
The Construction and Evaluation of a Multi-Task Convolutional Neural Network for a Cone-Beam Computed-Tomography-Based Assessment of Implant Stability
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Surgical Protocol and Resonance Frequency Analysis
2.2. CBCT Image Acquisition and Image Pre-Processing
2.3. Estimation of Sample Size
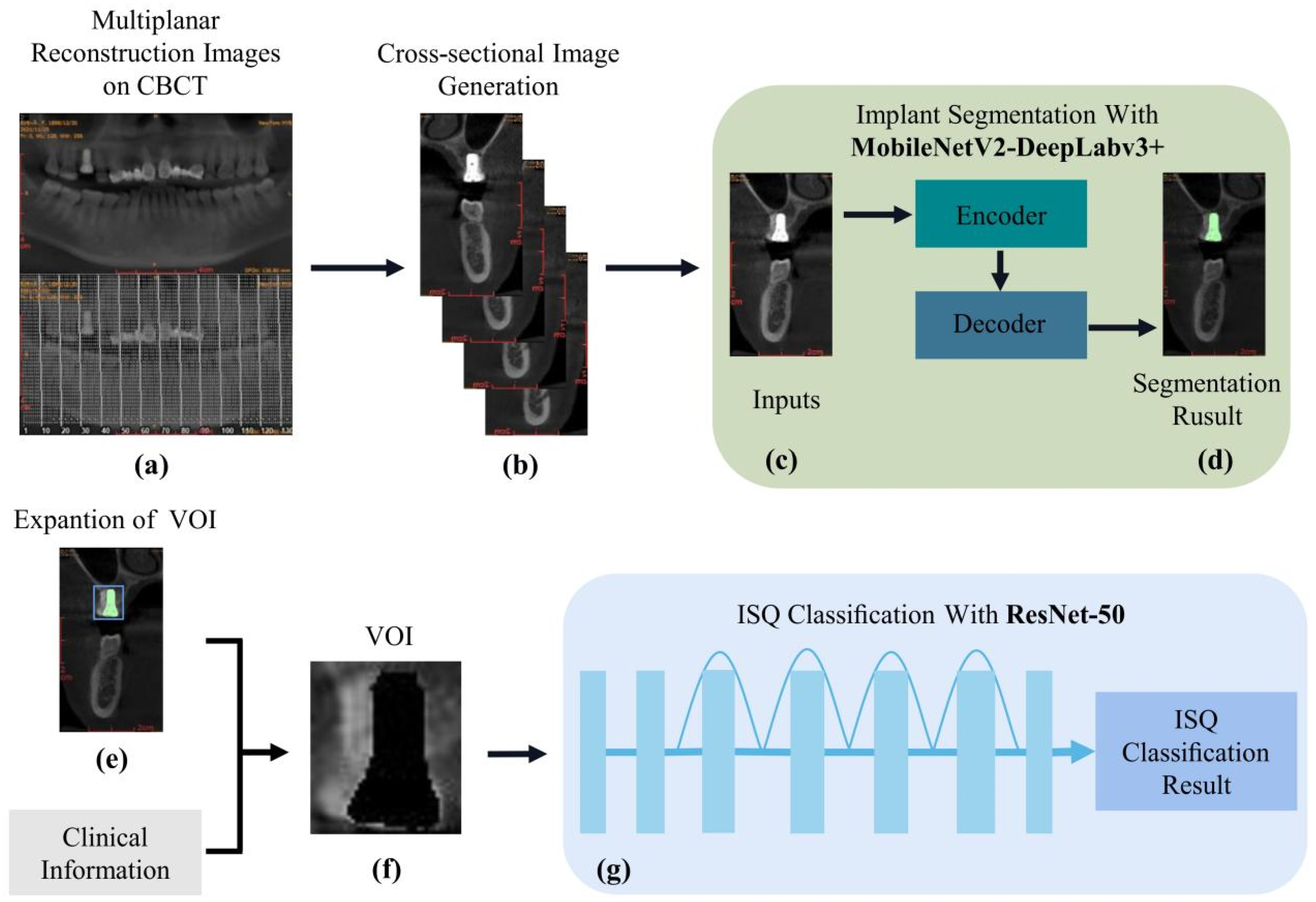
2.4. Construction of a Multi-Task Cascade Network
2.4.1. Construction of the MobilenetV2-DeeplabV3+ Implant Recognition and Segmentation Network
2.4.2. Training of the MobilenetV2-DeeplabV3+-Based Implant Recognition and Segmentation Network
2.4.3. Prior Knowledge-Based VOI Extractor
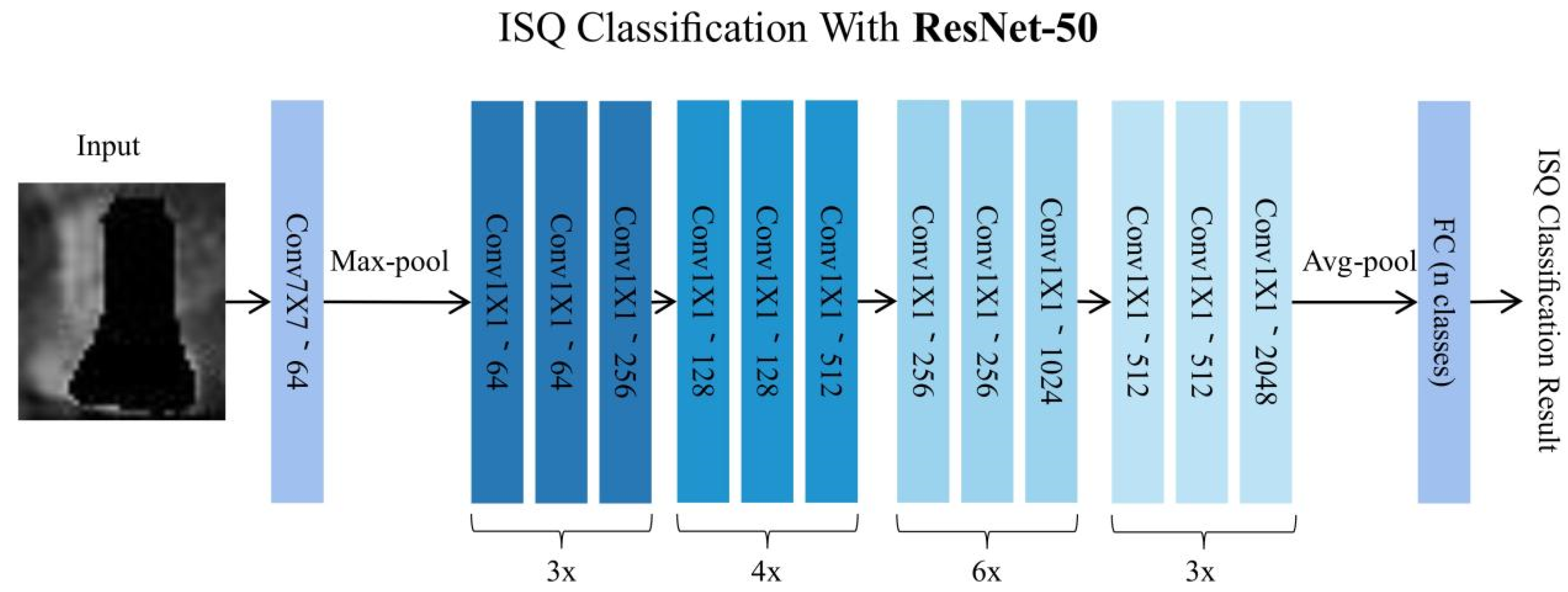
2.4.4. Construction of the ResNet-50-Based Implant Stability Classification Network
2.4.5. Training of the ResNet-50-Based Implant Stability Classification Network
2.5. Model Performance Evaluation and Statistical Analysis
3. Results
3.1. Performance of Implant Identification and Segmentation Based on MobilenetV2-DeeplabV3+
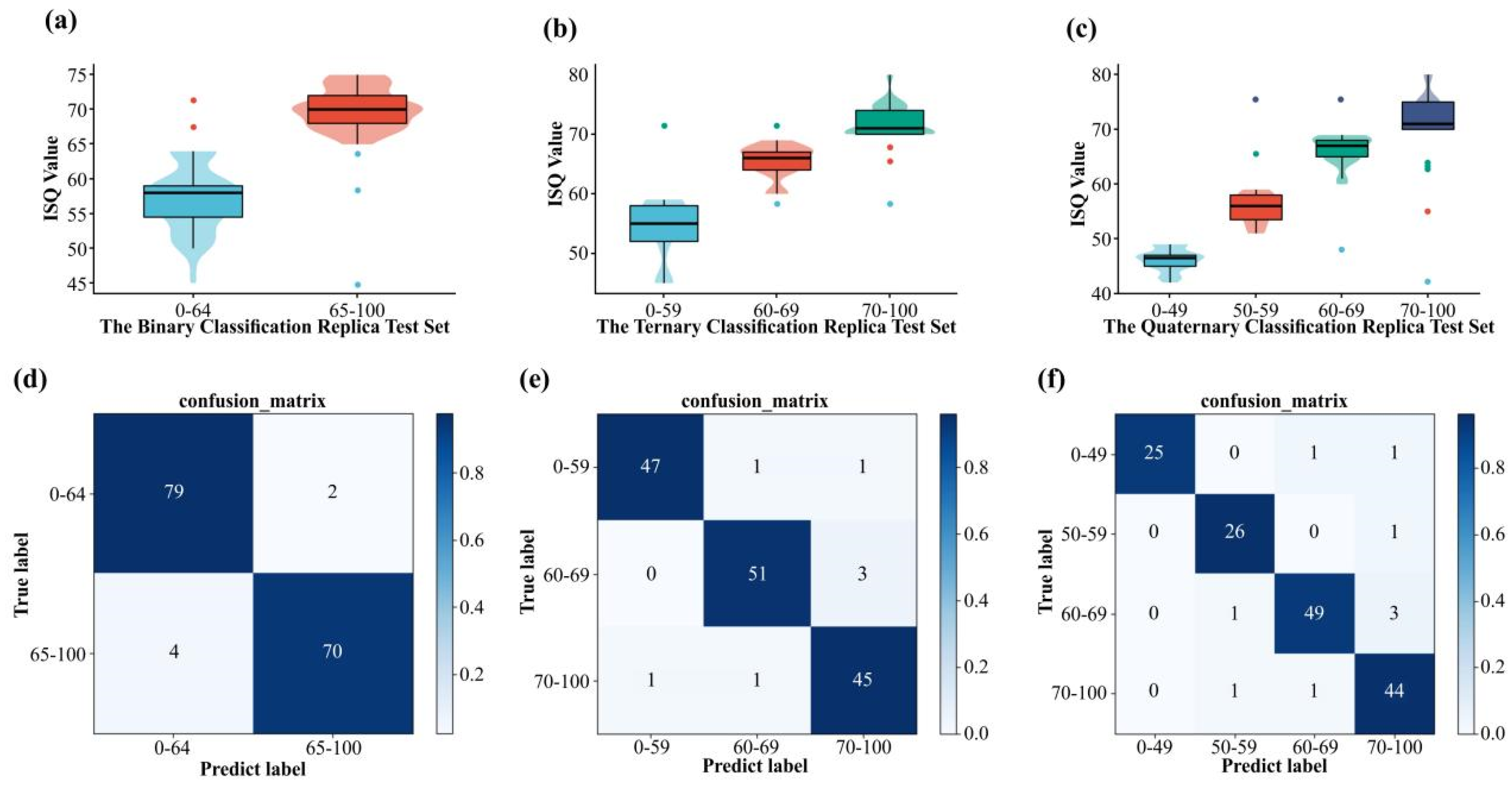
3.2. Classification Performance of Implant Stability Based on ResNet-50
3.3. Time Costs
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sennerby, L.; Meredith, N. Implant stability measurements using resonance frequency analysis: Biological and biomechanical aspects and clinical implications. Periodontology 2000 2008, 47, 51–66. [Google Scholar] [CrossRef] [PubMed]
- Bavetta, G.; Bavetta, G.; Randazzo, V.; Cavataio, A.; Paderni, C.; Grassia, V.; Dipalma, G.; Isacco, C.G.; Scarano, A.; De Vito, D.; et al. A Retrospective Study on Insertion Torque and Implant Stability Quotient (ISQ) as Stability Parameters for Immediate Loading of Implants in Fresh Extraction Sockets. BioMed Res. Int. 2019, 2019, 9720419. [Google Scholar] [CrossRef] [Green Version]
- Cassetta, M.; Brandetti, G.; Altieri, F. Are the Insertion Torque Value and Implant Stability Quotient Correlated, and If So, Can Insertion Torque Values Predict Secondary Implant Stability? A Prospective Parallel Cohort Study. Int. J. Oral Maxillofac. Implant. 2022, 37, 135–142. [Google Scholar] [CrossRef]
- Sim, C.P.C.; Lang, N.P. Factors influencing resonance frequency analysis assessed by Osstell™ mentor during implant tissue integration: I. Instrument positioning, bone structure, implant length. Clin. Oral Implant. Res. 2010, 21, 598–604. [Google Scholar] [CrossRef] [PubMed]
- Aparicio, C.; Lang, N.P.; Rangert, B. Validity and clinical significance of biomechanical testing of implant/bone interface. Clin. Oral Implant. Res. 2006, 17, 2–7. [Google Scholar] [CrossRef] [PubMed]
- Arsan, B.; Yalcin-Ülker, G.M.; Meral, D.G.; Erdem, T.L. Is there any predictive bone parameter for implant stability in 2-dimensional and 3-dimensional radiologic images? Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2021, 131, 371–379. [Google Scholar] [CrossRef]
- Magat, G.; Oncu, E.; Ozcan, S.; Orhan, K. Comparison of cone-beam computed tomography and digital panoramic radiography for detecting peri-implant alveolar bone changes using trabecular micro-structure analysis. J. Korean Assoc. Oral Maxillofac. Surg. 2022, 48, 41–49. [Google Scholar] [CrossRef]
- Krizhevsky, A.; Sutskever, I.; Hinton, G.E. Imagenet classification with deep convolutional neural networks. NIPS 2017, 60, 84–90. [Google Scholar] [CrossRef] [Green Version]
- Lahoud, P.; Diels, S.; Niclaes, L.; Van Aelst, S.; Willems, H.; Van Gerven, A.; Quirynen, M.; Jacobs, R. Development and validation of a novel artificial intelligence driven tool for accurate mandibular canal segmentation on CBCT. J. Dent. 2021, 116, 103891. [Google Scholar] [CrossRef]
- Gerhardt, M.D.N.; Fontenele, R.C.; Leite, A.F.; Lahoud, P.; Van Gerven, A.; Willems, H.; Smolders, A.; Beznik, T.; Jacobs, R. Automated detection and labelling of teeth and small edentulous regions on cone-beam computed tomography using convolutional neural networks. J. Dent. 2022, 122, 104139. [Google Scholar] [CrossRef]
- Li, S.; Liu, J.; Zhou, Z.; Zhou, Z.; Wu, X.; Li, Y.; Wang, S.; Liao, W.; Ying, S.; Zhao, Z. Artificial intelligence for caries and periapical periodontitis detection. J. Dent. 2022, 122, 104107. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Minnema, J.; Batenburg, K.; Forouzanfar, T.; Hu, F.; Wu, G. Multiclass CBCT Image Segmentation for Orthodontics with Deep Learning. J. Dent. Res. 2021, 100, 943–949. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.-Q.; Xu, Z.-N.; Mao, W.-Y.; Li, Y.; Zhang, X.-H.; Bai, H.-L.; Ding, P.; Fu, K.-Y. Deep learning-based evaluation of the relationship between mandibular third molar and mandibular canal on CBCT. Clin. Oral Investig. 2021, 26, 981–991. [Google Scholar] [CrossRef]
- Huang, Z.; Xia, T.; Kim, J.; Zhang, L.; Lie, B. Combining CNN With Pathological Information for the Detection of Transmissive Lesions of Jawbones From CBCT Images. In Proceedings of the 2021 43rd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Virtual, 31 October–4 November 2021. [Google Scholar]
- Insua, A.; Monje, A.; Wang, H.-L.; Miron, R.J. Basis of bone metabolism around dental implants during osseointegration and peri-implant bone loss. J. Biomed. Mater. Res. Part A 2017, 105, 2075–2089. [Google Scholar] [CrossRef]
- Chollet, F. Xception: Deep learning with depth-wise separable convolutions. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 1251–1258. [Google Scholar]
- Howard, A.G.; Zhu, M.; Chen, B.; Kalenichenko, D.; Wang, W.; Weyand, T.; Andreetto, M.; Adam, H. Mobilenets: Efficient Convolutional Neural Networks for Mobile Vision Applications. arXiv 2017, arXiv:1704.04861. [Google Scholar]
- Ioffe, S.; Szegedy, C. Batch normalization: Accelerating deep network training by reducing internal covariate shift. In Proceedings of the International Conference on Machine Learning, Lille, France, 7–9 July 2015; pp. 448–456. [Google Scholar]
- Glorot, X.; Bordes, A.; Bengio, Y. Deep sparse rectifier neural networks. In Proceedings of the Fourteenth International Conference on Artificial Intelligence and Statistics, Fort Lauderdale, FL, USA, 11–13 April 2011; pp. 315–323. [Google Scholar]
- Sandler, M.; Howard, A.; Zhu, M. Mobilenetv2: Inverted residuals and linear bottlenecks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Salt Lake City, UT, USA, 18–23 June 2018; pp. 4510–4520. [Google Scholar]
- Deng, J.; Dong, W.; Socher, R. Imagenet: A large-scale hierarchical image database. In Proceedings of the 2009 IEEE Conference on Computer Vision and Pattern Recognition, Miami, FL, USA, 20–25 June 2009; pp. 248–255. [Google Scholar]
- Wirth, A.J.; Goldhahn, J.; Flaig, C.; Arbenz, P.; Müller, R.; van Lenthe, G.H. Implant stability is affected by local bone microstructural quality. Bone 2011, 49, 473–478. [Google Scholar] [CrossRef]
- He, K.; Zhang, X.; Ren, S. Deep residual learning for image recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar]
- Abdulhameed, E.A.; Al-Rawi, N.H.; Uthman, A.; Samsudin, A.R. Bone Texture Fractal Dimension Analysis of Ultrasound-Treated Bone around Implant Site: A Double-Blind Clinical Trial. Int. J. Dent. 2018, 2018, 2672659. [Google Scholar] [CrossRef] [Green Version]
- Saberi, B.V.; Khosravifard, N.; Nooshmand, K.; Kajan, Z.D.; Ghaffari, M.E. Fractal analysis of the trabecular bone pattern in the presence/absence of metal artifact–producing objects: Comparison of cone-beam computed tomography with panoramic and periapical radiography. Dentomaxillofacial Radiol. 2021, 50, 20200559. [Google Scholar] [CrossRef]
- Franciotti, R.; Moharrami, M.; Quaranta, A.; Bizzoca, M.E.; Piattelli, A.; Aprile, G.; Perrotti, V. Use of fractal analysis in dental images for osteoporosis detection: A systematic review and meta-analysis. Osteoporos. Int. 2021, 32, 1041–1052. [Google Scholar] [CrossRef]
- Magat, G.; Sener, S.O. Evaluation of trabecular pattern of mandible using fractal dimension, bone area fraction, and gray scale value: Comparison of cone-beam computed tomography and panoramic radiography. Oral Radiol. 2018, 35, 35–42. [Google Scholar] [CrossRef]
- Gallucci, G.O.; Benic, G.I.; Eckert, S.E.; Papaspyridakos, P.; Schimmel, M.; Schrott, A.; Weber, H.-P. Consensus Statements and Clinical Recommendations for Implant Loading Protocols. Int. J. Oral Maxillofac. Implant. 2014, 29, 287–290. [Google Scholar] [CrossRef] [PubMed]
- Bornstein, M.M.; Hart, C.N.; Halbritter, S.A.; Morton, D.; Buser, D. Early Loading of Nonsubmerged Titanium Implants with a Chemically Modified Sand-Blasted and Acid-Etched Surface: 6-Month Results of a Prospective Case Series Study in the Posterior Mandible Focusing on Peri-Implant Crestal Bone Changes and Implant Stability Quotient (ISQ) Values. Clin. Implant Dent. Relat. Res. 2009, 11, 338–347. [Google Scholar] [CrossRef]
- Morton, D.; Gallucci, G.; Lin, W.; Pjetursson, B.; Polido, W.; Roehling, S.; Sailer, I.; Aghaloo, T.; Albera, H.; Bohner, L.; et al. Group 2 ITI Consensus Report: Prosthodontics and implant dentistry. Clin. Oral Implant. Res. 2018, 29, 215–223. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Z.; Yan, H.; Setzer, F.C.; Shi, K.J.; Mupparapu, M.; Li, J. Anatomically Constrained Deep Learning for Automating Dental CBCT Segmentation and Lesion Detection. IEEE Trans. Autom. Sci. Eng. 2020, 18, 603–614. [Google Scholar] [CrossRef]
- Li, J.; Jin, P.; Zhu, J.; Zou, H.; Xu, X.; Tang, M.; Zhou, M.; Gan, Y.; He, J.; Ling, Y.; et al. Multi-scale GCN-assisted two-stage network for joint segmentation of retinal layers and discs in peripapillary OCT images. Biomed. Opt. Express 2021, 12, 2204–2220. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.-R.; Bok, S.-C.; Choi, S.-C.; Lee, S.-S.; Heo, M.-S.; Huh, K.-H.; Kim, T.-I.; Yi, W.-J. The relationship between dental implant stability and trabecular bone structure using cone-beam computed tomography. J. Periodontal Implant Sci. 2016, 46, 116–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hussain, M.; Bird, J.J.; Faria, D.R. A Study on CNN Transfer Learning for Image Classification. In Advances in Computational Intelligence Systems, Proceedings of the UK Workshop on Computational Intelligence, Nottingham, UK, 5–7 September 2018; Springer: Berlin/Heidelberg, Germany, 2018; Volume 840, pp. 191–202. [Google Scholar] [CrossRef]
- Tajbakhsh, N.; Shin, J.Y.; Gurudu, S.R.; Hurst, R.T.; Kendall, C.B.; Gotway, M.B.; Liang, J. Convolutional Neural Networks for Medical Image Analysis: Full Training or Fine Tuning? IEEE Trans. Med. Imaging 2016, 35, 1299–1312. [Google Scholar] [CrossRef] [Green Version]
- Zhang, M.; Cui, Z.; Neumann, M.; Chen, Y. An End-to-End Deep Learning Architecture for Graph Classification. In Proceedings of the AAAI Conference on Artificial Intelligence, New Orleans, LA, USA, 2–7 February 2018. [Google Scholar] [CrossRef]
- Dai, J.; He, K.; Sun, J. Instance-Aware Semantic Segmentation via Multi-task Network Cascades. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Las Vegas, NV, USA, 27–30 June 2016; pp. 3150–3158. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Performance | Mean | Implant | Background |
|---|---|---|---|
| mIoU | 0.9440 | 0.8904 | 0.9976 |
| PA | 0.9676 | 0.9363 | 0.9989 |
| Recall | 0.9687 | 0.9383 | 0.9991 |
| Precision | 0.9733 | 0.9478 | 0.9987 |
| One-vs.-Rest Classification | Sensitivity | Specificity | PPV | NPV | F1 |
|---|---|---|---|---|---|
| Binary Classification as model outputs | |||||
| 65–100 vs. 0–64 | 0.9753 | 0.9459 | 0.9518 | 0.9722 | 0.9591 |
| Three Classification as model outputs | |||||
| 0–59 vs. others | 0.9592 | 0.9804 | 0.9792 | 0.9804 | 0.9692 |
| 60–69 vs. others | 0.9444 | 0.9792 | 0.9623 | 0.9691 | 0.9534 |
| 70–100 vs. others | 0.9574 | 0.9612 | 0.9184 | 0.9802 | 0.9379 |
| Four Classification as model outputs | |||||
| 0–49 vs. others | 0.9259 | 1.0000 | 1.0000 | 0.9844 | 0.9630 |
| 50–59 vs. others | 0.9630 | 0.9920 | 0.9286 | 0.9920 | 0.9458 |
| 60–70 vs. others | 0.9245 | 0.9800 | 0.9608 | 0.9608 | 0.9427 |
| 70–100 vs. others | 0.9565 | 0.9533 | 0.8980 | 0.9549 | 0.9272 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, Z.; Zheng, H.; Huang, J.; Yang, Y.; Wu, Y.; Ge, L.; Wang, L. The Construction and Evaluation of a Multi-Task Convolutional Neural Network for a Cone-Beam Computed-Tomography-Based Assessment of Implant Stability. Diagnostics 2022, 12, 2673. https://doi.org/10.3390/diagnostics12112673
Huang Z, Zheng H, Huang J, Yang Y, Wu Y, Ge L, Wang L. The Construction and Evaluation of a Multi-Task Convolutional Neural Network for a Cone-Beam Computed-Tomography-Based Assessment of Implant Stability. Diagnostics. 2022; 12(11):2673. https://doi.org/10.3390/diagnostics12112673
Chicago/Turabian StyleHuang, Zelun, Haoran Zheng, Junqiang Huang, Yang Yang, Yupeng Wu, Linhu Ge, and Liping Wang. 2022. "The Construction and Evaluation of a Multi-Task Convolutional Neural Network for a Cone-Beam Computed-Tomography-Based Assessment of Implant Stability" Diagnostics 12, no. 11: 2673. https://doi.org/10.3390/diagnostics12112673
APA StyleHuang, Z., Zheng, H., Huang, J., Yang, Y., Wu, Y., Ge, L., & Wang, L. (2022). The Construction and Evaluation of a Multi-Task Convolutional Neural Network for a Cone-Beam Computed-Tomography-Based Assessment of Implant Stability. Diagnostics, 12(11), 2673. https://doi.org/10.3390/diagnostics12112673