
Photodynamic Diagnosis Using 5-Aminolevulinic Acid with a Novel Compact System and Chromaticity Analysis for the Detection of Oral Cancer and High-Risk Potentially Malignant Oral Disorders

 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Compact PDD System
2.2. Patients
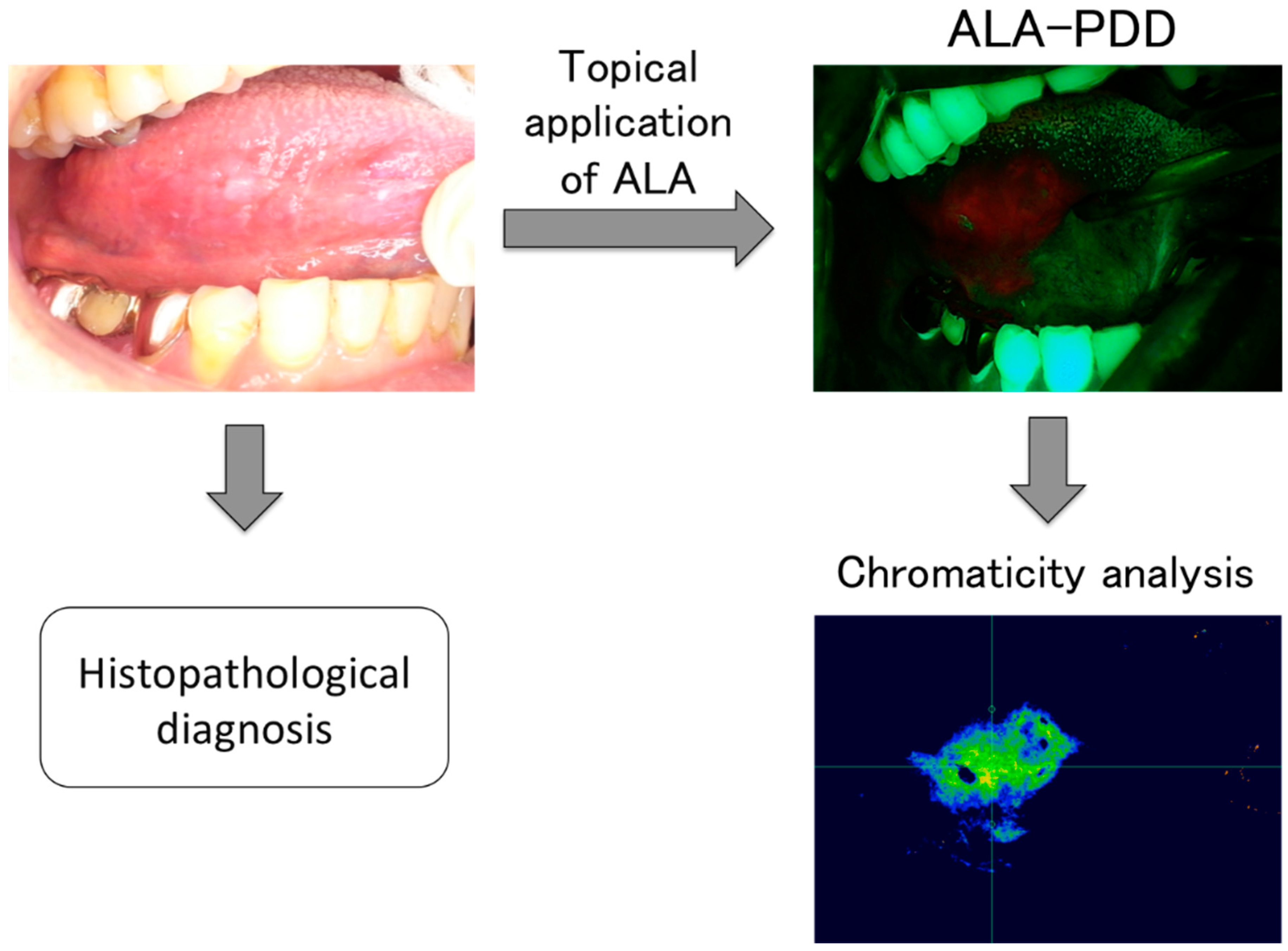
2.3. Examination Procedure
2.4. Statistical Analysis
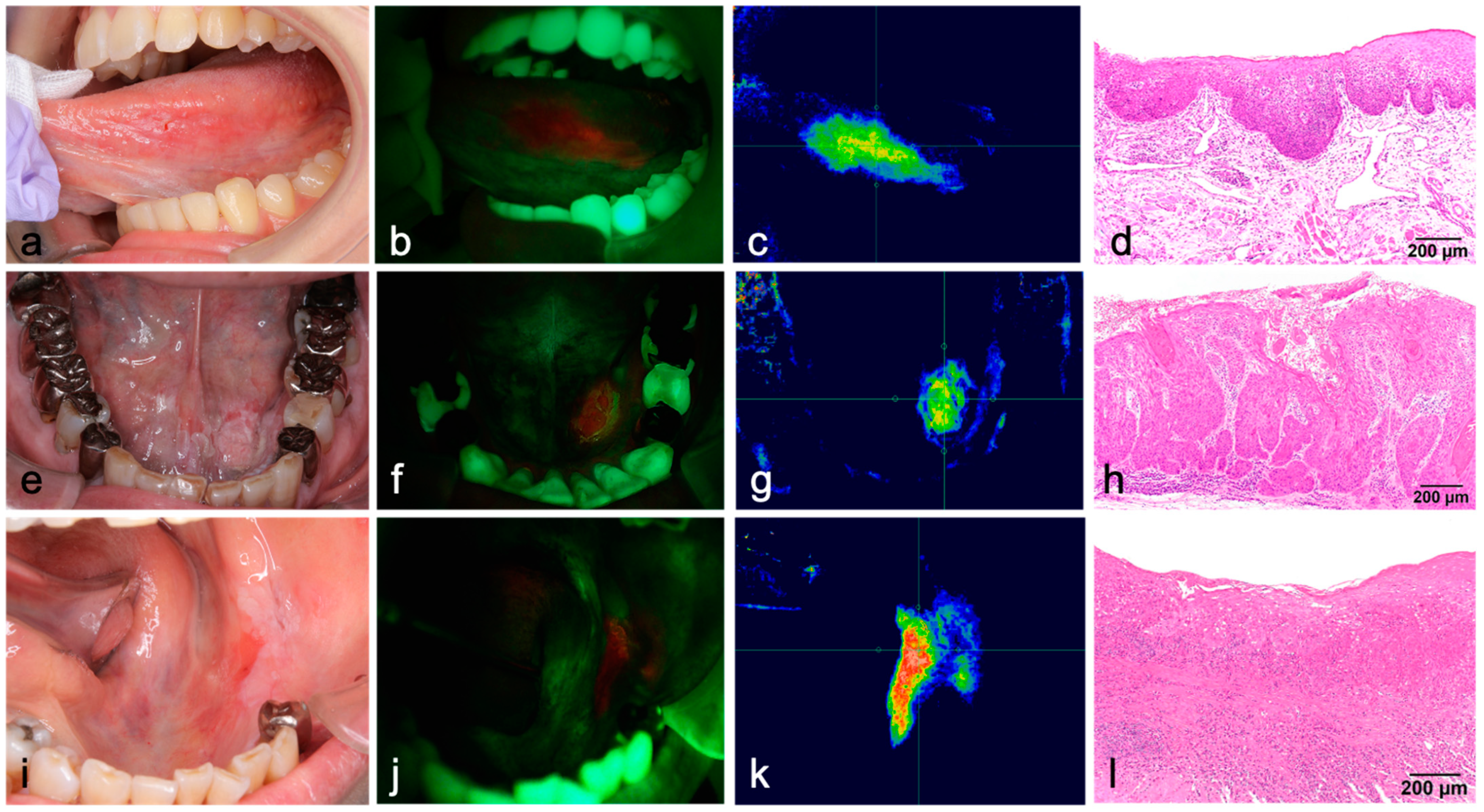
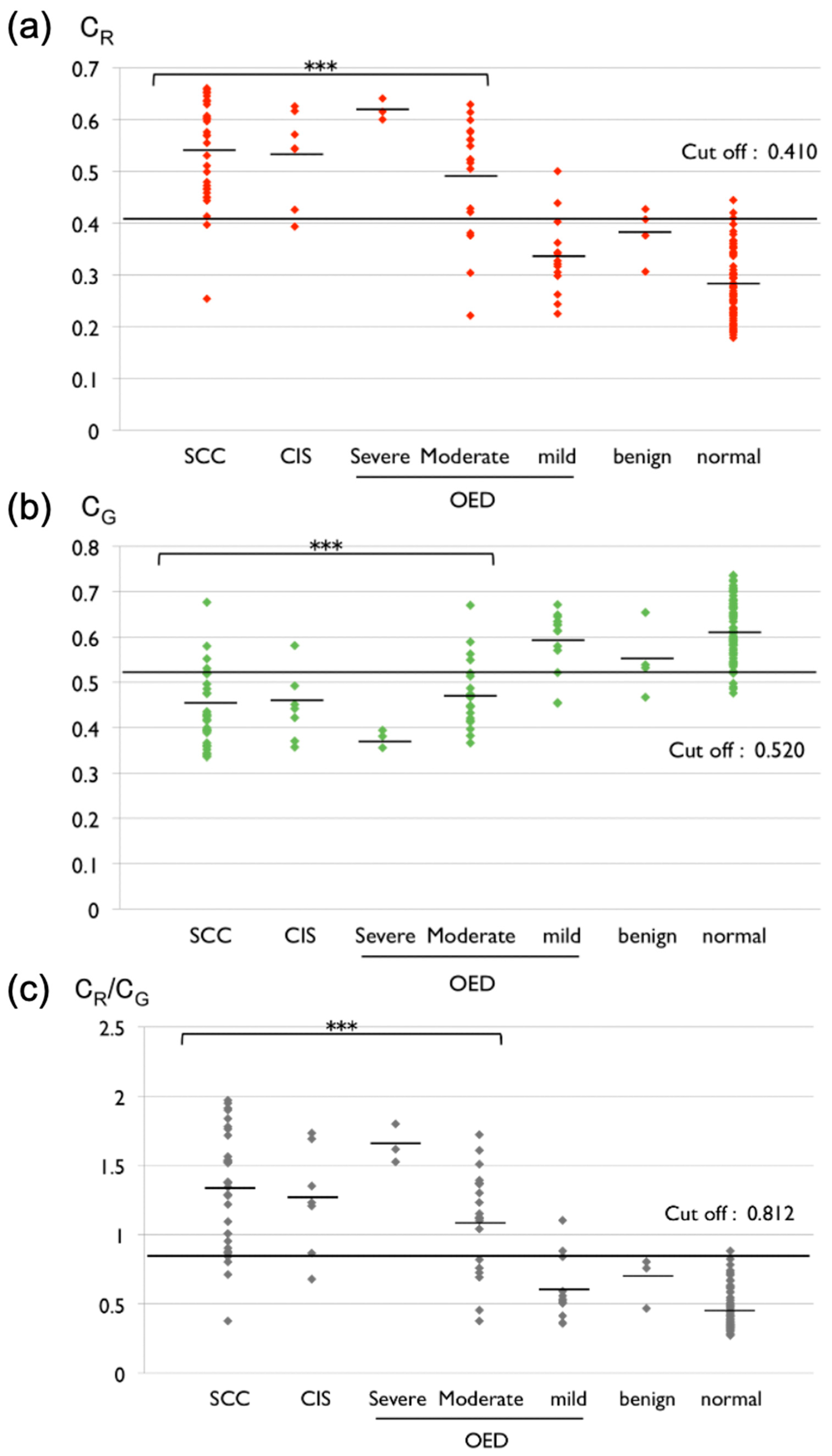
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Miranda-Filho, A.; Bray, F. Global patterns and trends in cancers of the lip, tongue and mouth. Oral Oncol. 2020, 102, 104551. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA A Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Warnakulasuriya, S. Global epidemiology of oral and oropharyngeal cancer. Oral Oncol. 2009, 45, 309–316. [Google Scholar] [CrossRef] [PubMed]
- Mehanna, H.M.; Rattay, T.; Smith, J.; McConkey, C.C. Treatment and follow-up of oral dysplasia—A systematic review and meta-analysis. Head Neck J. Sci. Spec. Head Neck 2009, 31, 1600–1609. [Google Scholar] [CrossRef]
- Sciubba, J.J. Oral cancer. The importance of early diagnosis and treatment. Am. J. Clin. Dermatol. 2001, 2, 239–251. [Google Scholar] [CrossRef]
- van der Waal, I. Are we able to reduce the mortality and morbidity of oral cancer; some considerations. Med. Oral Patol. Oral Y Cir. Buccal 2013, 18, e33–e37. [Google Scholar] [CrossRef]
- Reibel, J.; Gale, N.; Hille, J.; Hunt, J.L.; Lingen, M.; Muller, S.; Sloan, P.; Tilakarante, W.M.; Westra, W.H.; Williams, M.D.; et al. Oral potentially malignant disorders and oral epithelial dysplasia. In WHO Classification of Head and Neck Tumours, 4th ed.; El-Naggar, A.K., Chan, J.K.C., Grandis, J.R., Takata, T., Slootweg, P.P.J., Eds.; IARC: Lyon, France, 2017; pp. 112–115. [Google Scholar]
- Kuribayashi, Y.; Tsushima, F.; Sato, M.; Morita, K.; Omura, K. Recurrence patterns of oral leukoplakia after curative surgical resection: Important factors that predict the risk of recurrence and malignancy. J. Oral Pathol. Med. 2012, 41, 682–688. [Google Scholar] [CrossRef]
- Warnakulasuriya, S.; Kovacevic, T.; Madden, P.; Coupland, V.H.; Sperandio, M.; Odell, E.; Møller, H. Factors predicting malignant transformation in oral potentially malignant disorders among patients accrued over a 10-year period in South East England. J. Oral Pathol. Med. 2011, 40, 677–683. [Google Scholar] [CrossRef]
- Speight, P.M.; Khurram, S.A.; Kujan, O. Oral potentially malignant disorders: Risk of progression to malignancy. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2018, 125, 612–627. [Google Scholar] [CrossRef] [Green Version]
- Napier, S.S.; Speight, P.M. Natural history of potentially malignant oral lesions and conditions: An overview of the literature. J. Oral Pathol Med. 2008, 37, 1–10. [Google Scholar] [CrossRef]
- Epstein, J.B.; Güneri, P.; Boyacioglu, H.; Abt, E. The limitations of the clinical oral examination in detecting dysplastic oral lesions and oral squamous cell carcinoma. J. Am. Dent. Assoc. 2012, 143, 1332–1342. [Google Scholar] [CrossRef] [PubMed]
- Macey, R.; Walsh, T.; Brocklehurst, P.; Kerr, A.R.; Liu, J.L.; Lingen, M.W.; Ogden, G.R.; Warnakulasuriya, S.; Scully, C. Diagnostic tests for oral cancer and potentially malignant disorders in patients presenting with clinically evident lesions. Cochrane Database Syst. Rev. 2015, 2015, CD010276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, E.C.; Tan, M.T.; Schwarz, R.A.; Richards-Kortum, R.R.; Gillenwater, A.M.; Vigneswaran, N. Noninvasive diagnostic adjuncts for the evaluation of potentially premalignant oral epithelial lesions: Current limitations and future directions. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2018, 125, 670–681. [Google Scholar] [CrossRef] [PubMed]
- Patel, K.J.; de Silva, H.L.; Tong, D.C.; Love, R.M. Concordance between clinical and histopathologic diagnoses of oral mucosal lesions. J. Oral Maxillofac. Surg. 2011, 69, 125–133. [Google Scholar] [CrossRef]
- Warnakulasuriya, S.; Pindborg, J.J. Reliability of oral precancer screening by primary health care workers in Sri Lanka. Community Dent. Health 1990, 7, 73–79. [Google Scholar]
- Nagao, T.; Ikeda, N.; Fukano, H.; Miyazaki, H.; Yano, M.; Warnakulasuriya, S. Outcome following a population screening programme for oral cancer and precancer in Japan. Oral Oncol. 2000, 36, 340–346. [Google Scholar] [CrossRef]
- Kennedy, J.C.; Marcus, S.L.; Pottier, R.H. Photodynamic therapy (PDT) and photodiagnosis (PD) using endogenous photosensitization induced by 5-aminolevulinic acid (ALA): Mechanisms and clinical results. J. Clin. Laser Med. Surg. 1996, 14, 289–304. [Google Scholar] [CrossRef]
- Inoue, K.; Fukuhara, H.; Shimamoto, T.; Kamada, M.; Iiyama, T.; Miyamura, M.; Kurabayashi, A.; Furihata, M.; Tanimura, M.; Watanabe, H.; et al. Comparison between intravesical and oral administration of 5-aminolevulinic acid in the clinical benefit of photodynamic diagnosis for nonmuscle invasive bladder cancer. Cancer 2012, 118, 1062–1074. [Google Scholar] [CrossRef]
- Tamura, Y.; Kuroiwa, T.; Kajimoto, Y.; Miki, Y.; Miyatake, S.; Tsuji, M. Endoscopic identification and biopsy sampling of an intraventricular malignant glioma using a 5-aminolevulinic acid-induced protoporphyrin IX fluorescence imaging system. Technical note. J. Neurosurg. 2007, 106, 507–510. [Google Scholar] [CrossRef] [Green Version]
- Ishizuka, M.; Abe, F.; Sano, Y.; Takahashi, K.; Inoue, K.; Nakajima, M.; Kohda, T.; Komatsu, N.; Ogura, S.; Tanaka, T. Novel development of 5-aminolevurinic acid (ALA) in cancer diagnoses and therapy. Int. Immunopharmacol. 2011, 11, 358–365. [Google Scholar] [CrossRef]
- Kennedy, J.C.; Pottier, R.H. Endogenous protoporphyrin IX, a clinically useful photosensitizer for photodynamic therapy. J. Photochem. Photobiol. B Biol. 1992, 14, 275–292. [Google Scholar] [CrossRef]
- Peng, Q.; Moan, J.; Warloe, T.; Nesland, J.M.; Rimington, C. Distribution and photosensitizing efficiency of porphyrins induced by application of exogenous 5-aminolevulinic acid in mice bearing mammary carcinoma. Int. J. Cancer 1992, 52, 433–443. [Google Scholar] [CrossRef] [PubMed]
- Leunig, A.; Rick, K.; Stepp, H.; Gutmann, R.; Alwin, G.; Baumgartner, R.; Feyh, J. Fluorescence imaging and spectroscopy of 5-aminolevulinic acid induced protoporphyrin IX for the detection of neoplastic lesions in the oral cavity. Am. J. Surg. 1996, 172, 674–677. [Google Scholar] [CrossRef]
- Leunig, A.; Betz, C.S.; Mehlmann, M.; Stepp, H.; Arbogast, S.; Grevers, G.; Baumgartner, R. Detection of squamous cell carcinoma of the oral cavity by imaging 5-aminolevulinic acid-induced protoporphyrin IX fluorescence. Laryngoscope 2000, 110, 78–83. [Google Scholar] [CrossRef]
- Leunig, A.; Mehlmann, M.; Betz, C.; Stepp, H.; Arbogast, S.; Grevers, G.; Baumgartner, R. Fluorescence staining of oral cancer using a topical application of 5-aminolevulinic acid: Fluorescence microscopic studies. J. Photochem. Photobiol. B Biol. 2001, 60, 44–49. [Google Scholar] [CrossRef]
- Zheng, W.; Soo, K.C.; Sivanandan, R.; Olivo, M. Detection of neoplasms in the oral cavity by digitized endoscopic imaging of 5-aminolevulinic acid-induced protoporphyrin IX fluorescence. Int. J. Oncol. 2002, 21, 763–768. [Google Scholar] [CrossRef]
- Zheng, W.; Soo, K.C.; Sivanandan, R.; Olivo, M. Detection of squamous cell carcinomas and pre-cancerous lesions in the oral cavity by quantification of 5-aminolevulinic acid induced fluorescence endoscopic images. Lasers Surg. Med. 2002, 31, 151–157. [Google Scholar] [CrossRef]
- Zheng, W.; Olivo, M.; Soo, K.C. The use of digitized endoscopic imaging of 5-ALA-induced PPIX fluorescence to detect and diagnose oral premalignant and malignant lesions in vivo. Int. J. Cancer 2004, 110, 295–300. [Google Scholar] [CrossRef]
- Sharwani, A.; Jerjes, W.; Salih, V.; MacRobert, A.J.; El-Maaytah, M.; Khalil, H.S.; Hopper, C. Fluorescence spectroscopy combined with 5-aminolevulinic acid-induced protoporphyrin IX fluorescence in detecting oral premalignancy. J. Photochem. Photobiol. B Biol. 2006, 83, 27–33. [Google Scholar] [CrossRef]
- Edwards, P.C. The natural history of oral epithelial dysplasia: Perspective on Dost et al. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2014, 117, 263–266. [Google Scholar] [CrossRef]
- Dost, F.; Lê Cao, K.; Ford, P.J.; Ades, C.; Farah, C.S. Malignant transformation of oral epithelial dysplasia: A real-world evaluation of histopathologic grading. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2014, 117, 343–352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rashid, A.; Warnakulasuriya, S. The use of light-based (optical) detection systems as adjuncts in the detection of oral cancer and oral potentially malignant disorders: A systematic review. J. Oral Pathol. Med. 2015, 44, 307–328. [Google Scholar] [CrossRef] [PubMed]
- Nagi, R.; Reddy-Kantharaj, Y.B.; Rakesh, N.; Janardhan-Reddy, S.; Sahu, S. Efficacy of light based detection systems for early detection of oral cancer and oral potentially malignant disorders: Systematic review. Med. Oral Patol. Oral Cir. Bucal. 2016, 21, e447–e455. [Google Scholar] [CrossRef] [PubMed]
- Nankivell, P.P.; Williams, H.; Matthews, P.P.; Suortamo, S.; Snead, D.; McConkey, C.; Mehanna, H. The binary oral dysplasia grading system: Validity testing and suggested improvement. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 115, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Betz, C.S.; Stepp, H.; Janda, P.; Arbogast, S.; Grevers, G.; Baumgartner, R.; Leunig, A. A comparative study of normal inspection, autofluorescence and 5-ALA-induced PPIX fluorescence for oral cancer diagnosis. Int. J. Cancer 2002, 97, 245–252. [Google Scholar] [CrossRef] [PubMed]
- Kraft, M.; Betz, C.S.; Leunig, A.; Arens, C. Value of fluorescence endoscopy for the early diagnosis of laryngeal cancer and its precursor lesions. Head Neck 2011, 33, 941–948. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sex | |
| Male | 33 |
| Female | 34 |
| Age | 30–92 |
| Average | 64.8 |
| Site | |
| Tongue | 51 |
| Floor of mouth | 7 |
| Gingiva | 15 |
| Palatal | 1 |
| Buccal mucosa | 6 |
| Red Fluorescence | Histopathological Diagnosis | ||||||
|---|---|---|---|---|---|---|---|
| OSCC | CIS | OED | Benign | Total | |||
| Severe | Moderate | Mild | |||||
| Positive | 30 | 6 | 3 | 12 | 2 | 0 | 53 |
| Negative | 3 | 1 | 0 | 7 | 12 | 4 | 27 |
| Total | 33 | 7 | 3 | 19 | 14 | 4 | 80 |
| PDD | CR | CG | CR to CG | |
|---|---|---|---|---|
| AUC | — | 0.921 | 0.890 | 0.909 |
| Significance | — | p < 0.001 | p < 0.001 | p < 0.001 |
| Cutoff value | — | 0.410 | 0.520 | 0.812 |
| Sensitivity (%) | 82.3 | 88.7 | 83.3 | 85.5 |
| Specificity (%) | 88.9 | 83.3 | 83.9 | 83.3 |
| PPV | 0.962 | 0.948 | 0.945 | 0.946 |
| Accuracy | 0.838 | 0.875 | 0.838 | 0.850 |
| PDD | CR | CG | CR to CG | |
|---|---|---|---|---|
| AUC | — | 0.895 | 0.875 | 0.883 |
| Significance | — | p < 0.001 | p < 0.001 | p < 0.001 |
| Cutoff values | — | 0.414 | 0.520 | 0.804 |
| Sensitivity (%) | 72.4 | 82.8 | 83.3 | 79.3 |
| Specificity (%) | 88.9 | 83.3 | 82.8 | 83.3 |
| PPV | 0.913 | 0.889 | 0.889 | 0.885 |
| Accuracy | 0.787 | 0.830 | 0.830 | 0.809 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tatehara, S.; Sato, T.; Takebe, Y.; Fujinaga, M.; Tsutsumi-Arai, C.; Ito, Y.; Satomura, K. Photodynamic Diagnosis Using 5-Aminolevulinic Acid with a Novel Compact System and Chromaticity Analysis for the Detection of Oral Cancer and High-Risk Potentially Malignant Oral Disorders. Diagnostics 2022, 12, 1532. https://doi.org/10.3390/diagnostics12071532
Tatehara S, Sato T, Takebe Y, Fujinaga M, Tsutsumi-Arai C, Ito Y, Satomura K. Photodynamic Diagnosis Using 5-Aminolevulinic Acid with a Novel Compact System and Chromaticity Analysis for the Detection of Oral Cancer and High-Risk Potentially Malignant Oral Disorders. Diagnostics. 2022; 12(7):1532. https://doi.org/10.3390/diagnostics12071532
Chicago/Turabian StyleTatehara, Seiko, Toru Sato, Yusuke Takebe, Momoka Fujinaga, Chiaki Tsutsumi-Arai, Yumi Ito, and Kazuhito Satomura. 2022. "Photodynamic Diagnosis Using 5-Aminolevulinic Acid with a Novel Compact System and Chromaticity Analysis for the Detection of Oral Cancer and High-Risk Potentially Malignant Oral Disorders" Diagnostics 12, no. 7: 1532. https://doi.org/10.3390/diagnostics12071532
APA StyleTatehara, S., Sato, T., Takebe, Y., Fujinaga, M., Tsutsumi-Arai, C., Ito, Y., & Satomura, K. (2022). Photodynamic Diagnosis Using 5-Aminolevulinic Acid with a Novel Compact System and Chromaticity Analysis for the Detection of Oral Cancer and High-Risk Potentially Malignant Oral Disorders. Diagnostics, 12(7), 1532. https://doi.org/10.3390/diagnostics12071532