
Role of Diffusion Tensor Imaging in the Diagnosis of Traumatic Axonal Injury in Individual Patients with a Concussion or Mild Traumatic Brain Injury: A Mini-Review

Abstract
:1. Introduction
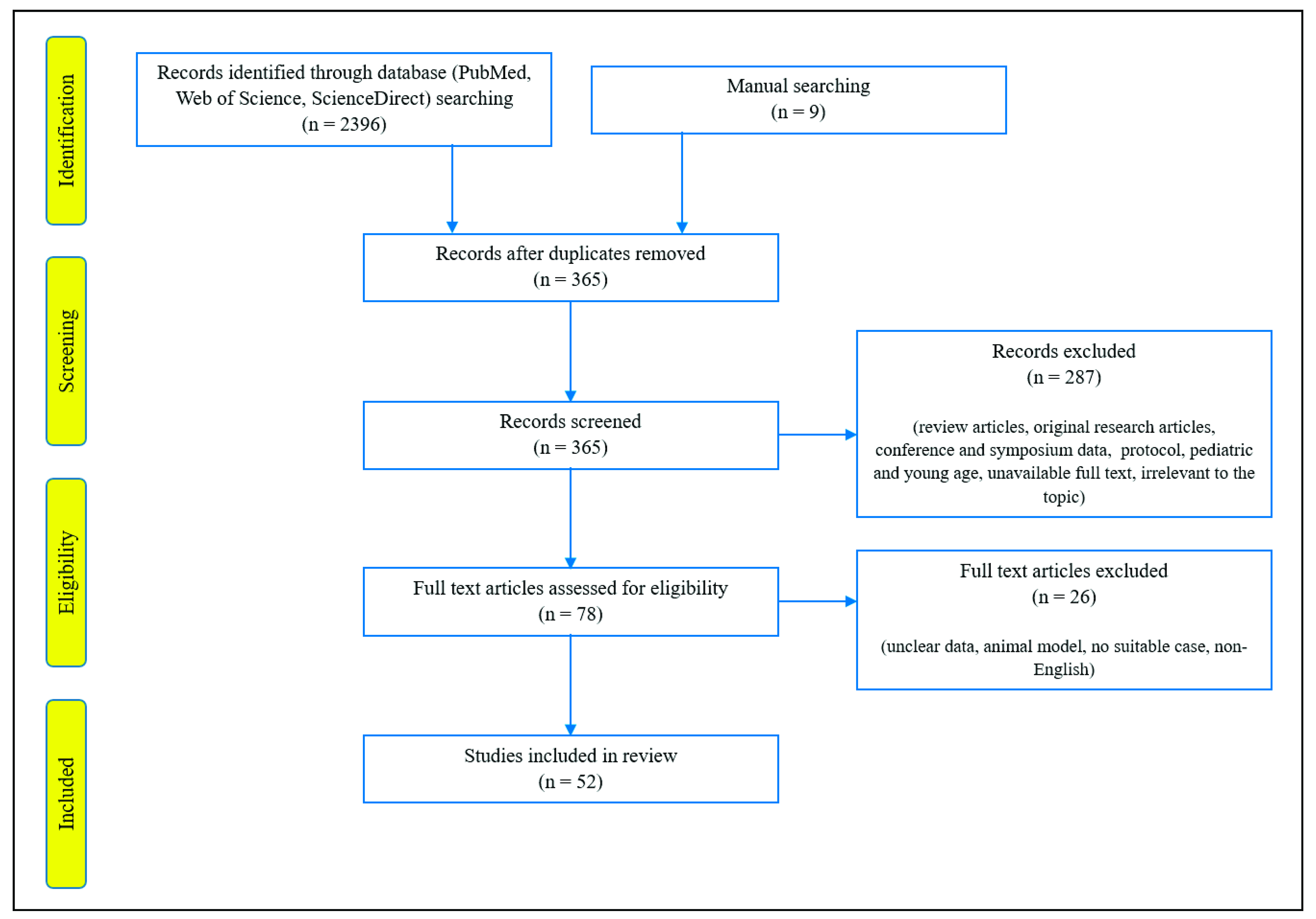
2. Method
3. Comparison of Diffusion Tensor Imaging and Diffusion Tensor Tractography in the Detection of Traumatic Axonal Injury in Concussion or Mild Traumatic Brain Injury
4. Diagnostic Approach to Traumatic Axonal Injuries in Individual Patients with Concussion
| Head trauma history compatible with mild TBI |
| ↓ |
| Development of new clinical symptoms and signs after head trauma |
| ↓ |
| Traumatic axonal injury findings on DTT for clinically relevant neural tracts |
| -Configuration: tearing, narrowing or discontinuation |
| -Significant change of DTT parameters: decreased fractional anisotropy or |
| tract volume, or increased mean diffusivity |
| ↓ |
| R/O Previous head trauma, concurrent neurological disease, aging or artifact of DTT |
| ↓ |
| R/O Other pathologies |
| (peripheral nerve injury, spinal cord injury, and musculoskeletal problems) |
| ↓ |
| Consider response to management for clinical symptoms |
| ↓ |
| Consider other clinical features and DTT findings of other neural tracts, |
| ↓ |
| Diagnosis of traumatic axonal injury |
5. Criteria for the Determination of Traumatic Axonal Injury Based on the Findings of Diffusion Tensor Tractography in Individual Patients with Concussion or mTBI
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gennarelli, T.A. Cerebral Concussion and Diffuse Brain Injuries, 3rd ed.; Williams & Wilkins: Baltimore, MD, USA, 1993. [Google Scholar]
- Jang, S.H. Diagnostic problems in diffuse axonal injury. Diagnostics 2020, 10, 117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Congress of Rehabilitation Medicine. Brain Injury Interdisciplinary Special Interest Group, Mild Traumatic Brain Injury Task Force Definition of mild traumatic brain injury. Definition of mild traumatic brain injury. J. Head Trauma Rehabil. 1993, 8, 86–87. [Google Scholar]
- Anderson, T.; Heitger, M.; Macleod, A.D. Concussion and mild head injury. Pract. Neurol. 2006, 6, 342–357. [Google Scholar] [CrossRef] [Green Version]
- Saatman, K.E.; Duhaime, A.C.; Bullock, R.; Maas, A.I.; Valadka, A.; Manley, G.T. Classification of traumatic brain injury for targeted therapies. J. Neurotrauma 2008, 25, 719–738. [Google Scholar] [CrossRef] [Green Version]
- Decuypere, M.; Klimo, P., Jr. Spectrum of traumatic brain injury from mild to severe. Surg. Clin. N. Am. 2012, 92, 939–957. [Google Scholar] [CrossRef]
- Povlishock, J.T.; Becker, D.P.; Cheng, C.L.; Vaughan, G.W. Axonal change in minor head injury. J. Neuropathol. Exp. Neurol. 1983, 42, 225–242. [Google Scholar] [CrossRef] [PubMed]
- Povlishock, J.T. Traumatically induced axonal injury: Pathogenesis and pathobiological implications. Brain Pathol. 1992, 2, 1–12. [Google Scholar]
- Povlishock, J.T.; Christman, C.W. The pathobiology of traumatically induced axonal injury in animals and humans: A review of current thoughts. J. Neurotrauma 1995, 12, 555–564. [Google Scholar] [CrossRef]
- Maxwell, W.L.; Povlishock, J.T.; Graham, D.L. A mechanistic analysis of nondisruptive axonal injury: A review. J. Neurotrauma 1997, 14, 419–440. [Google Scholar] [CrossRef]
- Johnson, V.E.; Stewart, W.; Smith, D.H. Axonal pathology in traumatic brain injury. Exp. Neurol. 2013, 246, 35–43. [Google Scholar] [CrossRef] [Green Version]
- Jang, S.H. Diagnostic history of traumatic axonal injury in patients with cerebral concussion and mild traumatic brain injury. Brain Neurorehabil. 2016, 9, e1. [Google Scholar] [CrossRef] [Green Version]
- Jang, S.H. Traumatic axonal injury. In Traumatic Brain Injury, 1st ed.; InTech: London, UK, 2018. [Google Scholar]
- Oppenheimer, D.R. Microscopic lesions in the brain following head injury. J. Neurol. Neurosurg. Psychiatry 1968, 31, 299–306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blumbergs, P.C.; Scott, G.; Manavis, J.; Wainwright, H.; Simpson, D.A.; McLean, A.J. Staining of amyloid precursor protein to study axonal damage in mild head injury. Lancet 1994, 344, 1055–1056. [Google Scholar] [CrossRef]
- Arfanakis, K.; Haughton, V.M.; Carew, J.D.; Rogers, B.P.; Dempsey, R.J.; Meyerand, M.E. Diffusion tensor MR imaging in diffuse axonal injury. AJNR Am. J. Neuroradiol. 2002, 23, 794–802. [Google Scholar]
- Hashimoto, K.; Okumura, A.; Shinoda, J.; Abo, M.; Nakamura, T. Tensor magnetic resonance imaging in a case of mild traumatic brain injury with lowered verbal intelligence quotient. J. Rehabil. Med. 2007, 39, 418–420. [Google Scholar] [CrossRef] [Green Version]
- Rosen, A.; Zhang, Y.; Zhan, W.; Kasprisin, A.; Martinson, S.; Cheng, J.; Weiner, M.; Yesavage, J.A.; Folio, L.; Ashford, J.W. Radiology corner. Case 41. Arcuate fasciculus damage seen on DTI in a blast-exposed soldier with mild traumatic brain injury (mTBI) with associated conduction aphasia. Mil Med. 2009, 174, v–vi. [Google Scholar]
- Hayes, J.P.; Morey, R.A.; Tupler, L.A. A case of frontal neuropsychological and neuroimaging signs following multiple primary-blast exposure. Neurocase 2012, 18, 258–269. [Google Scholar] [CrossRef] [PubMed]
- Lipton, M.L.; Kim, N.; Park, Y.K.; Hulkower, M.B.; Gardin, T.M.; Shifteh, K.; Kim, M.; Zimmerman, M.E.; Lipton, R.B.; Branch, C.A. Robust detection of traumatic axonal injury in individual mild traumatic brain injury patients: Intersubject variation, change over time and bidirectional changes in anisotropy. Brain Imaging Behav. 2012, 6, 329–342. [Google Scholar] [CrossRef]
- Shenton, M.E.; Hamoda, H.M.; Schneiderman, J.S.; Bouix, S.; Pasternak, O.; Rathi, Y.; Vu, M.A.; Purohit, M.P.; Helmer, K.; Koerte, I.; et al. A review of magnetic resonance imaging and diffusion tensor imaging findings in mild traumatic brain injury. Brain Imaging Behav. 2012, 6, 137–192. [Google Scholar] [CrossRef]
- Kim, N.; Branch, C.A.; Kim, M.; Lipton, M.L. Whole brain approaches for identification of microstructural abnormalities in individual patients: Comparison of techniques applied to mild traumatic brain injury. PLoS ONE 2013, 8, e59382. [Google Scholar] [CrossRef] [Green Version]
- Yeo, S.S.; Jang, S.H. Neural reorganization following bilateral injury of the fornix crus in a patient with traumatic brain injury. J. Rehabil. Med. 2013, 45, 595–598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwon, H.G.; Jang, S.H. Delayed gait disturbance due to injury of the corticoreticular pathway in a patient with mild traumatic brain injury. Brain Inj. 2014, 28, 511–514. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.D.; Jang, S.H. Changes of an injured fornix in a patient with mild traumatic brain injury: Diffusion tensor tractography follow-up study. Brain Inj. 2014, 28, 1485–1488. [Google Scholar] [CrossRef] [PubMed]
- Seo, J.P.; Jang, S.H. Injury of the spinothalamic tract in a patient with mild traumatic brain injury: Diffusion tensor tractography study. J. Rehabil. Med. 2014, 46, 374–377. [Google Scholar] [CrossRef] [Green Version]
- Suri, A.K.; Fleysher, R.; Lipton, M.L. Subject based registration for individualized analysis of diffusion tensor MRI. PLoS ONE 2015, 10, e0142288. [Google Scholar] [CrossRef] [Green Version]
- Jang, S.H.; Kwon, H.G. Injury of the dentato- rubro- thalamic tract in a patient with mild traumatic brain injury. Brain Inj. 2015, 29, 1725–1728. [Google Scholar] [CrossRef]
- Jang, S.H.; Kwon, H.G. Selective injury of fornical column in a patient with mild traumatic brain injury. Am. J. Phys. Med. Rehabil. 2015, 94, e86. [Google Scholar] [CrossRef]
- Jang, S.H.; Seo, J.P. Damage to the optic radiation in patients with mild traumatic brain injury. J. Neuroophthalmol. 2015, 35, 270–273. [Google Scholar] [CrossRef]
- Kim, J.W.; Lee, H.D.; Jang, S.H. Severe bilateral anterior cingulum injury in patients with mild traumatic brain injury. Neural. Regen. Res. 2015, 10, 1876–1878. [Google Scholar] [CrossRef]
- Seo, J.P.; Jang, S.H. Traumatic axonal injury of the corticospinal tract in the subcortical white matter in patients with mild traumatic brain injury. Brain Inj. 2015, 29, 110–114. [Google Scholar] [CrossRef]
- Jang, S.H.; Kim, S.H.; Lee, H.D. New neural tracts from bilateral fornical columns to compensate bilateral injury of fornical crura. Am. J. Phys. Med. Rehabil. 2016, 95, e75–e76. [Google Scholar] [CrossRef] [PubMed]
- Jang, S.H.; Kwon, H.G. Degeneration of an injured spinothalamic tract in a patient with mild traumatic brain injury. Brain Inj. 2016, 30, 1026–1028. [Google Scholar] [CrossRef] [PubMed]
- Jang, S.H.; Kwon, H.G. Injury of the ascending reticular activating system in patients with fatigue and hypersomnia following mild traumatic brain injury: Two case reports. Medicine 2016, 95, e2628. [Google Scholar] [CrossRef] [PubMed]
- Jang, S.H.; Lee, H.D. Central pain due to spinothalamic tract injury caused by indirect head trauma following a pratfall. Brain Inj. 2016, 30, 933–936. [Google Scholar] [CrossRef]
- Jang, S.H.; Lee, H.D. Compensatory neural tract from contralesional fornical body to ipsilesional medial temporal lobe in a patient with mild traumatic brain injury. Am. J. Phys. Med. Rehabil. 2016, 95, e14–e17. [Google Scholar] [CrossRef]
- Jang, S.H.; Seo, W.S.; Kwon, H.G. Post-traumatic narcolepsy and injury of the ascending reticular activating system. Sleep Med. 2016, 17, 124–125. [Google Scholar] [CrossRef]
- Jang, S.H.; Seo, Y.S. Dysarthria due to injury of the corticobulbar tract in a patient with mild traumatic brain injury. Am. J. Phys. Med. Rehabil. 2016, 95, e187–e188. [Google Scholar] [CrossRef]
- Jang, S.H.; Yi, J.H.; Kwon, H.G. Injury of the dorsolateral prefronto-thalamic tract in a patient with depression following mild traumatic brain injury: A case report. Medicine 2016, 95, e5009. [Google Scholar] [CrossRef]
- Jang, S.H.; Yi, J.H.; Kwon, H.G. Injury of the inferior cerebellar peduncle in patients with mild traumatic brain injury: A diffusion tensor tractography study. Brain Inj. 2016, 30, 1271–1275. [Google Scholar] [CrossRef]
- Yang, D.S.; Kwon, H.G.; Jang, S.H. Injury of the thalamocingulate tract in the papez circuit in patients with mild traumatic brain injury. Am. J. Phys. Med. Rehabil. 2016, 95, e34–e38. [Google Scholar] [CrossRef]
- Jang, S.H.; Kwon, H.G. Aggravation of an injured dentato-rubro-thalamic tract in a patient with mild traumatic brain injury: A case report. Medicine 2017, 96, e8253. [Google Scholar] [CrossRef] [PubMed]
- Jang, S.H.; Kwon, H.G. Aggravation of excessive daytime sleepiness concurrent with aggravation of an injured ascending reticular activating system in a patient with mild traumatic brain injury a case report. Medicine 2017, 96, e5958. [Google Scholar] [CrossRef] [PubMed]
- Jang, S.H.; Kwon, H.G. Akinetic mutism in a patient with mild traumatic brain injury: A diffusion tensor tractography study. Brain Inj. 2017, 31, 1159–1163. [Google Scholar] [CrossRef] [PubMed]
- Jang, S.H.; Kwon, H.G. Apathy Apathy due to injury of the prefrontocaudate tract following mild traumatic brain injury. Am. J. Phys. Med. Rehabil. 2017, 96, e130–e133. [Google Scholar] [CrossRef] [PubMed]
- Jang, S.H.; Kwon, H.G. Diffuse injury of the Papez circuit by focal head trauma: A diffusion tensor tractography study. Acta Neurol. Belg. 2017, 117, 389–391. [Google Scholar] [CrossRef] [PubMed]
- Jang, S.H.; Kwon, H.G. Injury of the cortico-ponto-cerebellar tract in a patient with mild traumatic brain injury: A case report. Medicine 2017, 96, e8749. [Google Scholar] [CrossRef] [PubMed]
- Jang, S.H.; Kwon, Y.H. Neural reorganization between injured cingula and the brainstem cholinergic nuclei in a patient with cerebral concussion: A case report. Medicine 2017, 96, e8436. [Google Scholar] [CrossRef]
- Jang, S.H.; Lee, H.D. Abundant unusual neural branches from the fornix in patients with mild traumatic brain injury: A diffusion tensor tractography study. Brain Inj. 2017, 31, 1530–1533. [Google Scholar] [CrossRef]
- Jang, S.H.; Lee, H.D. Severe and extensive traumatic axonal injury following minor and indirect head trauma. Brain Inj. 2017, 31, 416–419. [Google Scholar] [CrossRef]
- Jang, S.H.; Lee, H.D. Traumatic axonal injury despite clinical phenotype of mild traumatic brain injury: A case report. Brain Inj. 2017, 31, 1534–1537. [Google Scholar] [CrossRef]
- Jang, S.H.; Seo, J.P. Absent-mindedness and injury of the ascending reticular activating system in a patient with mild traumatic brain injury: A case report. Medicine 2017, 96, e9289. [Google Scholar] [CrossRef] [PubMed]
- Jang, S.H.; Seo, J.P. Delayed degeneration of the left fornical crus with verbal memory impairment in a patient with mild traumatic brain injury: A case report. Medicine 2017, 96, e9219. [Google Scholar] [CrossRef] [PubMed]
- Jang, S.H.; Seo, J.P. Limb-kinetic apraxia in a patient with mild traumatic brain injury: A case report. Medicine 2017, 96, e9008. [Google Scholar] [CrossRef] [PubMed]
- Jang, S.H.; Seo, J.P. Motor execution problem due to injured corticofugal tracts from the supplementary motor area in a patient with mild traumatic brain injury. Am. J. Phys. Med. Rehabil. 2017, 96, e193. [Google Scholar] [CrossRef]
- Jang, S.H.; Kim, S.H.; Seo, J.P. Recovery of an injured cingulum concurrent with improvement of short-term memory in a patient with mild traumatic brain injury. Brain Inj. 2018, 32, 144–146. [Google Scholar] [CrossRef]
- Jang, S.H.; Kwon, H.G. Injury of the Papez circuit in a patient with traumatic spinal cord injury and concomitant mild traumatic brain injury. Neural. Regen. Res. 2018, 13, 161–162. [Google Scholar] [CrossRef]
- Jung, S.H.; Lee, H.D. Weak phonation due to unknown injury of the corticobulbar tract in a patient with mild traumatic brain injury: A diffusion tensor tractography study. Neural. Regen. Res. 2018, 13, 936. [Google Scholar] [CrossRef]
- Jang, S.H.; Bae, C.H.; Seo, J.P. Injury of auditory radiation and sensorineural hearing loss from mild traumatic brain injury. Brain Inj. 2019, 33, 249–252. [Google Scholar] [CrossRef]
- Jang, S.H.; Kwon, Y.H.; Lee, S.J. Central pain due to injury of the spinothalamic tract misdiagnosed as complex regional pain syndrome: A case report. Diagnostics 2019, 9, 145. [Google Scholar] [CrossRef] [Green Version]
- Jang, S.H.; Lee, H.D. Diagnostic approach to traumatic axonal injury of the optic radiation in mild traumatic brain injury. Am. J. Phys. Med. Rehabil. 2019, 98, e92–e96. [Google Scholar] [CrossRef]
- Jang, S.H.; Lee, H.D. Diagnostic approach to traumatic axonal injury of the spinothalamic tract in individual patients with mild traumatic brain injury. Diagnostics 2019, 9, 199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jang, S.H.; Seo, Y.S. Diagnosis of conversion disorder using diffusion tensor tractography and transcranial magnetic stimulation in a patient with mild traumatic brain injury. Diagnostics 2019, 9, 155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jang, S.H.; Seo, Y.S. Headache due to spinothalamic tract injury in patients with mild traumatic brain injury: Two case reports. Medicine 2019, 98, e14306. [Google Scholar] [CrossRef]
- Lee, S.J.; Hoon, C.; Seo, J.P.; Jang, S.H. Diagnosis of tinnitus due to auditory radiation injury following whiplash injury: A case study. Diagnostics 2019, 10, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, M.C.; Seo, J.P. Injury of the dentato-rubro-thalamic tract in a patient with intentional tremor after mild traumatic brain injury: A case report. Brain Inj. 2020, 34, 1283–1286. [Google Scholar] [CrossRef]
- Churchill, N.W.; Hutchison, M.G.; Graham, S.J.; Schweizer, T.A. Baseline vs. cross-sectional MRI of concussion: Distinct brain patterns in white matter and cerebral blood flow. Sci. Rep. 2020, 10, 1643. [Google Scholar] [CrossRef] [Green Version]
- Jang, S.H.; Kwon, Y.H.; Lee, S.J. Abdominal pain due to the spinothalamic tract injury in patients with mild traumatic brain injury: A case report. BMC Neurol. 2020, 20, 117. [Google Scholar] [CrossRef] [Green Version]
- Jang, S.H.; Kwon, Y.H.; Lee, S.J. Contrecoup injury of the prefronto-thalamic tract in a patient with mild traumatic brain injury: A case report. Medicine 2020, 99, e21601. [Google Scholar] [CrossRef]
- Kang, D.H.; Kim, G.W. Changes in diffuse tensor imaging and therapeutic effect of repetitive transcranial magnetic stimulation in traumatic brain injury with central pain. Brain Sci. 2020, 10, 929. [Google Scholar] [CrossRef]
- Jang, S.H.; Seo, Y.S. Delayed onset of central pain due to traumatic axonal injury of the spinothalamic tract in a patient with mild traumatic brain injury. Pain Med. 2021, 22, 221–223. [Google Scholar] [CrossRef]
- Tayebi, M.; Holdsworth, S.J.; Champagne, A.A.; Cook, D.J.; Nielsen, P.; Lee, T.R.; Wang, A.; Fernandez, J.; Shim, V. The role of diffusion tensor imaging in characterizing injury patterns on athletes with concussion and subconcussive injury: A systematic review. Brain Inj. 2021, 35, 621–644. [Google Scholar] [CrossRef] [PubMed]
- Jang, S.H.; Kim, S.H.; Kwon, H.G. Diagnostic sensitivity of traumatic axonal injury of the spinothalamic tract in patients with mild traumatic brain injury. Medicine 2022, 101, e28536. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Friedland, R.P.; Auchus, A.P. Diffusion tensor imaging of normal-appearing white matter in mild cognitive impairment and early Alzheimer disease: Preliminary evidence of axonal degeneration in the temporal lobe. AJNR Am. J. Neuroradiol. 2007, 28, 1943–1948. [Google Scholar] [CrossRef] [Green Version]
- Son, S.M.; Ahn, Y.H.; Sakong, J.; Moon, H.K.; Ahn, S.H.; Lee, H.; Yu, I.K.; Shin, Y.J.; Jang, S.H. Diffusion tensor imaging demonstrates focal lesions of the corticospinal tract in hemiparetic patients with cerebral palsy. Neurosci. Lett. 2007, 420, 34–38. [Google Scholar] [CrossRef] [PubMed]
- O’Phelan, K.H.; Otoshi, C.K.; Ernst, T.; Chang, L.D. Common patterns of regional brain injury detectable by diffusion tensor imaging in otherwise normal-appearing white matter in patients with early moderate to severe traumatic brain injury. J. Neurotrauma 2018, 35, 739–749. [Google Scholar] [CrossRef]
- Salsone, M.; Caligiuri, M.E.; Vescio, V.; Arabia, G.; Cherubini, A.; Nicoletti, G.; Morelli, M.; Quattrone, A.; Vescio, B.; Nistico, R.; et al. Microstructural changes of normal-appearing white matter in vascular Parkinsonism. Park. Relat. Disord. 2019, 63, 60–65. [Google Scholar] [CrossRef]
- Ingo, C.; Lin, C.; Higgins, J.; Arevalo, Y.A.; Prabhakaran, S. Diffusion properties of normal-appearing white matter microstructure and severity of motor impairment in acute ischemic stroke. AJNR Am. J. Neuroradiol. 2020, 41, 71–78. [Google Scholar] [CrossRef]
- Margoni, M.; Villani, U.; Silvestri, E.; Franciotta, S.; Anglani, M.G.; Causin, F.; Rinaldi, F.; Perini, P.; Bertoldo, A.; Gallo, P. Quantification of normal-appearing white matter damage in early relapse-onset multiple sclerosis through neurite orientation dispersion and density imaging. Mult. Scler. Relat. Disord. 2022, 58, 103396. [Google Scholar] [CrossRef]
- Jang, S.H.; Byun, D.H. Hidden truth in cerebral concussion-traumatic axonal injury: A narrative mini-review. Healthcare 2022, 10, 931. [Google Scholar] [CrossRef]
- Jang, S.H. A review of corticospinal tract location at corona radiata and posterior limb of the internal capsule in human brain. Neurorehabilitation 2009, 24, 279–283. [Google Scholar] [CrossRef]
- Basser, P.J.; Pierpaoli, C. Microstructural and physiological features of tissues elucidated by quantitative-diffusion-tensor MRI. J. Magn. Reson. Ser. B 1996, 111, 209–219. [Google Scholar] [CrossRef]
- Mori, S.; Crain, B.J.; Chacko, V.P.; van Zijl, P.C. Three-dimensional tracking of axonal projections in the brain by magnetic resonance imaging. Ann. Neurol. 1999, 45, 265–269. [Google Scholar] [CrossRef]
- Kunimatsu, A.; Aoki, S.; Masutani, Y.; Abe, O.; Hayashi, N.; Mori, H.; Masumoto, T.; Ohtomo, K. The optimal trackability threshold of fractional anisotropy for diffusion tensor tractography of the corticospinal tract. Magn. Reson. Med. Sci. 2004, 3, 11–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.K.; Kim, D.I.; Kim, J.; Kim, D.J.; Kim, H.D.; Kim, D.S.; Mori, S. Diffusion-tensor MR imaging and fiber tractography: A new method of describing aberrant fiber connections in developmental CNS anomalies. Radiographics 2005, 25, 53–65. [Google Scholar] [CrossRef]
- Assaf, Y.; Pasternak, O. Diffusion tensor imaging (DTI)-based white matter mapping in brain research: A review. J. Mol. Neurosci. 2008, 34, 51–61. [Google Scholar] [CrossRef]
- Jang, S.H.; Chang, C.H.; Lee, J.; Kim, C.S.; Seo, J.P.; Yeo, S.S. Functional role of the corticoreticular pathway in chronic stroke patients. Stroke 2013, 44, 1099–1104. [Google Scholar] [CrossRef] [Green Version]
- Kasahara, K.; Hashimoto, K.; Abo, M.; Senoo, A. Voxel- and atlas-based analysis of diffusion tensor imaging may reveal focal axonal injuries in mild traumatic brain injury—Comparison with diffuse axonal injury. Magn. Reson. Imaging 2012, 30, 496–505. [Google Scholar] [CrossRef]
- Seo, J.P.; Kwon, Y.H.; Jang, S.H. Mini-review of studies reporting the repeatability and reproducibility of diffusion tensor imaging. Investig. Magn. Reson. Imaging 2019, 23, 26–33. [Google Scholar] [CrossRef]
- Parker, G.J.M.; Alexander, D.C. Probabilistic anatomical connectivity derived from the microscopic persistent angular structure of cerebral tissue. Philos. Trans. R. Soc. B Biol. Sci. 2005, 360, 893–902. [Google Scholar] [CrossRef]
- Yamada, K.; Sakai, K.; Akazawa, K.; Yuen, S.; Nishimura, T. MR Tractography: A review of its clinical applications. Magn. Reson. Med. Sci. 2009, 8, 165–174. [Google Scholar] [CrossRef] [Green Version]
- Jang, S.H.; Seo, Y.S. Diffusion tensor tractography characteristics of axonal injury in concussion/mild traumatic brain injury. Neural. Regen. Res. 2022, 17, 978–982. [Google Scholar] [CrossRef]
- Jang, S.H.; Kim, O.L.; Kim, S.H.; Lee, H.D. Differences in corpus callosum injury between cerebral concussion and diffuse axonal injury. Medicine 2019, 98, e17467. [Google Scholar] [CrossRef]
- Jang, S.H.; Lee, H.D. Diffusion tensor tractography studies on mechanisms of recovery of injured fornix. Neural. Regen. Res. 2017, 12, 1742–1744. [Google Scholar] [CrossRef]
- Eierud, C.; Craddock, R.C.; Fletcher, S.; Aulakh, M.; King-Casas, B.; Kuehl, D.; LaConte, S.M. Neuroimaging after mild traumatic brain injury: Review and meta-analysis. Neuroimage Clin. 2014, 4, 283–294. [Google Scholar] [CrossRef] [Green Version]
- Rajesh, A.; Cooke, G.E.; Monti, J.M.; Jahn, A.; Daugherty, A.M.; Cohen, N.J.; Kramer, A.F. Differences in brain architecture in remote mild traumatic brain injury. J. Neurotrauma 2017, 34, 3280–3287. [Google Scholar] [CrossRef]
- Crawford, J.R.; Garthwaite, P.H.; Porter, S. Point and interval estimates of effect sizes for the case-controls design in neuropsychology: Rationale, methods, implementations, and proposed reporting standards. Cogn. Neuropsychol. 2010, 27, 245–260. [Google Scholar] [CrossRef]
- Gelman, A. Bayesian Data Analysis, 3rd ed.; Chapman and Hall/CRC: London, UK, 2013. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Analysed Neural Structures | Authors and Publication Year | Clinical Features |
|---|---|---|
| Spinothalamic tract | Seo and Jang (2014) [26] Jang and Kwon (2016) [34] Jang and Lee (2016) [36] Jang and Lee (2017) [51] Jang and Lee (2017) [52] Jang et al. (2019) [61] Jang and Lee (2019) [63] Jang and Seo (2019) [65] Jang et al. (2020) [69] Kang and Kim (2020) [71] Jang and Seo (2021) [72] Jang et al. (2022) [74] | Central pain |
| Fornix | Yeo and Jang (2013) [23] Lee and Jang (2014) [25] Jang and Kwon (2015) [29] Jang et al. (2016) [33] Jang and Lee (2016) [37] Jang and Lee (2017) [50] Jang and Lee (2017) [52] Jang and Seo (2017) [54] | Memory impairment |
| ARAS | Jang et al. (2016) [38] Jang and Kwon (2016) [35] Jang and Kwon (2017) [44] Jang and Seo (2017) [53] | Narcolepsy Fatigue and hypersomnia Daytime hypersomnia Absent-mindedness |
| Prefronto-thalamic tract | Jang et al. (2016) [40] Jang and Kwon (2017) [45] Jang and Kwon (2017) [46] Jang et al. (2020) [70] | Depression Akinetic mutism Apathy Cognitive dysfunction and depression |
| Cingulum | Kim et al. (2015) [31] Jang and Kwon (2017) [49] Jang and Lee (2017) [52] Jang et al. (2018) [57] | Memory impairment |
| DRTT | Jang and Kwon (2015) [28] Jang and Kwon (2017) [43] Jang and Lee (2017) [51] Chang and Seo (2020) [67] | Tremor and truncal ataxia Tremor and truncal ataxia Tremor Tremor |
| Corticospinal tract | Seo and Jang (2015) [32] Jang and Lee (2017) [51] Jang and Lee (2017) [52] Jang and Seo (2019) [64] | Mild weakness Mild weakness Mild weakness Hemiparesis |
| Papez circuit | Yang et al. (2016) [42] Jang and Kwon (2017) [47] Jang and Kwon (2018) [58] | Memory impairment |
| Corpus callosum | Hashimoto et al. (2007) [17] Hayes et al. (2012) [19] | Lower verbal intelligence Memory, execution, and attention impairments |
| Corticofugal tract | Jang and Seo (2017) [55] Jang and Seo (2017) [56] | Limb-kinetic apraxia |
| Corticobulbar tract | Jang and Seo (2016) [39] Jang and Lee (2018) [59] | Dysarthria Weak phonation |
| Optic radiation | Jang and Seo (2015) [30] Jang and Lee (2019) [62] | Visual field defect |
| Auditory radiation | Jang et al. (2019) [60] Lee et al. (2019) [66] | Hearing impairment Tinnitus |
| CRT | Kwon and Jang (2014) [24] Jang and Lee (2017) [51] | Gait disturbance Mild proximal weakness |
| CPCT | Jang and Kwon (2017) [48] | Tremor and ataxia |
| Cerebellar peduncle | Jang et al. (2016) [41] | Balance problem |
| Arcuate fasciculus | Rosen et al. (2009) [18] | Conduction aphasia |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jang, S.-H.; Cho, M.-J. Role of Diffusion Tensor Imaging in the Diagnosis of Traumatic Axonal Injury in Individual Patients with a Concussion or Mild Traumatic Brain Injury: A Mini-Review. Diagnostics 2022, 12, 1580. https://doi.org/10.3390/diagnostics12071580
Jang S-H, Cho M-J. Role of Diffusion Tensor Imaging in the Diagnosis of Traumatic Axonal Injury in Individual Patients with a Concussion or Mild Traumatic Brain Injury: A Mini-Review. Diagnostics. 2022; 12(7):1580. https://doi.org/10.3390/diagnostics12071580
Chicago/Turabian StyleJang, Sung-Ho, and Min-Jye Cho. 2022. "Role of Diffusion Tensor Imaging in the Diagnosis of Traumatic Axonal Injury in Individual Patients with a Concussion or Mild Traumatic Brain Injury: A Mini-Review" Diagnostics 12, no. 7: 1580. https://doi.org/10.3390/diagnostics12071580
APA StyleJang, S. -H., & Cho, M. -J. (2022). Role of Diffusion Tensor Imaging in the Diagnosis of Traumatic Axonal Injury in Individual Patients with a Concussion or Mild Traumatic Brain Injury: A Mini-Review. Diagnostics, 12(7), 1580. https://doi.org/10.3390/diagnostics12071580