
D2BOF-COVIDNet: A Framework of Deep Bayesian Optimization and Fusion-Assisted Optimal Deep Features for COVID-19 Classification Using Chest X-ray and MRI Scans


 , ,
, ,
Abstract
:1. Introduction
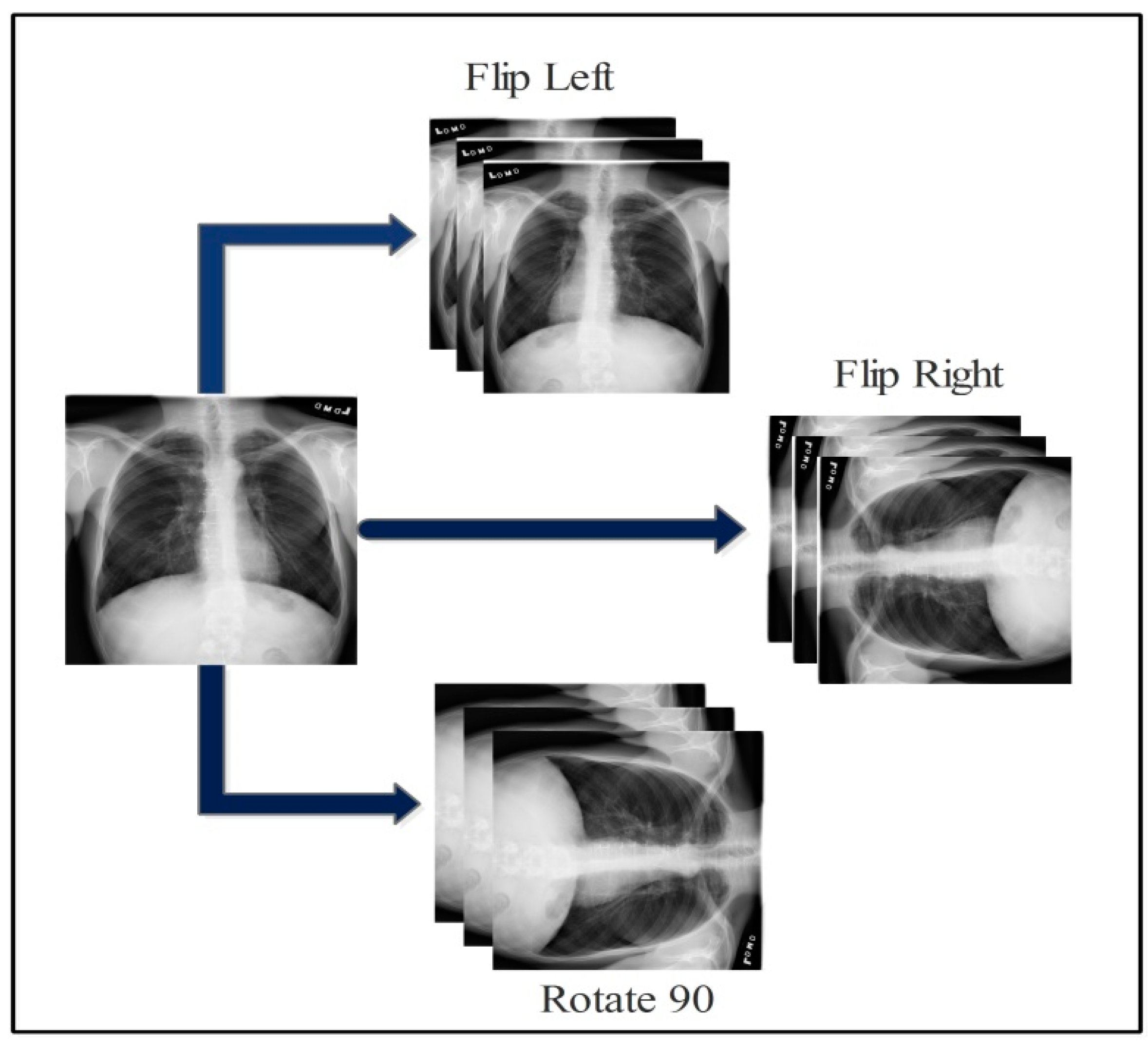
- Prepared a large dataset using flip and rotation operation from the original dataset and trained pre-trained deep learning models;
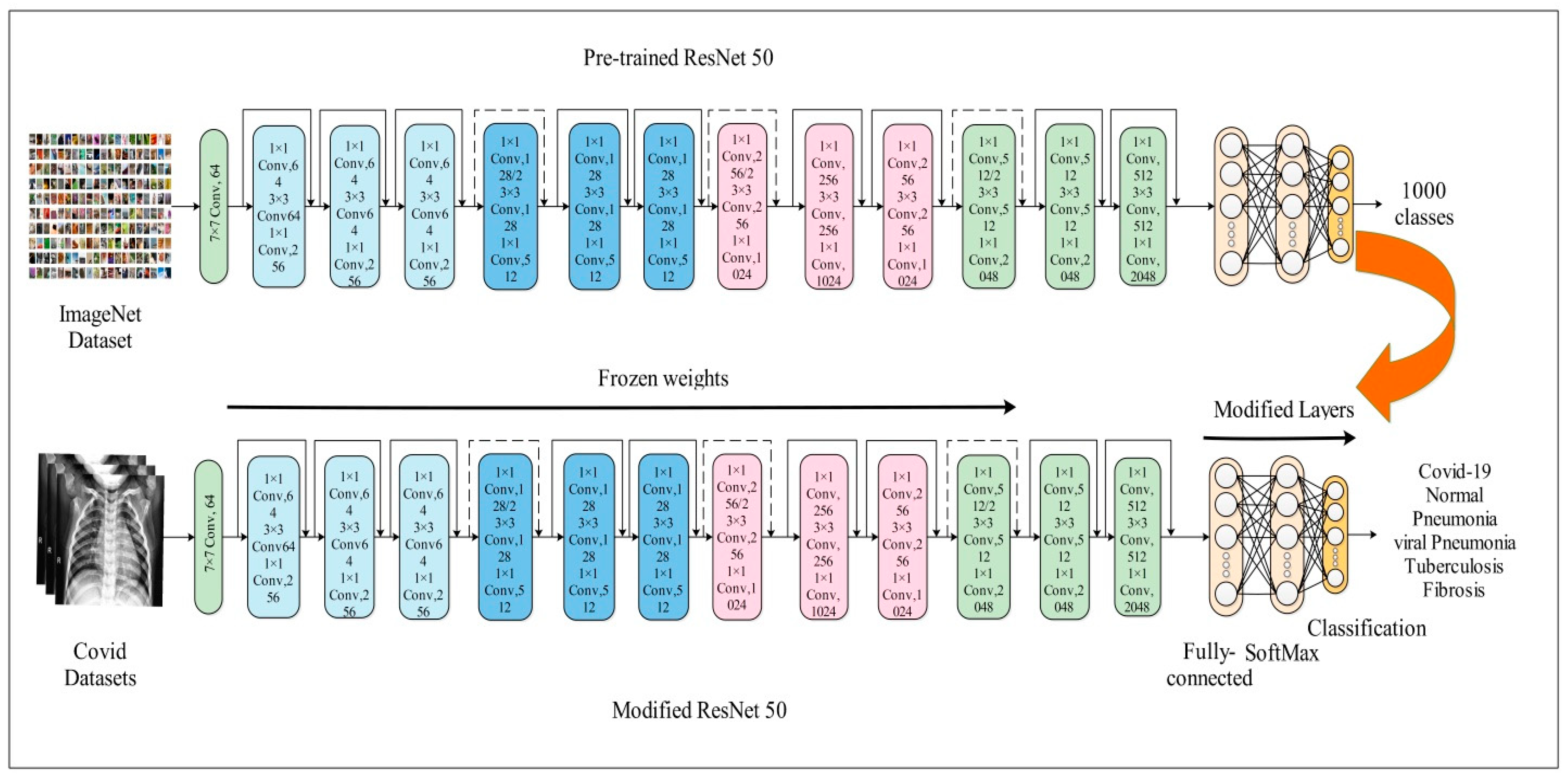
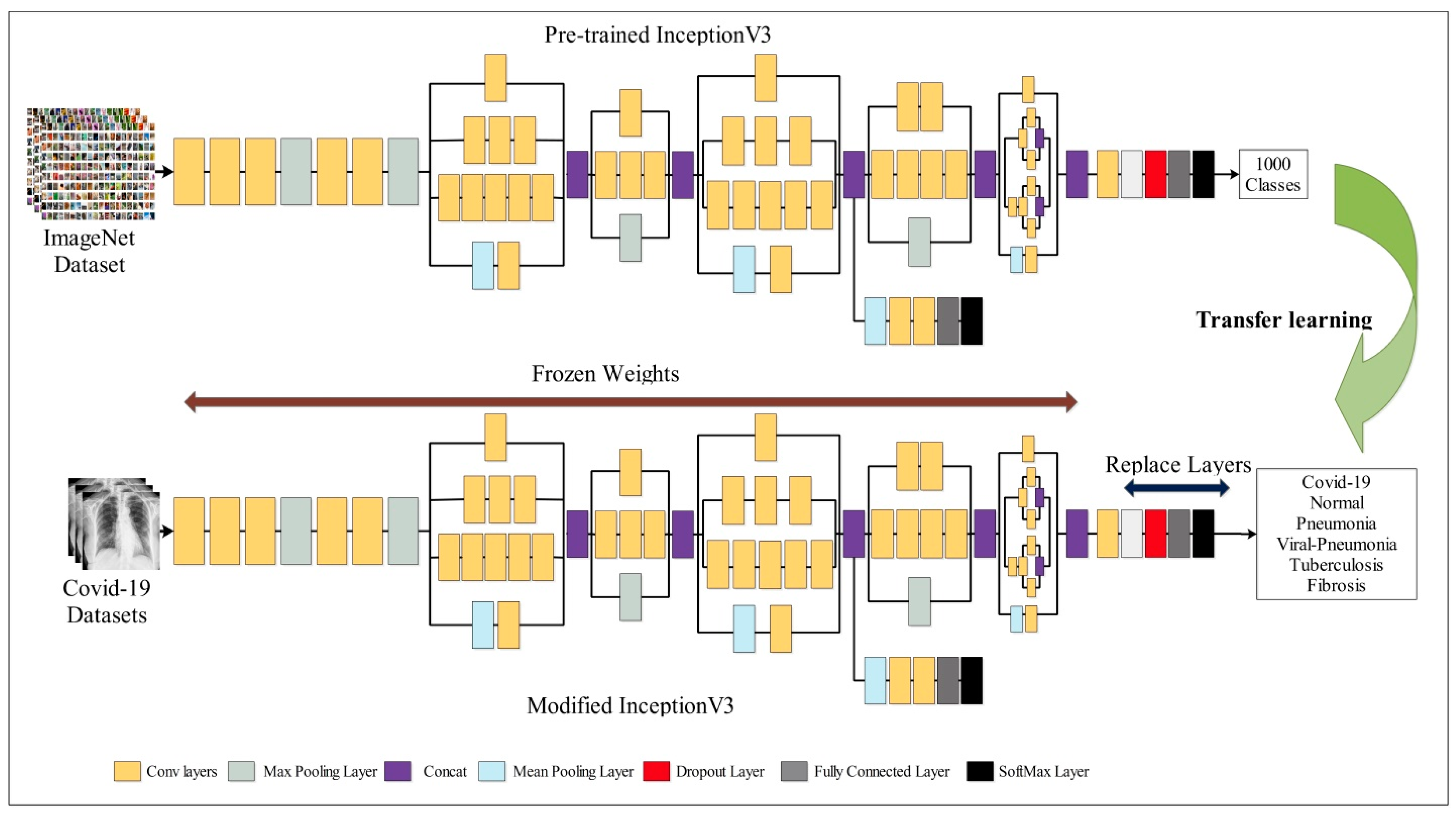
- Opted for the freezing weights procedure and selected hyperparameters through Bayesian optimization for efficient training using selected datasets;
- Proposed an improved canonical correlation analysis fusion technique for feature fusion of both deep learning models;
- Proposed an improved tree growth optimization for best feature selection.
2. Literature Review
3. Proposed Methodology
3.1. Dataset Selection and Normalization
3.2. Updated Pre-Trained RestNet50
3.3. Updated Pre-Trained InceptionV3
3.4. Hyperparameters Tuning Using BO
3.5. Improved Canonical Correlation Analysis Fusion
3.6. Improved Tree Growth Feature Selection
- Randomly generate the population of trees using lower and upper bounds, and calculate the fitness values;
- Considering feature selection, the objective is to minimize the solution. So, the minimum tree value is selected as the fittest value. At the kth iteration, presents the global best;
- Allow local search for B1 better solutions using the Equation (10). For every solution, do many local searches. If the value of the new answer is greater than the first response, then replace it with old value.where β presents the reduction rate of trees caused by aging high growth, and less food, and r presents , which causes the trees to satisfy the light, and the roots are instructed to move, absorb food and grow at a rate of units.
4. Experiment and Results
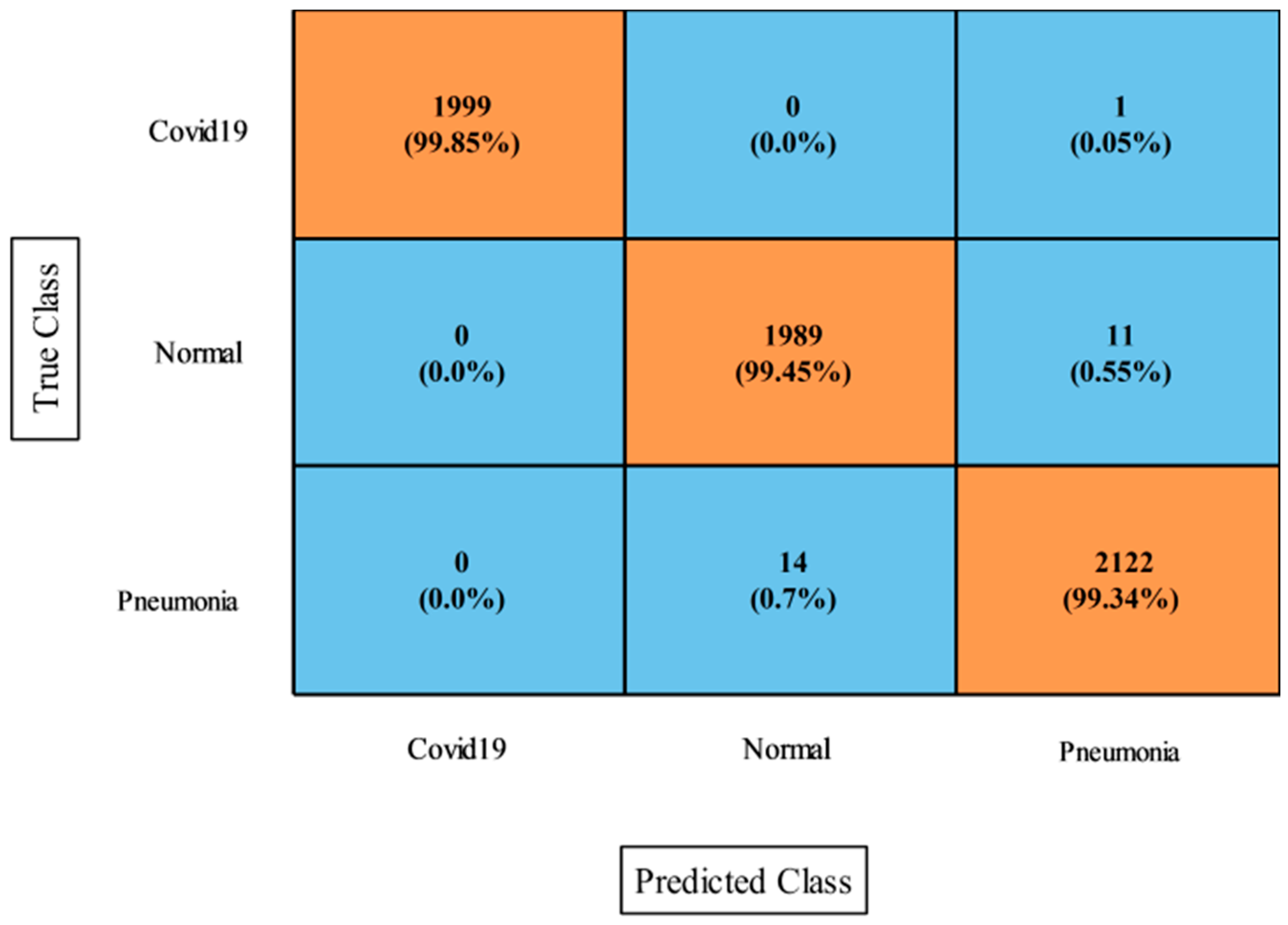
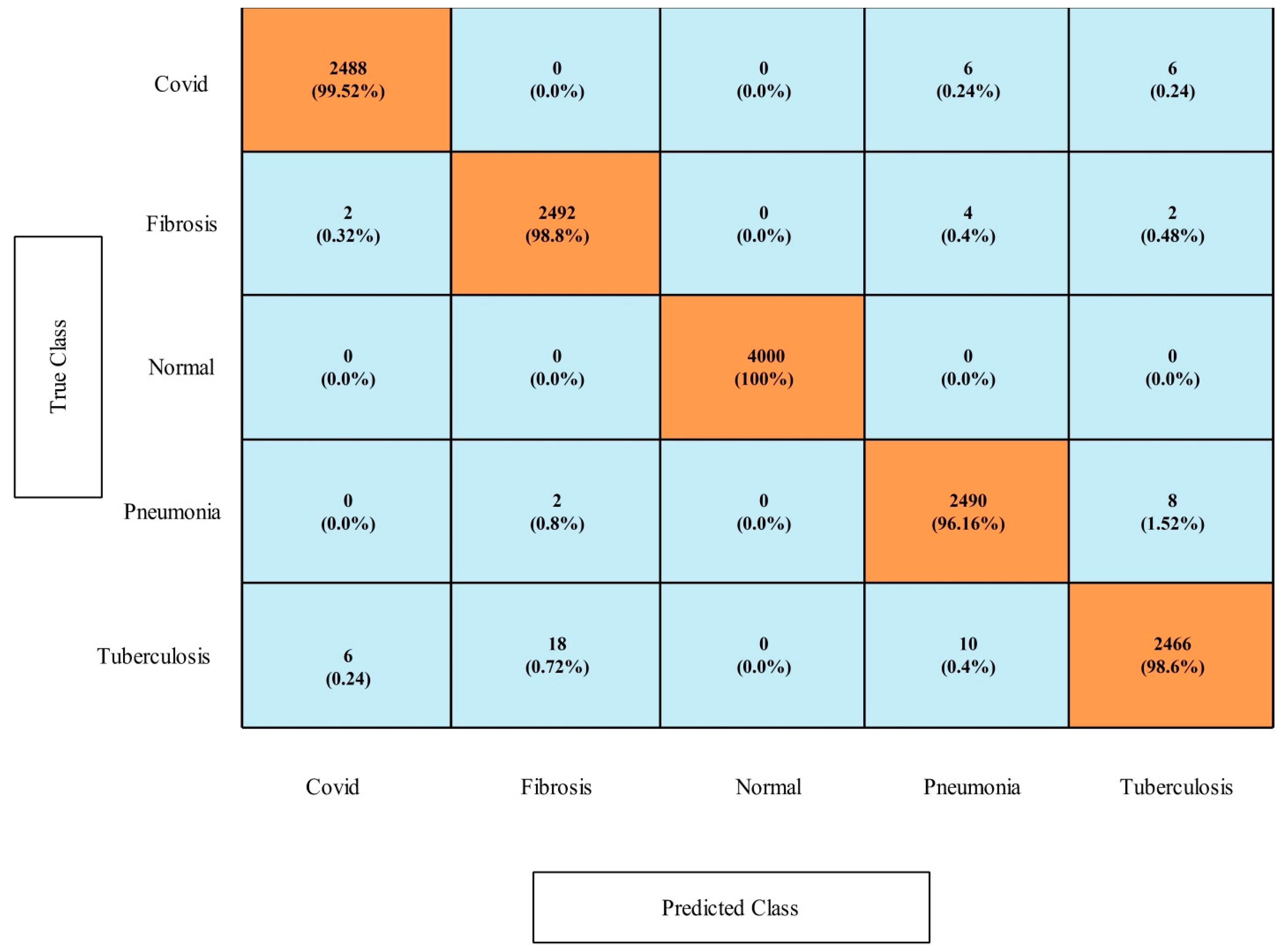
4.1. Chest X-ray (COVID-19 and Pneumonia) Dataset Results
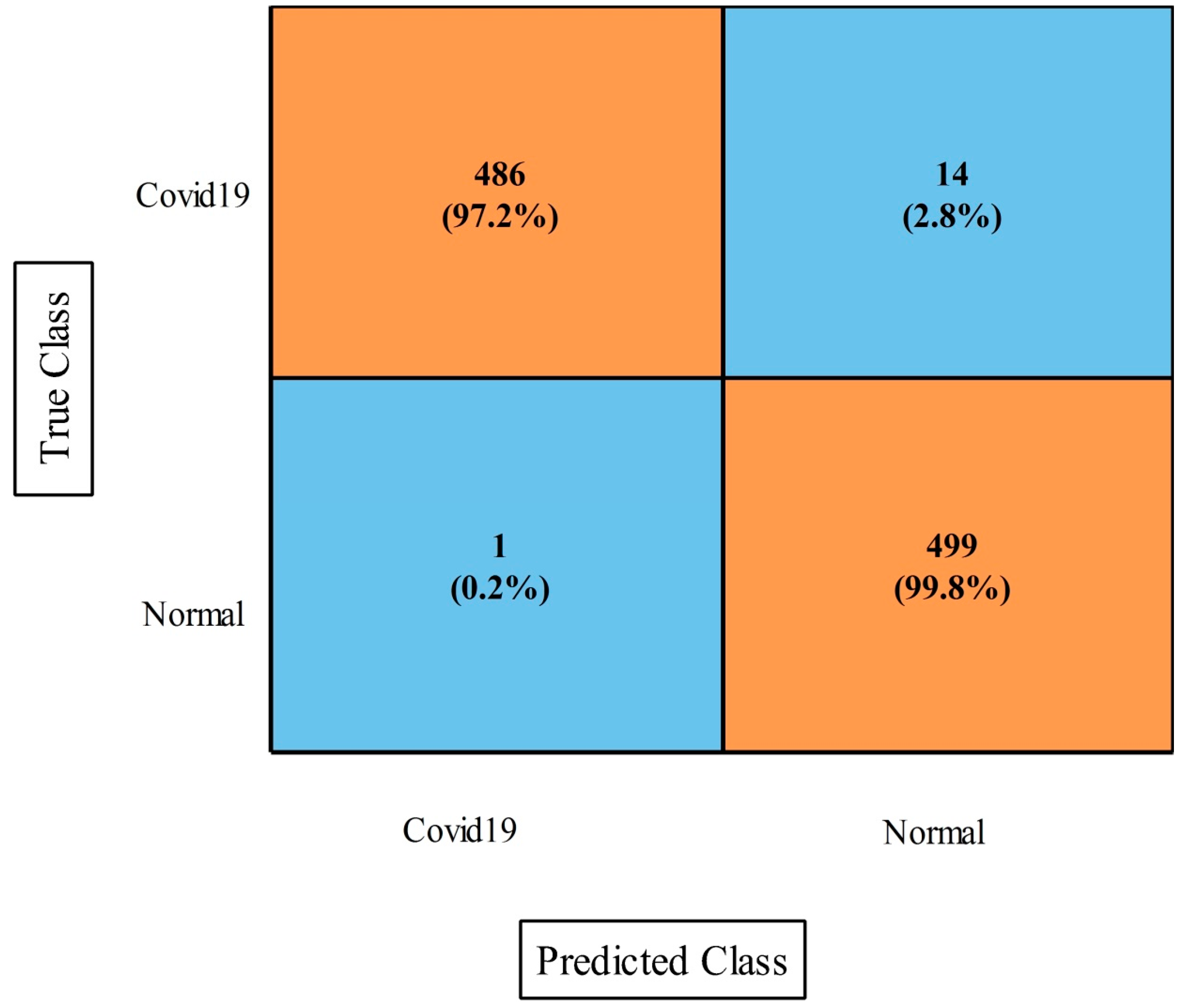
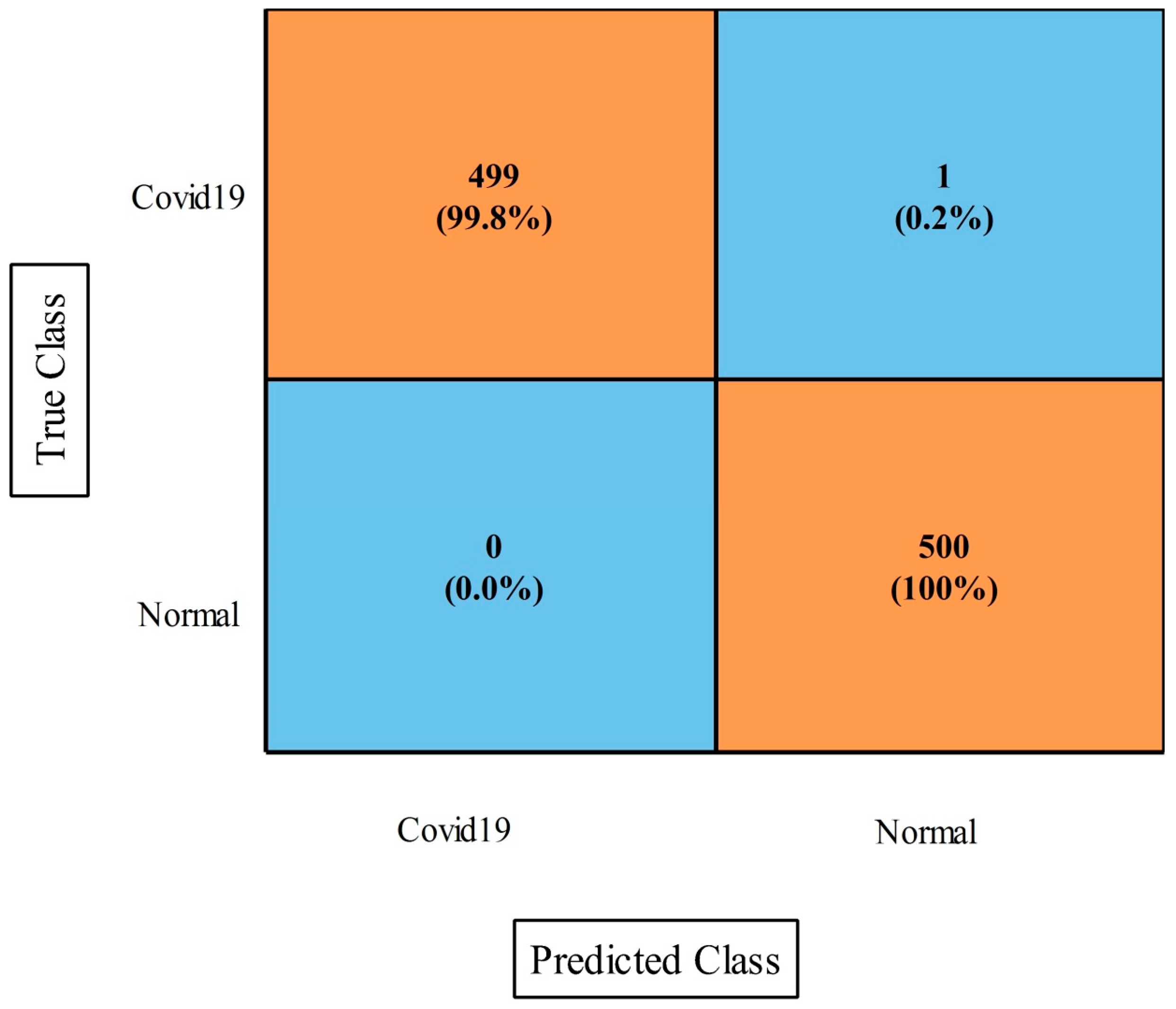
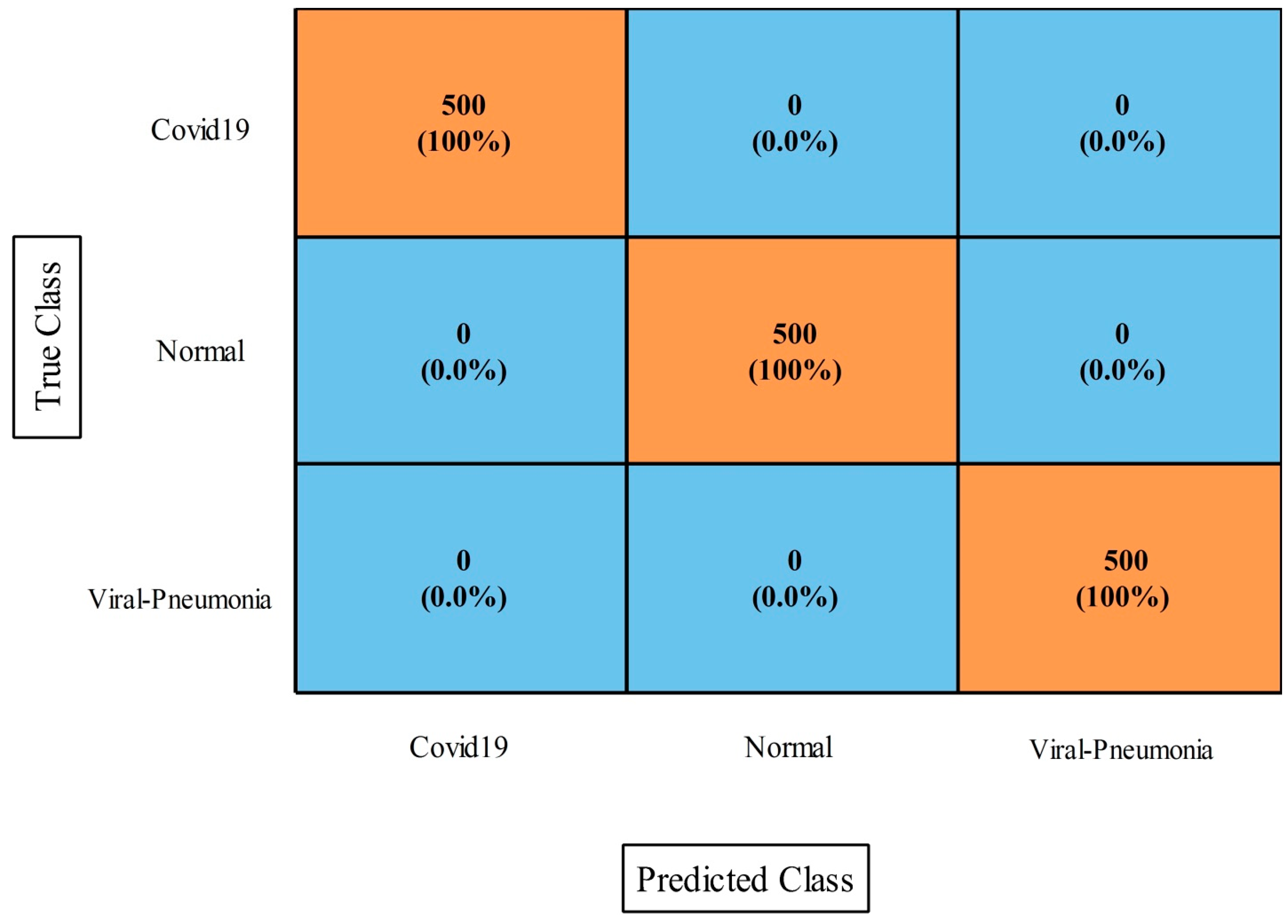
4.2. COVID-19 Patients Lungs X-ray Images Dataset
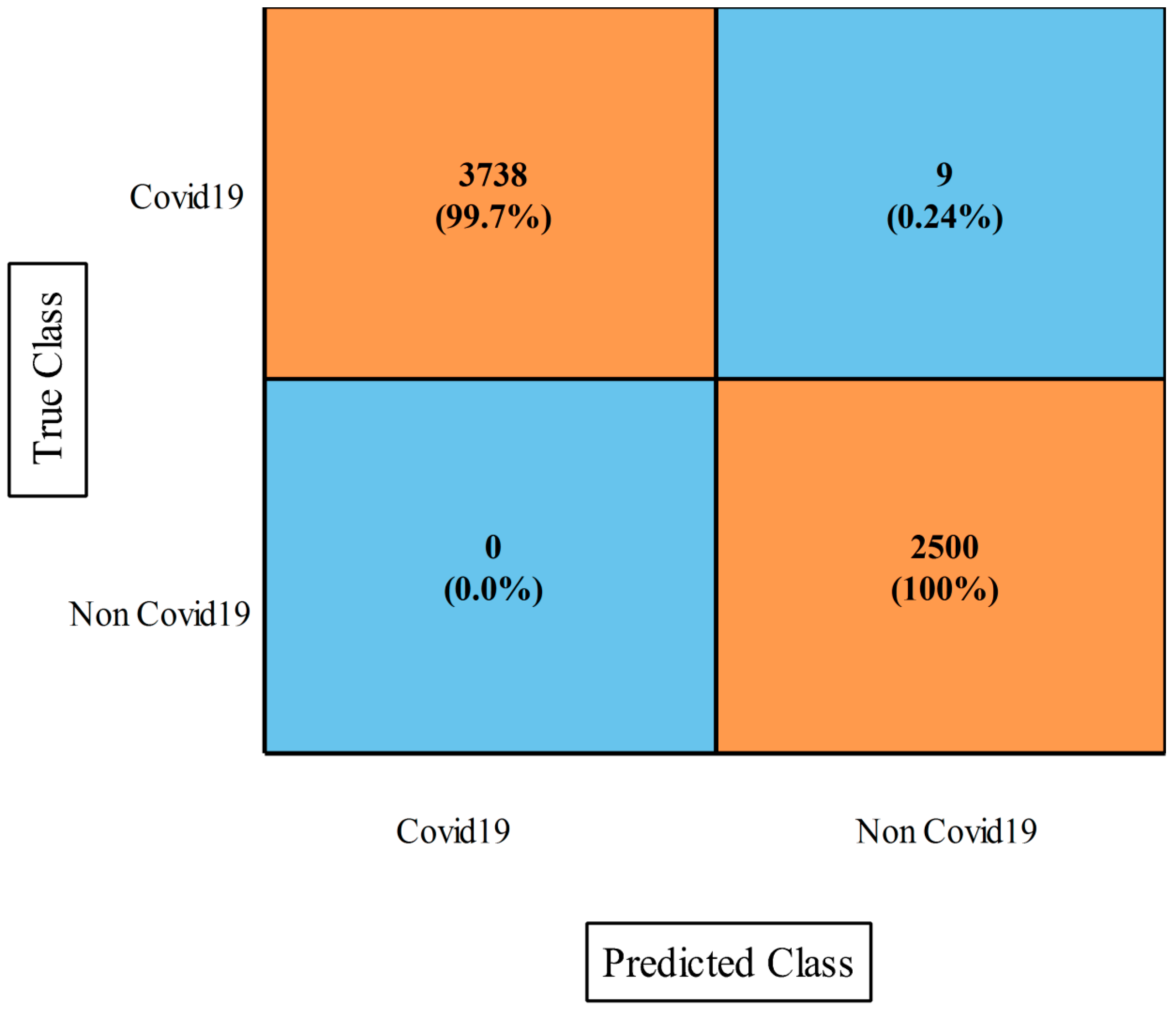
4.3. COVID-19 Lung CT Scans Dataset Results
4.4. COVID-19 Image Dataset Results
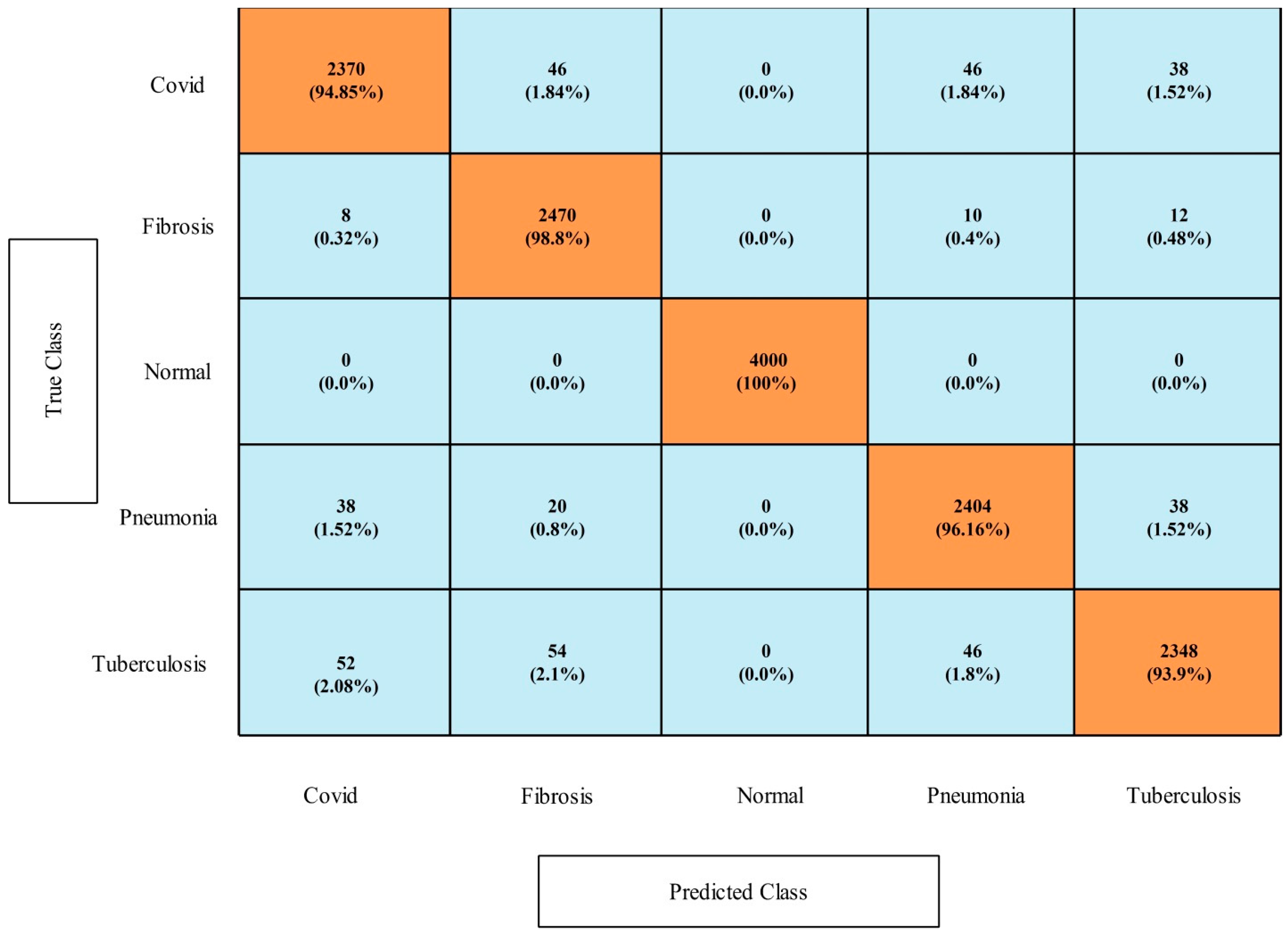
4.5. COVID-19 Detection Dataset Results
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A novel coronavirus from patients with pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Barth, R.F.; Buja, L.; Barth, A.L.; Carpenter, D.E.; Parwani, A.V. A Comparison of the Clinical, Viral, Pathologic, and Immunologic Features of Severe Acute Respiratory Syndrome (SARS), Middle East Respiratory Syndrome (MERS), and Coronavirus 2019 (COVID-19) Diseases. Arch. Pathol. Lab. Med. 2021, 145, 1194–1211. [Google Scholar] [CrossRef] [PubMed]
- Cui, J.; Li, F.; Shi, Z.-L. Origin and evolution of pathogenic coronaviruses. Nat. Rev. Microbiol. 2019, 17, 181–192. [Google Scholar] [CrossRef] [Green Version]
- Wong, C.K.; Lau, K.T.; Au, I.C.; Xiong, X.; Lau, E.H.; Cowling, B.J. Clinical improvement, outcomes, antiviral activity, and costs associated with early treatment with remdesivir for patients with coronavirus disease 2019 (COVID-19). Clin. Infect. Dis. 2022, 74, 1450–1458. [Google Scholar] [CrossRef]
- Ravi, V.; Narasimhan, H.; Chakraborty, C.; Pham, T.D. Deep learning-based meta-classifier approach for COVID-19 classification using CT scan and chest X-ray images. Multimed. Syst. 2022, 28, 1401–1415. [Google Scholar] [CrossRef]
- Verma, A.; Amin, S.B.; Naeem, M.; Saha, M. Detecting COVID-19 from chest computed tomography scans using AI-driven android application. Comput. Biol. Med. 2022, 143, 105298. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Kang, B.; Ma, J.; Zeng, X.; Xiao, M.; Guo, J.; Cai, M.; Yang, J.; Li, Y.; Meng, X.; et al. A deep learning algorithm using CT images to screen for Corona Virus Disease (COVID-19). Eur. Radiol. 2021, 31, 6096–6104. [Google Scholar] [CrossRef] [PubMed]
- Nanda, A.; Barik, R.C.; Bakshi, S. SSO-RBNN driven brain tumor classification with Saliency-K-means segmentation technique. Biomed. Signal Process. Control 2023, 81, 104356. [Google Scholar] [CrossRef]
- Dai, W.C.; Zhang, H.W.; Yu, J.; Xu, H.J.; Chen, H.; Luo, S.P.; Zhang, H.; Liang, L.H.; Wu, X.L.; Lei, Y.; et al. CT imaging and differential diagnosis of COVID-19. Can. Assoc. Radiol. J. 2020, 71, 195–200. [Google Scholar] [CrossRef] [Green Version]
- Littrup, P.J.; Freeman-Gibb, L.; Andea, A.; White, M.; Amerikia, K.C.; Bouwman, D.; Harb, T.; Sakr, W. Cryotherapy for breast fibroadenomas. Radiology 2005, 234, 63–72. [Google Scholar] [CrossRef]
- Zieleskiewicz, L.; Markarian, T.; Lopez, A.; Taguet, C.; Mohammedi, N.; Boucekine, M.; Baumstarck, K.; Besch, G.; Mathon, G.; Duclos, G.; et al. Comparative study of lung ultrasound and chest computed tomography scan in the assessment of severity of confirmed COVID-19 pneumonia. Intensive Care Med. 2020, 46, 1707–1713. [Google Scholar] [CrossRef] [PubMed]
- Khan, E.; Rehman, M.Z.U.; Ahmed, F.; Alfouzan, F.A.; Alzahrani, N.M.; Ahmad, J. Chest X-ray classification for the detection of COVID-19 using deep learning techniques. Sensors 2022, 22, 1211. [Google Scholar] [CrossRef] [PubMed]
- Castiglioni, I.; Rundo, L.; Codari, M.; Di Leo, G.; Salvatore, C.; Interlenghi, M.; Gallivanone, F.; Cozzi, A.; D’Amico, N.C.; Sardanelli, F. AI applications to medical images: From machine learning to deep learning. Phys. Med. 2021, 83, 9–24. [Google Scholar] [CrossRef] [PubMed]
- Marentakis, P.; Karaiskos, P.; Kouloulias, V.; Kelekis, N.; Argentos, S.; Oikonomopoulos, N.; Loukas, C. Lung cancer histology classification from CT images based on radiomics and deep learning models. Med. Biol. Eng. Comput. 2021, 59, 215–226. [Google Scholar] [CrossRef] [PubMed]
- Roy, S.; Meena, T.; Lim, S.-J. Demystifying Supervised Learning in Healthcare 4.0: A New Reality of Transforming Diagnostic Medicine. Diagnostics 2022, 12, 2549. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.A.; Azhar, M.; Ibrar, K.; Alqahtani, A.; Alsubai, S.; Binbusayyis, A.; Kim, Y.J.; Chang, B. COVID-19 classification from chest X-ray images: A framework of deep explainable artificial intelligence. Comput. Intell. Neurosci. 2022, 2022, 4254631. [Google Scholar] [CrossRef] [PubMed]
- Franklin, M.M.; Schultz, F.A.; Tafoya, M.A.; Kerwin, A.A.; Broehm, C.J.; Fischer, E.G.; Gullapalli, R.R.; Clark, D.P.; Hanson, J.A.; Martin, D.R. A deep learning convolutional neural network can differentiate between Helicobacter pylori gastritis and autoimmune gastritis with results comparable to gastrointestinal pathologists. Arch. Pathol. Lab. Med. 2022, 146, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Kaya, Y.; Yiner, Z.; Kaya, M.; Kuncan, F. A new approach to COVID-19 detection from X-ray images using angle transformation with GoogleNet and LSTM. Meas. Sci. Technol. 2022, 33, 124011. [Google Scholar] [CrossRef]
- Eken, S. A topic-based hierarchical publish/subscribe messaging middleware for COVID-19 detection in X-ray image and its metadata. Soft Comput. 2020, 2, 1–11. [Google Scholar] [CrossRef]
- Yilmaz, A. Çok kanallı CNN mimarisi ile X-Ray görüntülerinden COVID-19 tanısı. Gazi Üniversitesi Mühendislik Mimar. Fakültesi Derg. 2021, 36, 1761–1774. [Google Scholar] [CrossRef]
- Nair, R.; Alhudhaif, A.; Koundal, D.; Doewes, R.I.; Sharma, P. Deep learning-based COVID-19 detection system using pulmonary CT scans. Turk. J. Electr. Eng. Comput. Sci. 2021, 29, 2716–2727. [Google Scholar] [CrossRef]
- Hamza, A.; Khan, M.A.; Wang, S.H.; Alqahtani, A.; Alsubai, S.; Binbusayyis, A.; Hussein, H.S.; Martinetz, T.M.; Alshazly, H. COVID-classification using chest X-ray images: A framework of CNN-LSTM and improved max value moth flame optimization. Front. Public Health 2022, 10, 948205. [Google Scholar] [CrossRef] [PubMed]
- Fan, X.; Feng, X.; Dong, Y.; Hou, H. COVID-19 CT image recognition algorithm based on transformer and CNN. Displays 2022, 72, 102150. [Google Scholar] [CrossRef] [PubMed]
- Garg, A.; Salehi, S.; La Rocca, M.; Garner, R.; Duncan, D. Efficient and visualizable convolutional neural networks for COVID-19 classification using Chest CT. Expert Syst. Appl. 2022, 195, 116540. [Google Scholar] [CrossRef] [PubMed]
- Gayathri, J.; Abraham, B.; Sujarani, M.; Nair, M.S. A computer-aided diagnosis system for the classification of COVID-19 and non-COVID-19 pneumonia on chest X-ray images by integrating CNN with sparse autoencoder and feed forward neural network. Comput. Biol. Med. 2022, 141, 105134. [Google Scholar]
- AbdElhamid, A.A.; AbdElhalim, E.; Mohamed, M.A.; Khalifa, F. Multi-Classification of Chest X-rays for COVID-19 Diagnosis Using Deep Learning Algorithms. Appl. Sci. 2022, 12, 2080. [Google Scholar] [CrossRef]
- Kumar, R.; Arora, R.; Bansal, V.; Sahayasheela, V.J.; Buckchash, H.; Imran, J.; Narayanan, N.; Pandian, G.N.; Raman, B. Classification of COVID-19 from chest X-ray images using deep features and correlation coefficient. Multimed. Tools Appl. 2022, 81, 27631–27655. [Google Scholar] [CrossRef]
- Gampala, V.; Rathan, K.; Shajin, F.H.; Rajesh, P. Diagnosis of COVID-19 patients by adapting hyper parametertuned deep belief network using hosted cuckoo optimization algorithm. Electromagn. Biol. Med. 2022, 41, 257–271. [Google Scholar] [CrossRef]
- Thakur, S.; Kumar, A. X-ray and CT-scan-based automated detection and classification of covid-19 using convolutional neural networks (CNN). Biomed. Signal Process. Control 2021, 69, 102920. [Google Scholar] [CrossRef]
- Shah, V.; Keniya, R.; Shridharani, A.; Punjabi, M.; Shah, J.; Mehendale, N. Diagnosis of COVID-19 using CT scan images and deep learning techniques. Emerg. Radiol. 2021, 28, 497–505. [Google Scholar] [CrossRef]
- Barstugan, M.; Ozkaya, U.; Ozturk, S. Coronavirus (COVID-19) classification using ct images by machine learning methods. arXiv 2020, arXiv:2003.09424. [Google Scholar]
- Muhammad, G.; Hossain, M.S. COVID-19 and non-COVID-19 classification using multi-layers fusion from lung ultrasound images. Inf. Fusion 2021, 72, 80–88. [Google Scholar] [CrossRef] [PubMed]
- Hussain, E.; Hasan, M.; Rahman, M.A.; Lee, I.; Tamanna, T.; Parvez, M.Z. CoroDet: A deep learning based classification for COVID-19 detection using chest X-ray images. Chaos Solitons Fractals 2021, 142, 110495. [Google Scholar] [CrossRef] [PubMed]
- Ezzat, D.; Hassanien, A.E.; Ella, H.A. An optimized deep learning architecture for the diagnosis of COVID-19 disease based on gravitational search optimization. Appl. Soft Comput. 2021, 98, 106742. [Google Scholar] [CrossRef] [PubMed]
- Abirami, R.N.; Vincent, P.; Rajinikanth, V.; Kadry, S. COVID-19 classification using medical image synthesis by generative adversarial networks. Int. J. Uncertain. Fuzziness Knowl.-Based Syst. 2022, 13, 385–401. [Google Scholar] [CrossRef]
- Abirami, N.; Vincent, D.R.; Kadry, S. P2P-COVID-GAN: Classification and Segmentation of COVID-19 Lung Infections From CT Images Using GAN. Int. J. Data Warehous. Min. (IJDWM) 2021, 17, 101–118. [Google Scholar] [CrossRef]
- Khan, I.U.; Aslam, N. A deep-learning-based framework for automated diagnosis of COVID-19 using X-ray images. Information 2020, 11, 419. [Google Scholar] [CrossRef]
- Ullah, N.; Khan, J.A.; Almakdi, S.; Khan, M.S.; Alshehri, M.; Alboaneen, D.; Raza, A. A novel CovidDetNet deep learning model for effective COVID-19 infection detection using chest radiograph images. Appl. Sci. 2022, 12, 6269. [Google Scholar] [CrossRef]
- Arman, S.E.; Rahman, S.; Deowan, S.A. COVIDXception-Net: A Bayesian optimization-based deep learning approach to diagnose COVID-19 from X-Ray images. SN Comput. Sci. 2022, 3, 1–22. [Google Scholar] [CrossRef]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar]
- Mukti, I.Z.; Biswas, D. Transfer learning based plant diseases detection using ResNet50. In Proceedings of the 2019 4th International Conference on Electrical Information and Communication Technology (EICT), Khulna, Bangladesh, 20–22 December 2019; pp. 1–6. [Google Scholar]
- Tao, J.; Wang, H.; Zhang, X.; Li, X.; Yang, H. An object detection system based on YOLO in traffic scene. In Proceedings of the 2017 6th International Conference on Computer Science and Network Technology (ICCSNT), Dalian, China, 21–22 October 2017; pp. 315–319. [Google Scholar]
- Tio, A.E. Face shape classification using inception v3. arXiv 2019, arXiv:1911.07916. [Google Scholar]
- Dong, N.; Zhao, L.; Wu, C.-H.; Chang, J.-F. Inception v3 based cervical cell classification combined with artificially extracted features. Appl. Soft Comput. 2020, 93, 106311. [Google Scholar] [CrossRef]
- Cho, H.; Kim, Y.; Lee, E.; Choi, D.; Lee, Y.; Rhee, W. Basic enhancement strategies when using Bayesian optimization for hyperparameter tuning of deep neural networks. IEEE Access 2020, 8, 52588–52608. [Google Scholar] [CrossRef]
- Victoria, A.H.; Maragatham, G. Automatic tuning of hyperparameters using Bayesian optimization. Evol. Syst. 2021, 12, 217–223. [Google Scholar] [CrossRef]
- Kwak, N.; Choi, C.-H. Input feature selection for classification problems. IEEE Trans. Neural Netw. 2002, 13, 143–159. [Google Scholar] [CrossRef] [PubMed]
- Cheraghalipour, A.; Hajiaghaei-Keshteli, M.; Paydar, M.M. Tree Growth Algorithm (TGA): A novel approach for solving optimization problems. Eng. Appl. Artif. Intell. 2018, 72, 393–414. [Google Scholar] [CrossRef]
- Amin, J.; Sharif, M.; Gul, N.; Kadry, S.; Chakraborty, C. Quantum machine learning architecture for COVID-19 classification based on synthetic data generation using conditional adversarial neural network. Cogn. Comput. 2022, 14, 1677–1688. [Google Scholar] [CrossRef]
- Umer, M.J.; Amin, J.; Sharif, M.; Anjum, M.A.; Azam, F.; Shah, J.H. An integrated framework for COVID-19 classification based on classical and quantum transfer learning from a chest radiograph. Concurr. Comput. Pract. Exp. 2022, 34, e6434. [Google Scholar] [CrossRef]
- Lu, S.; Zhu, Z.; Gorriz, J.M.; Wang, S.H.; Zhang, Y.D. NAGNN: Classification of COVID-19 based on neighboring aware representation from deep graph neural network. Int. J. Intell. Syst. 2022, 37, 1572–1598. [Google Scholar] [CrossRef]
- Amin, J.; Anjum, M.A.; Sharif, M.; Rehman, A.; Saba, T.; Zahra, R. Microscopic segmentation and classification of COVID-19 infection with ensemble convolutional neural network. Microsc. Res. Tech. 2022, 85, 385–397. [Google Scholar] [CrossRef]
- Wang, S.-H.; Nayak, D.R.; Guttery, D.S.; Zhang, X.; Zhang, Y.-D. COVID-19 classification by CCSHNet with deep fusion using transfer learning and discriminant correlation analysis. Inf. Fusion 2021, 68, 131–148. [Google Scholar] [CrossRef]
- Behera, T.K.; Khan, M.A.; Bakshi, S. Brain MR Image Classification Using Superpixel-Based Deep Transfer Learning. IEEE J. Biomed. Health Inform. 2022; early access. [Google Scholar]
- Devi, S.; Bakshi, S.; Sahoo, M.N. Effect of situational and instrumental distortions on the classification of brain MR images. Biomed. Signal Process. Control 2023, 79, 104177. [Google Scholar] [CrossRef]


















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dataset | Training Images | Augmented Images | Training/Testing Images |
|---|---|---|---|
Chest X-ray (COVID-19 & Pneumonia)
| |||
| 576 1583 4273 | 4000 4000 4273 | 2000/2000 2000/2000 2137/2136 | |
COVID19 Patients Lungs X-ray Images
| |||
| 70 28 | 1000 1000 | 500/500 500/500 | |
COVID-19 Lung CT Scans
| |||
| 7496 944 | 7495 5000 | 3748/3747 2500/2500 | |
COVID-19 Detection
| |||
| 3616 1686 11,767 4265 3500 | 5000 5000 8000 5000 5000 | 2500/2500 2500/2500 4000/4000 2500/2500 2500/2500 | |
COVID-19 Image Dataset
| |||
| 111 70 70 | 1000 1000 1000 | 500/500 500/500 500/500 |
| Hyperparameters | Ranges |
|---|---|
| Learning Rate | [0.0001, 1] |
| Section Depth | [1, 3] |
| Momentum | [0.5, 0.98] |
| L2Regularization | [1e−9, 1e−3] |
| Dropout | [0.0, 0.8] |
| Activation type | RELU, tanh, sigmoid |
| Classifiers | Precision | Sensitivity | F1-Score | FPR | Kappa | MCC | Accuracy | Time (s) |
|---|---|---|---|---|---|---|---|---|
| NNN | 99.54 | 99.53 | 99.53 | 0.002 | 98.94 | 99.29 | 99.5 | 14.949 |
| MNN | 99.60 | 99.59 | 99.60 | 0.002 | 99.08 | 99.39 | 99.6 | 16.316 |
| WNN | 99.59 | 99.58 | 99.58 | 0.002 | 99.05 | 99.37 | 99.6 | 21.932 |
| Bi-layered NN | 98.90 | 98.89 | 98.90 | 0.005 | 97.51 | 98.34 | 98.9 | 19.737 |
| Tri-layered NN | 98.57 | 98.57 | 98.57 | 0.007 | 96.67 | 97.85 | 98.6 | 29.912 |
| Classifiers | Precision | Sensitivity | F1-Score | FPR | Kappa | MCC | Accuracy | Time (s) |
|---|---|---|---|---|---|---|---|---|
| NNN | 99.50 | 99.50 | 99.50 | 0.002 | 98.86 | 99.25 | 99.5 | 9.9754 |
| MNN | 99.55 | 99.55 | 99.55 | 0.002 | 98.97 | 99.32 | 99.5 | 8.6999 |
| WNN | 99.58 | 99.58 | 99.58 | 0.002 | 99.05 | 99.37 | 99.6 | 11.157 |
| Bi-layered NN | 99.21 | 99.21 | 99.21 | 0.004 | 98.20 | 98.81 | 99.2 | 12.029 |
| Tri-layered NN | 99.27 | 99.21 | 99.21 | 0.004 | 98.20 | 98.81 | 99.1 | 12.775 |
| Classifiers | Precision | Sensitivity | F1-Score | FPR | Kappa | MCC | Accuracy | Time (s) |
|---|---|---|---|---|---|---|---|---|
| NNN | 97.05 | 96.94 | 96.81 | 0.03 | 93.80 | 93.96 | 96.9 | 3.2829 |
| MNN | 98.21 | 98.32 | 98.27 | 0.002 | 96.60 | 96.64 | 98.3 | 3.1172 |
| WNN | 98.34 | 98.56 | 98.48 | 0.002 | 97.00 | 97.03 | 98.5 | 2.9841 |
| Bi-layered NN | 96.15 | 96.00 | 95.88 | 0.04 | 92.00 | 92.17 | 96.0 | 2.5945 |
| Tri-layered NN | 95.36 | 95.14 | 94.92 | 0.04 | 90.20 | 90.42 | 95.1 | 2.9175 |
| Classifiers | Precision | Sensitivity | F1-Score | FPR | Kappa | MCC | Accuracy | Time (s) |
|---|---|---|---|---|---|---|---|---|
| NNN | 97.05 | 96.94 | 96.81 | 0.03 | 93.80 | 93.96 | 96.9 | 3.2829 |
| MNN | 98.21 | 98.32 | 98.27 | 0.002 | 96.60 | 96.64 | 98.3 | 3.1172 |
| WNN | 98.34 | 98.56 | 98.48 | 0.002 | 97.00 | 97.03 | 98.5 | 2.9841 |
| Bi-layered NN | 96.15 | 96.00 | 95.88 | 0.04 | 92.00 | 92.17 | 96.0 | 2.5945 |
| Tri-layered NN | 95.36 | 95.14 | 94.92 | 0.04 | 90.20 | 90.42 | 95.1 | 2.9175 |
| Classifiers | Precision | Sensitivity | F1-Score | FPR | Kappa | MCC | Accuracy | Time (s) |
|---|---|---|---|---|---|---|---|---|
| NNN | 98.55 | 99.00 | 99.00 | 0.01 | 97.54 | 97.57 | 98.8 | 31.86 |
| MNN | 98.62 | 99.00 | 99.03 | 0.01 | 97.61 | 97.63 | 98.8 | 30.96 |
| WNN | 98.9 | 99.25 | 99.23 | 0.01 | 98.11 | 98.12 | 99.3 | 41.36 |
| Bi-layered NN | 95.90 | 96.94 | 96.45 | 0.035 | 95.39 | 95.39 | 96.4 | 37.27 |
| Tri-layered NN | 95.65 | 94.55 | 95.75 | 0.04 | 91.66 | 91.63 | 96.0 | 41.88 |
| Classifiers | Precision | Sensitivity | F1-Score | FPR | Kappa | MCC | Accuracy | Time (s) |
|---|---|---|---|---|---|---|---|---|
| NNN | 99.81 | 99.93 | 99.88 | 0.001 | 99.70 | 99.70 | 99.9 | 14.747 |
| MNN | 99.85 | 99.75 | 99.83 | 0.001 | 99.57 | 99.57 | 99.8 | 14.687 |
| WNN | 99.73 | 99.82 | 99.85 | 0.001 | 99.70 | 99.70 | 99.9 | 19.961 |
| Bi-layered NN | 98.62 | 98.15 | 98.95 | 0.005 | 97.40 | 97.42 | 98.4 | 19.054 |
| Tri-layered NN | 96.95 | 97.05 | 97.56 | 0.032 | 93.94 | 93.94 | 97.1 | 37.34 |
| Classifiers | Precision | Sensitivity | F1-Score | FPR | Kappa | MCC | Accuracy | Time |
|---|---|---|---|---|---|---|---|---|
| NNN | 95.72 | 95.68 | 95.69 | 0.009 | 87.95 | 94.75 | 96.1 | 42.351 |
| MNN | 96.94 | 96.88 | 96.90 | 0.006 | 97.30 | 96.23 | 97.2 | 25.885 |
| WNN | 96.66 | 96.66 | 96.65 | 0.007 | 90.67 | 95.93 | 97.0 | 36.578 |
| Bi-layered NN | 92.22 | 92.18 | 92.19 | 0.017 | 78.17 | 90.49 | 93.0 | 89.762 |
| Tri-layered NN | 91.53 | 91.46 | 91.49 | 0.018 | 76.16 | 89.63 | 92.4 | 87.431 |
| Classifiers | Precision | Sensitivity | F1-Score | FPR | Kappa | MCC | Accuracy | Time |
|---|---|---|---|---|---|---|---|---|
| NNN | 99.04 | 99.02 | 99.03 | 0.002 | 97.28 | 98.82 | 99.1 | 15.298 |
| MNN | 99.47 | 99.43 | 99.45 | 0.002 | 98.45 | 99.33 | 99.5 | 12.939 |
| WNN | 99.49 | 99.49 | 99.49 | 0.001 | 98.57 | 99.38 | 99.5 | 20.814 |
| Bi-layered NN | 97.42 | 97.41 | 97.41 | 0.005 | 92.77 | 96.85 | 97.7 | 19.818 |
| Tri-layered NN | 97.79 | 97.79 | 97.79 | 0.004 | 93.84 | 97.31 | 98.0 | 45.819 |
| Classifiers | Precision | Sensitivity | F1-Score | FPR | Kappa | MCC | Accuracy | Time |
|---|---|---|---|---|---|---|---|---|
| NNN | 99.93 | 99.93 | 99.93 | 0.00 | 99.85 | 99.90 | 99.9 | 2.1373 |
| MNN | 100 | 100 | 100 | 0.00 | 100 | 100 | 100 | 2.2438 |
| WNN | 100 | 100 | 100 | 0.00 | 100 | 100 | 100 | 2.8256 |
| Bi-layered NN | 99.93 | 99.93 | 99.93 | 0.00 | 99.85 | 99.90 | 99.9 | 2.1971 |
| Tri-layered NN | 99.93 | 99.93 | 99.93 | 0.00 | 99.85 | 99.90 | 99.9 | 2.4073 |
| Classifiers | Precision | Sensitivity | F1-Score | FPR | Kappa | MCC | Accuracy | Time |
|---|---|---|---|---|---|---|---|---|
| NNN | 100 | 100 | 100 | 0.00 | 100 | 100 | 100 | 2.3249 |
| MNN | 100 | 100 | 100 | 0.00 | 100 | 100 | 100 | 1.97 |
| WNN | 100 | 100 | 100 | 0.00 | 100 | 100 | 100 | 2.0038 |
| Bi-layered NN | 99.93 | 99.93 | 99.93 | 0.00 | 99.85 | 99.90 | 99.9 | 1.4186 |
| Tri-layered NN | 100 | 100 | 100 | 0.00 | 100 | 100 | 100 | 1.5376 |
| Sr. No | Reference | Year | Method | Accuracy (%) |
|---|---|---|---|---|
| 1 | [49] | 2022 | Quantum Machine learning using GAN | 95.0 |
| 2 | [50] | 2022 | Classical and quantum transfer learning for COVID-19 classification | 99.0 |
| 3 | [51] | 2022 | Neighboring aware based deep graph network | 99.2 |
| 4 | [52] | 2021 | Ensemble Convolutional neural network | 97.0 |
| 5 | [53] | 2021 | Deep based fusion transfer learning and DCA | 98.3 |
| Proposed Deep learning, Bayesian optimization, ICCA fusion and best features selection | 99.6 98.5 99.9 99.5 100 | |||
| Datasets and Classifier | CCA | ICCA | Accuracy (%) | Time (s) |
|---|---|---|---|---|
| Chest X-ray (COVID-19 and Pneumonia) | ✓ | 98.4 | 14.215 | |
| ✓ | 99.6 | 16.316 | ||
| COVID-19 Patients Lungs X-ray Images | ✓ | 96.2 | 1.9624 | |
| ✓ | 98.5 | 2.9841 | ||
| COVID-19 Lung CT Scans | ✓ | 98.9 | 37.142 | |
| ✓ | 99.3 | 41.368 | ||
| COVID-19 Detection | ✓ | 96.0 | 22.204 | |
| ✓ | 97.2 | 25.885 | ||
| COVID-19 Image Dataset | ✓ | 99.2 | 2.0426 | |
| ✓ | 100 | 2.2438 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hamza, A.; Khan, M.A.; Alhaisoni, M.; Al Hejaili, A.; Shaban, K.A.; Alsubai, S.; Alasiry, A.; Marzougui, M. D2BOF-COVIDNet: A Framework of Deep Bayesian Optimization and Fusion-Assisted Optimal Deep Features for COVID-19 Classification Using Chest X-ray and MRI Scans. Diagnostics 2023, 13, 101. https://doi.org/10.3390/diagnostics13010101
Hamza A, Khan MA, Alhaisoni M, Al Hejaili A, Shaban KA, Alsubai S, Alasiry A, Marzougui M. D2BOF-COVIDNet: A Framework of Deep Bayesian Optimization and Fusion-Assisted Optimal Deep Features for COVID-19 Classification Using Chest X-ray and MRI Scans. Diagnostics. 2023; 13(1):101. https://doi.org/10.3390/diagnostics13010101
Chicago/Turabian StyleHamza, Ameer, Muhammad Attique Khan, Majed Alhaisoni, Abdullah Al Hejaili, Khalid Adel Shaban, Shtwai Alsubai, Areej Alasiry, and Mehrez Marzougui. 2023. "D2BOF-COVIDNet: A Framework of Deep Bayesian Optimization and Fusion-Assisted Optimal Deep Features for COVID-19 Classification Using Chest X-ray and MRI Scans" Diagnostics 13, no. 1: 101. https://doi.org/10.3390/diagnostics13010101
APA StyleHamza, A., Khan, M. A., Alhaisoni, M., Al Hejaili, A., Shaban, K. A., Alsubai, S., Alasiry, A., & Marzougui, M. (2023). D2BOF-COVIDNet: A Framework of Deep Bayesian Optimization and Fusion-Assisted Optimal Deep Features for COVID-19 Classification Using Chest X-ray and MRI Scans. Diagnostics, 13(1), 101. https://doi.org/10.3390/diagnostics13010101