

Risk Factors and Interpretation of Inconclusive Endoscopic Ultrasound-Guided Fine Needle Aspiration Cytology in the Diagnosis of Solid Pancreatic Lesions
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
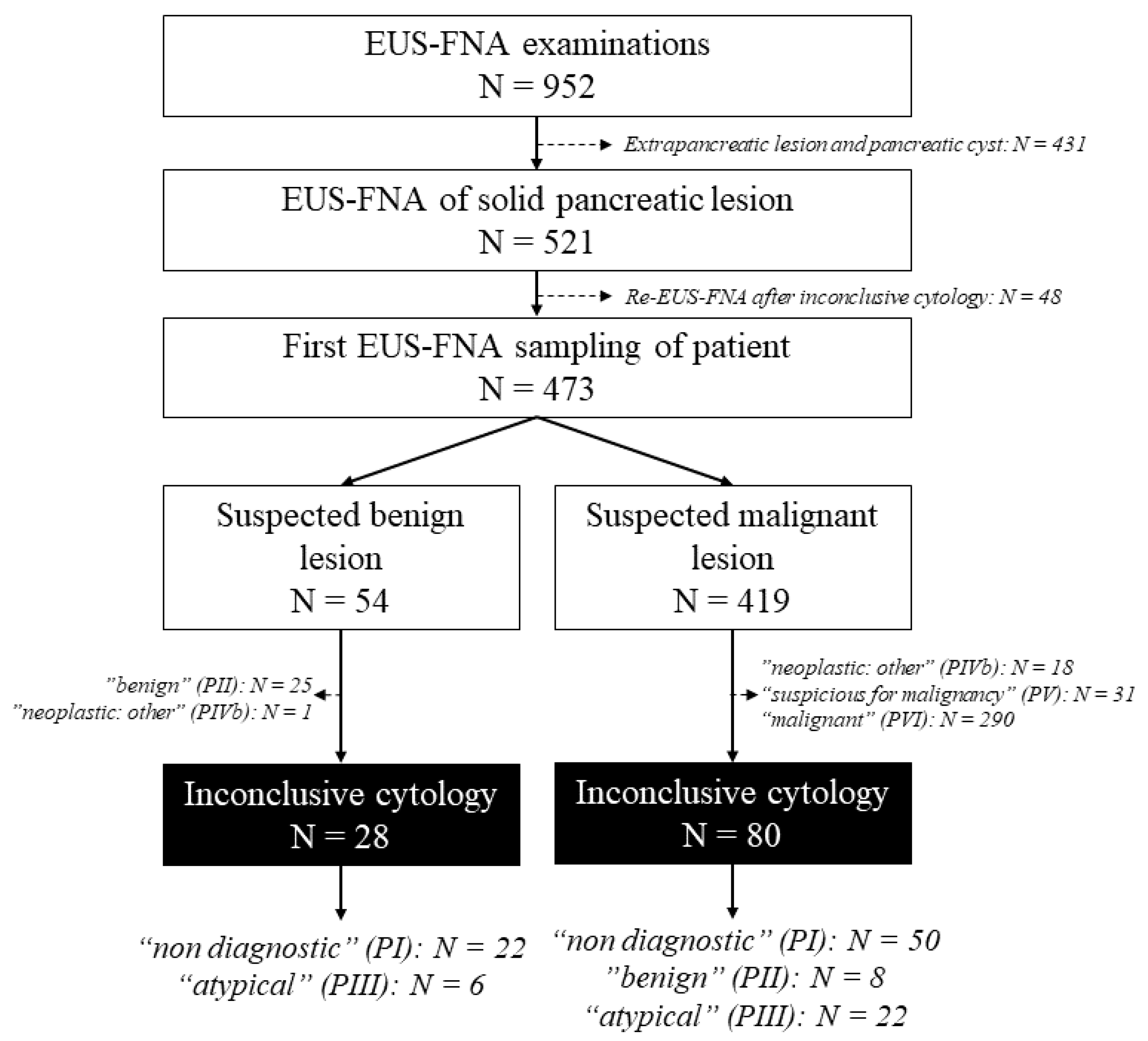
2.1. Patient Enrollment and Determination of Subgroups
2.2. Objectives of the Study and Clinical Validation of Cytological Findings
- (1)
- To determine the frequency and predictors of inconclusive cytological finding of the first pancreatic EUS-FNA sampling;
- (2)
- To determine the outcome of disease in patients with inconclusive cytology results.
2.3. EUS-FNA Procedure and Pathological Evaluation
2.4. Ethics Approval and Consent to Participate
2.5. Statistical Analysis
3. Results
3.1. Characteristics of Patients and EUS-FNA Samplings
3.2. Frequency and Predictors of Inconclusive Cytological Findings
3.3. Outcome Patients with Inconclusive Cytology Results
3.4. Clinical Factors Influencing the ROM
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dumonceau, J.M.; Deprez, P.; Jenssen, C.; Iglesias-Garcia, J.; Larghi, A.; Vanbiervliet, G.; Aithal, G.P.; Arcidiacono, P.G.; Bastos, P.; Carrara, S.; et al. Indications, results, and clinical impact of endoscopic ultrasound (EUS)-guided sampling in gastroenterology: European Society of Gastrointestinal Endoscopy (ESGE) Clinical Guideline—Updated January 2017. Endoscopy 2017, 49, 695–714. [Google Scholar] [CrossRef] [PubMed]
- Pouw, R.E.; Barret, M.; Biermann, K.; Bisschops, R.; Czakó, L.; Gecse, K.B.; de Hertogh, G.; Hucl, T.; Iacucci, M.; Jansen, M.; et al. Endoscopic tissue sampling—Part 1: Upper gastrointestinal and hepatopancreatobiliary tracts. European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy 2021, 53, 1174–1188. [Google Scholar] [CrossRef] [PubMed]
- Puli, S.R.; Bechtold, M.L.; Buxbaum, J.L.; Eloubeidi, M.A. How good is endoscopic ultrasound-guided fine-needle aspiration in diagnosing the correct etiology for a solid pancreatic mass? A meta-analysis and systematic review. Pancreas 2013, 42, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Mohan, B.P.; Madhu, D.; Reddy, N.; Charan, B.S.; Khan, S.R.; Garg, G.; Kassab, L.L.; Muthusamy, A.K.; Singh, A.; Chandan, S.; et al. Diagnostic accuracy of EUS-guided fine-needle biopsy sampling by macroscopic on-site evaluation: A systematic review and meta-analysis. Gastrointest. Endosc. 2022, 96, 909–917.e11. [Google Scholar] [CrossRef]
- Li, D.F.; Wang, J.-Y.; Yang, M.-F.; Xiong, F.; Zhang, D.-G.; Xu, Z.-L.; Luo, M.-H.; Jing, Z.-D.; Wang, K.-X.; Wang, L.-S.; et al. Factors associated with diagnostic accuracy, technical success and adverse events of endoscopic ultrasound-guided fine-needle biopsy: A systematic review and meta-analysis. J. Gastroenterol. Hepatol. 2020, 35, 1264–1276. [Google Scholar] [CrossRef]
- Tian, G.; Bao, H.; Li, J.; Jiang, T. Systematic Review and Meta-Analysis of Diagnostic Accuracy of Endoscopic Ultrasound (EUS)-Guided Fine-Needle Aspiration (FNA) Using 22-gauge and 25-gauge Needles for Pancreatic Masses. Med. Sci. Monit. 2018, 24, 8333–8341. [Google Scholar] [CrossRef]
- Tempero, M.A.; Malafa, M.P.; Al-Hawary, M.; Behrman, S.W.; Benson, A.B.; Cardin, D.B.; Chiorean, E.G.; Chung, V.; Czito, B.; Chiaro, M.D.; et al. Pancreatic Adenocarcinoma, Version 2.2021, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Canc. Netw. 2021, 19, 439–457. [Google Scholar] [CrossRef]
- Pitman, M.B.; Layfield, L.J. The Papanicolaou Society of Cytopathology System for Reporting Pancreaticobiliary Cytology; Springer International Publishing: Cham, Switzerland, 2015. [Google Scholar]
- Hoda, R.S.; Finer, E.B.; Arpin, R.N.; Rosenbaum, M.; Pitman, M.B. Risk of malignancy in the categories of the Papanicolaou Society of Cytopathology system for reporting pancreaticobiliary cytology. J. Am. Soc. Cytopathol. 2019, 8, 120–127. [Google Scholar] [CrossRef]
- Sung, S.; del Portillo, A.; Gonda, T.A.; Kluger, M.D.; Tiscornia-Wasserman, P.G. Update on risk stratification in the Papanicolaou Society of Cytopathology System for Reporting Pancreaticobiliary Cytology categories: 3-Year, prospective, single-institution experience. Cancer Cytopathol. 2020, 128, 29–35. [Google Scholar] [CrossRef]
- Hébert-Magee, S.; Bae, S.; Varadarajulu, S.; Ramesh, J.; Frost, A.R.; Eloubeidi, M.A.; Eltoum, I.A. The presence of a cytopathologist increases the diagnostic accuracy of endoscopic ultrasound-guided fine needle aspiration cytology for pancreatic adenocarcinoma: A meta-analysis. Cytopathology 2013, 24, 159–171. [Google Scholar] [CrossRef]
- Hewitt, M.J.; McPhail, M.J.; Possamai, L.; Dhar, A.; Vlavianos, P.; Monahan, K.J. EUS-guided FNA for diagnosis of solid pancreatic neoplasms: A meta-analysis. Gastrointest. Endosc. 2012, 75, 319–331. [Google Scholar] [CrossRef]
- Abdallah, M.A.; Ahmed, K.; Taha, W.; Musa, A.; Reardon, E.E.; Abdalla, A.O.; Trikudanathan, G. Endoscopic Ultrasound Guided Fine-Needle Aspiration for Solid Lesions in Chronic Pancreatitis: A Systematic Review and Meta-Analysis. Dig. Dis. Sci. 2022, 67, 2552–2561. [Google Scholar] [CrossRef]
- Lisotti, A.; Frazzoni, L.; Fuccio, L.; Serrani, M.; Cominardi, A.; Bazzoli, F.; Fusaroli, P. Repeat EUS-FNA of pancreatic masses after nondiagnostic or inconclusive results: Systematic review and meta-analysis. Gastrointest. Endosc. 2020, 91, 1234–1241.e4. [Google Scholar] [CrossRef]
- Guvendir, I.; Zemheri, I.E.; Ozdil, K. Impact of rapid on-site evaluation on diagnostic accuracy of EUS-guided fine-needle aspiration of solid pancreatic lesions: Experience from a single center. BMC Gastroenterol. 2022, 22, 264. [Google Scholar] [CrossRef] [PubMed]
- Sbeit, W.; Khoury, T. Endoscopic ultrasound fine needle biopsy was not more cost-effective than fine-needle aspiration with rapid on-site evaluation in gastrointestinal lesions diagnosis. Diagn. Cytopathol. 2021, 49, 944–947. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.I.; Chatterjee, A.; Berger, R.; Kanber, Y.; Wyse, J.; Lam, E.; Gan, I.; Auger, M.; Kenshil, S.; Telfordet, J.; et al. Endoscopic ultrasound (EUS)-guided fine needle biopsy alone vs. EUS-guided fine needle aspiration with rapid onsite evaluation in pancreatic lesions: A multicenter randomized trial. Endoscopy 2022, 54, 4–12. [Google Scholar] [CrossRef] [PubMed]
- Wani, S.; Mullady, D.; Early, D.S.; Rastogi, A.; Collins, B.; Wang, J.F.; Marshall, C.; Sams, S.B.; Yen, R.; Rizeq, M.; et al. The clinical impact of immediate on-site cytopathology evaluation during endoscopic ultrasound-guided fine needle aspiration of pancreatic masses: A prospective multicenter randomized controlled trial. Am. J. Gastroenterol. 2015, 110, 1429–1439. [Google Scholar] [CrossRef] [PubMed]
- Moura, D.T.H.; McCarty, T.R.; Jirapinyo, P.; Ribeiro, I.B.; Farias, G.F.A.; Madruga-Neto, A.C.; Ryou, M.; Thompson, C.C. Endoscopic ultrasound fine needle aspiration vs fine needle biopsy in solid lesions: A multi-center analysis. World J. Clin. Cases 2021, 9, 10507. [Google Scholar] [CrossRef]
- Nebel, J.A.; Soldan, M.; Dumonceau, J.M.; de Souza Carvalho, C.E.; Chagas, V.L.A.; de Assis, P.G.; Lapa E Silva, J.R.; Rezende, G.F.D.M. Rapid On-Site Evaluation by Endosonographer of Endoscopic Ultrasound Fine-Needle Aspiration of Solid Pancreatic Lesions: A Randomized Controlled Trial. Pancreas 2021, 50, 815–821. [Google Scholar] [CrossRef]
- Milluzzo, S.M.; Olivari, N.; Rossi, G.; Bianchi, D.; Liserre, B.; Graffeo, M.; Lovera, M.; Correale, L.; Hassan, C.; Spada, C. Rapid on-site evaluation improves the sensitivity of endoscopic ultrasound-guided fine needle aspiration (EUS-FNA) for solid pancreatic lesions irrespective of technique: A single-centre experience. Cytopathology 2023, 34, 318–324. [Google Scholar] [CrossRef]
- Moura, D.T.H.; McCarty, T.R.; Jirapinyo, P.; Ribeiro, I.B.; Hathorn, K.E.; Madruga-Neto, A.C.; Lee, L.S.; Thompson, C.C. Evaluation of endoscopic ultrasound fine-needle aspiration versus fine-needle biopsy and impact of rapid on-site evaluation for pancreatic masses. Endosc. Int. Open 2020, 8, E738–E747. [Google Scholar] [CrossRef]
- Zhang, S.; Ni, M.; Wang, P.; Zheng, J.; Sun, Q.; Xu, G.; Peng, C.; Shen, S.; Zhang, W.; Huang, S.; et al. Diagnostic value of endoscopic ultrasound-guided fine needle aspiration with rapid on-site evaluation performed by endoscopists in solid pancreatic lesions: A prospective, randomized controlled trial. J. Gastroenterol. Hepatol. 2022, 37, 1975–1982. [Google Scholar] [CrossRef] [PubMed]
- Guedes, H.G.; Hourneaux de Moura, D.T.; Duarte, R.B.; Cordero, M.A.C.; Santos, M.E.L.D.; Cheng, S.; Matuguma, S.E.; Chaves, D.M.; Bernardo, W.M.; de Moura, E.G.H. A comparison of the efficiency of 22G versus 25G needles in EUS-FNA for solid pancreatic mass assessment: A systematic review and meta-analysis. Clinics 2018, 73, e261. [Google Scholar] [CrossRef]
- Itonaga, M.; Yasukawa, S.; Fukutake, N.; Ogura, T.; Asada, M.; Shimokawa, T.; Inatomi, O.; Nakai, Y.; Shiomi, H.; Nebiki, H.; et al. Comparison of 22-gauge standard and Franseen needles in EUS-guided tissue acquisition for diagnosing solid pancreatic lesions: A multicenter randomized controlled trial. Gastrointest. Endosc. 2022, 96, 57–66.e2. [Google Scholar] [CrossRef]
- Oppong, K.W.; Bekkali, N.L.H.; Leeds, J.S.; Johnson, S.J.; Nayar, M.K.; Darné, A.; Egan, M.; Bassett, P.; Haugk, B. Fork-tip needle biopsy versus fine-needle aspiration in endoscopic ultrasound-guided sampling of solid pancreatic masses: A randomized crossover study. Endoscopy 2020, 52, 454–461. [Google Scholar] [CrossRef]
- Bang, J.Y.; Krall, K.; Jhala, N.; Singh, C.; Tejani, M.; Arnoletti, J.P.; Navaneethan, U.; Hawes, R.; Varadarajulu, S. Comparing Needles and Methods of Endoscopic Ultrasound-Guided Fine-Needle Biopsy to Optimize Specimen Quality and Diagnostic Accuracy for Patients with Pancreatic Masses in a Randomized Trial. Clin. Gastroenterol. Hepatol. 2021, 19, 825–835.e7. [Google Scholar] [CrossRef]
- van Riet, P.A.; Erler, N.S.; Bruno, M.J.; Cahen, D.L. Comparison of fine-needle aspiration and fine-needle biopsy devices for endoscopic ultrasound-guided sampling of solid lesions: A systemic review and meta-analysis. Endoscopy 2021, 53, 411–423. [Google Scholar] [CrossRef] [PubMed]
- Bang, J.Y.; Magee, S.H.; Ramesh, J.; Trevino, J.M.; Varadarajulu, S. Randomized trial comparing fanning with standard technique for endoscopic ultrasound-guided fine-needle aspiration of solid pancreatic mass lesions. Endoscopy 2013, 45, 445–450. [Google Scholar] [CrossRef] [PubMed]
- Polkowski, M.; Jenssen, C.; Kaye, P.; Carrara, S.; Deprez, P.; Gines, A.; Fernández-Esparrach, G.; Eisendrath, P.; Aithal, G.P.; Arcidiacono, P.; et al. Technical aspects of endoscopic ultrasound (EUS)-guided sampling in gastroenterology: European Society of Gastrointestinal Endoscopy (ESGE) Technical Guideline—March 2017. Endoscopy 2017, 49, 989–1006. [Google Scholar] [CrossRef]
- Crinò, S.F.; Bellocchi, M.C.C.; Di Mitriet, R.; Inzani, F.; Rimbaș, M.; Lisotti, A.; Manfredi, G.; Teoh, A.Y.B.; Mangiavillano, B.; Sendino, O.; et al. Wet-suction versus slow-pull technique for endoscopic ultrasound-guided fine-needle biopsy: A multicenter, randomized, crossover trial. Endoscopy 2023, 55, 225–234. [Google Scholar] [CrossRef]
- Bor, R.; Vasas, B.; Fábián, A.; Bálint, A.; Farkas, K.; Milassin, Á.; Czakó, L.; Rutka, M.; Molnár, T.; Szűcs, M.; et al. Prospective comparison of slow-pull and standard suction techniques of endoscopic ultrasound-guided fine needle aspiration in the diagnosis of solid pancreatic cancer. BMC Gastroenterol. 2019, 19, 6. [Google Scholar] [CrossRef]
- Nakai, Y.; Hamada, T.; Hakuta, R.; Sato, T.; Ishigaki, K.; Saito, K.; Saito, T.; Takahara, N.; Mizuno, S.; Kogure, H.; et al. A Meta-analysis of Slow Pull versus Suction for Endoscopic Ultrasound-Guided Tissue Acquisition. Gut Liver 2021, 15, 625–633. [Google Scholar] [CrossRef] [PubMed]
- Facciorusso, A.; Crinò, S.F.; Ramai, D.; Madhu, D.; Fugazza, A.; Carrara, S.; Spadaccini, M.; Mangiavillano, B.; Gkolfakis, P.; Mohan, B.P.; et al. Comparative diagnostic performance of different techniques for EUS-guided fine-needle biopsy sampling of solid pancreatic masses: A network meta-analysis. Gastrointest. Endosc. 2023, 97, 839–848.e5. [Google Scholar] [CrossRef] [PubMed]
- Ge, P.S.; Wani, S.; Watson, R.R.; Sedarat, A.; Kim, S.; Marshall, C.; Wilson, R.H.; Makker, J.; Mohamadnejad, M.; Komanduri, S.; et al. Per-Pass Performance Characteristics of Endoscopic Ultrasound-Guided Fine-Needle Aspiration of Malignant Solid Pancreatic Masses in a Large Multicenter Cohort. Pancreas 2018, 47, 296–301. [Google Scholar] [CrossRef]
- Wani, S.; Muthusamy, V.R.; McGrath, C.M.; Sepulveda, A.R.; Das, A.; Messersmith, W.; Kochman, M.L.; Shah, J. AGA White Paper: Optimizing Endoscopic Ultrasound-Guided Tissue Acquisition and Future Directions. Clin. Gastroenterol. Hepatol. 2018, 16, 318–327. [Google Scholar] [CrossRef] [PubMed]
- Mohamadnejad, M.; Mullady, D.; Early, D.S.; Collins, B.; Marshall, C.; Sams, S.; Yen, R.; Rizeq, M.; Romanas, M.; Nawaz, S.; et al. Increasing Number of Passes Beyond 4 Does Not Increase Sensitivity of Detection of Pancreatic Malignancy by Endoscopic Ultrasound-Guided Fine-Needle Aspiration. Clin. Gastroenterol. Hepatol. 2017, 15, 1071–1078.e2. [Google Scholar] [CrossRef] [PubMed]
- Uehara, H.; Ikezawa, K.; Kawada, N.; Fukutake, N.; Katayama, K.; Takakura, R.; Takano, Y.; Ishikawa, O.; Takenaka, A. Diagnostic accuracy of endoscopic ultrasound-guided fine needle aspiration for suspected pancreatic malignancy in relation to the size of lesions. J. Gastroenterol. Hepatol. 2011, 26, 1256–1261. [Google Scholar] [CrossRef]
- Ramesh, J.; Kim, H.; Reddy, K.; Eltoum, I.E.A. Performance characteristic of endoscopic ultrasound-guided fine needle aspiration is unaffected by pancreatic mass size. Endosc. Int. Open 2016, 4, E434. [Google Scholar] [CrossRef]
- Crinò, S.F.; Bellocchi, M.C.C.; Bernardoni, L.; Manfrin, E.; Parisi, A.; Amodio, A.; De Pretis, N.; Frulloni, L.; Gabbrielli, A. Diagnostic yield of EUS-FNA of small (≤15 mm) solid pancreatic lesions using a 25-gauge needle. Hepatobiliary Pancreat. Dis. Int. 2018, 17, 70–74. [Google Scholar] [CrossRef]
- Siddiqui, A.A.; Brown, L.J.; Hong, S.K.S.; Draganova-Tacheva, R.A.; Korenblit, J.; Loren, D.E.; Kowalski, T.E.; Solomides, C. Relationship of pancreatic mass size and diagnostic yield of endoscopic ultrasound-guided fine needle aspiration. Dig. Dis. Sci. 2011, 56, 3370–3375. [Google Scholar] [CrossRef]
- Facciorusso, A.; Mohan, B.P.; Crinò, S.F.; Ofosu, A.; Ramai, D.; Lisotti, A.; Chandan, S.; Fusaroli, P. Contrast-enhanced harmonic endoscopic ultrasound-guided fine-needle aspiration versus standard fine-needle aspiration in pancreatic masses: A meta-analysis. Expert Rev. Gastroenterol. Hepatol. 2021, 15, 821–828. [Google Scholar] [CrossRef] [PubMed]
- Bor, R.; Vasas, B.; Fábián, A.; Szűcs, M.; Füredi, Á.; Czakó, L.; Rutka, M.; Farkas, K.; Molnár, T.; Milassin, Á.; et al. Slow-pull technique yields better quality smears: Prospective comparison of slow-pull and standard suction techniques of endoscopic ultrasound-guided fine-needle aspiration. Scand. J. Gastroenterol. 2020, 55, 1369–1376. [Google Scholar] [CrossRef] [PubMed]
- Togliani, T.; Lisotti, A.; Rinaldi, R.; Fornelli, A.; Pilati, S.; Passigato, N.; Fusaroli, P. Tumor Location in the Head/Uncinate Process and Presence of Fibrosis Impair the Adequacy of Endoscopic Ultrasound-Guided Tissue Acquisition of Solid Pancreatic Tumors. Cancers 2022, 14, 3544. [Google Scholar] [CrossRef]
- So, H.; Seo, D.W.; Hwang, J.S.; Ko, S.W.; Oh, D.; Song, T.T.; Park, D.H.; Lee, S.K.; Kim, M.-H. Macroscopic on-site evaluation after EUS-guided fine needle biopsy may replace rapid on-site evaluation. Endosc. Ultrasound 2021, 10, 111–115. [Google Scholar] [CrossRef]
- Guan, C.; Wu, M.; Ye, J.; Liu, Z.; Mao, Z.; Lu, C.; Zhang, J. Macroscopic on site quality evaluation of biopsy specimens to improve the diagnostic accuracy of endoscopic ultrasound guided fine needle aspiration using a 22 gauge needle for solid lesions: A single center retrospective study. Exp. Ther. Med. 2023, 26, 338. [Google Scholar] [CrossRef]
- Iwashita, T.; Yasuda, I.; Mukai, T.; Doi, S.; Nakashima, M.; Uemura, S.; Mabuchi, M.; Shimizu, M.; Hatano, Y.; Hara, A.; et al. Macroscopic on-site quality evaluation of biopsy specimens to improve the diagnostic accuracy during EUS-guided FNA using a 19-gauge needle for solid lesions: A single-center prospective pilot study (MOSE study). Gastrointest. Endosc. 2015, 81, 177–185. [Google Scholar] [CrossRef] [PubMed]
- Rimbaş, M.; Horumbă, M.; Rizzatti, G.; Crinò, S.F.; Gasbarrini, A.; Costamagna, G.; Larghi, A. Interventional endoscopic ultrasound for pancreatic neuroendocrine neoplasms. Dig. Endosc. 2020, 32, 1031–1041. [Google Scholar] [CrossRef]
- Mastrosimini, M.G.; Manfrin, E.; Remo, A.; De Bellis, M.; Parisi, A.; Pedron, S.; Luchini, C.; Brunelli, M.; Ammendola, S.; Bernardoni, L.; et al. Endoscopic ultrasound fine-needle biopsy to assess DAXX/ATRX expression and alternative lengthening of telomeres status in non-functional pancreatic neuroendocrine tumors. Pancreatology 2023, 23, 429–436. [Google Scholar] [CrossRef]
- Gocun, P.U.; Simsek, B.; Ekinci, O.; Ekmen, N.; Arhan, M.; Karakan, T.; Ibis, M.; Cindoruk, M. Risk of Malignancy Using the Diagnostic Categories Proposed by the World Health. Organization International System for Reporting Pancreaticobiliary Cytopathology. Acta Cytol. 2022, 66, 475–485. [Google Scholar] [CrossRef]
- Gonzalez-Mancera, M.S.; Ahmadian, S.S.; Gomez-Fernandez, C.; Velez-Torres, J.; Jorda, M.; García-Buitrago, M.T. Risk of malignancy associated with the diagnostic categories proposed by the Papanicolaou Society of Cytopathology for pancreaticobiliary specimens: An institutional experience. Diagn. Cytopathol. 2022, 50, 49–56. [Google Scholar] [CrossRef]
- Nikas, I.P.; Proctor, T.; Seide, S.; Chatziioannou, S.S.; Reynolds, J.P.; Ntourakis, D. Diagnostic Performance of Pancreatic Cytology with the Papanicolaou Society of Cytopathology System: A Systematic Review, before Shifting into the Upcoming WHO International System. Int. J. Mol. Sci. 2022, 23, 1650. [Google Scholar] [CrossRef] [PubMed]
- Abdelgawwad, M.S.; Alston, E.; Eltoum, I.A. The frequency and cancer risk associated with the atypical cytologic diagnostic category in endoscopic ultrasound-guided fine-needle aspiration specimens of solid pancreatic lesions: A meta-analysis and argument for a Bethesda System for Reporting Cytopathology of the Pancreas. Cancer Cytopathol. 2013, 121, 620–628. [Google Scholar] [PubMed]
- Alston, E.; Bae, S.; Eltoum, I.A. Atypical cytologic diagnostic category in EUS-FNA of the pancreas: Follow-up, outcomes, and predictive models. Cancer Cytopathol. 2014, 122, 428–434. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics of Patients | Characteristics of EUS-FNAs | ||
|---|---|---|---|
| Male/female | 229/244 | Examiners A/B: | 348/125 |
| Age (year) | 66.63 ± 11.81 (18–95; median: 68) | Mean number of puncture per examination | 3.44 ± 1.07 |
| Mean size of lesion (mm) | 33.83 ± 14.18 | Number of puncture per examination | |
| Size of lesion | ≤2 punctures | 90 (53.93%) | |
| ≤20 mm | 76 (16.07%) | 3–4 punctures | 311 (14.78%) |
| 20–40 mm | 257 (54.33%) | >4 punctures | 72 (19.19%) |
| ≥40 mm | 140 (29.60%) | ||
| Mean number of smear pairs per examination | 2.11 ± 1.01 | ||
| Location of lesion | |||
| head | 255 (53.91%) | ||
| uncinate process | 67 (14.16%) | Sampling technique | |
| body | 90 (19.03%) | only slow-pull (SP) | 73 (15.43%) |
| tail | 60 (12.68%) | only standard suction (SS) | 46 (9.73%) |
| diffuse | 1 (0.21%) | both SP and SS | 354 (74.84%) |
| Histology of lesion | |||
| Ductal adenocarcinoma | 352 (74.42%) | Size of EUS needle | |
| Primary bile duct carcinoma | 2 (0.42%) | 19 G | 33 (6.98%) |
| Solid pseudopapillary npl. | 3 (0.63%) | 22 G | 395 (83.51%) |
| Well-differentiated NET | 15 (3.17%) | 25 G | 45 (9.51%) |
| Neuroendocrine carcinoma | 3 (0.63%) | ||
| Low-grade IPMN | 1 (0.21%) | Biliary stent | 129 (27.27%) |
| High grade IPMN (clinical suspicion of malignancy) | 2 (0.42%) | Type of lesion based on EUS image | |
| Myxofibrosarcoma | 1 (0.21%) | benign | 54 (11.42%) |
| Hematolymphoid tumor | 2 (0.42%) | malignant | 419 (88.58%) |
| Metastatic carcinoma | 15 (3.17%) | Cytological finding based on PSC System | |
| Ancient schwannoma | 1 (0.21%) | “non-diagnostic” | 72 (15.22%) |
| Serous cystadenoma | 1 (0.21%) | “benign” | 33 (6.97%) |
| Intrapancreatic spleen | 1 (0.21%) | “atypical” | 28 (5.92%) |
| Acute necrosing pancreatitis | 12 (2.54%) | “neoplastic: other” | 19 (4.02%) |
| Autoimmune pancreatitis | 4 (0.85%) | “suspicious for alignancy” | 31 (6.55%) |
| Chronic pancreatitis | 31 (6.55%) | ||
| Histologically unverified focal lesion disappeared during follow-up | 27 (5.71%) | “malignant” | 290 (61.31%) |
| Conclusive n = 365 | Inconclusive n = 108 | Odds Ratio (95% CI) | p Value | |
|---|---|---|---|---|
| Examiner | ||||
| ExA | 274 (78.74%) | 74 (21.26%) | ||
| ExB | 91 (72.80%) | 34 (27.20%) | 1.38 (0.86–2.20) | 0.176 |
| Location of lesion | ||||
| Head | 188 (73.73%) | 69 (27.06%) | ||
| Uncinate process | 50 (74.63%) | 17 (25.37%) | 0.92 (0.48–1.67) | 0.781 |
| Body | 72 (80.00%) | 18 (20.00%) | 0.67 (0.37–1.19) | 0.187 |
| Tail | 56 (93.33%) | 4 (6.67%) | 0.19 (0.06–0.49) | 0.002 |
| Size of lesion | ||||
| ≤20 mm | 43 (56.58%) | 33 (43.42%) | ||
| 20–40 mm | 197 (76.65%) | 60 (23.35%) | 0.40 (0.23–0.68) | 0.001 |
| ≥40 mm | 125 (89.29%) | 15 (10.71%) | 0.16 (0.08–0.31) | <0.001 |
| Size of needle | ||||
| 19 G | 30 (90.91%) | 3 (9.09%) | 0.35 (0.08–1.01) | 0.088 |
| 22 G | 307 (77.72%) | 88 (22.28%) | ||
| 25 G | 28 (62.22%) | 17 (37.78%) | 2.12 (1.09–4.01) | 0.023 |
| Sampling technique | ||||
| Both SP and SS | 50 (68.49%) | 72 (20.34%) | ||
| SP or SS alone | 33 (71.74%) | 36 (30.25%) | 1.70 (1.06–2.70) | 0.027 |
| Slow-pull (SP) | 83 (69.75%) | 23 (31.51%) | 1.80 (1.02–3.12) | 0.038 |
| Standard suction (SS) | 282 (79.66%) | 13 (28.26%) | 1.54 (0.75–3.02) | 0.219 |
| Number of punctures per procedure | ||||
| ≤2 punctures | 56 (62.22%) | 34 (37.78%) | 2.49 (1.49–4.14) | <0.001 |
| 3–4 punctures | 250 (80.39%) | 61 (19.61%) | ||
| >4 punctures | 59 (81.94%) | 13 (18.06%) | 0.90 (0.45–1.71) | 0.763 |
| Type of sample | ||||
| Only direct smears | 28 (73.68%) | 10 (26.32%) | 1.23 (0.55–2.54) | 0.594 |
| Direct smears and FFPE | 337 (77.47%) | 98 (22.53%) | ||
| Origin of lesion | ||||
| Benign | 27 (34.62%) | 51 (65.38%) | 11.20 (6.56–19.54) | <0.001 |
| Malignant | 338 (85.57%) | 57 (14.43%) | ||
| EUS morphology | ||||
| Malignant | 339 (80.91%) | 80 (19.09%) | ||
| Benign | 26 (48.15%) | 28 (51.85%) | 4.56 (2.54–8.25) | <0.001 |
| Presence of biliary stent | ||||
| Absence | 256 (77.58%) | 74 (22.42%) | ||
| Presence | 109 (76.22%) | 34 (23.78%) | 1.08 (0.67–1.71) | 0.748 |
| Plastic stent | 83 (74.11%) | 29 (25.89%) | 1.21 (0.73–1.97) | 0.453 |
| Metal stent | 26 (83.87%) | 5 (16.13%) | 0.67 (0.22–1.66) | 0.720 |
| All Cases n = 473 | Risk of Malignancy | Odds Ratio (95% CI) | p Value |
|---|---|---|---|
| Gender | |||
| Female | 88.11% | 2.02 (1.23–3.36) | 0.006 |
| Male | 78.60% | ||
| Size of lesion | |||
| ≤20 mm | 60.53% | ||
| 20–40 mm | 86.38% | 4.14 (2.31–7.42) | <0.001 |
| ≥40 mm | 90.71% | 6.37 (3.12–13.65) | <0.001 |
| PSC category | |||
| “non-diagnostic” (PI) | 48.61% | ||
| “negative for malignancy” (PII) | 3.03% | 0.03 (0.00–0.17) | 0.001 |
| “atypical” (PIII) | 75.00% | 3.17 (1.25–8.90) | 0.020 |
| EUS morphology | |||
| benign | 3.70% | 0.03 (0.00–0.01) | <0.001 |
| malignant | 93.79% | ||
| Tumor markers * | |||
| CA19-9 (n = 270) | 5.75 (2.99–11.22) | <0.001 | |
| CA19-9 elevation | 89.55% | ||
| CA19-9 normal | 59.42% | ||
| CEA (n = 236) | 3.94 (1.88–9.11) | 0.001 | |
| CEA elevation | 91.18% | ||
| CEA normal | 72.39% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bor, R.; Vasas, B.; Fábián, A.; Szűcs, M.; Bősze, Z.; Bálint, A.; Rutka, M.; Farkas, K.; Tóth, T.; Resál, T.; et al. Risk Factors and Interpretation of Inconclusive Endoscopic Ultrasound-Guided Fine Needle Aspiration Cytology in the Diagnosis of Solid Pancreatic Lesions. Diagnostics 2023, 13, 2841. https://doi.org/10.3390/diagnostics13172841
Bor R, Vasas B, Fábián A, Szűcs M, Bősze Z, Bálint A, Rutka M, Farkas K, Tóth T, Resál T, et al. Risk Factors and Interpretation of Inconclusive Endoscopic Ultrasound-Guided Fine Needle Aspiration Cytology in the Diagnosis of Solid Pancreatic Lesions. Diagnostics. 2023; 13(17):2841. https://doi.org/10.3390/diagnostics13172841
Chicago/Turabian StyleBor, Renáta, Béla Vasas, Anna Fábián, Mónika Szűcs, Zsófia Bősze, Anita Bálint, Mariann Rutka, Klaudia Farkas, Tibor Tóth, Tamás Resál, and et al. 2023. "Risk Factors and Interpretation of Inconclusive Endoscopic Ultrasound-Guided Fine Needle Aspiration Cytology in the Diagnosis of Solid Pancreatic Lesions" Diagnostics 13, no. 17: 2841. https://doi.org/10.3390/diagnostics13172841
APA StyleBor, R., Vasas, B., Fábián, A., Szűcs, M., Bősze, Z., Bálint, A., Rutka, M., Farkas, K., Tóth, T., Resál, T., Bacsur, P., Molnár, T., & Szepes, Z. (2023). Risk Factors and Interpretation of Inconclusive Endoscopic Ultrasound-Guided Fine Needle Aspiration Cytology in the Diagnosis of Solid Pancreatic Lesions. Diagnostics, 13(17), 2841. https://doi.org/10.3390/diagnostics13172841