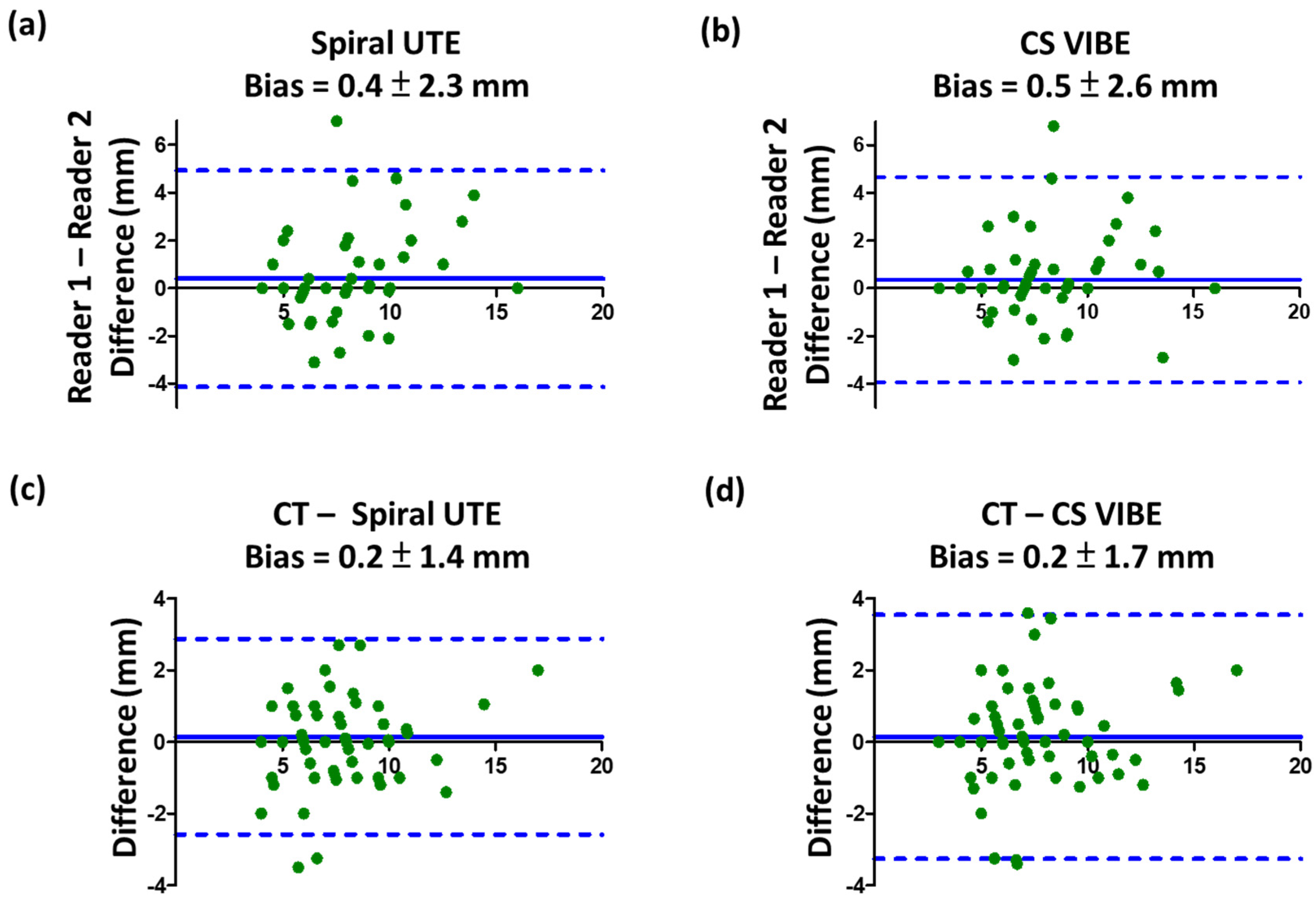
3.5. Inter-Reader and Inter-Modality Reliability Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- McWilliams, A.; Tammemagi, M.C.; Mayo, J.R.; Roberts, H.; Liu, G.; Soghrati, K.; Yasufuku, K.; Martel, S.; Laberge, F.; Gingras, M.; et al. Probability of cancer in pulmonary nodules detected on first screening CT. N. Engl. J. Med. 2013, 369, 910–919. [Google Scholar] [CrossRef] [Green Version]
- Huang, Y.S.; Hsu, H.H.; Chen, J.Y.; Tai, M.H.; Jaw, F.S.; Chang, Y.C. Quantitative computed tomography of pulmonary emphysema and ventricular function in chronic obstructive pulmonary disease patients with pulmonary hypertension. Korean J. Radiol. 2014, 15, 871–877. [Google Scholar] [CrossRef] [Green Version]
- Libby, D.M.; Smith, J.P.; Altorki, N.K.; Pasmantier, M.W.; Yankelevitz, D.; Henschke, C.I. Managing the small pulmonary nodule discovered by CT. Chest 2004, 125, 1522–1529. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swensen, S.J.; Jett, J.R.; Hartman, T.E.; Midthun, D.E.; Mandrekar, S.J.; Hillman, S.L.; Sykes, A.M.; Aughenbaugh, G.L.; Bungum, A.O.; Allen, K.L. CT screening for lung cancer: Five-year prospective experience. Radiology 2005, 235, 259–265. [Google Scholar] [CrossRef] [PubMed]
- McCunney, R.J.; Li, J. Radiation risks in lung cancer screening programs: A comparison with nuclear industry workers and atomic bomb survivors. Chest 2014, 145, 618–624. [Google Scholar] [CrossRef]
- Biederer, J.; Hintze, C.; Fabel, M. MRI of pulmonary nodules: Technique and diagnostic value. Cancer Imaging Off. Publ. Int. Cancer Imaging Soc. 2008, 8, 125–130. [Google Scholar] [CrossRef]
- Kurihara, Y.; Matsuoka, S.; Yamashiro, T.; Fujikawa, A.; Matsushita, S.; Yagihashi, K.; Nakajima, Y. MRI of pulmonary nodules. Am. J. Roentgenol. 2014, 202, W210–W216. [Google Scholar] [CrossRef] [PubMed]
- Dewes, P.; Frellesen, C.; Al-Butmeh, F.; Albrecht, M.H.; Scholtz, J.E.; Metzger, S.C.; Lehnert, T.; Vogl, T.J.; Wichmann, J.L. Comparative evaluation of non-contrast CAIPIRINHA-VIBE 3T-MRI and multidetector CT for detection of pulmonary nodules: In vivo evaluation of diagnostic accuracy and image quality. Eur. J. Radiol. 2016, 85, 193–198. [Google Scholar] [CrossRef]
- Hargreaves, B.A.; Saranathan, M.; Sung, K.; Daniel, B.L. Accelerated breast MRI with compressed sensing. Eur. J. Radiol. 2012, 81 (Suppl. S1), S54–S55. [Google Scholar] [CrossRef]
- Sun, W.; Wang, W.; Zhu, K.; Chen, C.Z.; Wen, X.X.; Zeng, M.S.; Rao, S.X. Feasibility of compressed sensing technique for isotropic dynamic contrast-enhanced liver magnetic resonance imaging. Eur. J. Radiol. 2021, 139, 109729. [Google Scholar] [CrossRef] [PubMed]
- Yoon, J.H.; Nickel, M.D.; Peeters, J.M.; Lee, J.M. Rapid Imaging: Recent Advances in Abdominal MRI for Reducing Acquisition Time and Its Clinical Applications. Korean J. Radiol. 2019, 20, 1597–1615. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collier, G.J.; Wild, J.M. In vivo measurement of gas flow in human airways with hyperpolarized gas MRI and compressed sensing. Magn. Reson. Med. 2015, 73, 2255–2261. [Google Scholar] [CrossRef] [Green Version]
- Yip, E.; Yun, J.; Wachowicz, K.; Heikal, A.A.; Gabos, Z.; Rathee, S.; Fallone, B.G. Prior data assisted compressed sensing: A novel MR imaging strategy for real time tracking of lung tumors. Med. Phys. 2014, 41, 082301. [Google Scholar] [CrossRef] [PubMed]
- Cha, M.J.; Park, H.J.; Paek, M.Y.; Stemmer, A.; Lee, E.S.; Park, S.B.; Kim, Y.S. Free-breathing ultrashort echo time lung magnetic resonance imaging using stack-of-spirals acquisition: A feasibility study in oncology patients. Magn. Reson. Imaging 2018, 51, 137–143. [Google Scholar] [CrossRef]
- Bae, K.; Jeon, K.N.; Hwang, M.J.; Lee, J.S.; Ha, J.Y.; Ryu, K.H.; Kim, H.C. Comparison of lung imaging using three-dimensional ultrashort echo time and zero echo time sequences: Preliminary study. Eur. Radiol. 2019, 29, 2253–2262. [Google Scholar] [CrossRef] [PubMed]
- Burris, N.S.; Johnson, K.M.; Larson, P.E.; Hope, M.D.; Nagle, S.K.; Behr, S.C.; Hope, T.A. Detection of Small Pulmonary Nodules with Ultrashort Echo Time Sequences in Oncology Patients by Using a PET/MR System. Radiology 2016, 278, 239–246. [Google Scholar] [CrossRef]
- Yu, N.; Yang, C.; Ma, G.; Dang, S.; Ren, Z.; Wang, S.; Yu, Y. Feasibility of pulmonary MRI for nodule detection in comparison to computed tomography. BMC Med. Imaging 2020, 20, 53. [Google Scholar] [CrossRef]
- Lin, M.W.; Tseng, Y.H.; Lee, Y.F.; Hsieh, M.S.; Ko, W.C.; Chen, J.Y.; Hsu, H.H.; Chang, Y.C.; Chen, J.S. Computed tomography-guided patent blue vital dye localization of pulmonary nodules in uniportal thoracoscopy. J. Thorac. Cardiovasc. Surg. 2016, 152, 535–544.e532. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.R.; Tseng, Y.H.; Lin, M.W.; Chen, H.M.; Chen, Y.C.; Chen, M.C.; Lee, Y.F.; Chen, J.S.; Chang, Y.C. Safety and efficacy of computed tomography-guided dye localization using patent blue V for single lung nodule for video-assisted thoracoscopic surgery: A retrospective study. Ann. Transl. Med. 2019, 7, 28. [Google Scholar] [CrossRef]
- Chandarana, H.; Feng, L.; Ream, J.; Wang, A.; Babb, J.S.; Block, K.T.; Otazo, R. Respiratory Motion-Resolved Compressed Sensing Reconstruction of Free-Breathing Radial Acquisition for Dynamic Liver Magnetic Resonance Imaging. Investig. Radiol. 2015, 50, 749. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, Y.S.; Niisato, E.; Su, M.M.; Benkert, T.; Hsu, H.H.; Shih, J.Y.; Chen, J.S.; Chang, Y.C. Detecting small pulmonary nodules with spiral ultrashort echo time sequences in 1.5 T MRI. Magma (N. Y.) 2021, 34, 399–409. [Google Scholar] [CrossRef]
- Larke, F.J.; Kruger, R.L.; Cagnon, C.H.; Flynn, M.J.; McNitt-Gray, M.M.; Wu, X.; Judy, P.F.; Cody, D.D. Estimated radiation dose associated with low-dose chest CT of average-size participants in the National Lung Screening Trial. Am. J. Roentgenol. 2011, 197, 1165–1169. [Google Scholar] [CrossRef] [PubMed]
- Ohno, Y.; Koyama, H.; Yoshikawa, T.; Kishida, Y.; Seki, S.; Takenaka, D.; Yui, M.; Miyazaki, M.; Sugimura, K. Standard-, Reduced-, and No-Dose Thin-Section Radiologic Examinations: Comparison of Capability for Nodule Detection and Nodule Type Assessment in Patients Suspected of Having Pulmonary Nodules. Radiology 2017, 284, 562–573. [Google Scholar] [CrossRef] [PubMed]
- Dournes, G.; Grodzki, D.; Macey, J.; Girodet, P.-O.; Fayon, M.; Chateil, J.-F.; Montaudon, M.; Berger, P.; Laurent, F. Quiet Submillimeter MR Imaging of the Lung Is Feasible with a PETRA Sequence at 1.5 T. Radiology 2015, 276, 258–265. [Google Scholar] [CrossRef]
- Kumar, S.; Rai, R.; Stemmer, A.; Josan, S.; Holloway, L.; Vinod, S.; Moses, D.; Liney, G. Feasibility of free breathing Lung MRI for Radiotherapy using non-Cartesian k-space acquisition schemes. Br. J. Radiol. 2017, 90, 20170037. [Google Scholar] [CrossRef] [Green Version]
- Feng, L.; Grimm, R.; Block, K.T.; Chandarana, H.; Kim, S.; Xu, J.; Axel, L.; Sodickson, D.K.; Otazo, R. Golden-angle radial sparse parallel MRI: Combination of compressed sensing, parallel imaging, and golden-angle radial sampling for fast and flexible dynamic volumetric MRI. Magn. Reson. Med. 2014, 72, 707–717. [Google Scholar] [CrossRef] [Green Version]
- Feng, L.; Axel, L.; Chandarana, H.; Block, K.T.; Sodickson, D.K.; Otazo, R. XD-GRASP: Golden-angle radial MRI with reconstruction of extra motion-state dimensions using compressed sensing. Magn. Reson. Med. 2016, 75, 775–788. [Google Scholar] [CrossRef] [Green Version]
- Jaspan, O.N.; Fleysher, R.; Lipton, M.L. Compressed sensing MRI: A review of the clinical literature. Br. J. Radiol. 2015, 88, 20150487. [Google Scholar] [CrossRef]
- Hatabu, H.; Ohno, Y.; Gefter, W.B.; Parraga, G.; Madore, B.; Lee, K.S.; Altes, T.A.; Lynch, D.A.; Mayo, J.R.; Seo, J.B.; et al. Expanding Applications of Pulmonary MRI in the Clinical Evaluation of Lung Disorders: Fleischner Society Position Paper. Radiology 2020, 297, 286–301. [Google Scholar] [CrossRef] [PubMed]
- Romei, C.; Turturici, L.; Tavanti, L.; Miedema, J.; Fiorini, S.; Marletta, M.; Wielopolski, P.; Tiddens, H.; Falaschi, F.; Ciet, P. The use of chest magnetic resonance imaging in interstitial lung disease: A systematic review. Eur. Respir. Rev. Off. J. Eur. Respir. Soc. 2018, 27. [Google Scholar] [CrossRef] [Green Version]
- Serai, S.D.; Rapp, J.B.; States, L.J.; Andronikou, S.; Ciet, P.; Lee, E.Y. Pediatric Lung MRI: Currently Available and Emerging Techniques. Am. J. Roentgenol. 2021, 216, 781–790. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | VIBE | Spiral UTE | CS-VIBE |
|---|---|---|---|
| TR | 3.90 ms | 3.72 ms | 4.13 ms |
| TE | 1.30 ms | 0.05 ms | 0.84 ms |
| Flip angle | 5° | 5° | 5° |
| Voxel matrix | 1.0 × 1.0 × 3.0 mm3 | 1.56 × 1.56 × 1.56 mm3 | 1.2 × 1.2 × 1.6 mm3 |
| Scan time | 11 s | 3.5–5 min, depending on the patient’s breathing pattern | 13 s |
| Acquired orientation | Transverse | Coronal | Transverse |
| Respiratory trigger | No | No | No |
| Acceleration factor | CAIPIRINHA iPAT = 3 | Spiral iPAT = 2 | Acceleration = 5 Iteration = 35 |
| Patient (n = 71) | ||
| Median age (range) in years | 60 (33–81) | |
| Gender (male/female) | (31/40) | |
| Number of nodules per patient | ||
| 1 | 50 (71%) | |
| 2 | 18 (25%) | |
| 3 | 2 (3%) | |
| 4 | 1 (1%) | |
| Nodule (n = 96) | ||
| Mean diameter (range), mm | 7.7 ± 3.9 (4–20) | |
| Number of nodules per size category | ||
| <6 mm | 28 (29%) | |
| ≥6–<8 mm | 28 (29%) | |
| ≥8–<10 mm | 19 (20%) | |
| ≥10 mm | 21 (22%) | |
| Number of nodules per location | ||
| RUL | 35 (36%) | |
| RML | 11 (11%) | |
| RLL | 16 (17%) | |
| LUL | 17 (18%) | |
| LLL | 17 (18%) | |
| Number of nodules per morphology category | ||
| Non-solid | 43 (45%) | |
| Part-solid | 35 (36%) | |
| Solid | 18 (19%) | |
| Number of nodules per surgical pathology a (n = 73) | ||
| Invasive adenocarcinoma | 27 (37%) | |
| Minimally invasive adenocarcinoma | 26 (36%) | |
| Squamous cell carcinoma | 1 (1%) | |
| Adenocarcinoma in situ | 11 (15%) | |
| Atypical adenomatous hyperplasia | 2 (3%) | |
| Idiopathic neuroendocrine cell hyperplasia | 1 (1%) | |
| Other benign lesions b | 5 (7%) | |
| Scores (mean ± SD) | VIBE | Spiral UTE | p-Value a (VIBE vs. Spiral UTE) | CS-VIBE | p-Value a (VIBE vs. CS-VIBE) | p-Value a (Spiral UTE vs. CS-VIBE) |
|---|---|---|---|---|---|---|
| Pulmonary vascular depiction | 3.3 ± 0.5 | 3.7 ± 0.6 | <0.001 | 3.8 ± 0.5 | <0.001 | 0.469 |
| Airway depiction | 3.0 ± 0.2 | 3.5 ± 0.6 | <0.001 | 3.3 ± 0.5 | <0.001 | 0.183 |
| Cardiac motion artifact | 3.3 ± 0.6 | 3.8 ± 0.4 | <0.001 | 3.1 ± 0.6 | 0.056 | 0.054 |
| Image noise for nodule detection | 2.8 ± 0.8 | 3.7 ± 0.7 | <0.001 | 3.4 ± 0.7 | <0.001 | 0.159 |
| Overall image quality | 3.0 ± 0.4 | 3.7 ± 0.6 | <0.001 | 3.5 ± 0.6 | <0.001 | 0.439 |
| Sensitivity (%) | Specificity (%) | False Positive Rate (%) | False Negative Rate (%) | Positive Predictive Value (%) | Negative Predictive Value (%) | p-Value * | ||
|---|---|---|---|---|---|---|---|---|
| Reader 1 | VIBE | 50/96 (52.1) | 251/259 (96.9) | 8/259 (3.1) | 46/96 (47.9) | 50/58 (86.2) | 251/297 (84.5) | - |
| Spiral UTE | 79/96 (82.3) | 256/259 (98.8) | 3/259 (1.2) | 17/96 (17.7) | 79/82 (96.3) | 256/273 (93.8) | <0.001 a | |
| CS-VIBE | 82/96 (85.4) | 257/259 (99.2) | 2/259 (0.8) | 14/96 (14.6) | 82/84 (97.6) | 257/271 (94.8) | 0.004 a 0.629 b | |
| Reader 2 | VIBE | 51/96 (53.1) | 252/259 (97.3) | 7/259 (2.7) | 45/96 (46.9) | 51/58 (87.9) | 252/297 (84.8) | - |
| Spiral UTE | 76/96 (79.2) | 257/259 (99.2) | 2/259 (0.8) | 20/96 (20.8) | 76/78 (97.4) | 257/277 (92.8) | <0.001 a | |
| CS-VIBE | 77/96 (80.2) | 258/259 (99.6) | 1/259 (0.4) | 19/96 (19.8) | 77/78 (98.7) | 258/277 (93.1) | <0.001 a 1.000 b | |
| Advantages | Disadvantages | |
|---|---|---|
| Chest CT |
|
|
| MRI VIBE |
|
|
| MRI Spiral UTE |
|
|
| MRI CS-VIBE |
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, Y.-S.; Niisato, E.; Su, M.-Y.M.; Benkert, T.; Chien, N.; Chiang, P.-Y.; Lee, W.-J.; Chen, J.-S.; Chang, Y.-C. Applying Compressed Sensing Volumetric Interpolated Breath-Hold Examination and Spiral Ultrashort Echo Time Sequences for Lung Nodule Detection in MRI. Diagnostics 2022, 12, 93. https://doi.org/10.3390/diagnostics12010093
Huang Y-S, Niisato E, Su M-YM, Benkert T, Chien N, Chiang P-Y, Lee W-J, Chen J-S, Chang Y-C. Applying Compressed Sensing Volumetric Interpolated Breath-Hold Examination and Spiral Ultrashort Echo Time Sequences for Lung Nodule Detection in MRI. Diagnostics. 2022; 12(1):93. https://doi.org/10.3390/diagnostics12010093
Chicago/Turabian StyleHuang, Yu-Sen, Emi Niisato, Mao-Yuan Marine Su, Thomas Benkert, Ning Chien, Pin-Yi Chiang, Wen-Jeng Lee, Jin-Shing Chen, and Yeun-Chung Chang. 2022. "Applying Compressed Sensing Volumetric Interpolated Breath-Hold Examination and Spiral Ultrashort Echo Time Sequences for Lung Nodule Detection in MRI" Diagnostics 12, no. 1: 93. https://doi.org/10.3390/diagnostics12010093
APA StyleHuang, Y.-S., Niisato, E., Su, M.-Y. M., Benkert, T., Chien, N., Chiang, P.-Y., Lee, W.-J., Chen, J.-S., & Chang, Y.-C. (2022). Applying Compressed Sensing Volumetric Interpolated Breath-Hold Examination and Spiral Ultrashort Echo Time Sequences for Lung Nodule Detection in MRI. Diagnostics, 12(1), 93. https://doi.org/10.3390/diagnostics12010093