
Water Fraction Ratio of the Sacroiliac Joint Subchondral Bone Marrow in Patients with Ankylosing Spondylitis Predicts the Degree of Disease Activity

Abstract
:1. Introduction
2. Methods
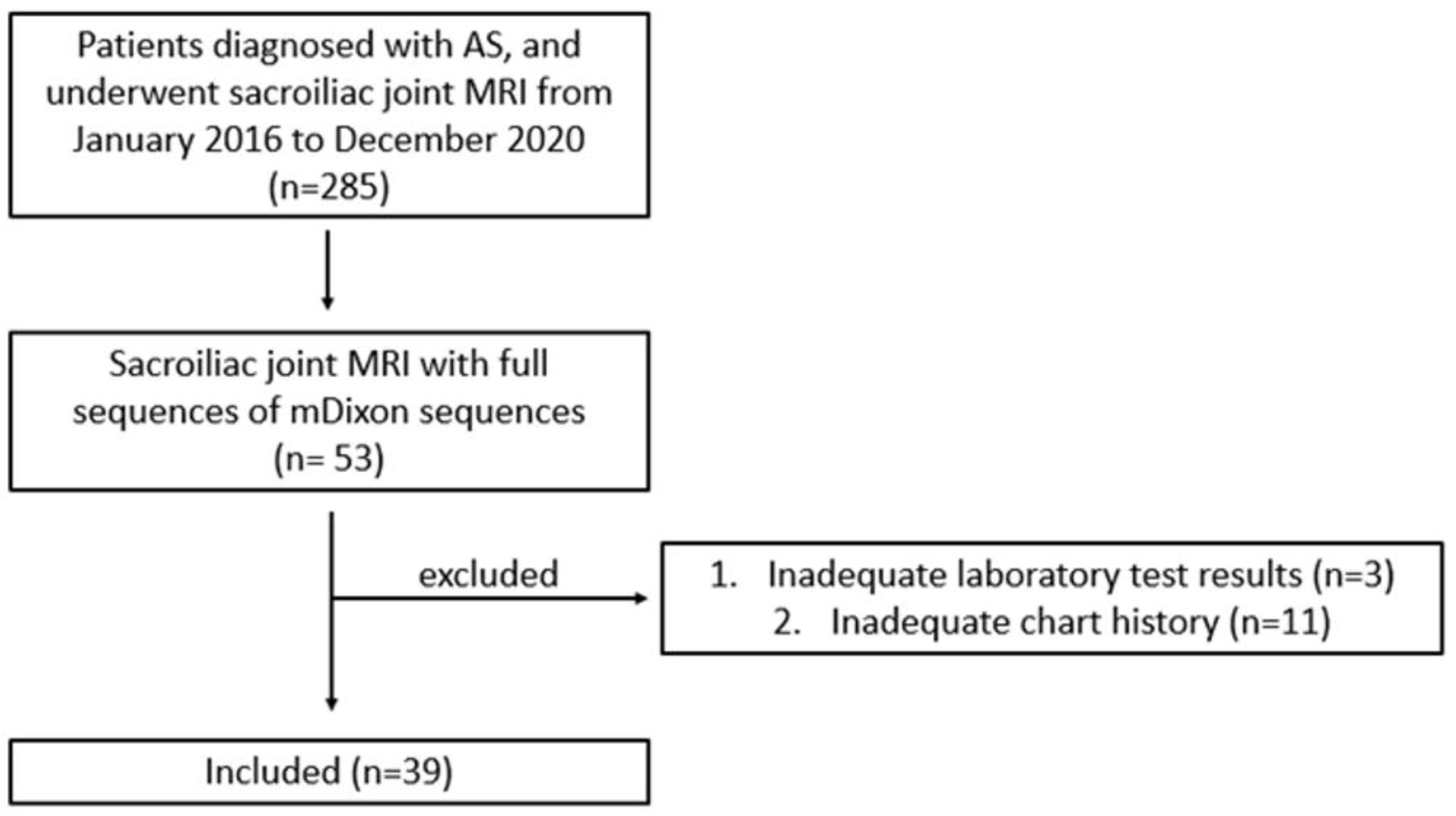
2.1. Study Population
2.2. Imaging Protocol and Reconstruction
2.3. Image Analyses
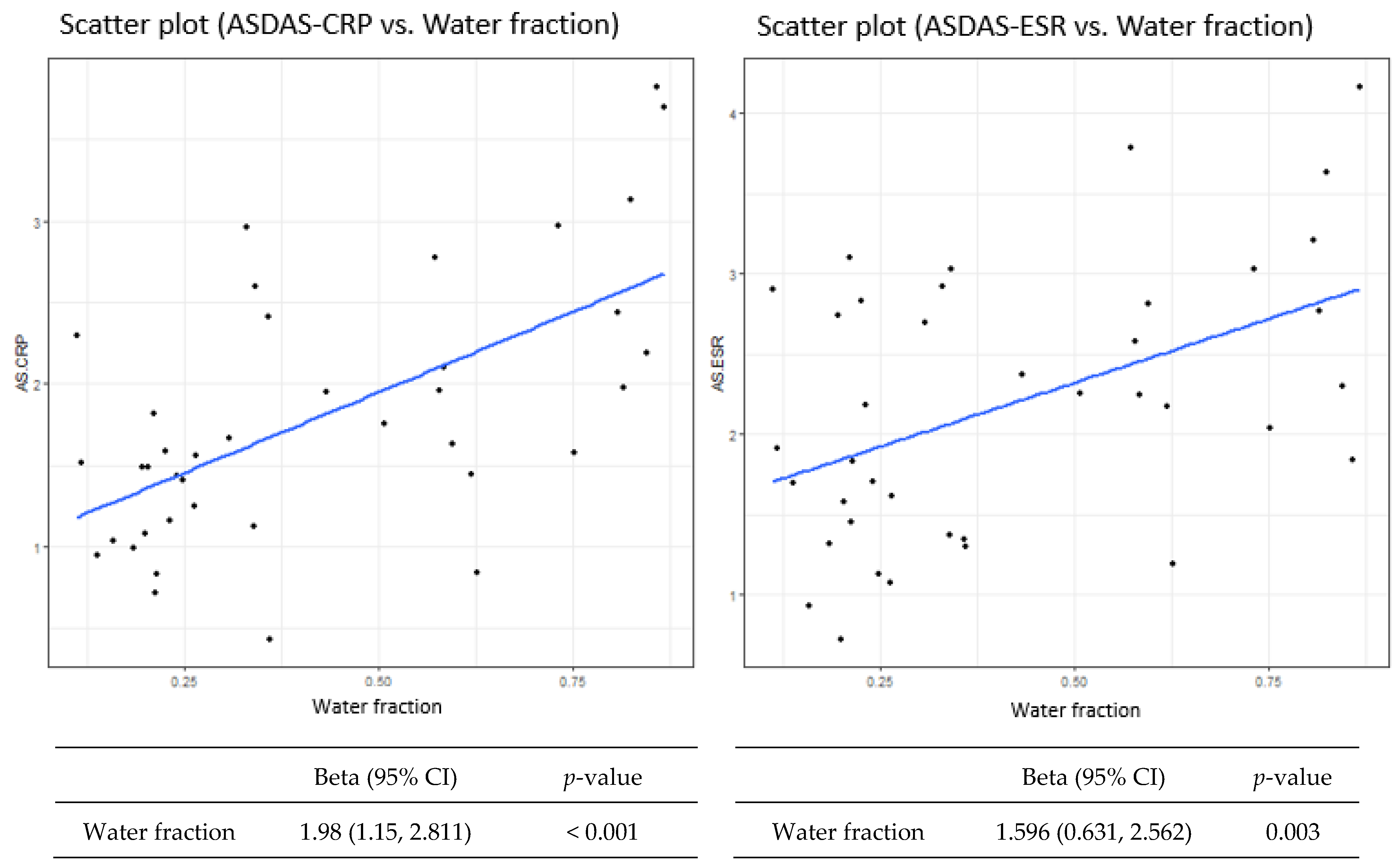
2.4. Statistical Analyses
3. Results
4. Discussion
- Water fraction parameters can be derived from mDixon MRI and can provide quantitative parameter of disease activity in ankylosing spondylitis patients.
- Retrospective study showed good correlation between the water fraction parameters with ASDAS scores.
- Water fraction could be utilized for therapeutic planning and treatment monitoring in ankylosing spondylitis patients when combined with conventional disease activity evaluations.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Braun, J.; Sieper, J. Ankylosing spondylitis. Lancet 2007, 369, 1379–1390. [Google Scholar] [CrossRef]
- Lipton, S.; Deodhar, A. The new ASAS classification criteria for axial and peripheral spondyloarthritis: Promises and pitfalls. Int. J. Clin. Rheumatol. 2012, 7, 675–682. [Google Scholar] [CrossRef]
- Rudwaleit, M.; van der Heijde, D.; Landewe, R.; Listing, J.; Akkoc, N.; Brandt, J.; Braun, J.; Chou, C.T.; Collantes-Estevez, E.; Dougados, M.; et al. The development of Assessment of SpondyloArthritis international Society classification criteria for axial spondyloarthritis (part II): Validation and final selection. Ann. Rheum. Dis. 2009, 68, 777–783. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Proft, F.; Poddubnyy, D. Ankylosing spondylitis and axial spondyloarthritis: Recent insights and impact of new classification criteria. Ther. Adv. Musculoskelet. Dis. 2018, 10, 129–139. [Google Scholar] [CrossRef]
- Zhu, W.; He, X.X.; Cheng, K.Y.; Zhang, L.J.; Chen, D.; Wang, X.; Qiu, G.X.; Cao, X.; Weng, X.S. Ankylosing spondylitis: Etiology, pathogenesis, and treatments. Bone Res. 2019, 7, 22. [Google Scholar] [CrossRef] [Green Version]
- Spoorenberg, A.; van Tubergen, A.; Landewe, R.; Dougados, M.; van der Linden, S.; Mielants, H.; van de Tempel, H.; van der Heijde, D. Measuring disease activity in ankylosing spondylitis: Patient and physician have different perspectives. Rheumatology 2005, 44, 789–795. [Google Scholar] [CrossRef] [Green Version]
- Machado, P.M.; Landewe, R.; Heijde, D.V.; Assessment of SpondyloArthritis international Society. Ankylosing Spondylitis Disease Activity Score (ASDAS): 2018 update of the nomenclature for disease activity states. Ann. Rheum. Dis. 2018, 77, 1539–1540. [Google Scholar] [CrossRef]
- Machado, P.; Landewe, R.; Lie, E.; Kvien, T.K.; Braun, J.; Baker, D.; van der Heijde, D.; Assessment of SpondyloArthritis international Society. Ankylosing Spondylitis Disease Activity Score (ASDAS): Defining cut-off values for disease activity states and improvement scores. Ann. Rheum. Dis. 2011, 70, 47–53. [Google Scholar] [CrossRef] [Green Version]
- Tsoi, C.; Griffith, J.F.; Lee, R.K.L.; Wong, P.C.H.; Tam, L.S. Imaging of sacroiliitis: Current status, limitations and pitfalls. Quant. Imaging Med. Surg. 2019, 9, 318–335. [Google Scholar] [CrossRef]
- Lambert, R.G.; Bakker, P.A.; van der Heijde, D.; Weber, U.; Rudwaleit, M.; Hermann, K.G.; Sieper, J.; Baraliakos, X.; Bennett, A.; Braun, J.; et al. Defining active sacroiliitis on MRI for classification of axial spondyloarthritis: Update by the ASAS MRI working group. Ann. Rheum. Dis. 2016, 75, 1958–1963. [Google Scholar] [CrossRef]
- Huang, Z.G.; Zhang, X.Z.; Wen, H.; Wang, G.C.; Zhou, H.Q.; Xin, L.; Wu, W. The application of MR imaging in the detection of hip involvement in patients with ankylosing spondylitis. Eur. J. Radiol. 2013, 82, 1487–1493. [Google Scholar] [CrossRef] [PubMed]
- MacEwan, I.J.; Glembotski, N.E.; D’Lima, D.; Bae, W.; Masuda, K.; Rashidi, H.H.; Mell, L.K.; Bydder, M. Proton density water fraction as a biomarker of bone marrow cellularity: Validation in ex vivo spine specimens. Magn. Reson. Imaging 2014, 32, 1097–1101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.H.; Lee, Y.H.; Hahn, S.; Suh, J.S. Fat fraction estimation of morphologically normal lumbar vertebrae using the two-point mDixon turbo spin-echo MRI with flexible echo times and multipeak spectral model of fat: Comparison between cancer and non-cancer patients. Magn. Reson. Imaging 2016, 34, 1114–1120. [Google Scholar] [CrossRef] [PubMed]
- Bray, T.J.P.; Bainbridge, A.; Punwani, S.; Ioannou, Y.; Hall-Craggs, M.A. Simultaneous Quantification of Bone Edema/Adiposity and Structure in Inflamed Bone Using Chemical Shift-Encoded MRI in Spondyloarthritis. Magn. Reson. Med. 2018, 79, 1031–1042. [Google Scholar] [CrossRef] [Green Version]
- Bray, T.J.P.; Chouhan, M.D.; Punwani, S.; Bainbridge, A.; Hall-Craggs, M.A. Fat fraction mapping using magnetic resonance imaging: Insight into pathophysiology. Br. J. Radiol. 2018, 91, 20170344. [Google Scholar] [CrossRef] [Green Version]
- Bray, T.J.P.; Sakai, N.; Dudek, A.; Fisher, C.; Rajesparan, K.; Lopes, A.; Ciurtin, C.; Sen, D.; Bainbridge, A.; Hall-Craggs, M.A. Histographic analysis of oedema and fat in inflamed bone marrow based on quantitative MRI. Eur. Radiol. 2020, 30, 5099–5109. [Google Scholar] [CrossRef] [Green Version]
- Guo, R.M.; Lin, W.S.; Liu, W.M.; Zhou, W.Y.; Cao, S.E.; Wang, J.; Li, Q.L. Quantification of fat infiltration in the sacroiliac joints with ankylosing spondylitis using IDEAL sequence. Clin. Radiol. 2018, 73, 231–236. [Google Scholar] [CrossRef]
- Koo, B.S.; Song, Y.; Shin, J.H.; Lee, S.; Ki, T.H. Evaluation of disease chronicity by bone marrow fat fraction using sacroiliac joint magnetic resonance imaging in patients with spondyloarthritis: A retrospective study. Int. J. Rheum. Dis. 2019, 22, 734–741. [Google Scholar] [CrossRef]
- Zhao, Y.H.; Li, S.L.; Liu, Z.Y.; Chen, X.; Zhao, X.C.; Hu, S.Y.; Liu, Z.H.; Mei, M.S.Y.J.; Chan, Q.; Liang, C.H. Detection of Active Sacroiliitis with Ankylosing Spondylitis through Intravoxel Incoherent Motion Diffusion-Weighted MR Imaging. Eur. Radiol. 2015, 25, 2754–2763. [Google Scholar] [CrossRef]
- Bradbury, L.A.; Hollis, K.A.; Gautier, B.; Shankaranarayana, S.; Robinson, P.C.; Saad, N.; Lê Cao, K.A.; Brown, M.A. Diffusion-weighted imaging is a sensitive and specific magnetic resonance sequence in the diagnosis of ankylosing spondylitis. J. Rheumatol. 2018, 45, 771–778. [Google Scholar] [CrossRef]
- Sanal, H.T.; Yilmaz, S.; Simsek, I.; Cinar, M.; Erdem, H.; Pay, S.; Dinc, A.; Tayfun, C. Apparent diffusion coefficients of sacroiliitis in patients with established ankylosing spondylitis. Clin. Imaging 2013, 37, 734–739. [Google Scholar] [CrossRef] [PubMed]
- Du, M.S.; Xiong, X.Q.; Liu, H.; Qin, X.; Hu, X.F.; Chen, W. The evaluation of bone marrow edema in sacroiliac joint in patients with ankylosing spondylitis using magnetic resonance imaging Dixon sequence. BMC Musculoskelet. Disord. 2021, 22, 919. [Google Scholar] [CrossRef] [PubMed]
- Bray, T.J.; Jones, A.; Bennett, A.N.; Conaghan, P.G.; Grainger, A.; Hodgson, R.; Hutchinson, C.; Leandro, M.; Mandl, P.; McGonagle, D.; et al. Recommendations for acquisition and interpretation of MRI of the spine and sacroiliac joints in the diagnosis of axial spondyloarthritis in the UK. Rheumatology 2019, 58, 1831–1838. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (N = 39) | |
|---|---|
| Age, mean ± SD years | 39.1 ± 14.4 |
| Male, n (%) | 18 (46.2) |
| HLA-B27 positivity, n (%) | 20 (51.3%) |
| CRP, mean ± SD | 6.98 ± 14.3 |
| ESR, mean ± SD | 24.4 ± 28.2 |
| ASDAS-CRP, mean ± SD | 1.80 ± 0.80 |
| ASDAS-ESR, mean ± SD | 2.20 ± 0.84 |
| Water fraction, mean ± SD | 42.3 ± 24.8 |
| Bone erosions, n (%) | 15 (38.5%) |
| Fatty infiltrations, n (%) | 10 (25.6%) |
| Sclerosis, n (%) | 15 (38.5%) |
| Ankylosis, n (%) | 3 (7.7%) |
| Joint space alterations, n (%) | 8 (20.5%) |
| Bone marrow enhancement, n (%) | 13 (33.3%) |
| Joint effusion, n (%) | 1 (2.6%) |
| Enthesitis, n (%) | 5 (12.8%) |
| Uveitis, n (%) | 4 (10.3%) |
| ASDAS-CRP | ASDAS-ESR | |||
|---|---|---|---|---|
| Variable | Beta (95% CI) | p value | Beta (95% CI) | p value |
| Age | 0.011 (−0.006 to 0.029) | 0.218 | 0.019 (0.002–0.037) | 0.039 * |
| Sex | 0.229 (−0.279 to 0.737) | 0.382 | −0.27 (−0.799 to 0.259) | 0.324 |
| Bone marrow oedema | 0.565 (0.085–1.045) | 0.027 * | 0.566 (0.062–1.07) | 0.034 * |
| HLA B27 | −0.001 (−0.513 to 0.511) | 0.998 | 0.047 (−0.488–0.581) | 0.865 |
| Fatty metaplasia | −0.204 (−0.786 to 0.378) | 0.497 | −0.266 (−0.872 to 0.34) | 0.395 |
| Bone Erosion | 0.773 (0.31–1.237) | 0.002 * | 0.791 (0.304–1.278) | 0.003 * |
| Sclerosis | 0.153 (−0.371 to 0.677) | 0.57 | 0.092 (−0.456 to 0.641) | 0.743 |
| Ankylosis | 0.659 (−0.278 to 1.595) | 0.176 | 0.576 (−0.41 to 1.562) | 0.26 |
| Joint space alteration | 0.086 (−0.547, 0.719) | 0.791 | 0.071 (−0.591, 0.732) | 0.836 |
| Bone marrow enhancement | 0.589 (0.081, 1.098) | 0.029 * | 0.631 (0.101, 1.16) | 0.025 * |
| Joint space fluid | −0.981 (−2.569 to 0.607) | 0.233 | −1.034 (−2.692 to 0.624) | 0.229 |
| Enthesitis | 0.48 (−0.27–1.229) | 0.218 | 0.576 (−0.202 to 1.354) | 0.155 |
| Uveitis | 0.198 (−0.643 to 1.039) | 0.647 | 0.425 (−0.445 to 1.296) | 0.344 |
| ASDAS-CRP > 1.3 | ASDAS-ESR > 1.3 | |||
|---|---|---|---|---|
| Variable | Odds ratio (95% CI) | p value | Odds ratio (95% CI) | p value |
| Age | 1.024 (0.972–1.079) | 0.374 | 1.025 (0.959–1.095) | 0.468 |
| Sex | 1.04 (0.256–4.218) | 0.956 | 0.368 (0.059, 2.302) | 0.285 |
| Bone marrow oedema | 3.077 (0.673–14.077) | 0.147 | 1.882 (0.302–11.728) | 0.498 |
| Water fraction | 177.68 | 0.028 * | 15.222 | 0.239 |
| HLA B27 | 0.495 (0.118–2.081) | 0.337 | 1.062 (0.187–6.052) | 0.946 |
| Fatty metaplasia | 0.889 (0.183–4.31) | 0.884 | 0.269 (0.044–1.637) | 0.154 |
| Bone Erosion | 26.407 (1.292–539.639) | 0.001 * | 10.892(0.517–9.567) | 0.036 * |
| Sclerosis | 0.667 (0.162–2.748) | 0.575 | 1.3 (0.207–8.148) | 0.779 |
| Ankylosis | 3.157 (0.096–103.877) | 0.404 | 1.492 (0.044–50.786) | 0.791 |
| Joint space alteration | 1.227 (0.207–7.265) | 0.821 | 0.444 (0.066–3.014) | 0.406 |
| Marrow enhancement | 2.912 (0.527–16.093) | 0.22 | 1 (0.158–6.329) | >0.999 |
| Joint space fluid | 0.123 (0.001–12.008) | 0.169 | 0.055 (0.001–5.541) | 0.062 |
| Enthesitis | 5.383 (0.208–138.985) | 0.179 | 0.69 (0.063–7.512) | 0.76 |
| Uveitis | 1.2 (0.111–12.953) | 0.881 | 0.5 (0.043–5.813) | 0.58 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, B.J.; Lee, Y.H.; Lee, J.; Kim, S.; Song, H.-T. Water Fraction Ratio of the Sacroiliac Joint Subchondral Bone Marrow in Patients with Ankylosing Spondylitis Predicts the Degree of Disease Activity. Diagnostics 2022, 12, 2842. https://doi.org/10.3390/diagnostics12112842
Kim BJ, Lee YH, Lee J, Kim S, Song H-T. Water Fraction Ratio of the Sacroiliac Joint Subchondral Bone Marrow in Patients with Ankylosing Spondylitis Predicts the Degree of Disease Activity. Diagnostics. 2022; 12(11):2842. https://doi.org/10.3390/diagnostics12112842
Chicago/Turabian StyleKim, Beum Jin, Young Han Lee, Joohee Lee, Sungjun Kim, and Ho-Taek Song. 2022. "Water Fraction Ratio of the Sacroiliac Joint Subchondral Bone Marrow in Patients with Ankylosing Spondylitis Predicts the Degree of Disease Activity" Diagnostics 12, no. 11: 2842. https://doi.org/10.3390/diagnostics12112842
APA StyleKim, B. J., Lee, Y. H., Lee, J., Kim, S., & Song, H. -T. (2022). Water Fraction Ratio of the Sacroiliac Joint Subchondral Bone Marrow in Patients with Ankylosing Spondylitis Predicts the Degree of Disease Activity. Diagnostics, 12(11), 2842. https://doi.org/10.3390/diagnostics12112842