
Predictive Factors of Adequate Bowel Cleansing for Colonoscopy in the Elderly: A Retrospective Analysis of a Prospective Cohort

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Techniques
2.3. Outcomes and Measurement
2.4. Statistical Analysis
2.5. Ethics
3. Results
3.1. Study Population and Characteristics
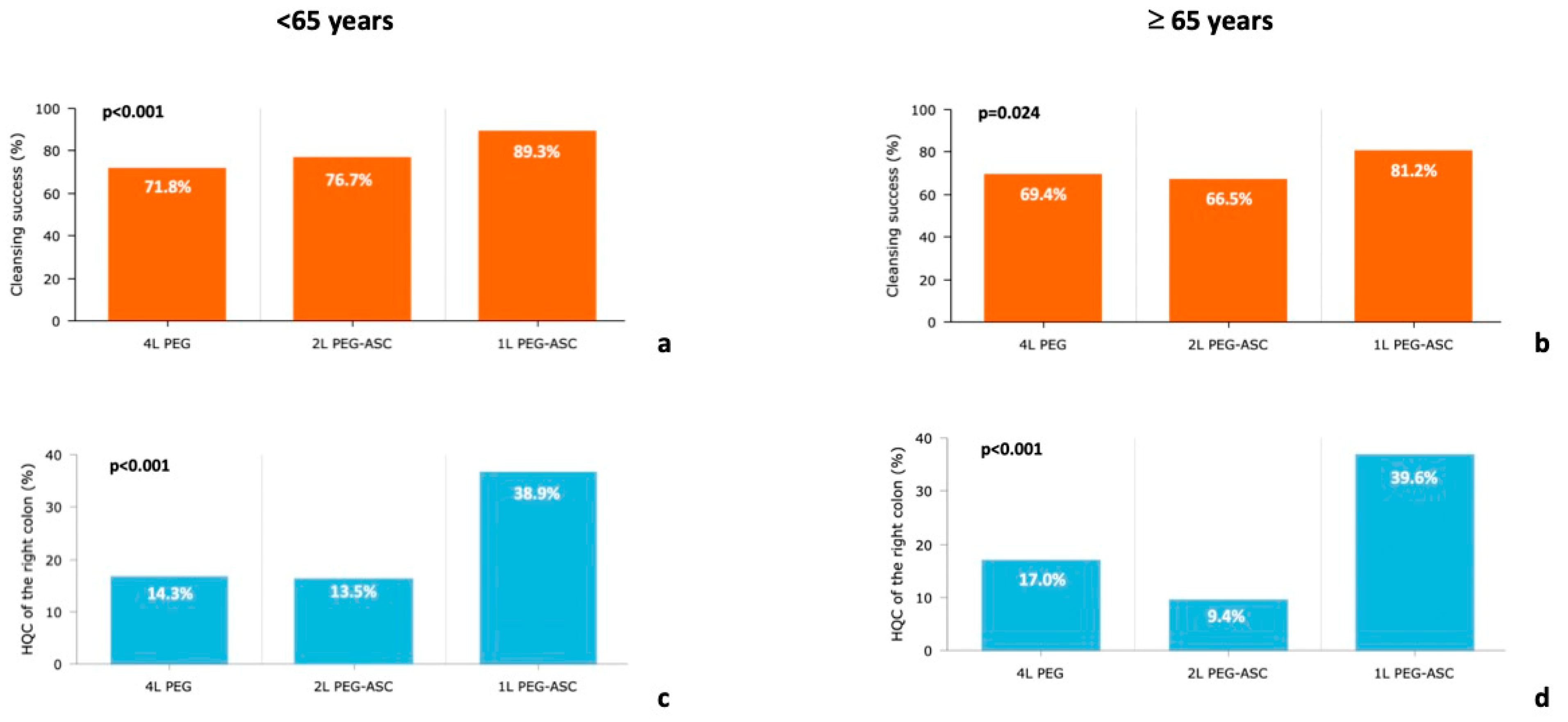
3.2. Bowel Cleansing Efficacy
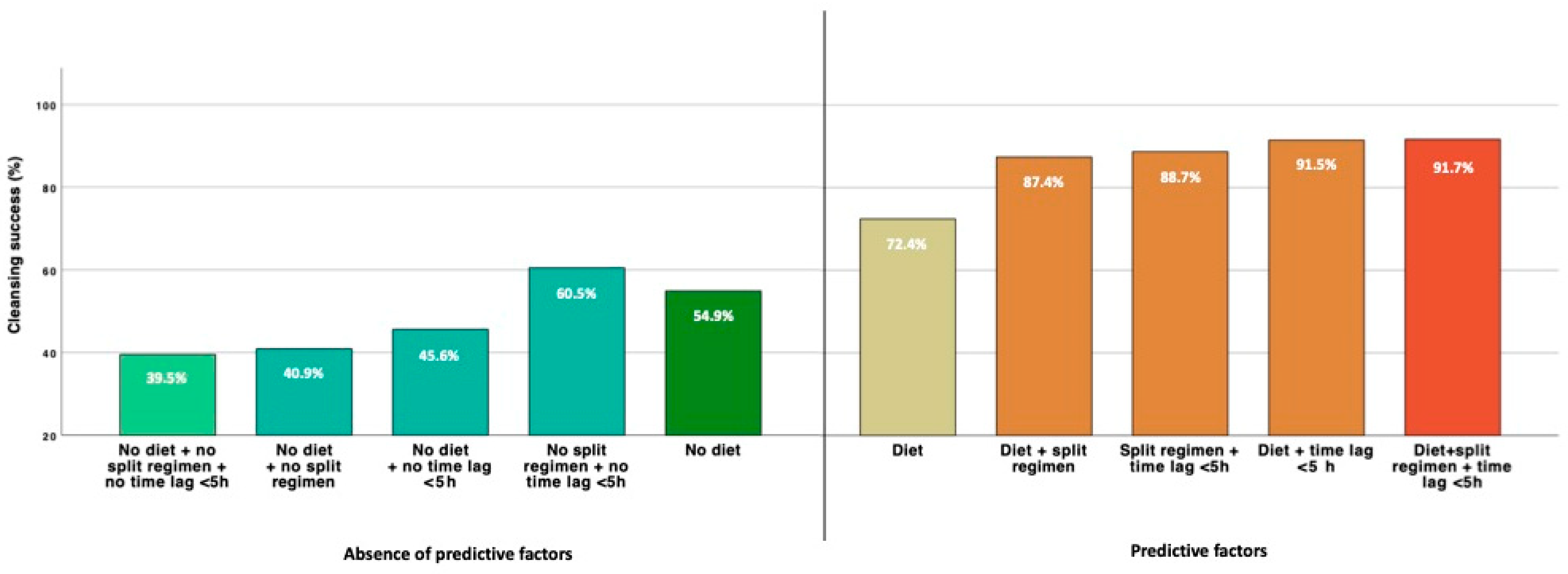
3.3. Predictors of Bowel Cleansing in the Elderly
3.4. Safety
4. Discussion
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Conflicts of Interest
References
- Løberg, M.; Kalager, M.; Holme, Ø.; Hoff, G.; Adami, H.O.; Bretthauer, M. Long-term colorectal-cancer mortality after adenoma removal. N. Engl. J. Med. 2014, 371, 799–807. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baxter, N.N.; Goldwasser, M.A.; Paszat, L.F.; Saskin, R.; Urbach, D.R.; Rabeneck, L. Association of colonoscopy and death from colorectal cancer. Ann. Intern. Med. 2009, 150, 1–8. [Google Scholar] [CrossRef]
- Sulz, M.C.; Kröger, A.; Prakash, M.; Manser, C.N.; Heinrich, H.; Misselwitz, B. Meta-analysis of the effect of bowel preparation on adenoma detection: Early adenomas affected stronger than advanced adenomas. PLoS ONE 2016, 11, e0154149. [Google Scholar] [CrossRef] [Green Version]
- Hassan, C.; Manning, J.; Álvarez González, M.A.; Sharma, P.; Epstein, M.; Bisschops, R. Improved detection of colorectal adenomas by high-quality colon cleansing. Endosc. Int. Open 2020, 8, E928–E937. [Google Scholar] [CrossRef]
- Clark, B.T.; Laine, L. High-quality bowel preparation is required for detection of sessile serrated polyps. Clin. Gastroenterol. Hepatol. 2016, 14, 1155–1162. [Google Scholar] [CrossRef] [Green Version]
- Rex, D.K.; Imperiale, T.F.; Latinovich, D.R.; Bratcher, L.L. Impact of bowel preparation on efficiency and cost of colonoscopy. Am. J. Gastroenterol. 2002, 97, 1696–1700. [Google Scholar] [CrossRef]
- Froehlich, F.; Wietlisbach, V.; Gonvers, J.J.; Burnand, B.; Vader, J.P. Impact of colonic cleansing on quality and diagnostic yield of colonoscopy: The European Panel of Appropriateness of Gastrointestinal Endos- copy European multicenter study. Gastrointest. Endosc. 2005, 61, 378–384. [Google Scholar] [CrossRef]
- Wexner, S.D.; Beck, D.E.; Baron, T.H.; Fanelli, R.D.; Hyman, N.; Shen, B.; Wasco, K.E. A consensus document on bowel preparation before colonoscopy: Prepared by a task force from the American Society of Colon and Rectal Surgeons (ASCRS), the American Society for Gastrointestinal Endoscopy (ASGE), and the Society of American Gastrointestinal and Endoscopic Surgeons (SAGES). Gastrointest. Endosc. 2006, 63, 894–909. [Google Scholar] [PubMed]
- Hillyer, G.C.; Basch, C.H.; Lebwohl, B.; Basch, C.E.; Kastrinos, F.; Insel, B.J.; Neugut, A.I. Shortened surveillance intervals following suboptimal bowel preparation for colonoscopy: Results of a national survey. Int. J. Color. Dis. 2013, 28, 73–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahmood, S.; Farooqui, S.M.; Madhoun, M.F. Predictors of inadequate bowel preparation for colonoscopy: A systematic review and meta-analysis. Eur. J. Gastroenterol. Hepatol. 2018, 30, 819–826. [Google Scholar] [CrossRef]
- Hassan, C.; Fuccio, L.; Bruno, M.; Pagano, N.; Spada, C.; Carrara, S.; Giordanino, C.; Rondonotti, E.; Curcio, G.; Dulbecco, P.; et al. A predictive model identifies patients most likely to have inadequate bowel preparation for colonoscopy. Clin. Gastroenterol. Hepatol. 2012, 10, 501–506. [Google Scholar] [CrossRef] [PubMed]
- Hassan, C.; East, J.; Radaelli, F.; Spada, C.; Benamouzig, R.; Bisschops, R.; Bretthauer, M.; Dekker, E.; Dinis-Ribeiro, M.; Ferlitsch, M.; et al. Bowel preparation for colonoscopy: European Society of Gastrointestinal Endoscopy (ESGE) Guideline-Update 2019. Endoscopy 2019, 51, 775–794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maida, M.; Sinagra, E.; Morreale, G.C.; Sferrazza, S.; Scalisi, G.; Schillaci, D.; Ventimiglia, M.; Macaluso, F.S.; Vettori, G.; Conoscenti, G.; et al. Effectiveness of very low-volume preparation for colonoscopy: A prospective, multicenter observational study. World J. Gastroenterol. 2020, 26, 1950–1961. [Google Scholar] [CrossRef] [PubMed]
- Lai, E.J.; Calderwood, A.H.; Doros, G.; Fix, O.K.; Jacobson, B.C. The Boston Bowel Preparation Scale: A valid and reliable instrument for colonoscopy-oriented re- search. Gastrointest. Endosc. 2009, 69, 620–625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Day, L.W.; Kwon, A.; Inadomi, J.M.; Walter, L.C.; Somsouk, M. Adverse events in older patients undergoing colonoscopy: A systematic review and meta-analysis. Gastrointest. Endosc. 2011, 74, 885–896. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Leo, M.; Iannone, A.; Arena, M.; Losurdo, G.; Palamara, M.A.; Iabichino, G.; Consolo, P.; Rendina, M.; Luigiano, C.; Di Leo, A. Novel frontiers of agents for bowel cleansing for colonoscopy. World J. Gastroenterol. 2021, 27, 7748–7770. [Google Scholar] [CrossRef]
- DeMicco, M.P.; Clayton, L.B.; Pilot, J.; Epstein, M.S.; Bekal, P.K.T.; Hardi, R.; Harper, W.L.; Henderson, J.B.; Jairath, V.; Jarrett, T.E.; et al. Novel 1 L polyethylene glycol-based bowel preparation NER1006 for overall and right-sided colon cleansing: A randomized controlled phase 3 trial versus trisulfate. Gastrointest. Endosc. 2018, 87, 677–687.e3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schreiber, S.; Baumgart, D.C.; Drenth, J.P.H.; Filip, R.S.; Clayton, L.B.; Hylands, K.; Repici, A.; Hassan, C.; on behalf of the DAYB Study Group. Colon cleansing efficacy and safety with 1 L NER1006 versus sodium picosulfate with magnesium citrate: A randomized phase 3 trial. Endoscopy 2019, 51, 73–84. [Google Scholar] [CrossRef]
- Bisschops, R.; Manning, J.; Clayton, L.B.; Shing, R.N.K.; Álvarez-González, M.; on behalf of the MORA Study Group. Colon cleansing efficacy and safety with 1 L NER1006 versus 2 L polyethylene glycol + ascorbate: A randomized phase 3 trial. Endoscopy 2019, 51, 60–72. [Google Scholar] [CrossRef]
- Maida, M.; Macaluso, F.S.; Sferrazza, S.; Ventimiglia, M.; Sinagra, E. Effectiveness and safety of NER1006 versus standard bowel preparations: A meta-analysis of randomized phase-3 clinical trials. Dig. Liver Dis. 2020, 52, 833–839. [Google Scholar] [CrossRef]
- Frazzoni, L.; Spada, C.; Radaelli, F.; Mussetto, A.; Laterza, L.; La Marca, M.; Piccirelli, S.; Cortellini, F.; Rondonotti, E.; Paci, V.; et al. 1L- vs. 4L-Polyethylene glycol for bowel preparation before colonoscopy among inpatients: A propensity score-matching analysis. Dig. Liver Dis. 2020, 52, 1486–1493. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.N.; Lee, C.K.; Im, J.P.; Choi, C.H.; Byeon, J.-S.; Cho, Y.-S.; Jung, S.-A.; Kim, T.I.; Jeen, Y.T. Efficacy and safety of split-dose bowel preparation with 1 L polyethylene glycol and ascorbate compared with 2 L polyethylene glycol and ascorbate in a Korean population: A phase 4, multicenter, randomized, endoscopist-blinded study. Gastrointest. Endosc. 2021, 95, 500–511.e2. [Google Scholar] [CrossRef] [PubMed]
- Repici, A.; Spada, C.; Cannizzaro, R.; Traina, M.; Maselli, R.; Maiero, S.; Galtieri, A.; Guarnieri, G.; Di Leo, M.; Lorenzetti, R.; et al. Novel 1-L polyethylene glycol + ascorbate versus high-volume polyethylene glycol regimen for colonoscopy cleansing: A multicenter, randomized, phase IV study. Gastrointest. Endosc. 2021, 94, 823–831.e9. [Google Scholar] [CrossRef] [PubMed]
- Arieira, C.; de Castro, F.D.; Carvalho, P.B.; Magalhães, J.; Xavier, S.; Sousa, C.; Rosa, B.; Cotter, J. Bowel cleansing efficacy for colonoscopy: Prospective, randomized comparative study of same-day dosing with 1-L and 2-L PEG + ascorbate. Endosc. Int. Open 2021, 09, E1602–E1610. [Google Scholar] [CrossRef] [PubMed]
- Yoon, J.Y.; Kim, H.G.; Cho, Y.S.; Kim, H.I.; Cha, J.M. 1 L- versus 2 L-polyethylene glycol with ascorbic acid for bowel preparation in elderly patients: A randomized multicenter study [published online ahead of print, 2022 Jan 15]. Surg. Endosc. 2022, 36, 5724–5733. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| <65 Years (N = 714) | ≥65 Years (N = 575) | p | |
|---|---|---|---|
| Male sex, n (%) | 363 (51.3%) | 314 (54.6%) | 0.234 |
| Age, years, mean (SD) | 50.5 ± 10.5 | 72.9 ± 5.9 | <0.001 |
| Weight, kg, mean (SD) | 72.7 ± 15.2 | 71.9 ± 13.8 | 0.335 |
| Height, cm, mean (SD) | 167.4 ± 9.2 | 163.8 ± 8.4 | <0.001 |
| BMI, mean (SD) | 25.8 ± 4.6 | 26.8 ± 4.7 | <0.001 |
| Comorbidities | |||
| - Hypertension | 167 (23.6%) | 322 (56.0%) | <0.001 |
| - Diabetes | 34 (4.8%) | 110 (19.1%) | <0.001 |
| - Constipation | 100 (14.1%) | 114 (19.8%) | 0.006 |
| - Obesity | 122 (17.2%) | 113 (19.7%) | 0.252 |
| Colonoscopy indication, n (%) | |||
| - Screening | 279 (39.1%) | 164 (28.5%) | |
| - Surveillance | 140 (19.6%) | 163 (28.3%) | <0.001 |
| - Diagnostic | 295 (41.3%) | 248 (43.2%) | |
| Previous inadequate cleansing | 27 (3.8%) | 40 (7.0%) | 0.012 |
| Outpatients | 692 (97.7%) | 542 (94.3%) | 0.001 |
| Low fiber diet ≥ 3 days | 605 (86.3%) | 845 (85.5%) | 0.696 |
| Split preparation regimen | 264 (37.3%) | 218 (38.0%) | 0.815 |
| Type of bowel solution | |||
| - 4L PEG | 259 (36.6%) | 229 (39.8%) | |
| - 2L PEG-PEG/ASC | 318 (44.9%) | 245 (42.6%) | 0.492 |
| - 1L PEG/ASC | 131 (18.5%) | 101 (17.6%) | |
| Adherence to bowel preparation | 653 (91.4%) | 526 (91.4%) | 0.951 |
| <65 Years (N = 714) | ≥65 Years (N = 575) | p | |
|---|---|---|---|
| Cecal intubation rate | 97.5% | 95.5% | 0.05 |
| BBPS total, mean (SD) | 6.6 ± 1.4 | 6.3 ± 1.6 | 0.007 |
| - Left colon, mean (SD) | 2.2 ± 0.5 | 2.2 ± 0.6 | 0.872 |
| - Transverse colon, mean (SD) | 2.1 ± 0.6 | 2.0 ± 0.6 | 0.166 |
| - Right colon, mean (SD) | 1.7 ± 0.6 | 1.7 ± 0.7 | 0.986 |
| Bowel cleansing success by preparation regimen | |||
| - Overall | 77.3% | 70.3% | 0.004 |
| - Day before regimen | 69.5% | 61.2% | 0.014 |
| - Afternoon/morning regimen | 90.2% | 84.9% | 0.078 |
| Bowel cleansing success by type of solution | |||
| - 4L PEG | 71.8% | 69.4% | 0.564 |
| - 2L PEG | 76.7% | 66.5% | 0.007 |
| - 1L PEG | 89.3% | 81.2% | 0.079 |
| HQC of the right colon by preparation regimen | |||
| - Overall | 18.5% | 17.7% | 0.724 |
| - Day before regimen | 10.8% | 8.7% | 0.317 |
| - Afternoon/morning regimen | 31.1% | 32.6% | 0.723 |
| HQC of the right colon by type of solution | |||
| - 4L PEG | 14.3% | 17.0% | 0.404 |
| - 2L PEG | 13.5% | 9.4% | 0.131 |
| - 1L PEG | 38.9% | 39.6% | 0.917 |
| Tolerability by type of solution | |||
| - 4L PEG | 7.2 ± 1.9 | 7.4 ± 1.9 | 0.466 |
| - 2L PEG | 7.0 ± 1.9 | 7.2 ± 1.9 | 0.224 |
| - 1L PEG | 7.8 ± 1.9 | 7.7 ± 1.9 | 0.595 |
| Predictors | Estimates | 95% CI | p |
|---|---|---|---|
| Cleansing success | |||
| Split regimen | 2.43 | 1.34–4.38 | 0.003 |
| Adequate cleansing at previous colonoscopy | 2.29 | 1.14–4.73 | 0.002 |
| Tolerability Score | 1.29 | 1.16–1.44 | <0.001 |
| Low fiber diet ≥ 3 days | 2.45 | 1.42–4.24 | 0.001 |
| Colonoscopy within 5 h after preparation | 2.67 | 1.28–5.56 | 0.008 |
| High-quality cleansing of the right colon | |||
| Solution type (ref = 2L PEG) | |||
| 1L PEG-ASC | 2.77 | 1.52–5.03 | 0.001 |
| 4L PEG | 3.78 | 2.03–7.03 | <0.001 |
| Split regimen | 4.58 | 2.43–8.64 | <0.001 |
| Adherence > 75% | 2.89 | 0.35–23.5 | 0.321 |
| Colonoscopy within 5 h after preparation | 0.99 | 0.55–1.79 | 0.986 |
| Tolerability Score | 1.20 | 1.05–1.38 | 0.005 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maida, M.; Facciorusso, A.; Sinagra, E.; Morreale, G.; Sferrazza, S.; Scalisi, G.; Pallio, S.; Camilleri, S. Predictive Factors of Adequate Bowel Cleansing for Colonoscopy in the Elderly: A Retrospective Analysis of a Prospective Cohort. Diagnostics 2022, 12, 2867. https://doi.org/10.3390/diagnostics12112867
Maida M, Facciorusso A, Sinagra E, Morreale G, Sferrazza S, Scalisi G, Pallio S, Camilleri S. Predictive Factors of Adequate Bowel Cleansing for Colonoscopy in the Elderly: A Retrospective Analysis of a Prospective Cohort. Diagnostics. 2022; 12(11):2867. https://doi.org/10.3390/diagnostics12112867
Chicago/Turabian StyleMaida, Marcello, Antonio Facciorusso, Emanuele Sinagra, Gaetano Morreale, Sandro Sferrazza, Giuseppe Scalisi, Socrate Pallio, and Salvatore Camilleri. 2022. "Predictive Factors of Adequate Bowel Cleansing for Colonoscopy in the Elderly: A Retrospective Analysis of a Prospective Cohort" Diagnostics 12, no. 11: 2867. https://doi.org/10.3390/diagnostics12112867
APA StyleMaida, M., Facciorusso, A., Sinagra, E., Morreale, G., Sferrazza, S., Scalisi, G., Pallio, S., & Camilleri, S. (2022). Predictive Factors of Adequate Bowel Cleansing for Colonoscopy in the Elderly: A Retrospective Analysis of a Prospective Cohort. Diagnostics, 12(11), 2867. https://doi.org/10.3390/diagnostics12112867