
Myelin-Weighted Imaging Presents Reduced Apparent Myelin Water in Patients with Alzheimer’s Disease

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. MRI Acquisition
2.3. Post-Processing for Mapping MWF
2.4. Statistical Analysis
2.4.1. Demographic Data and Clinical Outcome Scores
2.4.2. Voxel-Based Analysis of Apparent MWF Maps
2.4.3. Region-of-Interest (ROI)-Based Analysis of Apparent MWF Values
3. Results
3.1. Participant Characteristics
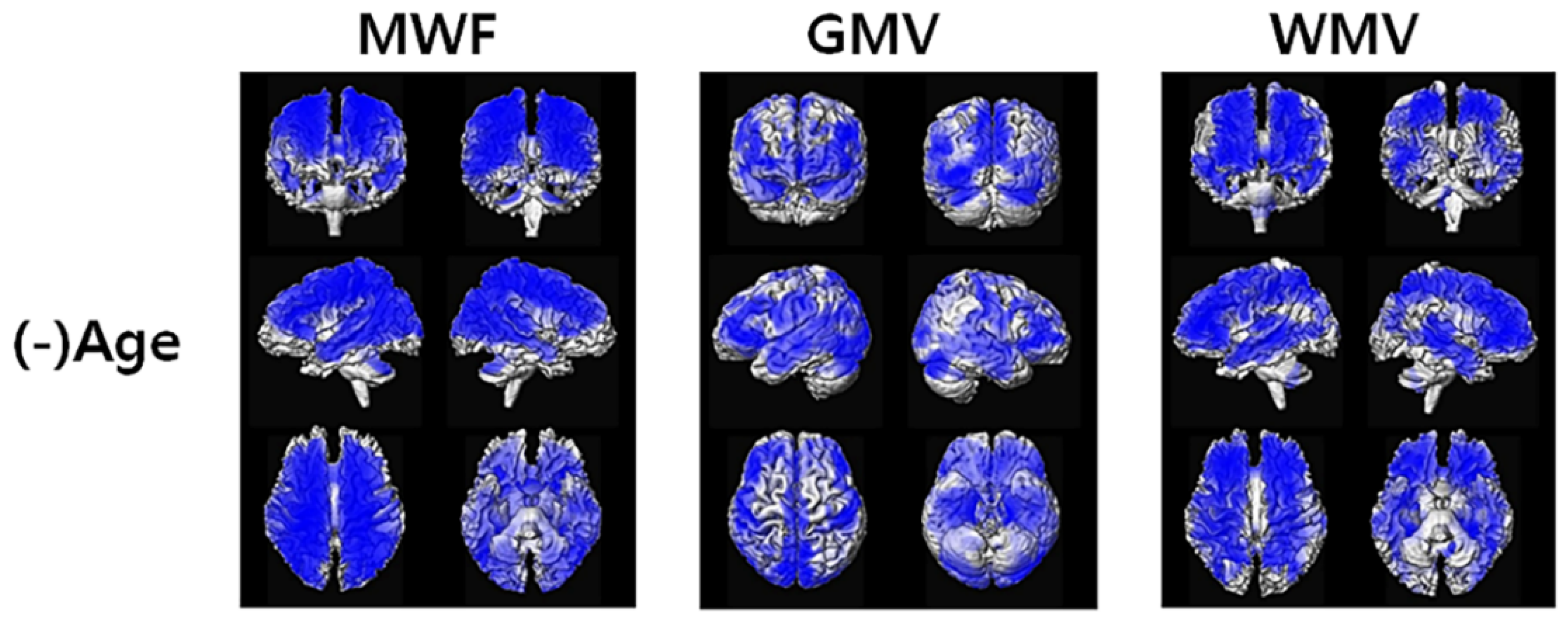
3.2. Voxel-Based Analysis of Apparent MWF Maps
3.3. ROI-Based Analysis of the Apparent MWF Maps
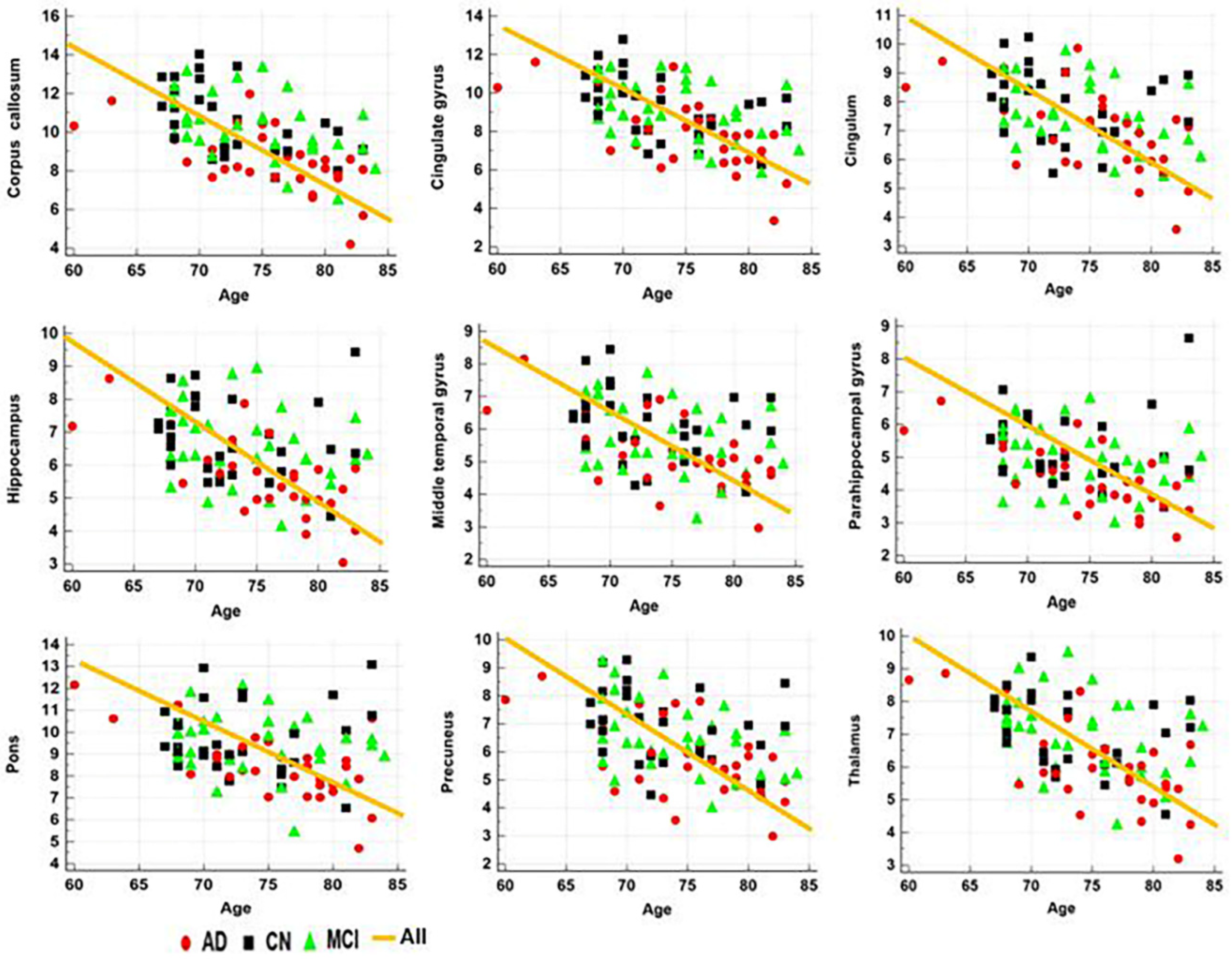
3.3.1. Correlation with Age and MMSE Scores
3.3.2. ROC Curve Analyses
4. Discussion
4.1. Apparent MWF Signals in AD
4.2. Apparent MWF Signals Correlate with MMSE Scores and/or Age
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Susuki, K. Myelin: A Specialized Membrane for Cell Communication. Nat. Educ. 2010, 3, 59. [Google Scholar]
- Hulshagen, L.; Krysko, O.; Bottelbergs, A.; Huyghe, S.; Klein, R.; Van Veldhoven, P.P.; De Deyn, P.P.; D’Hooge, R.; Hartmann, D.; Baes, M. Absence of functional peroxisomes from mouse CNS causes dysmyelination and axon degeneration. J. Neurosci. 2008, 28, 4015–4027. [Google Scholar] [CrossRef] [PubMed]
- Farooqui, A.A.; Horrocks, L.A.; Farooqui, T. Modulation of inflammation in brain: A matter of fat. J. Neurochem. 2007, 101, 577–599. [Google Scholar] [CrossRef]
- Bartzokis, G.; Sultzer, D.; Lu, P.H.; Nuechterlein, K.H.; Mintz, J.; Cummings, J.L. Heterogeneous age-related breakdown of white matter structural integrity: Implications for cortical “disconnection” in aging and Alzheimer’s disease. Neurobiol. Aging 2004, 25, 843–851. [Google Scholar] [CrossRef] [PubMed]
- Bartzokis, G.; Lu, P.H.; Mintz, J. Quantifying age-related myelin breakdown with MRI: Novel therapeutic targets for preventing cognitive decline and Alzheimer’s disease. J. Alzheimers Dis. 2004, 6, S53–S59. [Google Scholar] [CrossRef]
- Han, X.; Holtzman, D.M.; McKeel, D.W., Jr.; Kelley, J.; Morris, J.C. Substantial sulfatide deficiency and ceramide elevation in very early Alzheimer’s disease: Potential role in disease pathogenesis. J. Neurochem. 2002, 82, 809–818. [Google Scholar] [CrossRef]
- Roher, A.E.; Weiss, N.; Kokjohn, T.A.; Kuo, Y.M.; Kalback, W.; Anthony, J.; Watson, D.; Luehrs, D.C.; Sue, L.; Walker, D.; et al. Increased A beta peptides and reduced cholesterol and myelin proteins characterize white matter degeneration in Alzheimer’s disease. Biochemistry 2002, 41, 11080–11090. [Google Scholar] [CrossRef]
- Burns, J.M.; Church, J.A.; Johnson, D.K.; Xiong, C.; Marcus, D.; Fotenos, A.F.; Snyder, A.Z.; Morris, J.C.; Buckner, R.L. White matter lesions are prevalent but differentially related with cognition in aging and early Alzheimer disease. Arch. Neurol. 2005, 62, 1870–1876. [Google Scholar] [CrossRef]
- Svennerholm, L.; Gottfries, C.G. Membrane lipids, selectively diminished in Alzheimer brains, suggest synapse loss as a primary event in early-onset form (type I) and demyelination in late-onset form (type II). J. Neurochem. 1994, 62, 1039–1047. [Google Scholar] [CrossRef]
- Mitew, S.; Kirkcaldie, M.T.; Halliday, G.M.; Shepherd, C.E.; Vickers, J.C.; Dickson, T.C. Focal demyelination in Alzheimer’s disease and transgenic mouse models. Acta Neuropathol. 2010, 119, 567–577. [Google Scholar] [CrossRef]
- Stricker, N.H.; Schweinsburg, B.C.; Delano-Wood, L.; Wierenga, C.E.; Bangen, K.J.; Haaland, K.Y.; Frank, L.R.; Salmon, D.P.; Bondi, M.W. Decreased white matter integrity in late-myelinating fiber pathways in Alzheimer’s disease supports retrogenesis. Neuroimage 2009, 45, 10–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alonso-Ortiz, E.; Levesque, I.R.; Pike, G.B. MRI-based myelin water imaging: A technical review. Magn. Reson. Med. 2015, 73, 70–81. [Google Scholar] [CrossRef] [PubMed]
- Du, Y.P.; Chu, R.; Hwang, D.; Brown, M.S.; Kleinschmidt-DeMasters, B.K.; Singel, D.; Simon, J.H. Fast multislice mapping of the myelin water fraction using multicompartment analysis of T2* decay at 3T: A preliminary postmortem study. Magn. Reson. Med. 2007, 58, 865–870. [Google Scholar] [CrossRef]
- Hwang, D.; Kim, D.H.; Du, Y.P. In vivo multi-slice mapping of myelin water content using T2* decay. Neuroimage 2010, 52, 198–204. [Google Scholar] [CrossRef]
- Lenz, C.; Klarhofer, M.; Scheffler, K. Feasibility of in vivo myelin water imaging using 3D multigradient-echo pulse sequences. Magn. Reson. Med. 2012, 68, 523–528. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.D.; Wisnieff, C.; Cooper, M.A.; Kumar, D.; Raj, A.; Spincemaille, P.; Wang, Y.; Vartanian, T.; Gauthier, S.A. T2 prep three-dimensional spiral imaging with efficient whole brain coverage for myelin water quantification at 1.5 tesla. Magn. Reson. Med. 2012, 67, 614–621. [Google Scholar] [CrossRef]
- Prasloski, T.; Rauscher, A.; MacKay, A.L.; Hodgson, M.; Vavasour, I.M.; Laule, C.; Madler, B. Rapid whole cerebrum myelin water imaging using a 3D GRASE sequence. Neuroimage 2012, 63, 533–539. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Lee, H.M.; Oh, S.H.; Lee, J. Probing signal phase in direct visualization of short transverse relaxation time component (ViSTa). Magn. Reson. Med. 2015, 74, 499–505. [Google Scholar] [CrossRef] [Green Version]
- Oh, S.H.; Bilello, M.; Schindler, M.; Markowitz, C.E.; Detre, J.A.; Lee, J. Direct visualization of short transverse relaxation time component (ViSTa). Neuroimage 2013, 83, 485–492. [Google Scholar] [CrossRef] [Green Version]
- Wu, Z.; Bilgic, B.; He, H.; Tong, Q.; Sun, Y.; Du, Y.; Setsompop, K.; Zhong, J. Wave-CAIPI ViSTa: Highly accelerated whole-brain direct myelin water imaging with zero-padding reconstruction. Magn. Reson. Med. 2018, 80, 1061–1073. [Google Scholar] [CrossRef]
- Ahn, H.J.; Chin, J.; Park, A.; Lee, B.H.; Suh, M.K.; Seo, S.W.; Na, D.L. Seoul Neuropsychological Screening Battery-dementia version (SNSB-D): A useful tool for assessing and monitoring cognitive impairments in dementia patients. J. Korean Med. Sci. 2010, 25, 1071–1076. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petersen, R.C.; Doody, R.; Kurz, A.; Mohs, R.C.; Morris, J.C.; Rabins, P.V.; Ritchie, K.; Rossor, M.; Thal, L.; Winblad, B. Current concepts in mild cognitive impairment. Arch. Neurol. 2001, 58, 1985–1992. [Google Scholar] [CrossRef] [PubMed]
- Zhu, H.; Jones, C.K.; van Zijl, P.C.; Barker, P.B.; Zhou, J. Fast 3D chemical exchange saturation transfer (CEST) imaging of the human brain. Magn. Reson. Med. 2010, 64, 638–644. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guo, X.Y.; Chang, Y.; Kim, Y.; Rhee, H.Y.; Cho, A.R.; Park, S.; Ryu, C.W.; San Lee, J.; Lee, K.M.; Shin, W.; et al. Development and evaluation of a T1 standard brain template for Alzheimer disease. Quant. Imaging Med. Surg. 2021, 11, 2224–2244. [Google Scholar] [CrossRef]
- Bouhrara, M.; Reiter, D.A.; Bergeron, C.M.; Zukley, L.M.; Ferrucci, L.; Resnick, S.M.; Spencer, R.G. Evidence of demyelination in mild cognitive impairment and dementia using a direct and specific magnetic resonance imaging measure of myelin content. Alzheimers Dement. 2018, 14, 998–1004. [Google Scholar] [CrossRef]
- Dean, D.C., 3rd; Hurley, S.A.; Kecskemeti, S.R.; O’Grady, J.P.; Canda, C.; Davenport-Sis, N.J.; Carlsson, C.M.; Zetterberg, H.; Blennow, K.; Asthana, S.; et al. Association of Amyloid Pathology with Myelin Alteration in Preclinical Alzheimer Disease. JAMA Neurol. 2017, 74, 41–49. [Google Scholar] [CrossRef]
- Kavroulakis, E.; Simos, P.G.; Kalaitzakis, G.; Maris, T.G.; Karageorgou, D.; Zaganas, I.; Panagiotakis, S.; Basta, M.; Vgontzas, A.; Papadaki, E. Myelin content changes in probable Alzheimer’s disease and mild cognitive impairment: Associations with age and severity of neuropsychiatric impairment. J. Magn. Reson. Imaging 2018, 47, 1359–1372. [Google Scholar] [CrossRef]
- Ota, M.; Sato, N.; Kimura, Y.; Shigemoto, Y.; Kunugi, H.; Matsuda, H. Changes of Myelin Organization in Patients with Alzheimer’s Disease Shown by q-Space Myelin Map Imaging. Dement. Geriatr. Cogn. Disord. Extra 2019, 9, 24–33. [Google Scholar] [CrossRef]
- Bartzokis, G.; Cummings, J.L.; Sultzer, D.; Henderson, V.W.; Nuechterlein, K.H.; Mintz, J. White matter structural integrity in healthy aging adults and patients with Alzheimer disease: A magnetic resonance imaging study. Arch. Neurol. 2003, 60, 393–398. [Google Scholar] [CrossRef] [Green Version]
- Chalmers, K.; Wilcock, G.; Love, S. Contributors to white matter damage in the frontal lobe in Alzheimer’s disease. Neuropathol. Appl. Neurobiol. 2005, 31, 623–631. [Google Scholar] [CrossRef]
- Chia, L.S.; Thompson, J.E.; Moscarello, M.A. X-ray diffraction evidence for myelin disorder in brain from humans with Alzheimer’s disease. Biochim. Biophys. Acta 1984, 775, 308–312. [Google Scholar] [CrossRef]
- Englund, E.; Brun, A. White matter changes in dementia of Alzheimer’s type: The difference in vulnerability between cell compartments. Histopathology 1990, 16, 433–439. [Google Scholar] [CrossRef] [PubMed]
- Leow, A.D.; Yanovsky, I.; Parikshak, N.; Hua, X.; Lee, S.; Toga, A.W.; Jack, C.R., Jr.; Bernstein, M.A.; Britson, P.J.; Gunter, J.L.; et al. Alzheimer’s disease neuroimaging initiative: A one-year follow up study using tensor-based morphometry correlating degenerative rates, biomarkers and cognition. Neuroimage 2009, 45, 645–655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carmeli, C.; Donati, A.; Antille, V.; Viceic, D.; Ghika, J.; von Gunten, A.; Clarke, S.; Meuli, R.; Frackowiak, R.S.; Knyazeva, M.G. Demyelination in mild cognitive impairment suggests progression path to Alzheimer’s disease. PLoS ONE 2013, 8, e72759. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bartzokis, G.; Lu, P.H.; Tingus, K.; Mendez, M.F.; Richard, A.; Peters, D.G.; Oluwadara, B.; Barrall, K.A.; Finn, J.P.; Villablanca, P.; et al. Lifespan trajectory of myelin integrity and maximum motor speed. Neurobiol. Aging 2010, 31, 1554–1562. [Google Scholar] [CrossRef] [Green Version]
- Bartzokis, G.; Beckson, M.; Lu, P.H.; Nuechterlein, K.H.; Edwards, N.; Mintz, J. Age-related changes in frontal and temporal lobe volumes in men: A magnetic resonance imaging study. Arch. Gen. Psychiatry 2001, 58, 461–465. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | CN(1) | MCI(2) | AD(3) | Statistical Tests (Post Hoc) |
|---|---|---|---|---|
| No. of participants | 29 | 32 | 31 | 92 (total) |
| Demographic data and neuropsychologic test | ||||
| Age (year) * | 73.00 ± 5.01 | 74.31 ± 5.02 | 75.42 ± 5.71 | F = 1.586/p = 0.210 |
| Sex # (male/female) | 13/16 (M:44.8% F:55.2%) | 11/21 (M:34.4% F:65.6%) | 5/26 (M:16.13% F:83.87%) | χ2 < 3.673/p > 0.055 |
| MMSE * (/30) | 27.93 ± 2.02 | 26.53 ± 1.90 | 19.39 ± 4.74 | F = 63.375/p < 0.001 (1, 3), (2, 3) |
| CDR(range) | 0 (0–0.5) | 0.5 (0.5) | 1 (0.5–2) | N/A |
| ROI | MRI Measures | CN(1) | MCI(2) | AD(3) | ANOVA, F/p-Value * (Post Hoc) |
|---|---|---|---|---|---|
| Corpus callosum | MWF | 10.60 ± 7.80 | 10.31 ± 1.65 | 8.59 ± 1.70 | F = 12.204/p < 0.001 (1, 3), (2, 3) |
| GMV | 0.12 ± 0.013 | 0.11 ± 0.01 | 0.11 ± 0.01 | F = 2.982/p = 0.056 | |
| WMV | 0.42 ± 0.06 | 0.39 ± 0.04 | 0.36 ± 0.05 | F = 9.711/p < 0.001 (1, 3), (2, 3) | |
| Cingulate gyrus | MWF | 9.34 ± 1.60 | 9.10 ± 1.55 | 7.88 ± 1.81 | F = 6.718/p = 0.002 (1, 3), (2, 3) |
| GMV | 0.26 ± 0.03 | 0.24 ± 0.02 | 0.23 ± 0.03 | F = 6.044/p = 0.003 (1,3) | |
| WMV | 0.36 ± 0.05 | 0.33 ± 0.04 | 0.31 ± 0.04 | F = 12.562/p < 0.001 (1, 3), (2, 3) | |
| Cingulum | MWF | 7.88 ± 1.29 | 7.66 ± 1.17 | 6.92 ± 1.42 | F = 4.673/p = 0.012 (1, 3) |
| GMV | 0.34 ± 0.04 | 0.32 ± 0.03 | 0.30 ± 0.04 | F = 9.970/p < 0.001 (1, 2), (1, 3) | |
| WMV | 0.26 ± 0.04 | 0.24 ± 0.03 | 0.22 ± 0.03 | F = 12.661/p < 0.001 (1, 2, 3) | |
| Hippocampus | MWF | 6.83 ± 1.18 | 6.56 ± 1.19 | 5.64 ± 1.19 | F = 8.269/p = 0.001 (1, 3), (2, 3) |
| GMV | 0.37 ± 0.05 | 0.33 ± 0.05 | 0.28 ± 0.04 | F = 20.880/p < 0.001 (1, 2, 3) | |
| WMV | 0.26 ± 0.03 | 0.25 ± 0.03 | 0.22 ± 0.03 | F = 16.568/p < 0.001 (1, 3), (2, 3) | |
| Middle temporal gyrus | MWF | 6.18 ± 1.05 | 5.78 ± 1.09 | 5.21 ± 1.05 | F = 6.250/p = 0.003 (1, 3) |
| GMV | 0.33 ± 0.04 | 0.32 ± 0.03 | 0.29 ± 0.04 | F = 13.417/p < 0.001 (1, 3), (2, 3) | |
| WMV | 0.20 ± 0.02 | 0.18 ± 0.02 | 0.16 ± 0.02 | F = 13.223/p < 0.001 (1, 3),(2, 3) | |
| Parahippocampal gyrus | MWF | 5.35 ± 1.08 | 4.97 ± 0.95 | 4.34 ± 0.97 | F = 7.914/p = 0.001 (1, 3), (2, 3) |
| GMV | 0.41 ± 0.05 | 0.38 ± 0.05 | 0.34 ± 0.05 | F = 18.772/p < 0.001 (1, 2, 3) | |
| WMV | 0.21 ± 0.02 | 0.19 ± 0.02 | 0.17 ± 0.03 | F = 16.048/p < 0.001 (1, 3), (2, 3) | |
| Pons | MWF | 9.74 ± 1.60 | 9.46 ± 1.36 | 8.47 ± 0.48 | F = 6.143/p = 0.003 (1, 3), (2, 3) |
| GMV | 0.04 ± 0.004 | 0.03 ± 0.004 | 0.03 ± 0.004 | F = 6.778/p = 0.002 (1, 3) | |
| WMV | 0.53 ± 0.06 | 0.52 ± 0.05 | 0.49 ± 0.06 | F = 4.878/p = 0.010 (1, 3) | |
| Precuneus | MWF | 6.99 ± 1.23 | 6.49 ± 1.32 | 5.68 ± 1.35 | F = 7.712/p = 0.001 (1, 3) |
| GMV | 0.33 ± 0.03 | 0.31 ± 0.03 | 0.29 ± 0.04 | F = 7.488/p = 0.001 (1, 3) | |
| WMV | 0.26 ± 0.03 | 0.23 ± 0.03 | 0.32 ± 0.03 | F = 13.292/p < 0.001 (1, 2), (1, 3) | |
| Thalamus | MWF | 7.11 ± 1.09 | 6.98 ± 1.21 | 6.07 ± 1.31 | F = 6.617/p = 0.002 (1, 3),(2, 3) |
| GMV | 0.37 ± 0.04 | 0.36 ± 0.04 | 0.33 ± 0.05 | F = 4.516/p = 0.014 (1, 3), (2, 3) | |
| WMV | 0.27 ± 0.04 | 0.25 ± 0.03 | 0.24 ± 0.04 | F = 4.017/p = 0.021 (1, 3) |
| ROI | Regressors | MWF | GMV | WMV | |||
|---|---|---|---|---|---|---|---|
| Corpus callosum | Age | −0.565 | <0.0001 | −0.178 | 0.0905 | −0.361 | 0.0004 |
| *adjMMSE | 0.349 | 0.0007 | 0.281 | 0.0069 | 0.338 | 0.0011 | |
| Cingulate gyrus | Age | −0.537 | <0.0001 | −0.400 | 0.0001 | −0.467 | <0.0001 |
| *adjMMSE | 0.235 | 0.0248 | 0.276 | 0.0081 | 0.365 | 0.0004 | |
| Cingulum | Age | −0.481 | <0.0001 | −0.474 | <0.0001 | −0.459 | <0.0001 |
| *adjMMSE | 0.151 | 0.1519 | 0.367 | 0.0004 | 0.353 | 0.0006 | |
| Hippocampus | Age | −0.429 | <0.0001 | −0.545 | <0.0001 | −0.468 | <0.0001 |
| *adjMMSE | 0.251 | 0.0165 | 0.539 | <0.0001 | 0.421 | <0.0001 | |
| Middle temporal gyrus | Age | −0.462 | <0.0001 | −0.429 | <0.0001 | −0.446 | <0.0001 |
| *adjMMSE | 0.186 | 0.0771 | 0.442 | <0.0001 | 0.322 | 0.0019 | |
| Parahippocampal gyrus | Age | −0.371 | 0.0003 | −0.546 | <0.0001 | −0.456 | <0.0001 |
| *adjMMSE | 0.248 | 0.0179 | 0.544 | <0.0001 | 0.423 | <0.0001 | |
| Pons | Age | −0.321 | 0.0018 | −0.355 | 0.0005 | −0.218 | 0.0366 |
| *adjMMSE | 0.252 | 0.0161 | 0.367 | 0.0003 | 0.305 | 0.0032 | |
| Precuneus | Age | −0.481 | <0.0001 | −0.517 | <0.0001 | −0.496 | <0.0001 |
| *adjMMSE | 0.263 | 0.0117 | 0.424 | <0.0001 | 0.406 | 0.0001 | |
| Thalamus | Age | −0.487 | <0.0001 | −0.417 | <0.0001 | −0.204 | 0.0509 |
| *adjMMSE | 0.234 | 0.0257 | 0.242 | 0.0209 | 0.262 | 0.0122 | |
| MRI Measures | CN vs. MCI | CN vs. AD | MCI vs. AD | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SE | SP | AUC | p | SE | SP | AUC | p | SE | SP | AUC | p | |
| Hippo GMV | 50.00 | 82.76 | 0.691 | 0.0058 | 86.21 | 80.65 | 0.883 | <0.0001 | 61.29 | 84.37 | 0.771 | <0.0001 |
| Hippo WMV | 71.87 | 65.52 | 0.659 | 0.0260 | 93.10 | 70.97 | 0.860 | <0.0001 | 77.42 | 68.75 | 0.740 | 0.0001 |
| CC MWF | 75.00 | 41.38 | 0.517 | 0.8222 | 86.21 | 67.74 | 0.799 | <0.0001 | 70.97 | 84.37 | 0.779 | <0.0001 |
| GMV + MWF | 50.00 | 82.76 | 0.691 | 0.0056 | 93.10 | 77.42 | 0.898 | <0.0001 | 70.97 | 87.50 | 0.803 | <0.0001 |
| GMV + WMV | 84.37 | 55.17 | 0.690 | 0.0063 | 89.66 | 77.42 | 0.888 | <0.0001 | 67.74 | 81.25 | 0.779 | <0.0001 |
| WMV + MWF | 71.87 | 62.07 | 0.650 | 0.0367 | 96.55 | 70.97 | 0.891 | <0.0001 | 70.97 | 81.25 | 0.794 | <0.0001 |
| GMV + WMV + MWF | 84.37 | 55.17 | 0.690 | 0.0063 | 96.55 | 77.42 | 0.905 | <0.0001 | 70.97 | 84.37 | 0.812 | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lim, S.-H.; Lee, J.; Jung, S.; Kim, B.; Rhee, H.Y.; Oh, S.-H.; Park, S.; Cho, A.R.; Ryu, C.-W.; Jahng, G.-H. Myelin-Weighted Imaging Presents Reduced Apparent Myelin Water in Patients with Alzheimer’s Disease. Diagnostics 2022, 12, 446. https://doi.org/10.3390/diagnostics12020446
Lim S-H, Lee J, Jung S, Kim B, Rhee HY, Oh S-H, Park S, Cho AR, Ryu C-W, Jahng G-H. Myelin-Weighted Imaging Presents Reduced Apparent Myelin Water in Patients with Alzheimer’s Disease. Diagnostics. 2022; 12(2):446. https://doi.org/10.3390/diagnostics12020446
Chicago/Turabian StyleLim, Seung-Hyun, Jiyoon Lee, Sumin Jung, Bokyung Kim, Hak Young Rhee, Se-Hong Oh, Soonchan Park, Ah Rang Cho, Chang-Woo Ryu, and Geon-Ho Jahng. 2022. "Myelin-Weighted Imaging Presents Reduced Apparent Myelin Water in Patients with Alzheimer’s Disease" Diagnostics 12, no. 2: 446. https://doi.org/10.3390/diagnostics12020446
APA StyleLim, S. -H., Lee, J., Jung, S., Kim, B., Rhee, H. Y., Oh, S. -H., Park, S., Cho, A. R., Ryu, C. -W., & Jahng, G. -H. (2022). Myelin-Weighted Imaging Presents Reduced Apparent Myelin Water in Patients with Alzheimer’s Disease. Diagnostics, 12(2), 446. https://doi.org/10.3390/diagnostics12020446