




Functional Magnetic Resonance Urography in Children—Tips and Pitfalls


Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Imaging Protocol Evaluation
2.3. Assessment of Image Quality
2.4. Contrast-to-Noise Ratio (CNR) and Signal-to-Noise-Ratio (SNR) Measurements
2.5. Signal Intensity Curves Evaluation
- Separation of the aorta (Figure 3)—the number of time points was found so that the aorta was marked significantly against the background of the organs (the moment of the highest signal intensity in the vessel),
- Separation of the kidneys (Figure 4)—the number of time points was found where contrast is first seen in the calyces,
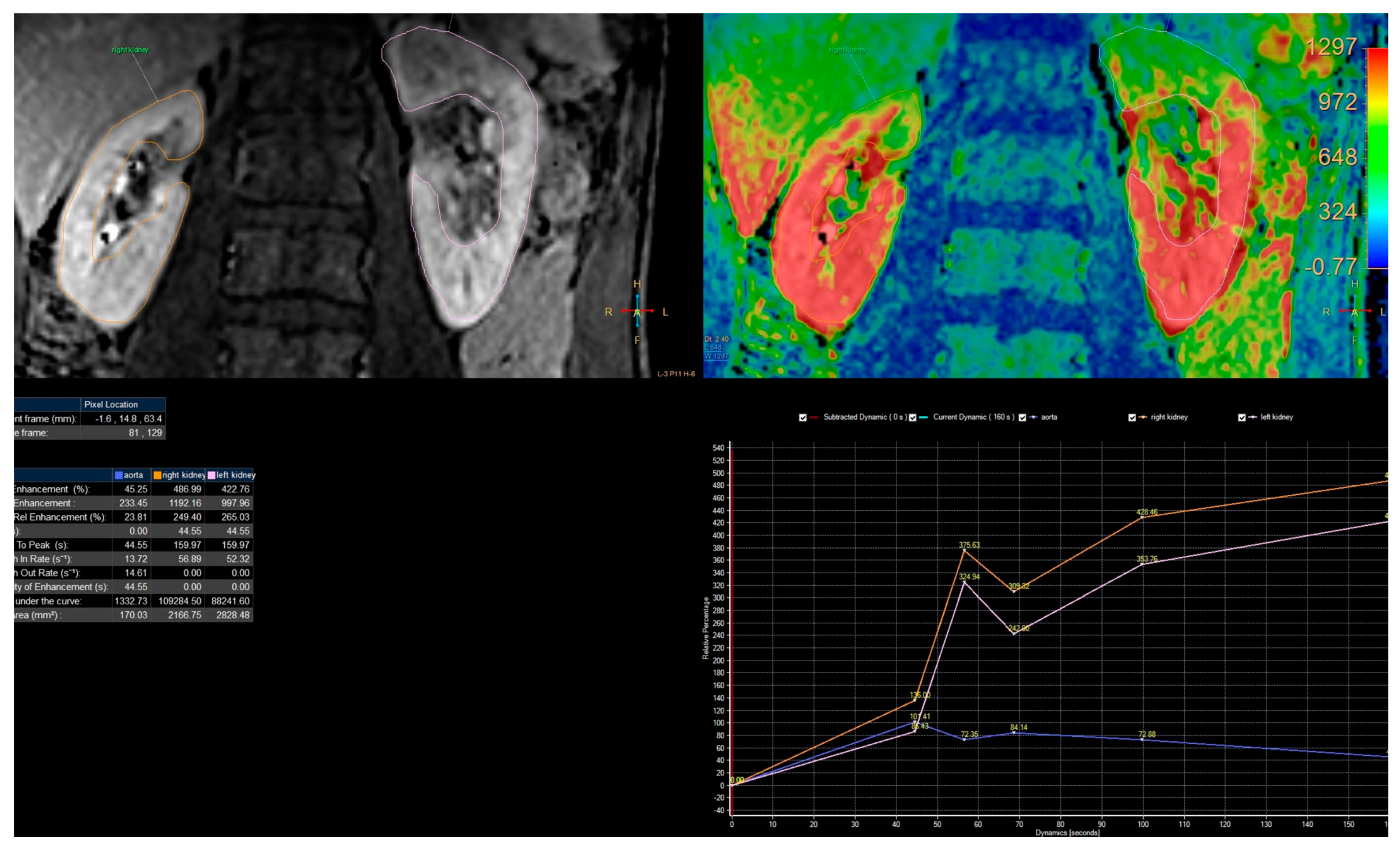
- Biophysical model analysis (Figure 5)—estimation of functional parameters for the aorta and each kidney.
2.6. Statistical Analysis
3. Results
3.1. Evaluation of Imaging Techniques
3.2. Assessment of Image Quality
3.3. Contrast-to-Noise Ratio (CNR) and Signal-to-Noise-Ratio (SNR) Measurements
- Cortex: 2nd and 3rd (Z = −2.429, p = 0.015), 2nd and 4th (Z = −2.626, p = 0.009),
- Medulla: 2nd and 3rd (Z = −2.324, p = 0.020), 2nd and 4th (Z = −2.626, p = 0.009).
3.4. Quality of Enhancement Curves
4. Discussion
- High-field MRI: using a higher magnetic field strength can improve the signal-to-noise ratio and overall image quality.
- Parallel imaging: this technique allows data to be acquired from multiple coils simultaneously, reducing acquisition time and improving spatial resolution.
- Motion correction: motion artifacts can negatively impact image quality, but motion compensation algorithms can compensate for patient movement and improve image quality.
- Compressed sensing: this signal processing technique can reconstruct high-quality images from undersampled data.
- Deep learning: the newest technique uses deep learning methods such as convolutional neural networks to improve image quality by reducing noise and enhancing contrast.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McClennan, B.L. Imaging the Renal Mass: A Historical Review. Radiology 2014, 273, S126–S141. [Google Scholar] [CrossRef] [PubMed]
- Nicolau, C.; Aldecoa, I.; Bunesch, L.; Mallofre, C.; Sebastia, C. The Role of Contrast Agents in the Diagnosis of Renal Diseases. Curr. Probl. Diagn. Radiol. 2015, 44, 346–359. [Google Scholar] [CrossRef] [PubMed]
- Świętoń, D.; Bernard, W.; Grzywińska, M.; Czarniak, P.; Durawa, A.; Kaszubowski, M.; Piskunowicz, M.; Szurowska, E. A Comparability of Renal Length and Volume Measurements in MRI and Ultrasound in Children. Front. Pediatr. 2021, 9, 778079. [Google Scholar] [CrossRef] [PubMed]
- Dickerson, E.C.; Dillman, J.R.; Smith, E.A.; DiPietro, M.A.; Lebowitz, R.L.; Darge, K. Pediatric MR Urography: Indications, Techniques, and Approach to Review. RadioGraphics 2015, 35, 1208–1230. [Google Scholar] [CrossRef]
- Grenier, N.; Merville, P.; Combe, C. Radiologic imaging of the renal parenchyma structure and function. Nat. Rev. Nephrol. 2016, 12, 348–359. [Google Scholar] [CrossRef]
- Sudah, M.; Masarwah, A.; Kainulainen, S.; Pitkänen, M.; Matikka, H.; Dabravolskaite, V.; Aaltomaa, S.; Vanninen, R. Comprehensive MR Urography Protocol: Equally Good Diagnostic Performance and Enhanced Visibility of the Upper Urinary Tract Compared to Triple-Phase CT Urography. PLoS ONE 2016, 11, e0158673. [Google Scholar] [CrossRef]
- Rodigas, J.; Kirsch, H.; John, U.; Seifert, P.; Winkens, T.; Stenzel, M.; Mentzel, H.-J. Static and Functional MR Urography to Assess Congenital Anomalies of the Kidney and Urinary Tract in Infants and Children: Comparison With MAG3 Renal Scintigraphy and Sonography. Am. J. Roentgenol. 2018, 211, 193–203. [Google Scholar] [CrossRef]
- Grattan-Smith, J.D.; Chow, J.; Kurugol, S.; Jones, R.A. Quantitative renal magnetic resonance imaging: Magnetic resonance urography. Pediatr. Radiol. 2022, 52, 228–248. [Google Scholar] [CrossRef]
- Chen, Z.; Huang, H.; Yang, J.; Cai, H.; Yu, Y. The diagnostic value of magnetic resonance urography for detecting ureteric obstruction: A systematic review and meta-analysis. Ann. Med. 2020, 52, 275–282. [Google Scholar] [CrossRef]
- Kurugol, S.; Seager, C.M.; Thaker, H.; Coll-Font, J.; Afacan, O.; Nichols, R.C.; Warfield, S.K.; Lee, R.S.; Chow, J.S. Feed and wrap magnetic resonance urography provides anatomic and functional imaging in infants without anesthesia. J. Pediatr. Urol. 2019, 16, 116–120. [Google Scholar] [CrossRef]
- Taylor, A.; Nally, J.V. Clinical applications of renal scintigraphy. Am. J. Roentgenol. 1995, 164, 31–41. [Google Scholar] [CrossRef] [PubMed]
- Perez-Brayfield, M.R.; Kirsch, A.J.; Jones, R.A.; Grattan-Smith, J.D. A Prospective Study Comparing Ultrasound, Nuclear Scintigraphy and Dynamic Contrast Enhanced Magnetic Resonance Imaging in the Evaluation of Hydronephrosis. J. Urol. 2003, 170, 1330–1334. [Google Scholar] [CrossRef] [PubMed]
- Dillman, J.R.; Trout, A.T.; Smith, E.A. MR urography in children and adolescents: Techniques and clinical applications. Abdom. Imaging 2016, 41, 1007–1019. [Google Scholar] [CrossRef] [PubMed]
- Świȩtoń, D.; Grzywińska, M.; Czarniak, P.; Gołȩbiewski, A.; Durawa, A.; Teodorczyk, J.; Kaszubowski, M.; Piskunowicz, M. The Emerging Role of MR Urography in Imaging Megaureters in Children. Front. Pediatr. 2022, 10, 839128. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.; Dong, B.; Zhang, C.; Tao, X.; Wang, P.; Zhu, L. The histogram analysis of apparent diffusion coefficient in differential diagnosis of parotid tumor. Dentomaxillofacial Radiol. 2020, 49, 20190420. [Google Scholar] [CrossRef] [PubMed]
- Zhu, W.; Ma, M.; Zheng, M.; Hao, H.; Yang, K.; Zhou, L.; Zhang, J.; Wang, H.; Li, X. Cine magnetic resonance urography for postoperative evaluation of reconstructive urinary tract after ileal ureter substitution: Initial experience. Clin. Radiol. 2020, 75, 480.e1–480.e9. [Google Scholar] [CrossRef]
- Riccabona, M. Pediatric MRU?its potential and its role in the diagnostic work-up of upper urinary tract dilatation in infants and children. World J. Urol. 2004, 22, 79–87. [Google Scholar] [CrossRef]
- Grattan-Smith, J.D.; Little, S.B.; Jones, R.A. MR urography evaluation of obstructive uropathy. Pediatr. Radiol. 2007, 38, 49–69. [Google Scholar] [CrossRef]
- Available, N.A.N. European Society of Urogenital Radiology (ESUR). Eur. Radiol. 2000, 10, E1–E26. [Google Scholar] [CrossRef]
- Ramamurthy, N.; Moosavi, B.; McInnes, M.; Flood, T.; Schieda, N. Multiparametric MRI of solid renal masses: Pearls and pitfalls. Clin. Radiol. 2014, 70, 304–316. [Google Scholar] [CrossRef]
- Esmaeili, M.; Esmaeili, M.; Ghane, F.; Alamdaran, A. Comparison Between Diuretic Urography (IVP) and Diuretic Renography for Diagnosis of Ureteropelvic Junction Obstruction in Children. Iran. J. Pediatr. 2016, 26, e4293. [Google Scholar] [CrossRef] [PubMed]
- Jones, R.A.; Schmotzer, B.; Little, S.B.; Grattan-Smith, J.D. MRU post-processing. Pediatr. Radiol. 2007, 38, 18–27. [Google Scholar] [CrossRef] [PubMed]
- Avni, E.; Bali, M.A.; Regnault, M.; Damry, N.; Degroot, F.; Metens, T.; Matos, C. MR urography in children. Eur. J. Radiol. 2002, 43, 154–166. [Google Scholar] [CrossRef] [PubMed]
- Koninklijke Philips, N.V. Encase. 2017. Available online: http://onprc.ohsu.edu/xd/education/schools/school-of-medicine/departments/clinical-departments/diagnostic-radiology/administration/mri-protocols/upload/R5-3-IS-ENCASE.pdf (accessed on 23 August 2019).
- Kanki, A.; Ito, K.; Tamada, T.; Noda, Y.; Yamamoto, A.; Tanimoto, D.; Sato, T.; Higaki, A. Corticomedullary differentiation of the kidney: Evaluation with noncontrast-enhanced steady-state free precession (SSFP) MRI with time-spatial labeling inversion pulse (time-SLIP). J. Magn. Reson. Imaging 2012, 37, 1178–1181. [Google Scholar] [CrossRef]
- Chuck, N.C.; Steidle, G.; Blume, I.; Fischer, M.A.; Nanz, D.; Boss, A. Diffusion Tensor Imaging of the Kidneys: Influence of b-Value and Number of Encoding Directions on Image Quality and Diffusion Tensor Parameters. J. Clin. Imaging Sci. 2013, 3, 53. [Google Scholar] [CrossRef]
- Welvaert, M.; Rosseel, Y. On the Definition of Signal-To-Noise Ratio and Contrast-To-Noise Ratio for fMRI Data. PLoS ONE 2013, 8, e77089. [Google Scholar] [CrossRef]
- Notohamiprodjo, M.; Dietrich, O.; Horger, W.; Horng, A.; Helck, A.D.; Herrmann, K.A.; Reiser, M.F.; Glaser, C. Diffusion Tensor Imaging (DTI) of the Kidney at 3 Tesla–Feasibility, Protocol Evaluation and Comparison to 1.5 Tesla. Investig. Radiol. 2010, 45, 245–254. [Google Scholar] [CrossRef]
- Khrichenko, D.; Darge, K. Functional analysis in MR urography—Made simple. Pediatr. Radiol. 2009, 40, 182–199. [Google Scholar] [CrossRef]
- Serai, S.D.; Hu, H.H.; Ahmad, R.; White, S.; Pednekar, A.; Anupindi, S.A.; Lee, E.Y. Newly Developed Methods for Reducing Motion Artifacts in Pediatric Abdominal MRI: Tips and Pearls. Am. J. Roentgenol. 2020, 214, 1042–1053. [Google Scholar] [CrossRef]
- Brodsky, E.K.; Bultman, E.M.; Johnson, K.M.; Horng, D.E.; Schelman, W.R.; Block, W.F.; Reeder, S.B. High-spatial and high-temporal resolution dynamic contrast-enhanced perfusion imaging of the liver with time-resolved three-dimensional radial MRI. Magn. Reson. Med. 2013, 71, 934–941. [Google Scholar] [CrossRef]
- Deshmane, A.; Gulani, V.; Griswold, M.A.; Seiberlich, N. Parallel MR imaging. J. Magn. Reson. Imaging 2012, 36, 55–72. [Google Scholar] [CrossRef]
- Geerts-Ossevoort, L.; De Weerdt, E.; Duijndam, A.; van IJperen, G.; Peeters, H.; Doneva, M.; Nijenhuis, M.; Huang, A. Compressed SENSE Speed done right. Every time. Philips FieldStrength Mag. 2018, p. 6619. Available online: https://www.usa.philips.com/c-dam/b2bhc/master/landing-pages/compressed-sense-redesign/brochure-compressed-spreads.pdf (accessed on 13 March 2019).
- Bardo, D.M.E.; Rubert, N. Radial sequences and compressed sensing in pediatric body magnetic resonance imaging. Pediatr. Radiol. 2021, 52, 382–390. [Google Scholar] [CrossRef] [PubMed]
- Tustison, N.J.; Avants, B.B.; Cook, P.A.; Zheng, Y.; Egan, A.; Yushkevich, P.A.; Gee, J.C. N4ITK: Improved N3 Bias Correction. IEEE Trans. Med. Imaging 2010, 29, 1310–1320. [Google Scholar] [CrossRef] [PubMed]
- Morin, C.E.; McBee, M.P.; Trout, A.T.; Reddy, P.P.; Dillman, J.R. Use of MR Urography in Pediatric Patients. Curr. Urol. Rep. 2018, 19, 93. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Jung, S.; Jung, K.-J.; Kim, D.-H. Deep Learning in MR Motion Correction: A Brief Review and a New Motion Simulation Tool (view2Dmotion). Investig. Magn. Reson. Imaging 2020, 24, 196–206. [Google Scholar] [CrossRef]
- Pawar, K.; Chen, Z.; Shah, N.J.; Egan, G.F. Suppressing motion artefacts in MRI using an Inception-ResNet network with motion simulation augmentation. NMR Biomed. 2019, 35, e4225. [Google Scholar] [CrossRef]
- Sommer, K.; Saalbach, A.; Brosch, T.; Hall, C.; Cross, N.; Andre, J. Correction of Motion Artifacts Using a Multiscale Fully Convolutional Neural Network. Am. J. Neuroradiol. 2020, 41, 416–423. [Google Scholar] [CrossRef]
- Chavhan, G.B.; Babyn, P.S.; Vasanawala, S.S. Abdominal MR Imaging in Children: Motion Compensation, Sequence Optimization, and Protocol Organization. RadioGraphics 2013, 33, 703–719. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1st Protocol | 2nd Protocol | 3rd Protocol | 4th Protocol | ||||
|---|---|---|---|---|---|---|---|
| 1 | Survey | 1 | Survey | 1 | Survey | 1 | Survey |
| 2 | T1_TFE_IP_Cor_FB | 2 | T1_TFE_IP_Cor_FB | 2 | mDixon_Tra | 2 | T2W_TSE_Tra_HR |
| 3 | T1_TFE_IP_Tra_FB | 3 | VISTA_COR | 3 | VISTA_COR_Sense | 3 | VISTA_COR_Sense |
| 4 | BTFE_SPIR_COR_FB | 4 | BTFE_SPIR_SAG_FB | 4 | DWI_5b_Tra_navi | 4 1 | BTFE_SPIR_SAG_FB |
| 5 | T2_TSE_TRA_FB | 5 | T2_TSE_HR_TRA_FB | 5 | T2W_TSE_Tra_HR | 5 | mDixon_Tra |
| 6 | T2W_SPAIR_TRA_FB | 6 | STIR_Tra_FB | 6 | T2_SPAIR_TRA | 6 | DWI_5b_Tra_navi |
| 7 | VISTA_COR | 7 | DWI_5b_Tra_navi | 7 | BTFE_SPIR_SAG_FB | 7 | STIR_Tra_FB |
| 8 | sMRCP_3D_HR_COR | 8 | mDIXON_ TRA_FB | 8 | THRIVE_COR_3D | 8 2 | sMRCP_3D_HR_COR |
| 9 | e-THRIVE_COR_FB | 9 | THRIVE_COR_FB | 9 | sT1W_FFE_IP | 9 | e-THRIVE_COR_FB |
| 10 | T1_TFE_IP_COR_FB | 10 | T1_TFE_IP_COR_FB | 10 | mDixon_Tra | ||
| Parameters | 1st Protocol | 2nd Protocol | 3rd Protocol | 4th Protocol |
|---|---|---|---|---|
| Slice thickness/gap (mm) | 5 | 3 | 3 | 4 |
| Suppress fat | SPAIR | SPIR | SPIR | SPAIR |
| Flip angle | 10 | 25 | 25 | 10 |
| Number of averages | 3 | 1 | 1 | 1 |
| TE/TR (ms) | Default | Default | default | default |
| Matrix | ≈214/214 | ≈214/214 | ≈232/232 | ≈384/384 |
| Time (s) per dynamic | ≈10 | ≈12 | ≈8 | ≈8 |
| Breath hold | Free breath | Free breath | Free breath | Free breath |
| Sense | - | + | + | + |
| ENCASE | - | - | - | + |
| Number of dynamics | 10 | 25 | ≈25–30 | ≈40–50 |
| Number of dynamics without contrast | 1 | 1 | 5–7 | >7 |
| Delay between dynamics | 30 s | 30 s | 30 s | For the beginning, dynamics were acquired one by one, without delay. After a few minutes—30 s |
| Plane | Coronal with the angle of the oblique-coronal plane in long axis kidney | Coronal with the angle of the oblique-coronal plane in long axis kidney | Coronal with the angle of the oblique-coronal plane in long axis kidney | Coronal with a maximum of 5 degrees |
| Number of Protocol | Visual Assessment with a 4-Point Scale | |||||
|---|---|---|---|---|---|---|
| N | Minimum | Maximum | Mean | Median | Standard Error | |
| 1st protocol | 20 | 2.00 | 4.00 | 2.85 | 3 | 0.18 |
| 2nd protocol | 32 | 1.00 | 4.00 | 2.78 | 3 | 0.13 |
| 3rd protocol | 22 | 1.00 | 4.00 | 3.27 | 3 | 0.19 |
| 4th protocol | 17 | 3.00 | 4.00 | 3.77 | 4 | 0.11 |
| Number of Protocol | Contrast to Noise Ratio (CNR) | |||||
|---|---|---|---|---|---|---|
| N | Minimum | Maximum | Mean | Median | Standard Error | |
| 1st protocol | 20 | 1.33 | 17.13 | 7.07 | 6,28 | 0.91 |
| 2nd protocol | 32 | 0.43 | 15.73 | 6.15 | 5.29 | 0.72 |
| 3rd protocol | 22 | 1.83 | 24.82 | 8.84 | 6.34 | 1.43 |
| 4th protocol | 17 | 0.35 | 17.44 | 8.59 | 8.16 | 1.04 |
| Number of Protocol | Signal to Noise Ratio (SNR) in Medulla | Signal to Noise Ratio (SNR) in Cortex | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| N | Minimum | Maximum | Mean | Median | Standard Error | Minimum | Maximum | Mean | Median | Standard Error | |
| 1st protocol | 20 | 5.18 | 86.11 | 23.867 | 17.89 | 4.39 | 6.51 | 90.68 | 30.98 | 24.10 | 4.24 |
| 2nd protocol | 32 | 8.09 | 34.75 | 16.22 | 12.09 | 1.31 | 11.82 | 45.75 | 22.38 | 19.55 | 1.61 |
| 3rd protocol | 22 | 7.20 | 94.76 | 26.37 | 18.62 | 4.24 | 12.48 | 118.94 | 35.22 | 26.80 | 5.07 |
| 4th protocol | 17 | 5.95 | 39.81 | 23.14 | 22.52 | 2.38 | 13.12 | 49.99 | 31.74 | 33.21 | 2.91 |
| TTP Standard Deviation | ||
|---|---|---|
| IntelliSpace Portal | ChopfMRU | |
| 1st protocol | 15.241 | 14.560 |
| 2nd protocol | 10.550 | 13.768 |
| 3rd protocol | 9.214 | 11.520 |
| 4th protocol | 5.506 | 5.599 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grzywińska, M.; Świętoń, D.; Sabisz, A.; Piskunowicz, M. Functional Magnetic Resonance Urography in Children—Tips and Pitfalls. Diagnostics 2023, 13, 1786. https://doi.org/10.3390/diagnostics13101786
Grzywińska M, Świętoń D, Sabisz A, Piskunowicz M. Functional Magnetic Resonance Urography in Children—Tips and Pitfalls. Diagnostics. 2023; 13(10):1786. https://doi.org/10.3390/diagnostics13101786
Chicago/Turabian StyleGrzywińska, Małgorzata, Dominik Świętoń, Agnieszka Sabisz, and Maciej Piskunowicz. 2023. "Functional Magnetic Resonance Urography in Children—Tips and Pitfalls" Diagnostics 13, no. 10: 1786. https://doi.org/10.3390/diagnostics13101786
APA StyleGrzywińska, M., Świętoń, D., Sabisz, A., & Piskunowicz, M. (2023). Functional Magnetic Resonance Urography in Children—Tips and Pitfalls. Diagnostics, 13(10), 1786. https://doi.org/10.3390/diagnostics13101786