
In Vivo Evaluation of the Effects of SMILE with Different Amounts of Stromal Ablation on Corneal Biomechanics by Optical Coherence Elastography

 ,
, 
 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. SMILE Procedure
2.3. Pre- and Postoperative Examinations
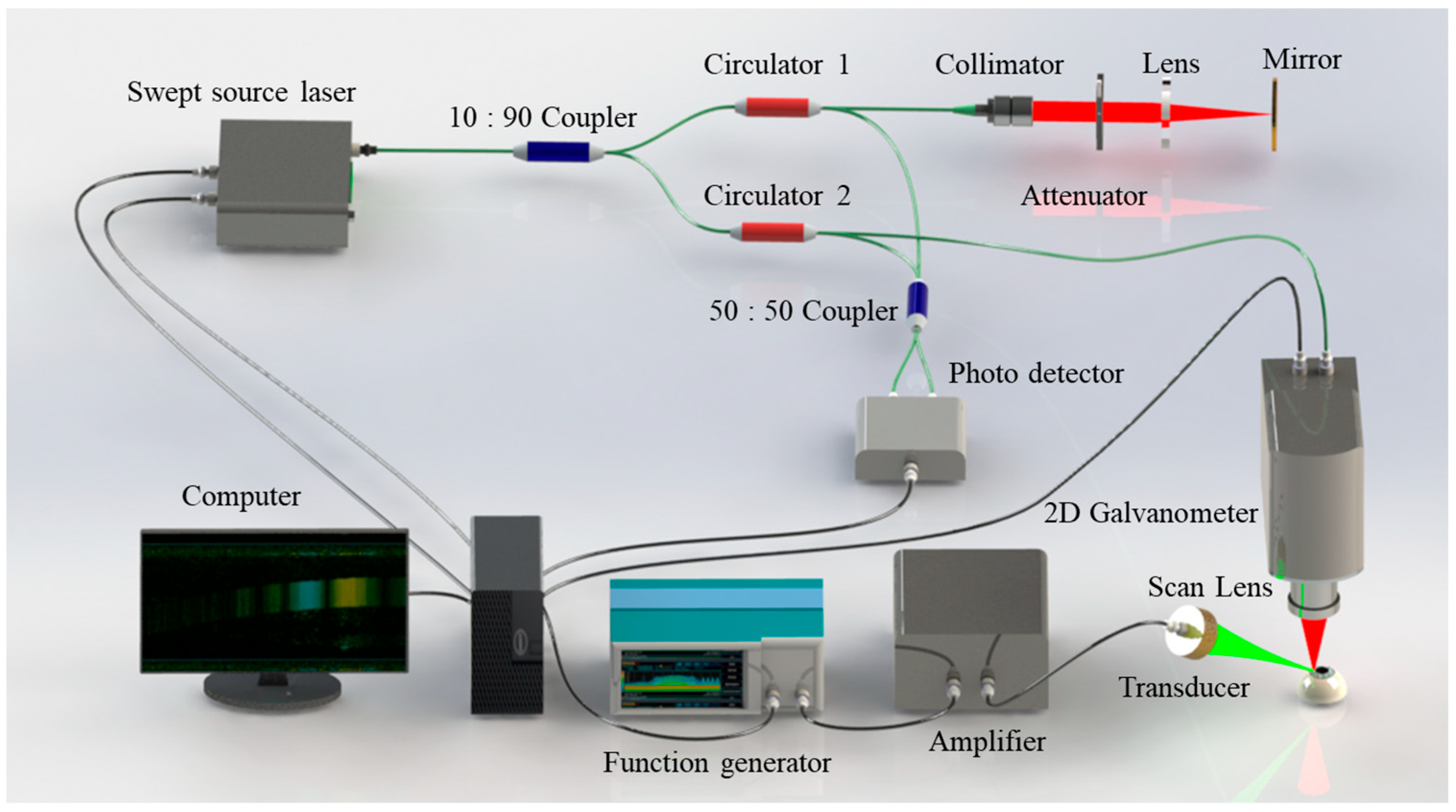
2.4. OCE System Setup
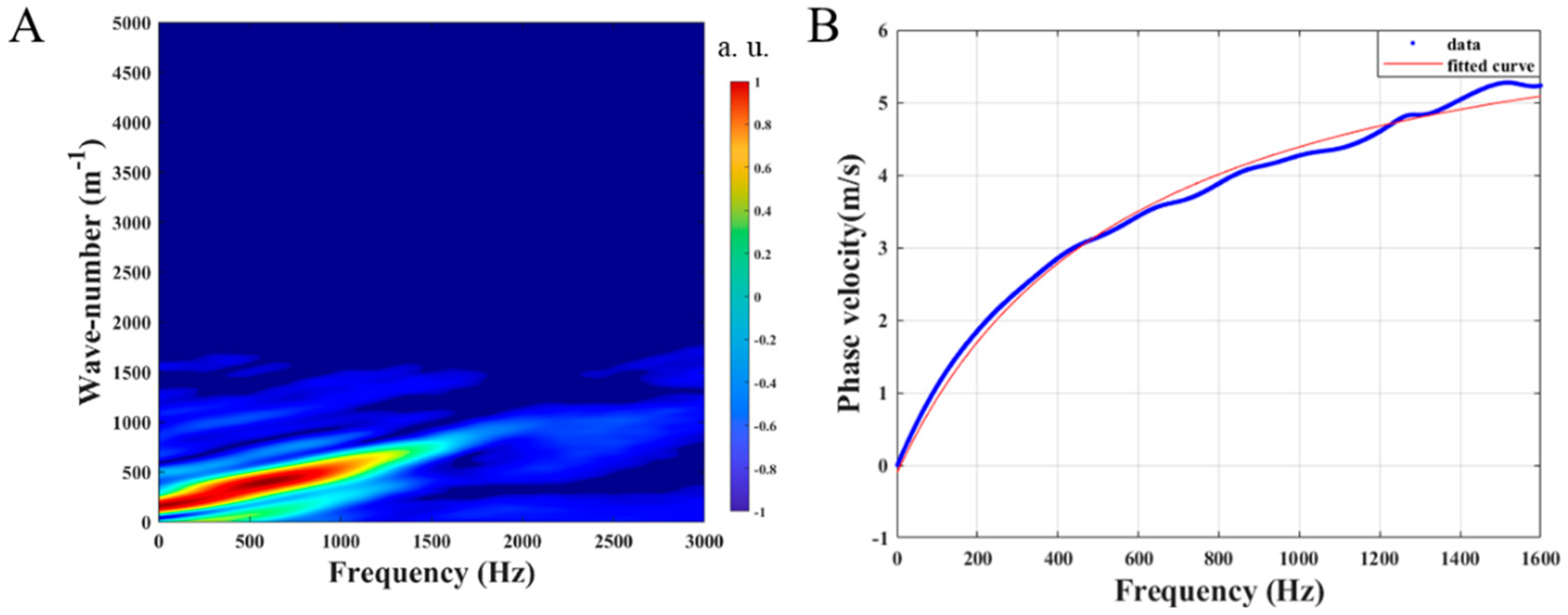
2.5. Antisymmetric Lamb Wave Model for Cornea
2.6. Statistical Analysis
3. Results
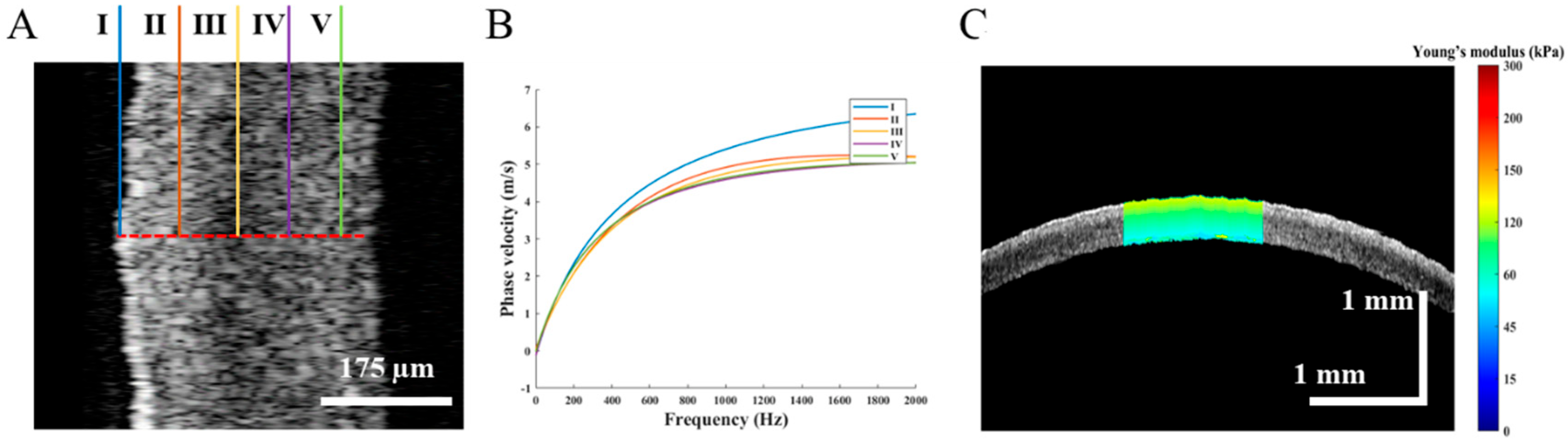
3.1. OCE Examination before the SMILE Surgery
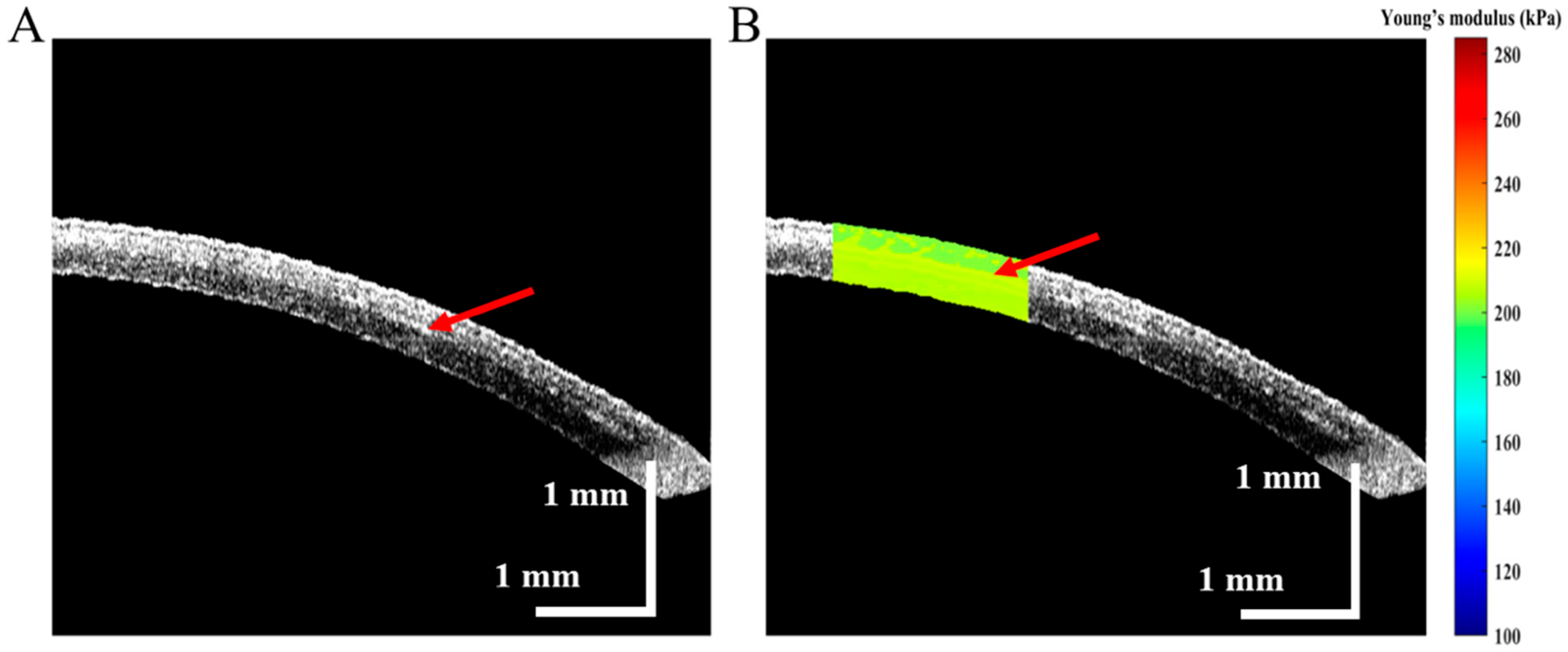
3.2. Post-Operation OCE Examination of SMILE Surgery
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sakimoto, T.; Rosenblatt, M.I.; Azar, D.T. Laser eye surgery for refractive errors. Lancet 2006, 367, 1432–1447. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.-I.; Alió del Barrio, J.L.; Wilkins, M.; Cochener, B.; Ang, M. Refractive surgery. Lancet 2019, 393, 2085–2098. [Google Scholar] [CrossRef] [PubMed]
- Randleman, J.B.; Russell, B.; Ward, M.A.; Thompson, K.P.; Stulting, R.D. Risk factors and prognosis for corneal ectasia after LASIK. Ophthalmology 2003, 110, 267–275. [Google Scholar] [CrossRef] [PubMed]
- Randleman, J.B.; Woodward, M.; Lynn, M.J.; Stulting, R.D. Risk assessment for ectasia after corneal refractive surgery. Ophthalmology 2008, 115, 37–50. [Google Scholar] [CrossRef] [PubMed]
- Reinstein, D.Z.; Archer, T.J.; Randleman, J.B. Mathematical model to compare the relative tensile strength of the cornea after PRK, LASIK, and small incision lenticule extraction. J. Refract. Surg. 2013, 29, 454–460. [Google Scholar] [CrossRef] [Green Version]
- Fernandez, J.; Rodriguez-Vallejo, M.; Martinez, J.; Tauste, A.; Pinero, D.P. Corneal biomechanics after laser refractive surgery: Unmasking differences between techniques. J. Cataract. Refract. Surg. 2018, 44, 390–398. [Google Scholar] [CrossRef] [Green Version]
- Sinha Roy, A.; Dupps, W.J., Jr.; Roberts, C.J. Comparison of biomechanical effects of small-incision lenticule extraction and laser in situ keratomileusis: Finite-element analysis. J. Cataract. Refract. Surg. 2014, 40, 971–980. [Google Scholar] [CrossRef]
- Guo, H.; Hosseini-Moghaddam, S.M.; Hodge, W. Corneal biomechanical properties after SMILE versus FLEX, LASIK, LASEK, or PRK: A systematic review and meta-analysis. BMC Ophthalmol. 2019, 19, 167. [Google Scholar] [CrossRef] [Green Version]
- Pedersen, I.B.; Bak-Nielsen, S.; Vestergaard, A.H.; Ivarsen, A.; Hjortdal, J. Corneal biomechanical properties after LASIK, ReLEx flex, and ReLEx smile by Scheimpflug-based dynamic tonometry. Graefes. Arch. Clin. Exp. Ophthalmol. 2014, 252, 1329–1335. [Google Scholar] [CrossRef]
- Shen, Y.; Chen, Z.; Knorz, M.C.; Li, M.; Zhao, J.; Zhou, X. Comparison of corneal deformation parameters after SMILE, LASEK, and femtosecond laser-assisted LASIK. J. Refract. Surg. 2014, 30, 310–318. [Google Scholar] [CrossRef]
- Wang, D.; Liu, M.; Chen, Y.; Zhang, X.; Xu, Y.; Wang, J.; To, C.H.; Liu, Q. Differences in the corneal biomechanical changes after SMILE and LASIK. J. Refract. Surg. 2014, 30, 702–707. [Google Scholar] [CrossRef] [PubMed]
- Agca, A.; Ozgurhan, E.B.; Demirok, A.; Bozkurt, E.; Celik, U.; Ozkaya, A.; Cankaya, I.; Yilmaz, O.F. Comparison of corneal hysteresis and corneal resistance factor after small incision lenticule extraction and femtosecond laser-assisted LASIK: A prospective fellow eye study. Cont. Lens. Anterior. Eye 2014, 37, 77–80. [Google Scholar] [CrossRef] [PubMed]
- Shetty, R.; Francis, M.; Shroff, R.; Pahuja, N.; Khamar, P.; Girrish, M.; Nuijts, R.; Sinha Roy, A. Corneal Biomechanical Changes and Tissue Remodeling After SMILE and LASIK. Invest. Ophthalmol. Vis. Sci. 2017, 58, 5703–5712. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, R.; Qian, X.; Gong, C.; Zhang, J.; Liu, Y.; Xu, B.; Humayun, M.S.; Zhou, Q. Simultaneous Assessment of the Whole Eye Biomechanics Using Ultrasonic Elastography. IEEE Trans. Biomed. Eng. 2022, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Qian, X.; Li, R.; Lu, G.; Jiang, L.; Kang, H.; Kirk Shung, K.; Humayun, M.S.; Zhou, Q. Ultrasonic elastography to assess biomechanical properties of the optic nerve head and peripapillary sclera of the eye. Ultrasonics 2021, 110, 106263. [Google Scholar] [CrossRef]
- Scarcelli, G.; Yun, S.H. Confocal Brillouin microscopy for three-dimensional mechanical imaging. Nat. Photonics. 2007, 2, 39–43. [Google Scholar] [CrossRef]
- Scarcelli, G.; Pineda, R.; Yun, S.H. Brillouin optical microscopy for corneal biomechanics. Investig. Ophthalmol. Vis. Sci. 2012, 53, 185–190. [Google Scholar] [CrossRef]
- Vaughan, J.; Randall, J. Brillouin scattering, density and elastic properties of the lens and cornea of the eye. Nature 1980, 284, 489–491. [Google Scholar] [CrossRef]
- Shao, P.; Eltony, A.M.; Seiler, T.G.; Tavakol, B.; Pineda, R.; Koller, T.; Seiler, T.; Yun, S.H. Spatially-resolved Brillouin spectroscopy reveals biomechanical abnormalities in mild to advanced keratoconus in vivo. Sci. Rep. 2019, 9, 7467. [Google Scholar] [CrossRef] [Green Version]
- Seiler, T.G.; Shao, P.; Eltony, A.; Seiler, T.; Yun, S.H. Brillouin Spectroscopy of Normal and Keratoconus Corneas. Am. J. Ophthalmol. 2019, 202, 118–125. [Google Scholar] [CrossRef]
- Randleman, J.B.; Su, J.P.; Scarcelli, G. Biomechanical Changes After LASIK Flap Creation Combined With Rapid Cross-Linking Measured With Brillouin Microscopy. J. Refract. Surg. 2017, 33, 408–414. [Google Scholar] [CrossRef] [Green Version]
- Prevedel, R.; Diz-Munoz, A.; Ruocco, G.; Antonacci, G. Brillouin microscopy: An emerging tool for mechanobiology. Nat. Methods 2019, 16, 969–977. [Google Scholar] [CrossRef]
- Liu, P.Y.; Chin, L.K.; Ser, W.; Chen, H.F.; Hsieh, C.M.; Lee, C.H.; Sung, K.B.; Ayi, T.C.; Yap, P.H.; Liedberg, B.; et al. Cell refractive index for cell biology and disease diagnosis: Past, present and future. Lab. Chip. 2016, 16, 634–644. [Google Scholar] [CrossRef]
- Nikolic, M.; Scarcelli, G. Long-term Brillouin imaging of live cells with reduced absorption-mediated damage at 660 nm wavelength. Biomed Opt. Express 2019, 10, 1567–1580. [Google Scholar] [CrossRef]
- Qi, W.; Chen, R.; Chou, L.; Liu, G.; Zhang, J.; Zhou, Q.; Chen, Z. Phase-resolved acoustic radiation force optical coherence elastography. J. Biomed. Opt. 2012, 17, 110505. [Google Scholar] [CrossRef] [Green Version]
- Kennedy, K.M.; McLaughlin, R.A.; Kennedy, B.F.; Tien, A.; Latham, B.; Saunders, C.M.; Sampson, D.D. Needle optical coherence elastography for the measurement of microscale mechanical contrast deep within human breast tissues. J. Biomed. Opt. 2013, 18, 121510. [Google Scholar] [CrossRef]
- Liang, X.; Crecea, V.; Boppart, S.A. Dynamic Optical Coherence Elastography: A Review. J. Innov. Opt. Health Sci. 2010, 3, 221–233. [Google Scholar] [CrossRef] [Green Version]
- Schmitt, J.M. OCT elastography: Imaging microscopic deformation and strain of tissue. Opt. Express 1998, 3, 199–211. [Google Scholar] [CrossRef] [Green Version]
- Liang, X.; Oldenburg, A.L.; Crecea, V.; Chaney, E.J.; Boppart, S.A. Optical micro-scale mapping of dynamic biomechanical tissue properties. Opt. Express 2008, 16, 11052–11065. [Google Scholar] [CrossRef] [Green Version]
- Li, R.; Du, Z.; Qian, X.; Li, Y.; Martinez-Camarillo, J.-C.; Jiang, L.; Humayun, M.S.; Chen, Z.; Zhou, Q. High resolution optical coherence elastography of retina under prosthetic electrode. Quant. Imaging Med. Surg. 2021, 11, 918. [Google Scholar] [CrossRef]
- Du, Z.; Li, R.; Qian, X.; Lu, G.; Li, Y.; He, Y.; Qu, Y.; Jiang, L.; Chen, Z.; Humayun, M.S. Quantitative confocal optical coherence elastography for evaluating biomechanics of optic nerve head using Lamb wave model. Neurophotonics 2019, 6, 041112. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Wang, Y.; Shen, M.; Jin, Z.; Chen, Y.; Zhou, Y.; Qu, J.; Zhu, D. In vivo evaluation of corneal biomechanical properties by optical coherence elastography at different cross-linking irradiances. J. Biomed. Opt. 2019, 24, 105001. [Google Scholar] [CrossRef] [PubMed]
- Singh, M.; Li, J.; Han, Z.; Vantipalli, S.; Liu, C.H.; Wu, C.; Raghunathan, R.; Aglyamov, S.R.; Twa, M.D.; Larin, K.V. Evaluating the Effects of Riboflavin/UV-A and Rose-Bengal/Green Light Cross-Linking of the Rabbit Cornea by Noncontact Optical Coherence Elastography. Investig. Ophthalmol. Vis. Sci. 2016, 57, OCT112–OCT120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Twa, M.D.; Li, J.; Vantipalli, S.; Singh, M.; Aglyamov, S.; Emelianov, S.; Larin, K.V. Spatial characterization of corneal biomechanical properties with optical coherence elastography after UV cross-linking. Biomed. Opt. Express 2014, 5, 1419–1427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, M.; Li, J.; Vantipalli, S.; Han, Z.; Larin, K.V.; Twa, M.D. Optical coherence elastography for evaluating customized riboflavin/UV-A corneal collagen crosslinking. J. Biomed. Opt. 2017, 22, 91504. [Google Scholar] [CrossRef]
- Han, Z.; Li, J.; Singh, M.; Aglyamov, S.R.; Wu, C.; Liu, C.H.; Larin, K.V. Analysis of the effects of curvature and thickness on elastic wave velocity in cornea-like structures by finite element modeling and optical coherence elastography. Appl. Phys. Lett. 2015, 106, 233702. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Han, Z.; Singh, M.; Twa, M.D.; Larin, K.V. Differentiating untreated and cross-linked porcine corneas of the same measured stiffness with optical coherence elastography. J. Biomed. Opt. 2014, 19, 110502. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Zhu, J.; Chen, J.J.; Yu, J.; Jin, Z.; Miao, Y.; Browne, A.W.; Zhou, Q.; Chen, Z. Simultaneously imaging and quantifying in vivo mechanical properties of crystalline lens and cornea using optical coherence elastography with acoustic radiation force excitation. APL Photonics 2019, 4, 106104. [Google Scholar] [CrossRef] [Green Version]
- Lan, G.; Gu, B.; Larin, K.V.; Twa, M.D. Clinical Corneal Optical Coherence Elastography Measurement Precision: Effect of Heartbeat and Respiration. Transl. Vis. Sci. Technol. 2020, 9, 3. [Google Scholar] [CrossRef] [Green Version]
- Zvietcovich, F.; Pongchalee, P.; Meemon, P.; Rolland, J.P.; Parker, K.J. Reverberant 3D optical coherence elastography maps the elasticity of individual corneal layers. Nat. Commun. 2019, 10, 4895. [Google Scholar] [CrossRef]
- De Stefano, V.S.; Ford, M.R.; Seven, I.; Dupps, W.J., Jr. Live human assessment of depth-dependent corneal displacements with swept-source optical coherence elastography. PLoS ONE 2018, 13, e0209480. [Google Scholar] [CrossRef] [Green Version]
- Barnett, S.B.; Duck, F.; Ziskin, M. WFUMB Symposium on Safety of Ultrasound in Medicine: Conclusions and recommendations on biological effects and safety of ultrasound contrast agents, 2006. Ultrasound Med. Biol. 2007, 33, 233–234. [Google Scholar] [CrossRef]
- Shih, C.C.; Qian, X.; Ma, T.; Han, Z.; Huang, C.C.; Zhou, Q.; Shung, K.K. Quantitative Assessment of Thin-Layer Tissue Viscoelastic Properties Using Ultrasonic Micro-Elastography With Lamb Wave Model. IEEE Trans. Med. Imaging 2018, 37, 1887–1898. [Google Scholar] [CrossRef]
- Qian, X.; Ma, T.; Shih, C.C.; Heur, M.; Zhang, J.; Shung, K.K.; Varma, R.; Humayun, M.S.; Zhou, Q. Ultrasonic Microelastography to Assess Biomechanical Properties of the Cornea. IEEE Trans. Biomed. Eng. 2019, 66, 647–655. [Google Scholar] [CrossRef]
- Nenadic, I.Z.; Urban, M.W.; Aristizabal, S.; Mitchell, S.A.; Humphrey, T.C.; Greenleaf, J.F. On Lamb and Rayleigh wave convergence in viscoelastic tissues. Phys. Med. Biol. 2011, 56, 6723–6738. [Google Scholar] [CrossRef]
- Nenadic, I.Z.; Urban, M.W.; Mitchell, S.A.; Greenleaf, J.F. Lamb wave dispersion ultrasound vibrometry (LDUV) method for quantifying mechanical properties of viscoelastic solids. Phys. Med. Biol. 2011, 56, 2245–2264. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.; Larin, K.V. Noncontact depth-resolved micro-scale optical coherence elastography of the cornea. Biomed. Opt. Express 2014, 5, 3807–3821. [Google Scholar] [CrossRef] [Green Version]
- Giri, P.; Azar, D.T. Risk profiles of ectasia after keratorefractive surgery. Curr. Opin. Ophthalmol. 2017, 28, 337–342. [Google Scholar] [CrossRef]
- Moshirfar, M.; Motlagh, M.N.; Murri, M.S.; Momeni-Moghaddam, H.; Ronquillo, Y.C.; Hoopes, P.C. Advances in biomechanical parameters for screening of refractive surgery candidates: A review of the literature, part III. Med. Hypothesis Discov. Innov. Ophthalmol. 2019, 8, 219. [Google Scholar]
- Correia, F.F.; Ramos, I.; Roberts, C.J.; Steinmueller, A.; Krug, M.; Ambrósio Jr, R. Impact of chamber pressure and material properties on the deformation response of corneal models measured by dynamic ultra-high-speed Scheimpflug imaging. Arq. Bras. Oftalmol. 2013, 76, 278–281. [Google Scholar] [CrossRef] [Green Version]
- Roberts, C.J. Concepts and misconceptions in corneal biomechanics. J. Cataract. Refract. Surg. 2014, 40, 862–869. [Google Scholar] [CrossRef] [PubMed]
- Chong, J.; Dupps, W.J., Jr. Corneal biomechanics: Measurement and structural correlations. Exp. Eye Res. 2021, 205, 108508. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Wang, L.; Ji, J.; Yao, W.; Wei, W.; Fan, J.; Joshi, S.; Li, D.; Fan, Y. A mechanical model of the cornea considering the crimping morphology of collagen fibrils. Investig. Ophthalmol. Vis. Sci. 2014, 55, 2739–2746. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elsheikh, A.; Wang, D.; Pye, D. Determination of the modulus of elasticity of the human cornea. J. Refract. Surg. 2007, 23, 808–818. [Google Scholar] [CrossRef] [PubMed]
- Kling, S.; Hafezi, F. Corneal biomechanics—A review. Ophthalmic. Physiol. Opt. 2017, 37, 240–252. [Google Scholar] [CrossRef] [Green Version]
- Last, J.A.; Thomasy, S.M.; Croasdale, C.R.; Russell, P.; Murphy, C.J. Compliance profile of the human cornea as measured by atomic force microscopy. Micron 2012, 43, 1293–1298. [Google Scholar] [CrossRef] [Green Version]
- Ma, J.; Cao, N.J.; Xia, L.K. Efficacy, safety, predictability, aberrations and corneal biomechnical parameters after SMILE and FLEx: Meta-analysis. Int. J. Ophthalmol. 2016, 9, 757–762. [Google Scholar] [CrossRef]
- Sefat, S.M.; Wiltfang, R.; Bechmann, M.; Mayer, W.J.; Kampik, A.; Kook, D. Evaluation of Changes in Human Corneas After Femtosecond Laser-Assisted LASIK and Small-Incision Lenticule Extraction (SMILE) Using Non-Contact Tonometry and Ultra-High-Speed Camera (Corvis ST). Curr. Eye Res. 2016, 41, 917–922. [Google Scholar] [CrossRef]
- Seiler, T.; Koufala, K.; Richter, G. Iatrogenic keratectasia after laser in situ keratomileusis. J. Refract. Surg. 1998, 14, 312–317. [Google Scholar] [CrossRef]
- Santhiago, M.R.; Wilson, S.E.; Hallahan, K.M.; Smadja, D.; Lin, M.; Ambrosio, R., Jr.; Singh, V.; Sinha Roy, A.; Dupps, W.J., Jr. Changes in custom biomechanical variables after femtosecond laser in situ keratomileusis and photorefractive keratectomy for myopia. J. Cataract. Refract. Surg. 2014, 40, 918–928. [Google Scholar] [CrossRef]
- Santhiago, M.R. Percent tissue altered and corneal ectasia. Curr. Opin. Ophthalmol. 2016, 27, 311–315. [Google Scholar] [CrossRef]
- Spiru, B.; Kling, S.; Hafezi, F.; Sekundo, W. Biomechanical Differences Between Femtosecond Lenticule Extraction (FLEx) and Small Incision Lenticule Extraction (SmILE) Tested by 2D-Extensometry in Ex Vivo Porcine Eyes. Investig. Ophthalmol. Vis. Sci. 2017, 58, 2591–2595. [Google Scholar] [CrossRef] [Green Version]
- Roberts, C.J.; Dupps, W.J., Jr. Biomechanics of corneal ectasia and biomechanical treatments. J. Cataract. Refract. Surg. 2014, 40, 991–998. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Data (Mean ± SD) | -3D (n = 6) | -6D (n = 6) | p-Value |
|---|---|---|---|
| CCT (Pre-), µm | 339 ± 3.4 | 345 ± 6.3 | 0.09 > 0.05 |
| CCT (Post-), µm | 278 ± 6.0 | 249 ± 6.9 | 1.6 × 10−5 < 0.05 |
| RSB, µm | 168 ± 6.0 | 139 ± 6.9 | 1.6 × 10−5 < 0.05 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhu, Y.; Zhao, Y.; Zhang, Y.; Yang, H.; Shi, J.; Cai, H.; Zhang, D.; Huang, G.; He, X.; Wu, X. In Vivo Evaluation of the Effects of SMILE with Different Amounts of Stromal Ablation on Corneal Biomechanics by Optical Coherence Elastography. Diagnostics 2023, 13, 30. https://doi.org/10.3390/diagnostics13010030
Zhu Y, Zhao Y, Zhang Y, Yang H, Shi J, Cai H, Zhang D, Huang G, He X, Wu X. In Vivo Evaluation of the Effects of SMILE with Different Amounts of Stromal Ablation on Corneal Biomechanics by Optical Coherence Elastography. Diagnostics. 2023; 13(1):30. https://doi.org/10.3390/diagnostics13010030
Chicago/Turabian StyleZhu, Yirui, Yanzhi Zhao, Yubao Zhang, Hongwei Yang, Jiulin Shi, Hongling Cai, Dong Zhang, Guofu Huang, Xingdao He, and Xiaoshan Wu. 2023. "In Vivo Evaluation of the Effects of SMILE with Different Amounts of Stromal Ablation on Corneal Biomechanics by Optical Coherence Elastography" Diagnostics 13, no. 1: 30. https://doi.org/10.3390/diagnostics13010030
APA StyleZhu, Y., Zhao, Y., Zhang, Y., Yang, H., Shi, J., Cai, H., Zhang, D., Huang, G., He, X., & Wu, X. (2023). In Vivo Evaluation of the Effects of SMILE with Different Amounts of Stromal Ablation on Corneal Biomechanics by Optical Coherence Elastography. Diagnostics, 13(1), 30. https://doi.org/10.3390/diagnostics13010030