
CT Brain Perfusion in the Prediction of Final Infarct Volume: A Prospective Study of Different Software Settings for Acute Ischemic Core Calculation

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patient Selection
- Underwent technically successful EVT immediately after initial CT;
- Technically compliant initial CTP study available;
- Underwent MRI 24 ± 2 h after EVT;
- Agreed with enrolment in the study and provided signed, informed consent.
- Unsuccessful EVT: TICI (Thrombolysis in cerebral infarction scale) < 2b; periprocedural complications such as arterial dissection, intracranial hemorrhage, etc.;
- Inability to undergo MRI follow-up due to poor overall condition of a patient after EVT, contraindications to MRI as pacemakers, implantable cardioverter-defibrillator, or claustrophobia;
- Patient disagreement with enrolment in the study or MRI follow-up.
2.2. Initial CT Imaging and Post-Processing
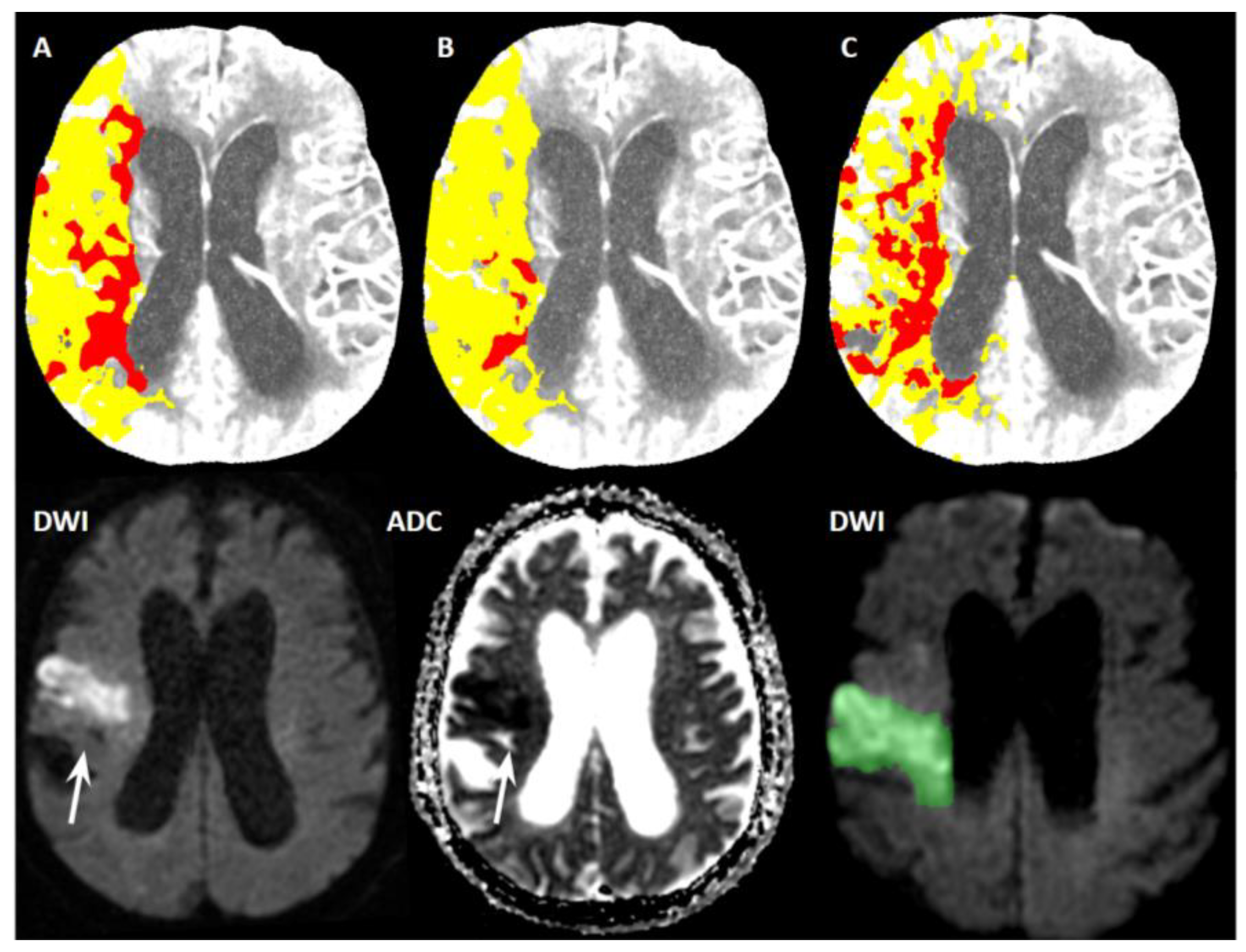
- Setting A (our adjustment of default syngo.via settings)
- Setting B (adjustment of syngo.via settings by Siemens professionals)
- Setting C (default syngo.via settings)
2.3. Follow-Up MRI and Evaluation
2.4. Statistical Analysis
3. Results
3.1. Patient Selection
3.2. CTP and MRI Data
- Setting A (CBF < 30%, TMAX > 6 s): The median ischemic core volume was 34 mL (IQR 46.5 mL).
- Setting B (CBF < 20%, TMAX > 6 s): The median ischemic core volume was 10 mL (IQR 24 mL).
- Setting C (CBV < 1.2 mL/100 mL, CBF < 27 mL/100 mL/min): The median ischemic core volume was 23 mL (IQR 22 mL).
3.3. Agreement of CTP and MRI Data
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Powers, W.J.; Rabinstein, A.A.; Ackerson, T.; Adeoye, O.M.; Bambakidis, N.C.; Becker, K.; Biller, J.; Brown, M.; Demaerschalk, B.M.; Hoh, B.; et al. Guidelines for the Early Management of Patients with Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A Guideline for Healthcare Professionals from the American Heart Association/American Stroke Association. Stroke 2019, 50, e344–e418. [Google Scholar]
- Goyal, M.; Menon, B.K.; van Zwam, W.H.; Dippel, D.W.; Mitchell, P.J.; Demchuk, A.M.; Dávalos, A.; Majoie, C.B.; van der Lugt, A.; de Miquel, M.A.; et al. Endovascular thrombectomy after large-vessel ischaemic stroke: A meta-analysis of individual patient data from five randomised trials. Lancet 2016, 387, 1723–1731. [Google Scholar] [CrossRef]
- Albers, G.W.; Lansberg, M.G.; Kemp, S.; Tsai, J.P.; Lavori, P.; Christensen, S.; Mlynash, M.; Kim, S.; Hamilton, S.; Yeatts, S.D.; et al. A multicenter randomized controlled trial of endovascular therapy following imaging evaluation for ischemic stroke (DEFUSE 3). Int. J. Stroke 2017, 12, 896–905. [Google Scholar] [CrossRef] [PubMed]
- Jovin, T.G.; Ribo, M.; Pereira, V.; Furlan, A.; Bonafe, A.; Baxter, B.; Gupta, R.; Lopes, D.; Jansen, O.; Smith, W.; et al. Diffusion-weighted imaging or computerized tomography perfusion assessment with clinical mismatch in the triage of wake up and late presenting strokes undergoing neurointervention with Trevo (DAWN) trial methods. Int. J. Stroke 2017, 12, 641–652. [Google Scholar] [CrossRef] [PubMed]
- Alves, J.E.; Carneiro, Â.; Xavier, J. Reliability of CT perfusion in the evaluation of the ischaemic penumbra. Neuroradiol. J. 2014, 27, 91–95. [Google Scholar] [CrossRef]
- Malikova, H.; Weichet, J. Diagnosis of Ischemic Stroke: As Simple as Possible. Diagnostics 2022, 12, 1452. [Google Scholar] [CrossRef]
- Xiong, Y.; Huang, C.C.; Fisher, M.; Hackney, D.B.; Bhadelia, R.A.; Selim, M.H. Comparison of Automated CT Perfusion Softwares in Evaluation of Acute Ischemic Stroke. J. Stroke Cerebrovasc. Dis. 2019, 28, 104392. [Google Scholar] [CrossRef]
- Bathla, G.; Limaye, K.; Policeni, B.; Klotz, E.; Juergens, M.; Derdeyn, C. Achieving comparable perfusion results across vendors. The next step in standardizing stroke care: A technical report. J. Neurointerv. Surg. 2019, 11, 1257–1260. [Google Scholar] [CrossRef]
- Koopman, M.S.; Berkhemer, O.A.; Geuskens, R.; Emmer, B.J.; van Walderveen, M.; Jenniskens, S.; van Zwam, W.H.; van Oostenbrugge, R.J.; van der Lugt, A.; Dippel, D.W.J.; et al. Comparison of three commonly used CT perfusion software packages in patients with acute ischemic stroke. J. Neurointerv. Surg. 2019, 11, 1249–1256. [Google Scholar] [CrossRef]
- Karhi, S.; Tähtinen, O.; Aherto, J.; Matikka, H.; Manninen, H.; Nerg, O.; Taina, M.; Jäkälä, P.; Vanninen, R. Effect of different thresholds for CT perfusion volumetric analysis on estimated ischemic core and penumbral volumes. PLoS ONE 2021, 16, e0249772. [Google Scholar] [CrossRef]
- Mangla, R.; Ekhom, S.; Jahromi, B.S.; Almast, J.; Mangla, M.; Westesson, P.L. CT perfusion in acute stroke: Know the mimics, potential pitfalls, artifacts, and technical errors. Emerg. Radiol. 2014, 21, 49–65. [Google Scholar] [CrossRef] [PubMed]
- Zussman, B.M.; Boghosian, G.; Gorniak, R.J.; Olszewski, M.E.; Read, K.M.; Siddiqui, K.M.; Flanders, A.E. The relative effect of vendor variability in CT perfusion results: A method comparison study. AJR Am. J. Roentgenol. 2011, 197, 468–473. [Google Scholar] [CrossRef] [PubMed]
- Kudo, K.; Sasaki, M.; Yamada, K.; Momoshima, S.; Utsunomiya, H.; Shirato, H.; Ogasawara, K. Differences in CT perfusion maps generated by different commercial software: Quantitative analysis by using identical source data of acute stroke patients. Radiology 2010, 254, 200–209. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Pelegrí, M.; Biarnés, C.; Thió-Henestrosa, S.; Remollo, S.; Gimeno, A.; Cuba, V.; Teceño, M.; Martí-Navas, M.; Serena, J.; Pedraza, S.; et al. Higher agreement in endovascular treatment decision-making than in parametric quantifications among automated CT perfusion software packages in acute ischemic stroke. J. X-ray Sci. Technol. 2021, 29, 823–834. [Google Scholar] [CrossRef]
- Kremenova, K.; Holesta, M.; Peisker, T.; Girsa, D.; Weichet, J.; Lukavsky, J.; Malikova, H. Is limited-coverage CT perfusion helpful in treatment decision-making in patients with acute ischemic stroke? Quant. Imaging Med. Surg. 2020, 10, 1908–1916. [Google Scholar] [CrossRef]
- Malikova, H.; Kremenova, K.; Budera, P.; Herman, D.; Weichet, J.; Lukavsky, J.; Osmancik, P. Silent strokes after thoracoscopic epicardial ablation and catheter ablation for atrial fibrillation: Not all lesions are permanent on follow-up magnetic resonance imaging. Quant. Imaging Med. Surg. 2021, 11, 3219–3233. [Google Scholar] [CrossRef]
- Peisker, T.; Vaško, P.; Mikulenka, P.; Lauer, D.; Kožnar, B.; Sulženko, J.; Roháč, F.; Kučera, D.; Girsa, D.; Kremeňová, K.; et al. Clinical and radiological factors predicting stroke outcome after successful mechanical intervention in anterior circulation. Eur. Heart J. Suppl. J. Eur. Soc. Cardiol. 2022, 24, B48–B52. [Google Scholar] [CrossRef]
- Fabritius, M.P.; Wölfer, T.A.; Herzberg, M.; Tiedt, S.; Puhr-Westerheide, D.; Grosu, S.; Maurus, S.; Geyer, T.; Curta, A.; Kellert, L.; et al. Course of Early Neurologic Symptom Severity after Endovascular Treatment of Anterior Circulation Large Vessel Occlusion Stroke: Association with Baseline Multiparametric CT Imaging and Clinical Parameters. Diagnostics 2021, 11, 1272. [Google Scholar] [CrossRef]
- Barber, P.A.; Demchuk, A.M.; Zhang, J.; Buchan, A.M. Validity and reliability of a quantitative computed tomography score in predicting outcome of hyperacute stroke before thrombolytic therapy. ASPECTS Study Group. Alberta Stroke Programme Early CT Score. Lancet 2000, 355, 1670–1674. [Google Scholar] [CrossRef]
- Martins, N.; Aires, A.; Mendez, B.; Boned, S.; Rubiera, M.; Tomasello, A.; Coscojuela, P.; Hernandez, D.; Muchada, M.; Rodríguez-Luna, D.; et al. Ghost Infarct Core and Admission Computed Tomography Perfusion: Redefining the Role of Neuroimaging in Acute Ischemic Stroke. Interv. Neurol. 2018, 7, 513–521. [Google Scholar] [CrossRef]
- Boned, S.; Padroni, M.; Rubiera, M.; Tomasello, A.; Coscojuela, P.; Romero, N.; Muchada, M.; Rodríguez-Luna, D.; Flores, A.; Rodríguez, N.; et al. Admission CT perfusion may overestimate initial infarct core: The ghost infarct core concept. J. Neurointerv. Surg. 2017, 9, 66–69. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, G.M.; Mohammaden, M.H.; Haussen, D.C.; Bouslama, M.; Ravindran, K.; Pisani, L.; Prater, A.; Frankel, M.R.; Nogueira, R.G. Ghost infarct core following endovascular reperfusion: A risk for computed tomography perfusion misguided selection in stroke. Int. J. Stroke 2022, 17, 897–905. [Google Scholar] [CrossRef] [PubMed]
- Rotem, S.H.; Mor, S.; Chen, B.; Firas, S.; Elliot, S.; Ayelet, E.; Eitan, A.; Gregory, T. Infarct Core Reliability by CT Perfusion is a Time-Dependent Phenomenon. J. Neuroimaging 2020, 30, 240–245. [Google Scholar] [PubMed]
- Mendez, A.A.; Quispe-Orozco, D.; Dandapat, S.; Samaniego, E.A.; Tamadonfar, E.; Zevallos, C.B.; Farooqui, M.; Derdeyn, C.P.; Ortega-Gutierrez, S. Overestimation of core infarct by computed tomography perfusion in the golden hour. Brain Circ. 2020, 6, 211–214. [Google Scholar]
- Berge, E.; Whiteley, W.; Audebert, H.; De Marchis, G.M.; Fonseca, A.C.; Padiglioni, C.; de la Ossa, N.P.; Strbian, D.; Tsivgoulis, G.; Turc, G. European Stroke Organisation (ESO) guidelines on intravenous thrombolysis for acute ischaemic stroke. Eur. Stroke J. 2021, 6, 1–62. [Google Scholar] [CrossRef]
- Schaefer, P.W. Applications of DWI in clinical neurology. J. Neurol. Sci. 2001, 186, 25–35. [Google Scholar] [CrossRef]
- Kidwell, C.S.; Chalela, J.A.; Saver, J.L.; Starkman, S.; Hill, M.D.; Demchuk, A.M.; Butman, J.A.; Patronas, N.; Alger, J.R.; Latour, L.L.; et al. Comparison of MRI and CT for detection of acute intracerebral hemorrhage. JAMA 2004, 292, 1823–1830. [Google Scholar] [CrossRef]
- Vilela, P.; Rowley, H.A. Brain ischemia: CT and MRI techniques in acute ischemic stroke. Eur. J. Radiol. 2017, 96, 162–172. [Google Scholar] [CrossRef]
- Molad, J. CT Perfusion: More Than What You Thought. AJNR Am. J. Neuroradiol. 2021, 42, 73–74. [Google Scholar] [CrossRef]
- Austein, F.; Riedel, C.; Kerby, T.; Meyne, J.; Binder, A.; Lindner, T.; Huhndorf, M.; Wodarg, F.; Jansen, O. Comparison of Perfusion CT Software to Predict the Final Infarct Volume After Thrombectomy. Stroke 2016, 47, 2311–2317. [Google Scholar] [CrossRef]
- Fahmi, F.; Marquering, H.A.; Streekstra, G.J.; Beenen, L.F.; Velthuis, B.K.; VanBavel, E.; Majoie, C.B. Differences in CT perfusion summary maps for patients with acute ischemic stroke generated by 2 software packages. AJNR Am. J. Neuroradiol. 2012, 33, 2074–2080. [Google Scholar] [CrossRef] [PubMed]
- Hoving, J.W.; Marquering, H.A.; Majoie, C.; Yassi, N.; Sharma, G.; Liebeskind, D.S.; van der Lugt, A.; Roos, Y.B.; van Zwam, W.; van Oostenbrugge, R.J.; et al. Volumetric and Spatial Accuracy of Computed Tomography Perfusion Estimated Ischemic Core Volume in Patients with Acute Ischemic Stroke. Stroke 2018, 49, 2368–2375. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Parameter | NECT | CTA | CTP |
|---|---|---|---|
| Rotation time (s) | 1 | 0.28 | 0.28 |
| Tube voltage (kVp) | 120 | 120 ** | 70 |
| Tube current (mAs) | 273 * | 84 * | 200 |
| Gantry tilt | no | no | no |
| Field of view (mm) | 250 | 250 | 200 |
| Iterative reconstruction | Yes | Yes | No |
| Reconstruction filter | Soft tissue | Soft tissue | Soft tissue |
| Primary reconstruction slice thickness/increment (mm) | 3/3 | 0.75/0.5 | 1.5/1 |
| Multiplanar reconstruction slice thickness/increment (mm) | 3/3 | 10/2 | - |
| Sequence | TR (ms) | TE (ms) | TI (ms) | Slice Thickness (mm) |
|---|---|---|---|---|
| T2 FLAIR | 8500 | 123.66 | 2000 | 5 |
| GRE T2 * | 800 | 20 | - | 5 |
| DWI | 8000 | 20 | - | 5 |
| 3D TOF | 27 | 6.8 | - | 1.2 |
| No. of Patients (%) | Mean ± SD | ||
|---|---|---|---|
| Age | - | 68 ± 11.2 | |
| Sex | Female | 15 (32) | - |
| Male | 32 (68) | - | |
| Occluded artery | M1 segment of MCA | 21 (45) | - |
| M2 segment of MCA | 12 (26) | - | |
| ICA | 3 (6) | - | |
| Tandem occlusion | 11 (23) | - | |
| Side of occlusion | Right | 21 (45) | - |
| Left | 26 (55) | - | |
| ASPECTS | - | 7.5 ± 1.9 | |
| NIHSS | - | 13.5 ± 5.1 | |
| LKW-CT time (min) | - | 126 ± 83 | |
| CT-groin puncture time (min) | - | 50 ± 16 | |
| LKW-recanalization time (min) | - | 213 ± 86 | |
| Bridging IVT | 29 (62) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kremenova, K.; Lukavsky, J.; Holesta, M.; Peisker, T.; Lauer, D.; Weichet, J.; Malikova, H. CT Brain Perfusion in the Prediction of Final Infarct Volume: A Prospective Study of Different Software Settings for Acute Ischemic Core Calculation. Diagnostics 2022, 12, 2290. https://doi.org/10.3390/diagnostics12102290
Kremenova K, Lukavsky J, Holesta M, Peisker T, Lauer D, Weichet J, Malikova H. CT Brain Perfusion in the Prediction of Final Infarct Volume: A Prospective Study of Different Software Settings for Acute Ischemic Core Calculation. Diagnostics. 2022; 12(10):2290. https://doi.org/10.3390/diagnostics12102290
Chicago/Turabian StyleKremenova, Karin, Jiri Lukavsky, Michal Holesta, Tomas Peisker, David Lauer, Jiri Weichet, and Hana Malikova. 2022. "CT Brain Perfusion in the Prediction of Final Infarct Volume: A Prospective Study of Different Software Settings for Acute Ischemic Core Calculation" Diagnostics 12, no. 10: 2290. https://doi.org/10.3390/diagnostics12102290
APA StyleKremenova, K., Lukavsky, J., Holesta, M., Peisker, T., Lauer, D., Weichet, J., & Malikova, H. (2022). CT Brain Perfusion in the Prediction of Final Infarct Volume: A Prospective Study of Different Software Settings for Acute Ischemic Core Calculation. Diagnostics, 12(10), 2290. https://doi.org/10.3390/diagnostics12102290