

Analysis of Spinal Ischemia after Frozen Elephant Trunk for Acute Aortic Dissection: An Observational, Single-Center Study

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Liu, Z.-G.; Sun, L.-Z.; Chang, Q.; Zhu, J.-M.; Dong, C.; Yu, C.-T.; Liu, Y.-M.; Zhang, H.-T. Should the “elephant trunk” be skeletonized? Total arch replacement combined with stented elephant trunk implantation for Stanford type A aortic dissection. J. Thorac. Cardiovasc. Surg. 2006, 131, 107–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uchida, N.; Shibamura, H.; Katayama, A.; Shimada, N.; Sutoh, M.; Ishihara, H. Operative Strategy for Acute Type A Aortic Dissection: Ascending Aortic or Hemiarch Versus Total Arch Replacement With Frozen Elephant Trunk. Ann. Thorac. Surg. 2009, 87, 773–777. [Google Scholar] [CrossRef] [PubMed]
- Hori, D.; Kusadokoro, S.; Adachi, K.; Kimura, N.; Yuri, K.; Matsumoto, H.; Yamaguchi, A. Risk factors for spinal cord injury in patients undergoing frozen elephant trunk technique for acute aortic dissection. Gen. Thorac. Cardiovasc. Surg. 2019, 68, 328–334. [Google Scholar] [CrossRef] [PubMed]
- Cao, P.; De Rango, P.; Czerny, M.; Evangelista, A.; Fattori, R.; Nienaber, C.; Rousseau, H.; Schepens, M. Systematic review of clinical outcomes in hybrid procedures for aortic arch dissections and other arch diseases. J. Thorac. Cardiovasc. Surg. 2012, 144, 1286–1300.e2. [Google Scholar] [CrossRef] [Green Version]
- Lin, H.-H.; Liao, S.-F.; Wu, C.-F.; Li, P.-C.; Li, M.-L. Outcome of Frozen Elephant Trunk Technique for Acute Type A Aortic Dissection. Medicine 2015, 94, e694. [Google Scholar] [CrossRef]
- Roy, A.; Mc Gorrian, C.; Treacy, C.; Kavanaugh, E.; Brennan, A.; Mahon, N.; Murray, P.T. A Comparison of Traditional and Novel Definitions (RIFLE, AKIN, and KDIGO) of Acute Kidney Injury for the Prediction of Outcomes in Acute Decompensated Heart Failure. Cardiorenal Med. 2013, 3, 26–37. [Google Scholar] [CrossRef]
- Lombardi, J.V.; Hughes, G.C.; Appoo, J.J.; Bavaria, J.E.; Beck, A.W.; Cambria, R.P.; Charlton-Ouw, K.; Eslami, M.H.; Kim, K.M.; Leshnower, B.G.; et al. Society for Vascular Surgery (SVS) and Society of Thoracic Surgeons (STS) Reporting Standards for Type B Aortic Dissections. Ann. Thorac. Surg. 2020, 109, 959–981. [Google Scholar] [CrossRef]
- Knipp, B.S.; Deeb, G.M.; Prager, R.L.; Williams, C.Y.; Upchurch, G.R.; Patel, H.J. A contemporary analysis of outcomes for operative repair of type A aortic dissection in the United States. Surgery 2007, 142, 524–528.e1. [Google Scholar] [CrossRef]
- Conzelmann, L.O.; Weigang, E.; Mehlhorn, U.; Abugameh, A.; Hoffmann, I.; Blettner, M.; Etz, C.D.; Czerny, M.; Vahl, C.F. Mortality in patients with acute aortic dissection type A: Analysis of pre- and intraoperative risk factors from the German Registry for Acute Aortic Dissection Type A (GERAADA). Eur. J. Cardio-Thorac. Surg. 2015, 49, e44–e52. [Google Scholar] [CrossRef] [Green Version]
- Pape, L.; Awais, M.; Woznicki, E. Presentation, Diagnosis, and Outcomes of Acute Aortic Dissection: Seventeen-Year Trends From the International Registry of Acute Aortic Dissection. J. Vasc. Surg. 2016, 63, 552–553. [Google Scholar] [CrossRef]
- Hobbs, R.; Si, M.-S. Commentary: Modified Frozen Elephant Trunk. J. Thorac. Cardiovasc. Surg. 2022, 163, 1763–1764. [Google Scholar] [CrossRef] [PubMed]
- Berdajs, D.A.; Koechlin, L.; Reid, G.; Grob, F.; Gahl, B.; Schurr, U.; Reuthebuch, O.; Eckstein, F. Modified frozen elephant trunk procedure as standard approach in acute type A aortic dissection: A propensity-weighted analysis. J. Thorac. Cardiovasc. Surg. 2022, 163, 1754–1761.e3. [Google Scholar] [CrossRef] [PubMed]
- Katayama, K.; Uchida, N.; Katayama, A.; Takahashi, S.; Takasaki, T.; Kurosaki, T.; Imai, K.; Sueda, T. Multiple factors predict the risk of spinal cord injury after the frozen elephant trunk technique for extended thoracic aortic disease. Eur. J. Cardio-Thorac. Surg. 2014, 47, 616–620. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roselli, E.E.; Bakaeen, F.G.; Johnston, D.R.; Soltesz, E.G.; Tong, M.Z. Role of the frozen elephant trunk procedure for chronic aortic dissection. Eur. J. Cardio-Thorac. Surg. 2017, 51, i35–i39. [Google Scholar] [CrossRef] [Green Version]
- Kozlov, B.N.; Panfilov, D.S.; Ponomarenko, I.V.; Miroshnichenko, A.G.; A Nenakhova, A.; I Maksimov, A.; Shipulin, V.M. The risk of spinal cord injury during the frozen elephant trunk procedure in acute aortic dissection. Interact. Cardiovasc. Thorac. Surg. 2018, 26, 972–976. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liakopoulos, O.J. Commentary: Spinal Cord Injury after the Frozen Elephant Trunk Procedure: Are We Really Safe Now? J. Thorac. Cardiovasc. Surg. 2020, 159, 1199–1200. [Google Scholar] [CrossRef] [Green Version]
- Spanos, K.; Kölbel, T.; Kubitz, J.C.; Wipper, S.; Konstantinou, N.; Heidemann, F.; Rohlffs, F.; Debus, S.E.; Tsilimparis, N. Risk of spinal cord ischemia after fenestrated or branched endovascular repair of complex aortic aneurysms. J. Vasc. Surg. 2019, 69, 357–366. [Google Scholar] [CrossRef] [PubMed]
- Sosnowski, P.; Mikrut, K.; Krauss, H. Hypothermia—Mechanism of action and pathophysiological changes in the human body. Postępy Hig. I Med. Doświadczalnej 2015, 69, 69–79. [Google Scholar] [CrossRef]
- Barnett, H.J.; Mohr, J.P.; Stein, B.M.; Yatsu, F.M. (Eds.) Spinal Cord Ischemia. In Stroke Pathophysiology, Diagnosis, and Management; Churchill Livingstone: Philadelphia, PA, USA, 1998; p. 423. [Google Scholar]
- Radiology Key. Spinal Cord Infarction. 2022. Available online: https://radiologykey.com/spinal-cord-infarction/ (accessed on 13 June 2022).
- Ius, F.; Hagl, C.; Haverich, A.; Pichlmaier, M. Elephant trunk procedure 27 years after Borst: What remains and what is new? Eur. J. Cardio-Thorac. Surg. 2011, 40, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Uchida, N.; Shibamura, H.; Katayama, A.; Sutoh, M.; Kuraoka, M.; Ishihara, H. Long-term results of the frozen elephant trunk technique for the extensive arteriosclerotic aneurysm. J. Thorac. Cardiovasc. Surg. 2010, 139, 913–917. [Google Scholar] [CrossRef]
- Dagenais, F.; Shetty, R.; Normand, J.-P.; Turcotte, R.; Mathieu, P.; Voisine, P. Extended Applications of Thoracic Aortic Stent Grafts. Ann. Thorac. Surg. 2006, 82, 567–572. [Google Scholar] [CrossRef] [PubMed]
- Chan, Y.C.; Cheng, S.W.; Ting, A.C.; Ho, P. Supra-aortic hybrid endovascular procedures for complex thoracic aortic disease: Single center early to midterm results. J. Vasc. Surg. 2008, 48, 571–579. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Etz, C. Spinale Ischämie. Gefässchirurgie 2017, 22, 81–82. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Total (n = 31) | SCI (n = 4) | Non-SCI (n = 27) | p-Value |
|---|---|---|---|---|
| Demographic characteristic | ||||
| Age (years), mean ± SD | 57.1 ± 1.6 | 62.5 ± 3 | 62.5 ± 3 | 0.379 |
| Female gender, n (%) | 6 (19.3) | 3 (75) | 3 (11.1) | 0.016 |
| BMI (kg/m2), mean ± SD | 27.7 ± 0.90 | 24.6 ± 0.66 | 27 ± 0.98 | 0.272 |
| Medical history, n (%) | ||||
| Hypertension | 22 (70.9) | 2 (50) | 20 (74.0) | 0.560 |
| Previous stroke/TIA | 2 (6.4) | 0 (0) | 2 (7.4) | 0.747 |
| COPD | 3 (9.6) | 1 (25.0) | 2 (7.4) | 0.349 |
| Diabetes | 1 (3.2) | 0 (0) | 1 (3.7) | 0.871 |
| Coronary artery disease | 6 (19.3) | 1 (25.0) | 5 (18.5) | 0.745 |
| Chronic heart disease | 2 (6.4) | 0 (0) | 2 (7.4) | 0.755 |
| Current/previous smoker | 9 (29.0) | 2 (50) | 7 (25.9) | 0.345 |
| Atrial fibrillation | 5 (16.1) | 1 (25) | 4 (14.8) | 0.525 |
| Preoperative cerebral ischemia | 0 | 0 | 0 | 0 |
| Postoperative visceral ischemia | 5 (16.1) | 0 (0) | 5 (18.5) | 0.589 |
| Medication treatment, n (%) | ||||
| ß-blocker | 12 (38.7) | 0 (0) | 12 (44.4) | 0.121 |
| ACE inhibitor | 5 (16.1) | 0 (0) | 5 (18.5) | 0.475 |
| Aspirin | 5 (16.1) | 1 (25) | 4 (14.8) | 0.553 |
| Statin | 4 (12.9) | 0 (0) | 4 (14.8) | 0.558 |
| Anticoagulation | 2 (6.4) | 0 (0) | 2 (7.4) | 0.747 |
| Variable | Total (n = 31) | SCI (n = 4) | Non-SCI (n = 27) | p-Value |
|---|---|---|---|---|
| CPB time (min) (mean ± SD) | 216.4 ± 8.0 | 209.7 ± 6.4 | 217,5 ± 9.4 | 0.743 |
| Aorta clamping time (min) (mean ± SD) | 138 ± 9.1 | 140.7 ± 10.7 | 137.6 ± 10.5 | 0.908 |
| Hypothermic circulatory arrest time (min) (mean ± SD) | 49.2 ± 1.7 | 54.5 ± 8.8 | 48.4 ± 1.5 | 0.240 |
| CABG, n (%) | 2 (6.4) | 0 | 2 (7.4) | 0.755 |
| Concomitant aortic valve replacement, n (%) | 20 (64.5) | 4 (100) | 16(59.2) | 0.237 |
| PRBC units (mean ± SD) | 9.7 ± 1.1 | 9 ± 1.0 | 9.8 ± 1.2 | 0.809 |
| PC units (mean ± SD) | 2.3 ± 0.45 | 1 ± 0.40 | 2.5 ± 0.50 | 0.268 |
| Fibrinogen units (mean ± SD) | 5.1 ± 0.44 | 4.2 ± 0.62 | 5.3 ± 0.50 | 0.419 |
| PL units (mean ± SD) | 4.6 ± 1.1 | 2.2 ± 1.3 | 4.9 ± 1.3 | 0.452 |
| PCC units (mean ± SD) | 4 ± 0.58 | 2.5 ± 1.04 | 4.2 ± 0.64 | 0.291 |
| FET prothesis length 150 mm | 11 (0.35) | 1 (0.25) | 10 (37.0) | 0.712 |
| Variable | Total (n = 31) | SCI (n = 4) | Non-SCI (n = 27) | p-Value |
|---|---|---|---|---|
| Laboratory data | ||||
| Creatinine (mg/dL) | 0.96 ± 0.06 | 1.0 ± 0.06 | 0.667 ± 0.08 | 0.032 |
| Hemoglobin (mg/dL) | 13.2 ± 0.34 | 11.3 ± 1.5 | 13.5 ± 0.3 | 0.29 |
| Platelet count (×1000/μL) | 199.5 ± 16.73 | 288 ± 113.6 | 188 ± 12.4 | 0.472 |
| Risk factor for SCI, n (%) | ||||
| Hypoxemia (day 0) (mmHg) | 5 (16.1) | 1 (25.0) | 4 (14.8) | 0.553 |
| Hypoxemia (POD 1) (mmHg) | 11 (35.4) | 2 (50.0) | 9 (33.3) | 0.336 |
| Hypoxemia (POD 2) (mmHg) | 13 (41.9) | 3 (75.0) | 10 (37.0) | 0.124 |
| Hypoxemia (POD 3) (mmHg) | 26 (83.8) | 3 (75.0) | 23 (85.1) | 0.454 |
| Hypotension (day 0) (mmHg) | 26 (83.8) | 3 (75.0) | 23 (85.1) | 0.454 |
| Hypotension (POD 1) (mmHg) | 1 (3.2) | 0 (0) | 1 (3.7) | 0.871 |
| Hypotension (POD 2) (mmHg) | 18 (58.0) | 2 (50.0) | 16 (59.2) | 0.452 |
| Hypotension (POD 3) (mmHg) | 12 (38.7) | 2 (50.0) | 10 (37.0) | 0.705 |
| Dominating left vertebral artery | 16 (51.6) | 1(25.0) | 15(55.5) | 0.275 |
| Postoperative cerebral ischemia | 4 (12.9) | 1 (0.25) | 3 (11.1) | 0.429 |
| Postoperative visceral ischemia | 9 (29.0) | 2 (50) | 7 (25.9) | 0.429 |
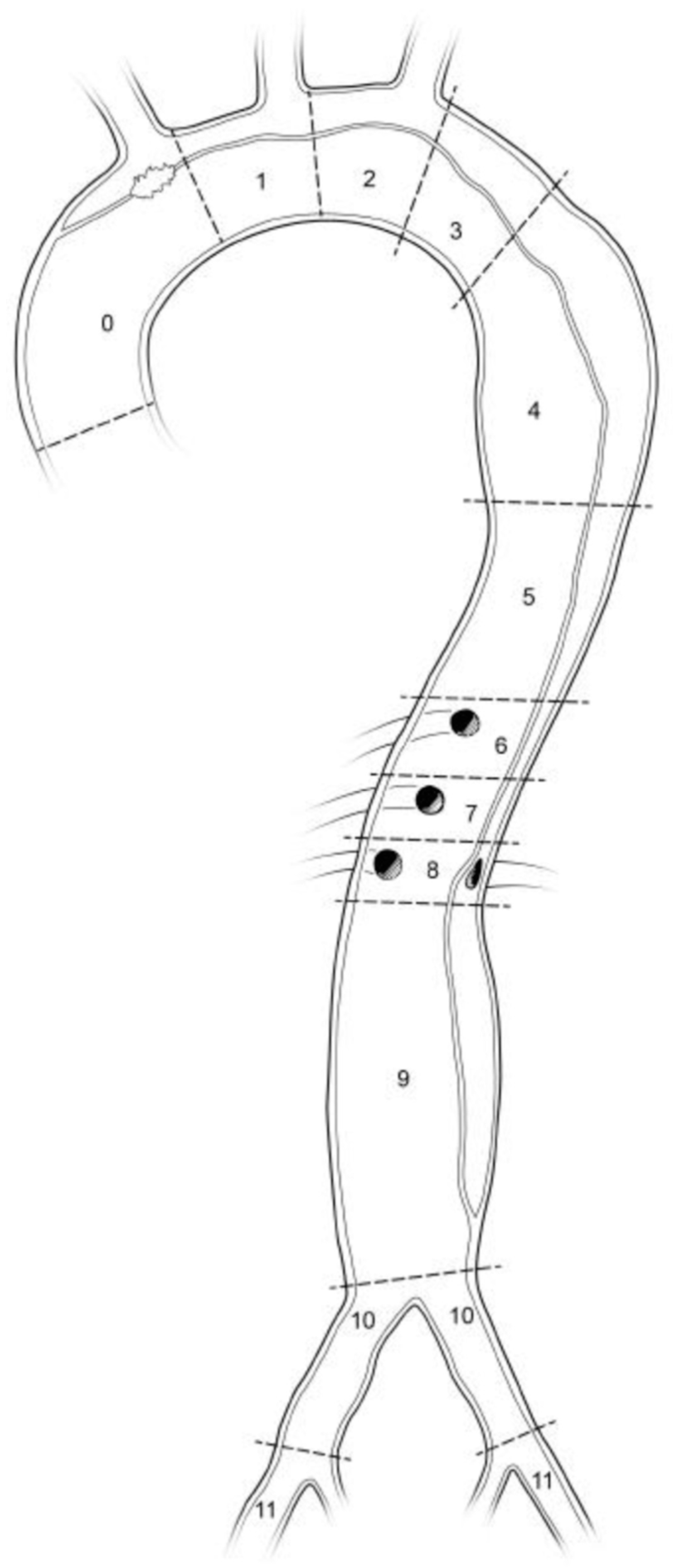
| Thrombosis extension in false lumen, n (%) | ||||
| Zones 3–4 | 24 (77.4) | 0 (0) | 24 (88.8) | |
| Zones 5–6 | 5 (16.1) | 2 (50.0) | 3 (11.1) | |
| Zones 7–9 | 2 (6.4) | 2 (50.0) | 0 (0) | 0.002 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cuellar, F.L.; Oberhuber, A.; Martens, S.; Rukosujew, A.; Marchiori, E.; Ibrahim, A. Analysis of Spinal Ischemia after Frozen Elephant Trunk for Acute Aortic Dissection: An Observational, Single-Center Study. Diagnostics 2022, 12, 2781. https://doi.org/10.3390/diagnostics12112781
Cuellar FL, Oberhuber A, Martens S, Rukosujew A, Marchiori E, Ibrahim A. Analysis of Spinal Ischemia after Frozen Elephant Trunk for Acute Aortic Dissection: An Observational, Single-Center Study. Diagnostics. 2022; 12(11):2781. https://doi.org/10.3390/diagnostics12112781
Chicago/Turabian StyleCuellar, Frederico Lomonaco, Alexander Oberhuber, Sven Martens, Andreas Rukosujew, Elena Marchiori, and Abdulhakim Ibrahim. 2022. "Analysis of Spinal Ischemia after Frozen Elephant Trunk for Acute Aortic Dissection: An Observational, Single-Center Study" Diagnostics 12, no. 11: 2781. https://doi.org/10.3390/diagnostics12112781
APA StyleCuellar, F. L., Oberhuber, A., Martens, S., Rukosujew, A., Marchiori, E., & Ibrahim, A. (2022). Analysis of Spinal Ischemia after Frozen Elephant Trunk for Acute Aortic Dissection: An Observational, Single-Center Study. Diagnostics, 12(11), 2781. https://doi.org/10.3390/diagnostics12112781