
Comparison Study of Myocardial Radiomics Feature Properties on Energy-Integrating and Photon-Counting Detector CT

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
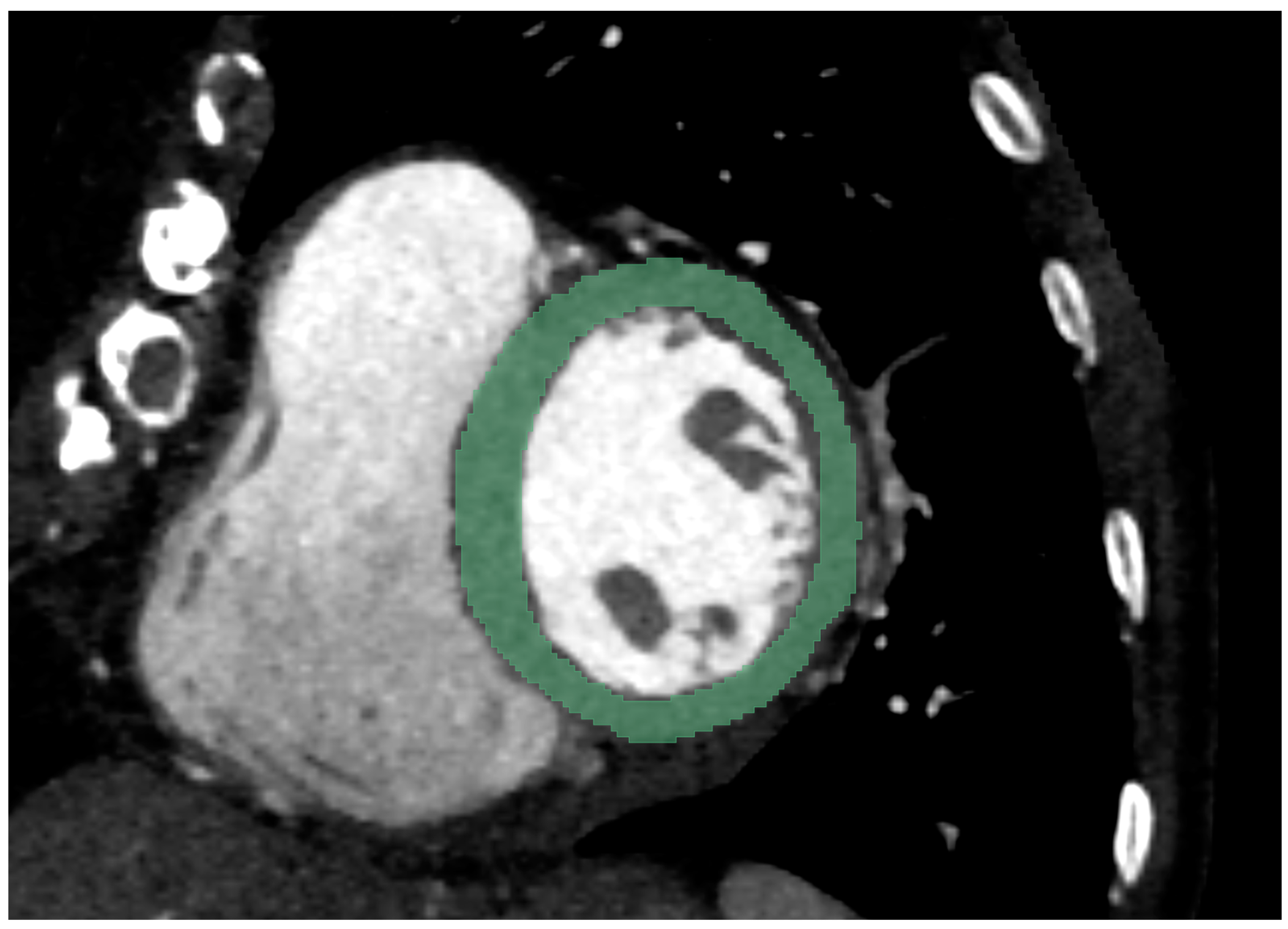
2.1. Chest CT Imaging
2.2. Chest CT Imaging Analysis
2.3. Radiomics Feature Extraction
2.4. Statistical Analysis
3. Results
3.1. Patient Collective
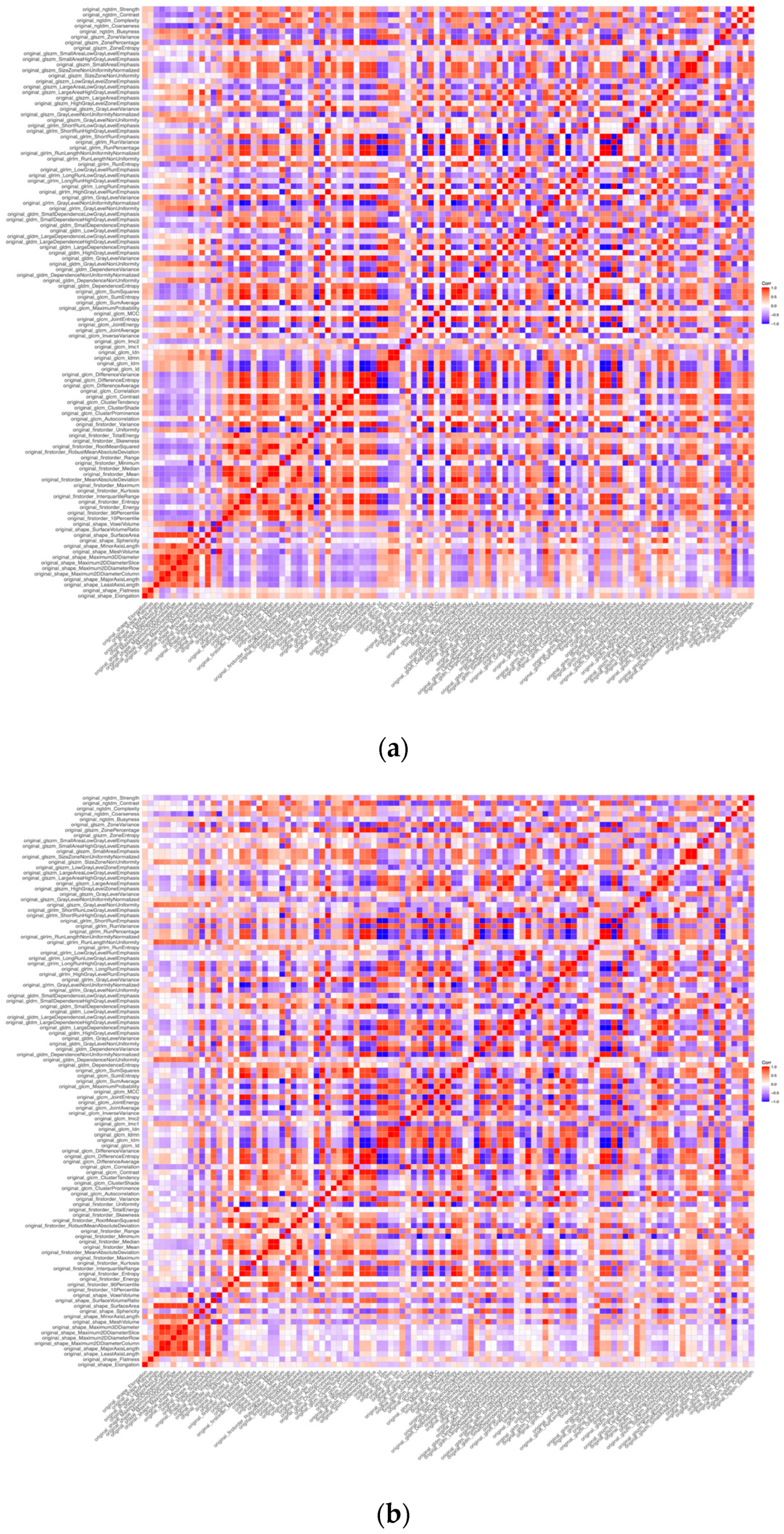
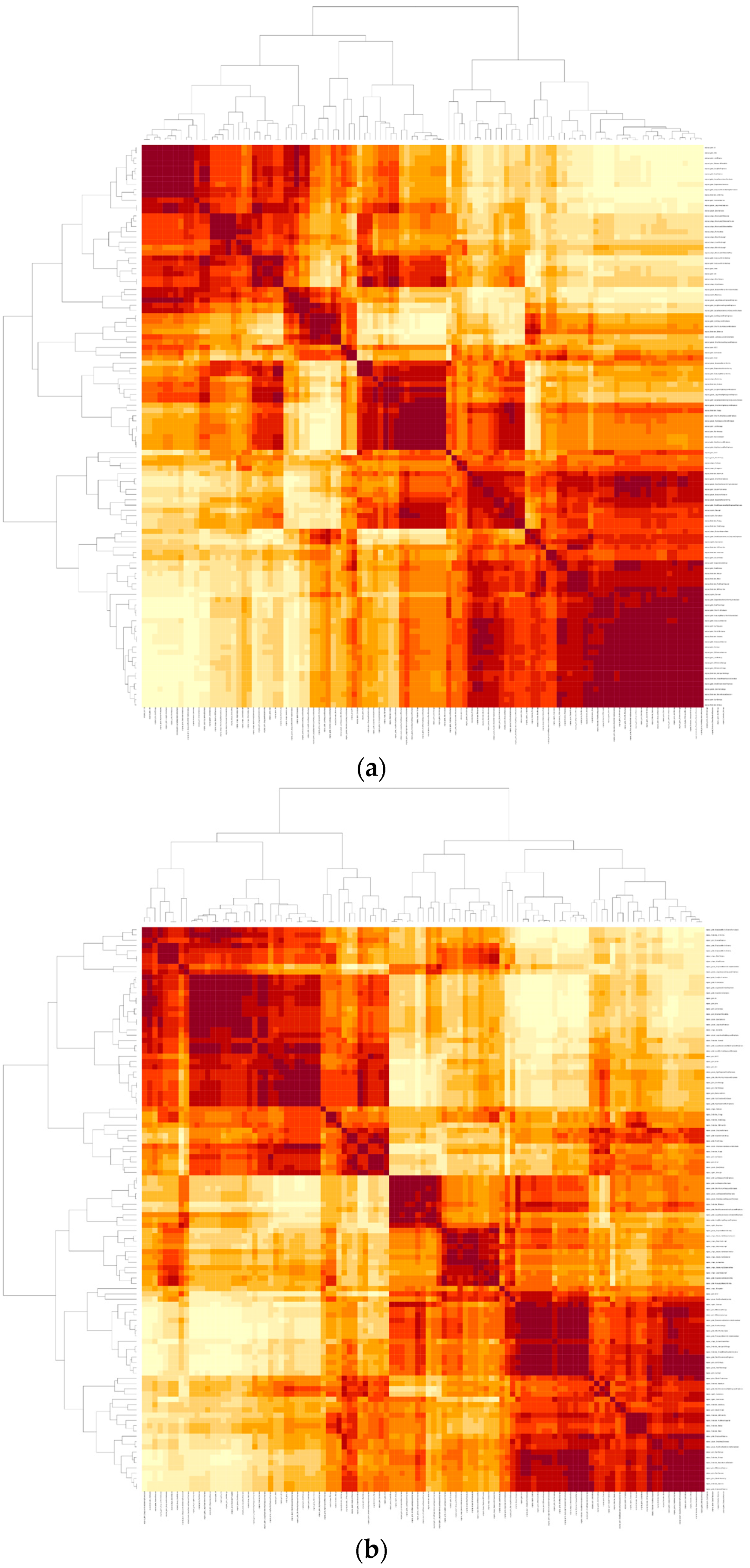
3.2. Cluster Analysis
3.3. Radiomics Feature Assessment
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gillies, R.J.; Kinahan, P.E.; Hricak, H. Radiomics: Images Are More than Pictures, They Are Data. Radiology 2016, 278, 563–577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, P.; Xue, Y.; Schoepf, U.J.; Varga-Szemes, A.; Griffith, J.; Yacoub, B.; Zhou, F.; Zhou, C.; Yang, Y.; Xing, W.; et al. Radiomics: The Next Frontier of Cardiac Computed Tomography. Circ. Cardiovasc. Imaging 2021, 14, e011747. [Google Scholar] [CrossRef] [PubMed]
- Castellano, G.; Bonilha, L.; Li, L.M.; Cendes, F. Texture analysis of medical images. Clin. Radiol. 2004, 59, 1061–1069. [Google Scholar] [CrossRef]
- van Griethuysen, J.J.M.; Fedorov, A.; Parmar, C.; Hosny, A.; Aucoin, N.; Narayan, V.; Beets-Tan, R.G.; Fillion-Robin, J.C.; Pieper, S.; Aerts, H.J. Computational Radiomics System to Decode the Radiographic Phenotype. Cancer Res. 2017, 77, e104–e107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Z.; Wang, S.; Dong, D.; Fang, C.; Zhou, X.; Sun, K.; Li, L.; Li, B.; Wang, M.; Tian, J. The Applications of Radiomics in Precision Diagnosis and Treatment of Oncology: Opportunities and Challenges. Theranostics 2019, 9, 1303–1322. [Google Scholar] [CrossRef] [PubMed]
- Enke, J.S.; Moltz, J.H.; D’Anastasi, M.; Kunz, W.G.; Schmidt, C.; Maurus, S.; Mühlberg, A.; Katzmann, A.; Sühling, M.; Hahn, H.; et al. Radiomics Features of the Spleen as Surrogates for CT-Based Lymphoma Diagnosis and Subtype Differentiation. Cancers 2022, 14, 713. [Google Scholar] [CrossRef]
- Woźnicki, P.; Westhoff, N.; Huber, T.; Riffel, P.; Froelich, M.F.; Gresser, E.; von Hardenberg, J.; Mühlberg, A.; Michel, M.S.; Schoenberg, S.O.; et al. Multiparametric MRI for Prostate Cancer Characterization: Combined Use of Radiomics Model with PI-RADS and Clinical Parameters. Cancers 2020, 12, 1767. [Google Scholar] [CrossRef] [PubMed]
- Mühlberg, A.; Holch, J.W.; Heinemann, V.; Huber, T.; Moltz, J.; Maurus, S.; Jäger, N.; Liu, L.; Froelich, M.F.; Katzmann, A.; et al. The relevance of CT-based geometric and radiomics analysis of whole liver tumor burden to predict survival of patients with metastatic colorectal cancer. Eur. Radiol. 2021, 31, 834–846. [Google Scholar] [CrossRef]
- Jiang, Y.; Chen, C.; Xie, J.; Wang, W.; Zha, X.; Lv, W.; Chen, H.; Hu, Y.; Li, T.; Yu, J.; et al. Radiomics signature of computed tomography imaging for prediction of survival and chemotherapeutic benefits in gastric cancer. EBioMedicine 2018, 36, 171–182. [Google Scholar] [CrossRef] [Green Version]
- Hassani, C.; Saremi, F.; Varghese, B.A.; Duddalwar, V. Myocardial Radiomics in Cardiac MRI. Am. J. Roentgenol. 2020, 214, 536–545. [Google Scholar] [CrossRef]
- Mannil, M.; Eberhard, M.; von Spiczak, J.; Heindel, W.; Alkadhi, H.; Baessler, B. Artificial Intelligence and Texture Analysis in Cardiac Imaging. Curr. Cardiol. Rep. 2020, 22, 131. [Google Scholar] [CrossRef] [PubMed]
- Leiner, T.; Rueckert, D.; Suinesiaputra, A.; Baeßler, B.; Nezafat, R.; Išgum, I.; Young, A.A. Machine learning in cardiovascular magnetic resonance: Basic concepts and applications. J. Cardiovasc. Magn. Reson. 2019, 21, 61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mannil, M.; von Spiczak, J.; Manka, R.; Alkadhi, H. Texture Analysis and Machine Learning for Detecting Myocardial Infarction in Noncontrast Low-Dose Computed Tomography: Unveiling the Invisible. Investig. Radiol. 2018, 53, 338–343. [Google Scholar] [CrossRef] [PubMed]
- Hinzpeter, R.; Wagner, M.W.; Wurnig, M.C.; Seifert, B.; Manka, R.; Alkadhi, H. Texture analysis of acute myocardial infarction with CT: First experience study. PLoS ONE 2017, 12, e0186876. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Global Status Report on Noncommunicable Diseases 2014; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Knuuti, J.; Wijns, W.; Saraste, A.; Capodanno, D.; Barbato, E.; Funck-Brentano, C.; Prescott, E.; Storey, R.F.; Deaton, C.; Cuisset, T.; et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur. Heart J. 2020, 41, 407–477. [Google Scholar] [CrossRef]
- Maurovich-Horvat, P.; Bosserdt, M.; Kofoed, K.F.; Rieckmann, N.; Benedek, T.; Donnelly, P.; Rodriguez-Palomares, J.; Erglis, A.; Štěchovský, C.; The DISCHARGE Trial Group. CT or Invasive Coronary Angiography in Stable Chest Pain. N. Engl. J. Med. NEJM 2022, 22, 963. [Google Scholar] [CrossRef]
- Schoepf, U.J.; Emrich, T. A Brave New World: Toward Precision Phenotyping and Understanding of Coronary Artery Disease Using Radiomics Plaque Analysis. Radiology 2021, 299, 107–108. [Google Scholar] [CrossRef]
- Wen, D.; Xu, Z.; An, R.; Ren, J.; Jia, Y.; Li, J.; Zheng, M. Predicting haemodynamic significance of coronary stenosis with radiomics-based pericoronary adipose tissue characteristics. Clin. Radiol. 2022, 77, e154–e161. [Google Scholar] [CrossRef]
- Wang, Y.; Osborne, M.T.; Tung, B.; Li, M.; Li, Y. Imaging Cardiovascular Calcification. JAHA 2018, 7, e008564. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.; Park, C.M.; Park, S.J.; Song, Y.S.; Lee, J.H.; Hwang, E.J.; Goo, J.M. Temporal Changes of Texture Features Extracted From Pulmonary Nodules on Dynamic Contrast-Enhanced Chest Computed Tomography: How Influential Is the Scan Delay? Investig. Radiol. 2016, 51, 569–574. [Google Scholar] [CrossRef]
- Mayerhoefer, M.E.; Szomolanyi, P.; Jirak, D.; Berg, A.; Materka, A.; Dirisamer, A.; Trattnig, S. Effects of Magnetic Resonance Image Interpolation on the Results of Texture-Based Pattern Classification: A Phantom Study. Investig. Radiol. 2009, 44, 405–411. [Google Scholar] [CrossRef] [PubMed]
- Mayerhoefer, M.E.; Szomolanyi, P.; Jirak, D.; Materka, A.; Trattnig, S. Effects of MRI acquisition parameter variations and protocol heterogeneity on the results of texture analysis and pattern discrimination: An application-oriented study: Effects of MRI acquisition parameters on texture analysis. Med. Phys. 2009, 36, 1236–1243. [Google Scholar] [CrossRef] [PubMed]
- Jirák, D.; Dezortová, M.; Hájek, M. Phantoms for texture analysis of MR images. Long-term and multi-center study. Med. Phys. 2004, 31, 616–622. [Google Scholar] [CrossRef] [PubMed]
- Waugh, S.A.; Lerski, R.A.; Bidaut, L.; Thompson, A.M. The influence of field strength and different clinical breast MRI protocols on the outcome of texture analysis using foam phantoms: Influence of different MRI protocols on texture analysis. Med. Phys. 2011, 38, 5058–5066. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Willemink, M.J.; Persson, M.; Pourmorteza, A.; Pelc, N.J.; Fleischmann, D. Photon-counting CT: Technical Principles and Clinical Prospects. Radiology 2018, 289, 293–312. [Google Scholar] [CrossRef]
- Rajendran, K.; Petersilka, M.; Henning, A.; Shanblatt, E.R.; Schmidt, B.; Flohr, T.G.; Ferrero, A.; Baffour, F.; Diehn, F.E.; Yu, L.; et al. First Clinical Photon-counting Detector CT System: Technical Evaluation. Radiology 2022, 21, 2579. [Google Scholar] [CrossRef]
- Fedorov, A.; Beichel, R.; Kalpathy-Cramer, J.; Finet, J.; Fillion-Robin, J.C.; Pujol, S.; Bauer, C.; Jennings, D.; Fennessy, F.; Sonka, M.; et al. 3D Slicer as an image computing platform for the Quantitative Imaging Network. Magn. Reson. Imaging 2012, 30, 1323–1341. [Google Scholar] [CrossRef] [Green Version]
- R: The R Project for Statistical Computing. Available online: https://www.r-project.org/ (accessed on 17 March 2022).
- Zhao, B.; Tan, Y.; Tsai, W.Y.; Schwartz, L.H.; Lu, L. Exploring Variability in CT Characterization of Tumors: A Preliminary Phantom Study. Transl. Oncol. 2014, 7, 88–93. [Google Scholar] [CrossRef] [Green Version]
- Mackin, D.; Fave, X.; Zhang, L.; Fried, D.; Yang, J.; Taylor, B.; Rodriguez-Rivera, E.; Dodge, C.; Jones, A.K.; Court, L. Measuring Computed Tomography Scanner Variability of Radiomics Features. Investig. Radiol. 2015, 50, 757–765. [Google Scholar] [CrossRef]
- Solomon, J.; Mileto, A.; Nelson, R.C.; Roy Choudhury, K.; Samei, E. Quantitative Features of Liver Lesions, Lung Nodules, and Renal Stones at Multi–Detector Row CT Examinations: Dependency on Radiation Dose and Reconstruction Algorithm. Radiology 2016, 279, 185–194. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| EICT | PCCT | p Value | |
|---|---|---|---|
| Patient parameters | |||
| n | 25 | 25 | |
| Age | 56.88 (10.79) | 56.08 (13.98) | 0.822 |
| Sex | 10 male (40.0%) | 18 male (72.0%) | 0.046 |
| Stent | 0 | 0 | N/A |
| Significant stenosis
(>50%) | 0 | 0 | N/A |
| Agatston Score | 55.38 (110.55) | 38.29 (87.76) | 0.548 |
| Mean HU Value | 114.52 (50.87) | 125.13 (42.04) | 0.123 |
| Scanner parameters | |||
| Tube voltage | 100 | 120 | N/A |
| Slice thickness | 5 mm | 5 mm | N/A |
| Kernel | Bv40 | Bv40 | N/A |
| Tube | Vectron ® | Vectron ® | N/A |
| Feature Mean (SD) | EICT | PCCT | t Test | F Test |
|---|---|---|---|---|
| n | 25 | 25 | ||
| First order features | ||||
| original_firstorder_Maximum | 517.90 (120.68) | 604.00 (119.59) | 0.015 | 0.965 |
| original_firstorder_Median | 124.93 (25.88) | 126.65 (17.04) | 0.782 | 0.046 |
| original_firstorder_Skewness | −0.28 (0.97) | 0.28 (0.86) | 0.035 | 0.557 |
| Feature Mean (SD) | EICT | PCCT | t Test | F Test |
|---|---|---|---|---|
| n | 25 | 25 | ||
| Gray Level Co-Occurrence Matrix (GLCM) | ||||
| original_glcm_Contrast | 2.76 (1.00) | 3.43 (1.30) | 0.049 | 0.206 |
| original_glcm_Correlation | 0.64 (0.03) | 0.57 (0.07) | <0.001 | <0.001 |
| original_glcm_Idmn | 1.00 (0.0006) | 1.00 (0.001) | 0.115 | <0.001 |
| original_glcm_Idn | 0.97 (0.00) | 0.97 (0.01) | 0.194 | <0.001 |
| original_glcm_Imc1 | −0.15 (0.02) | −0.13 (0.04) | 0.002 | 0.007 |
| original_glcm_Imc2 | 0.73 (0.04) | 0.66 (0.08) | 0.001 | <0.001 |
| original_glcm_InverseVariance | 0.46 (0.01) | 0.45 (0.02) | 0.016 | 0.062 |
| original_glcm_MCC | 0.71 (0.04) | 0.67 (0.07) | 0.025 | 0.011 |
| Gray Level Dependence Matrix (GLDM) | ||||
| original_gldm_DependenceNonUniformityNormalized | 0.07 (0.01) | 0.08 (0.01) | 0.074 | 0.042 |
| original_gldm_LowGrayLevelEmphasis | 0.00 (0.00) | 0.00 (0.00) | 0.074 | <0.001 |
| original_gldm_SmallDependenceLowGrayLevelEmphasis | 0.00 (0.00) | 0.00 (0.00) | 0.032 | <0.001 |
| Gray Level Run Length Matrix (GLRLM) | ||||
| original_glrlm_LongRunEmphasis | 2.87 (0.60) | 2.80 (0.93) | 0.772 | 0.04 |
| original_glrlm_LongRunLowGrayLevelEmphasis | 0.01 (0.00) | 0.01 (0.01) | 0.202 | 0.016 |
| original_glrlm_LowGrayLevelRunEmphasis | 0.00 (0.00) | 0.00 (0.00) | 0.076 | <0.001 |
| original_glrlm_RunVariance | 0.82 (0.28) | 0.79 (0.44) | 0.802 | 0.033 |
| original_glrlm_ShortRunLowGrayLevelEmphasis | 0.00 (0.00) | 0.00 (0.00) | 0.062 | <0.001 |
| Gray Level Size Zone Matrix (GLSZM) | ||||
| original_glszm_GrayLevelNonUniformity | 304.54 (69.82) | 397.07 (160.54) | 0.011 | <0.001 |
| original_glszm_LowGrayLevelZoneEmphasis | 0.00 (0.00) | 0.01 (0.00) | 0.111 | <0.001 |
| original_glszm_SizeZoneNonUniformity | 1215.38 (435.47) | 1622.80 (651.64) | 0.012 | 0.054 |
| original_glszm_SizeZoneNonUniformityNormalized | 0.27 (0.04) | 0.29 (0.03) | 0.023 | 0.662 |
| original_glszm_SmallAreaEmphasis | 0.53 (0.04) | 0.56 (0.03) | 0.028 | 0.488 |
| original_glszm_SmallAreaLowGrayLevelEmphasis | 0.00 (0.00) | 0.00 (0.00) | 0.068 | <0.001 |
| original_glszm_ZoneEntropy | 6.82 (0.11) | 6.66 (0.17) | <0.001 | 0.054 |
| Neighbouring Grey Tone Difference Matrix (NGTDM) | ||||
| original_ngtdm_Busyness | 6.54 (2.31) | 9.96 (7.85) | 0.042 | <0.001 |
| original_ngtdm_Coarseness | 0.00 (0.00) | 0.00 (0.00) | 0.011 | 0.178 |
| original_ngtdm_Contrast | 0.01 (0.00) | 0.01 (0.00) | 0.153 | 0.013 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ayx, I.; Tharmaseelan, H.; Hertel, A.; Nörenberg, D.; Overhoff, D.; Rotkopf, L.T.; Riffel, P.; Schoenberg, S.O.; Froelich, M.F. Comparison Study of Myocardial Radiomics Feature Properties on Energy-Integrating and Photon-Counting Detector CT. Diagnostics 2022, 12, 1294. https://doi.org/10.3390/diagnostics12051294
Ayx I, Tharmaseelan H, Hertel A, Nörenberg D, Overhoff D, Rotkopf LT, Riffel P, Schoenberg SO, Froelich MF. Comparison Study of Myocardial Radiomics Feature Properties on Energy-Integrating and Photon-Counting Detector CT. Diagnostics. 2022; 12(5):1294. https://doi.org/10.3390/diagnostics12051294
Chicago/Turabian StyleAyx, Isabelle, Hishan Tharmaseelan, Alexander Hertel, Dominik Nörenberg, Daniel Overhoff, Lukas T. Rotkopf, Philipp Riffel, Stefan O. Schoenberg, and Matthias F. Froelich. 2022. "Comparison Study of Myocardial Radiomics Feature Properties on Energy-Integrating and Photon-Counting Detector CT" Diagnostics 12, no. 5: 1294. https://doi.org/10.3390/diagnostics12051294
APA StyleAyx, I., Tharmaseelan, H., Hertel, A., Nörenberg, D., Overhoff, D., Rotkopf, L. T., Riffel, P., Schoenberg, S. O., & Froelich, M. F. (2022). Comparison Study of Myocardial Radiomics Feature Properties on Energy-Integrating and Photon-Counting Detector CT. Diagnostics, 12(5), 1294. https://doi.org/10.3390/diagnostics12051294