
Tissue Fraction Correction and Visual Analysis Increase Diagnostic Sensitivity in Predicting Malignancy of Ground-Glass Nodules on [18F]FDG PET/CT: A Bicenter Retrospective Study

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
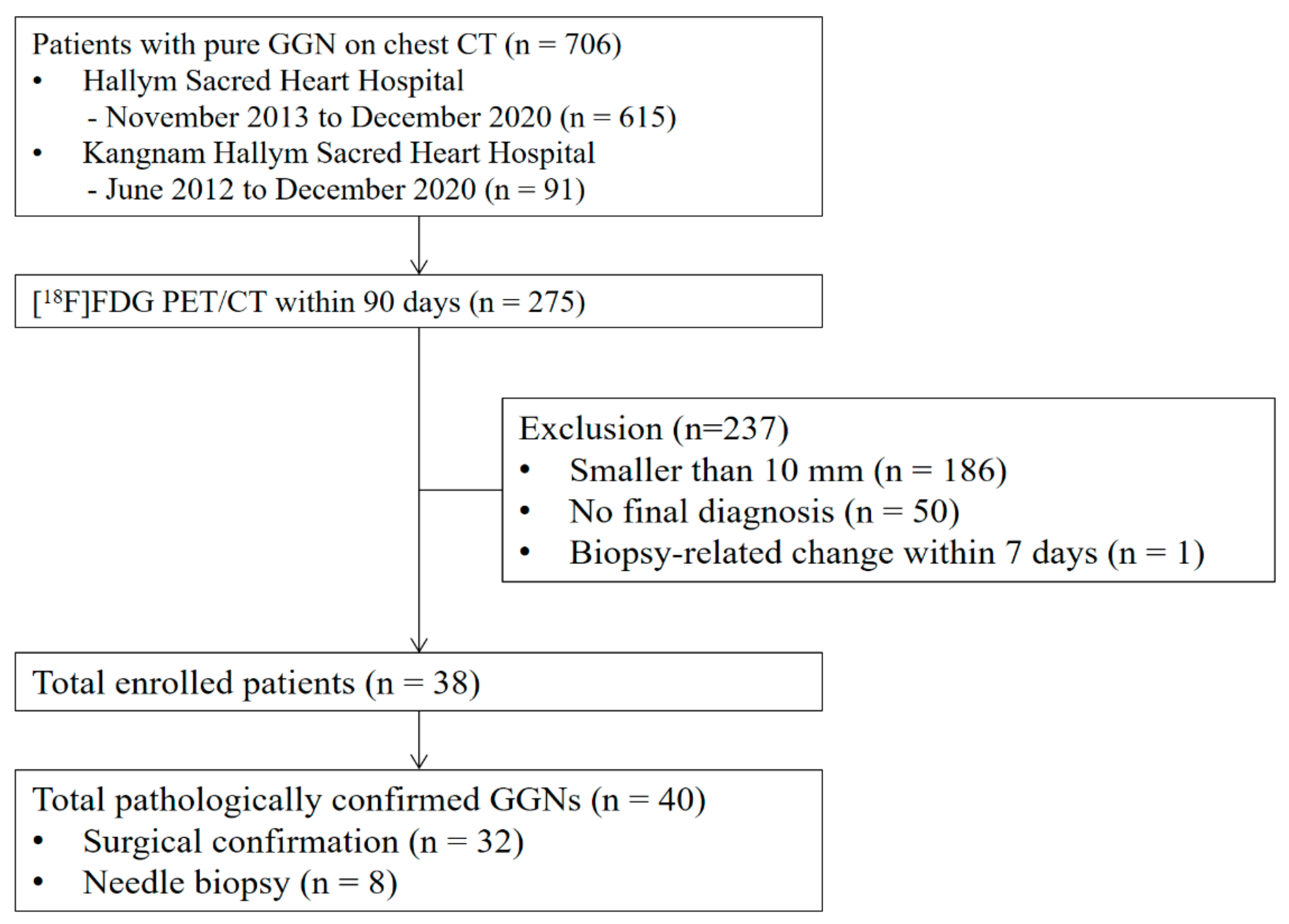
2.1. Subjects
2.2. PET/CT Imaging Protocol
2.3. PET/CT Image Analysis
- By adopting the method of Lambrou et al., the SUV of the solid portion within the GGN can be obtained by excluding the air fraction in which [18F]FDG is not distributed.
- This study was conducted on pure GGNs only, and we assumed that the density within a GGN was homogeneous.
- The tissue fraction of the GGN is k, and the air fraction is (1 − k).
- The HU of a GGN (HUGGN) can be expressed as follows:HUGGN = k HUTissue + (1 − k) HUAir
- Converting to the expression for k, we find the following:k = (HUGGN − HUAir)/(HUTissue − HUAir)
- We assumed that the HU of the lung tissue fraction of the GGN would be similar to that of other solid organs, such as the liver; therefore, we assigned a value of 50 to HUTissue. HUAir was −1000. The HUGGN of each GGN was measured on low-dose precontrast CT images of PET/CT because many patients only had enhanced chest CT images.
- If SUVmax is divided by k, the tissue-fraction–corrected SUVmax (SUVmaxTF) excluding the air fraction can be obtained.
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Chest CT and [18F]FDG PET/CT Characteristics
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Niu, R.; Shao, X.; Shao, X.; Wang, J.; Jiang, Z.; Wang, Y. Lung Adenocarcinoma Manifesting as Ground-Glass Opacity Nodules 3 Cm or Smaller: Evaluation with Combined High-Resolution CT and PET/CT Modality. Am. J. Roentgenol. 2019, 213, W236–W245. [Google Scholar] [CrossRef] [PubMed]
- Goo, J.M.; Park, C.M.; Lee, H.J. Ground-Glass Nodules on Chest CT as Imaging Biomarkers in the Management of Lung Ade-Nocarcinoma. Am. J. Roentgenol. 2011, 196, 533–543. [Google Scholar] [CrossRef] [PubMed]
- Zhuo, Y.; Shan, F.; Yang, S.; Zhan, Y.; Shi, Y.; Zhang, Z. Advances in Differential Diagnosis of Pulmonary Ground Glass Opacity on High Resolution Computed Tomography and Histopathology. Rad. Infect. Dis. 2020, 7, 7–11. [Google Scholar] [CrossRef]
- Park, C.M.; Goo, J.M.; Lee, H.J.; Lee, C.H.; Chun, E.J.; Im, J.G. Nodular Ground-Glass Opacity at Thin-Section CT: HIstologic Correlation and Evaluation of Change at Follow-Up. RadioGraphics 2007, 27, 391–408. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.J.; Goo, J.M.; Lee, C.H.; Yoo, C.G.; Kim, Y.T.; Im, J.G. Nodular Ground-Glass Opacities on Thin-Section CT: Size Change During Follow-Up and Pathological Results. Korean J. Radiol. 2007, 8, 22–31. [Google Scholar] [CrossRef] [Green Version]
- Nakata, M.; Saeki, H.; Takata, I.; Segawa, Y.; Mogami, H.; Mandai, K.; Eguchi, K. Focal Ground-Glass Opacity Detected by Low-Dose Helical CT. Chest 2002, 121, 1464–1467. [Google Scholar] [CrossRef]
- Christensen, J.A.; Nathan, M.A.; Mullan, B.P.; Hartman, T.E.; Swensen, S.J.; Lowe, V.J. Characterization of the Solitary Pulmonary Nodule: 18F-FDG PET Versus Nodule-Enhancement CT. Am. J. Roentgenol. 2006, 187, 1361–1367. [Google Scholar] [CrossRef] [Green Version]
- Gould, M.K.; Maclean, C.C.; Kuschner, W.G.; Rydzak, C.E.; Owens, D.K. Accuracy of Positron Emission Tomography for Diagnosis of Pulmonary Nodules and Mass Lesions: A Meta-Analysis. JAMA 2001, 285, 914–924. [Google Scholar] [CrossRef]
- Lowe, V.J.; Fletcher, J.W.; Gobar, L.; Lawson, M.; Kirchner, P.; Valk, P.; Karis, J.; Hubner, K.; Delbeke, D.; Heiberg, E.V.; et al. Prospective Investigation of Positron Emission Tomography in Lung Nodules. J. Clin. Oncol. 1998, 16, 1075–1084. [Google Scholar] [CrossRef]
- MacMahon, H.; Naidich, D.P.; Goo, J.M.; Lee, K.S.; Leung, A.N.C.; Mayo, J.R.; Mehta, A.C.; Ohno, Y.; Powell, C.A.; Prokop, M.; et al. Guidelines for Management of Incidental Pulmonary Nodules Detected on CT Images: From the Fleischner Society 2017. Radiology 2017, 284, 228–243. [Google Scholar] [CrossRef] [Green Version]
- Heyneman, L.E.; Patz, E.F. PET Imaging in Patients with Bronchioloalveolar Cell Carcinoma. Lung Cancer 2002, 38, 261–266. [Google Scholar] [CrossRef]
- Higashi, K.; Ueda, Y.; Seki, H.; Yuasa, K.; Oguchi, M.; Noguchi, T.; Taniguchi, M.; Tonami, H.; Okimura, T.; Yamamoto, I. Fluorine-18-FDG PET Imaging Is Negative in Bronchioloalveolar Lung Carcinoma. J. Nucl. Med. 1998, 39, 1016–1020. [Google Scholar]
- Hu, L.; Pan, Y.; Zhou, Z.; Gao, J. Application of Positron Emission Tomography-Computed Tomography in the Diagnosis of Pulmonary Ground-Glass Nodules. Exp. Ther. Med. 2017, 14, 5109–5113. [Google Scholar] [CrossRef]
- Nishii, K.; Bessho, A.; Fukamatsu, N.; Ogata, Y.; Hosokawa, S.; Sakugawa, M.; Kaji, M. Statistical Analysis of (18). Mol. Clin. Oncol. 2018, 9, 279–282. [Google Scholar] [CrossRef] [Green Version]
- Wu, H.B.; Wang, L.; Wang, Q.S.; Han, Y.J.; Li, H.S.; Zhou, W.L.; Tian, Y. Adenocarcinoma with BAC Features Presented as the Nonsolid Nodule Is Prone to Be False-Negative on 18F-FDG PET/CT. BioMed Res. Int. 2015, 2015, 243681. [Google Scholar] [CrossRef] [Green Version]
- Nomori, H.; Watanabe, K.; Ohtsuka, T.; Naruke, T.; Suemasu, K.; Uno, K. Evaluation of F-18 Fluorodeoxyglucose (FDG) PET Scanning for Pulmonary Nodules Less Than 3 Cm in Diameter, with Special Reference to the CT Images. Lung Cancer 2004, 45, 19–27. [Google Scholar] [CrossRef]
- Lambrou, T.; Groves, A.M.; Erlandsson, K.; Screaton, N.; Endozo, R.; Win, T.; Porter, J.C.; Hutton, B.F. The Importance of Correction for Tissue Fraction Effects in Lung PET: Preliminary Findings. Eur. J. Nucl. Med. Mol. Imaging 2011, 38, 2238–2246. [Google Scholar] [CrossRef]
- Coleman, R.E. PET in Lung Cancer. J. Nucl. Med. 1999, 40, 814–820. [Google Scholar]
- Bondue, B.; Castiaux, A.; Van Simaeys, G.; Mathey, C.; Sherer, F.; Egrise, D.; Lacroix, S.; Huaux, F.; Doumont, G.; Goldman, S. Absence of Early Metabolic Response Assessed by 18F-FDG PET/CT After Initiation of Antifibrotic Drugs in IPF Patients. Respir. Res. 2019, 20, 10. [Google Scholar] [CrossRef]
- Travis, W.D.; Brambilla, E.; Noguchi, M.; Nicholson, A.G.; Geisinger, K.R.; Yatabe, Y.; Beer, D.G.; Powell, C.A.; Riely, G.J.; Van Schil, P.E.; et al. International Association for the Study of Lung Cancer/American Thoracic Society/European Respiratory Society International Multidisciplinary Classification of Lung Adenocarcinoma. J. Thorac. Oncol. 2011, 6, 244–285. [Google Scholar] [CrossRef] [Green Version]
- Evangelista, L.; Panunzio, A.; Scagliori, E.; Sartori, P. Ground Glass Pulmonary Nodules: Their Significance in Oncology Patients and the Role of Computer Tomography and 18F-fluorodeoxyglucose Positron Emission Tomography. Eur. J. Hybrid Imaging 2018, 2, 2. [Google Scholar] [CrossRef] [Green Version]
- Vesselle, H.; Salskov, A.; Turcotte, E.; Wiens, L.; Schmidt, R.; Jordan, C.D.; Vallières, E.; Wood, D.E. Relationship Between Non-Small Cell Lung Cancer FDG Uptake at PET, Tumor Histology, and Ki-67 Proliferation Index. J. Thorac. Oncol. 2008, 3, 971–978. [Google Scholar] [CrossRef] [Green Version]
- Yoshizawa, A.; Motoi, N.; Riely, G.J.; Sima, C.S.; Gerald, W.L.; Kris, M.G.; Park, B.J.; Rusch, V.W.; Travis, W.D. Impact of Proposed IASLC/ATS/ERS Classification of Lung Adenocarcinoma: Prognostic Subgroups and Implications for Further Revision of Staging Based on Analysis of 514 Stage I Cases. Mod. Pathol. 2011, 24, 653–664. [Google Scholar] [CrossRef]
- Warth, A.; Muley, T.; Meister, M.; Stenzinger, A.; Thomas, M.; Schirmacher, P.; Schnabel, P.A.; Budczies, J.; Hoffmann, H.; Weichert, W. The Novel Histologic International Association for the Study of Lung Cancer/American Thoracic Society/European Respiratory Society Classification System of Lung Adenocarcinoma Is a Stage-Independent Predictor of Survival. J. Clin. Oncol. 2012, 30, 1438–1446. [Google Scholar] [CrossRef]
- Moon, Y.; Lee, K.Y.; Park, J.K. The Prognosis of Invasive Adenocarcinoma Presenting as Ground-Glass Opacity on Chest Computed Tomography After Sublobar Resection. J. Thorac. Dis. 2017, 9, 3782–3792. [Google Scholar] [CrossRef] [Green Version]
- Hasegawa, M.; Sone, S.; Takashima, S.; Li, F.; Yang, Z.G.; Maruyama, Y.; Watanabe, T. Growth Rate of Small Lung Cancers Detected on Mass CT Screening. Br. J. Radiol. 2000, 73, 1252–1259. [Google Scholar] [CrossRef]
- Goudarzi, B.; Jacene, H.A.; Wahl, R.L. Diagnosis and Differentiation of Bronchioloalveolar Carcinoma from Adenocarcinoma with Bronchioloalveolar Components with Metabolic and Anatomic Characteristics Using PET/CT. J. Nucl. Med. 2008, 49, 1585–1592. [Google Scholar] [CrossRef] [Green Version]
- McDermott, S.; Kilcoyne, A.; Wang, Y.; Scott, J.A.; Halpern, E.F.; Ackman, J.B. Comparison of the (18)F-FDG Avidity at PET of Benign and Malignant Pure Ground-Glass Opacities: A Paradox? Clin. Radiol. 2019, 74, 187–195. [Google Scholar] [CrossRef]
- Ikeda, K.; Awai, K.; Mori, T.; Kawanaka, K.; Yamashita, Y.; Nomori, H. Differential Diagnosis of Ground-Glass Opacity Nodules: CT Number Analysis by Three-Dimensional Computerized Quantification. Chest 2007, 132, 984–990. [Google Scholar] [CrossRef]
- Qi, L.; Xue, K.; Li, C.; He, W.; Mao, D.; Xiao, L.; Hua, Y.; Li, M. Analysis of CT Morphologic Features and Attenuation for Differentiating Among Transient Lesions, Atypical Adenomatous Hyperplasia, Adenocarcinoma In Situ, Minimally Invasive and Invasive Adenocarcinoma Presenting as Pure Ground-Glass Nodules. Sci. Rep. 2019, 9, 14586. [Google Scholar] [CrossRef] [Green Version]
- Kim, T.J.; Park, C.M.; Goo, J.M.; Lee, K.W. Is There a Role for FDG PET in the Management of Lung Cancer Manifesting Pre-Dominantly as Ground-Glass Opacity? Am. J. Roentgenol. 2012, 198, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Shao, X.; Niu, R.; Jiang, Z.; Shao, X.; Wang, Y. Role of PET/CT in Management of Early Lung Adenocarcinoma. Am. J. Roentgenol. 2020, 214, 437–445. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.H.; Ryu, S.Y.; Lee, H.Y.; Choi, J.Y.; Kwon, O.J.; Kim, H.K.; Shim, Y.M. Evaluating the Tumor Biology of Lung Adenocarcinoma: A Multimodal Analysis. Medicine 2019, 98, e16313. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | n = 38 |
|---|---|
| Age at diagnosis, year, median (Q1–Q3) | 64.0 (59.0–68.0) |
| Sex | |
| Male, n (%) | 13 (34%) |
| Female, n (%) | 25 (66%) |
| Smoking history | |
| Current smoker, n (%) | 3 (8%) |
| Former smoker, n (%) | 0 (0%) |
| Nonsmoker, n (%) | 35 (92%) |
| Reason for [18F]FDG PET/CT | |
| For ground-glass nodule evaluation, n (%) | 35 (92%) |
| For other malignancy evaluation, n (%) | 3 (8%) |
| Interval between CT and [18F]FDG PET/CT, days, median (Q1–Q3) | 17.5 (11.5–24.8) |
| Interval between [18F]FDG PET/CT and biopsy, days, median (Q1–Q3) | 5.0 (2.0–10.5) |
| Characteristics | Adenocarcinoma (n = 25) | Minimally Invasive Adenocarcinoma (n = 9) | Adenocarcinoma In Situ (n = 6) | Total (n = 40) | p |
|---|---|---|---|---|---|
| Size of nodule, mm | 19.0 (15.0–23.0) | 13.3 (10.0–20.0) | 14.7 (12.0–16.8) | 16.8 (12.0–23.0) | 0.125 |
| Hounsfield unit | −437 (−529–−377) | −411 (−631–−313) | −577 (−631–−435) | −437 (−598–−379) | 0.406 |
| Method for pathological confirmation | 0.227 | ||||
| Needle biopsy | 7 (28%) | 0 (0%) | 1 (17%) | 8 (20%) | |
| Surgery | 18 (72%) | 9 (100%) | 5 (83%) | 32 (80%) | |
| Visual analysis of [18F]FDG PET/CT | 0.001 * | ||||
| Positive | 22 (88%) | 4 (44%) | 1 (17%) | 27 (68%) | |
| Semi-quantitative analysis of [18F]FDG PET/CT | |||||
| SUVmax | 1.3 (1.1–1.8) | 1.1 (0.7–1.8) | 0.6 (0.5–0.9) | 1.3 (0.8–1.8) | 0.033 * |
| SUVmaxTF | 2.6 (2.2–3.1) | 2.2 (1.9–2.9) | 1.6 (1.5–1.7) | 2.4 (1.9–3.0) | 0.018 * |
| SUVmax ≥ 2.5 | 2 (8%) | 0 (0%) | 0 (0%) | 2 (5%) | 0.990 |
| SUVmaxTF ≥ 2.5 | 15 (60%) | 4 (44%) | 1 (17%) | 20 (50%) | 0.195 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Song, Y.H.; Moon, J.W.; Kim, Y.N.; Woo, J.Y.; Son, H.J.; Lee, S.H.; Hwang, H.S. Tissue Fraction Correction and Visual Analysis Increase Diagnostic Sensitivity in Predicting Malignancy of Ground-Glass Nodules on [18F]FDG PET/CT: A Bicenter Retrospective Study. Diagnostics 2022, 12, 1292. https://doi.org/10.3390/diagnostics12051292
Song YH, Moon JW, Kim YN, Woo JY, Son HJ, Lee SH, Hwang HS. Tissue Fraction Correction and Visual Analysis Increase Diagnostic Sensitivity in Predicting Malignancy of Ground-Glass Nodules on [18F]FDG PET/CT: A Bicenter Retrospective Study. Diagnostics. 2022; 12(5):1292. https://doi.org/10.3390/diagnostics12051292
Chicago/Turabian StyleSong, Yun Hye, Jung Won Moon, Yoo Na Kim, Ji Young Woo, Hye Joo Son, Suk Hyun Lee, and Hee Sung Hwang. 2022. "Tissue Fraction Correction and Visual Analysis Increase Diagnostic Sensitivity in Predicting Malignancy of Ground-Glass Nodules on [18F]FDG PET/CT: A Bicenter Retrospective Study" Diagnostics 12, no. 5: 1292. https://doi.org/10.3390/diagnostics12051292
APA StyleSong, Y. H., Moon, J. W., Kim, Y. N., Woo, J. Y., Son, H. J., Lee, S. H., & Hwang, H. S. (2022). Tissue Fraction Correction and Visual Analysis Increase Diagnostic Sensitivity in Predicting Malignancy of Ground-Glass Nodules on [18F]FDG PET/CT: A Bicenter Retrospective Study. Diagnostics, 12(5), 1292. https://doi.org/10.3390/diagnostics12051292