
Spinal Metastasis in a Patient with Supratentorial Glioblastoma with Primitive Neuronal Component: A Case Report with Clinical and Molecular Evaluation

 , , ,
, , ,  , ,
, ,
Abstract
:1. Introduction
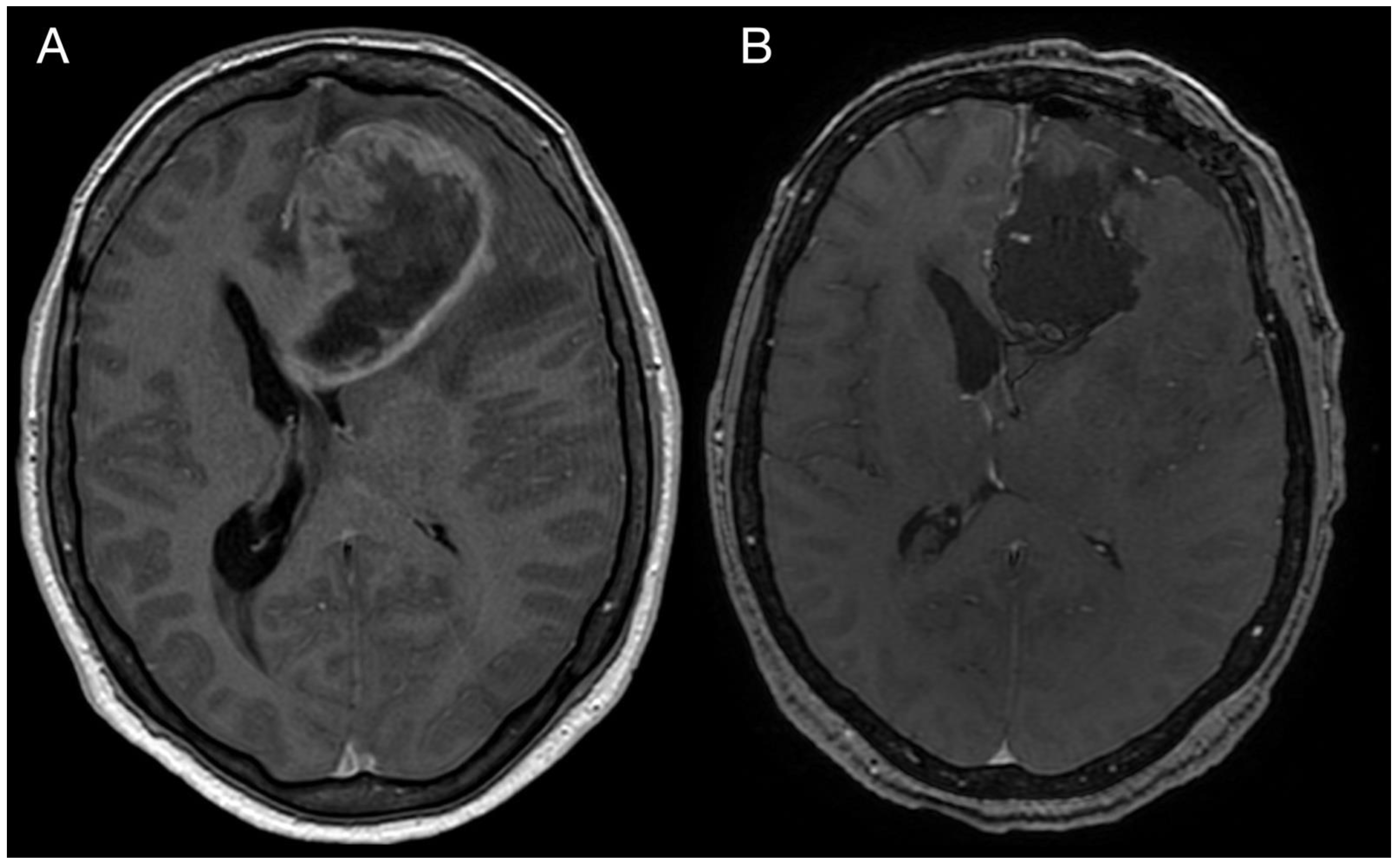
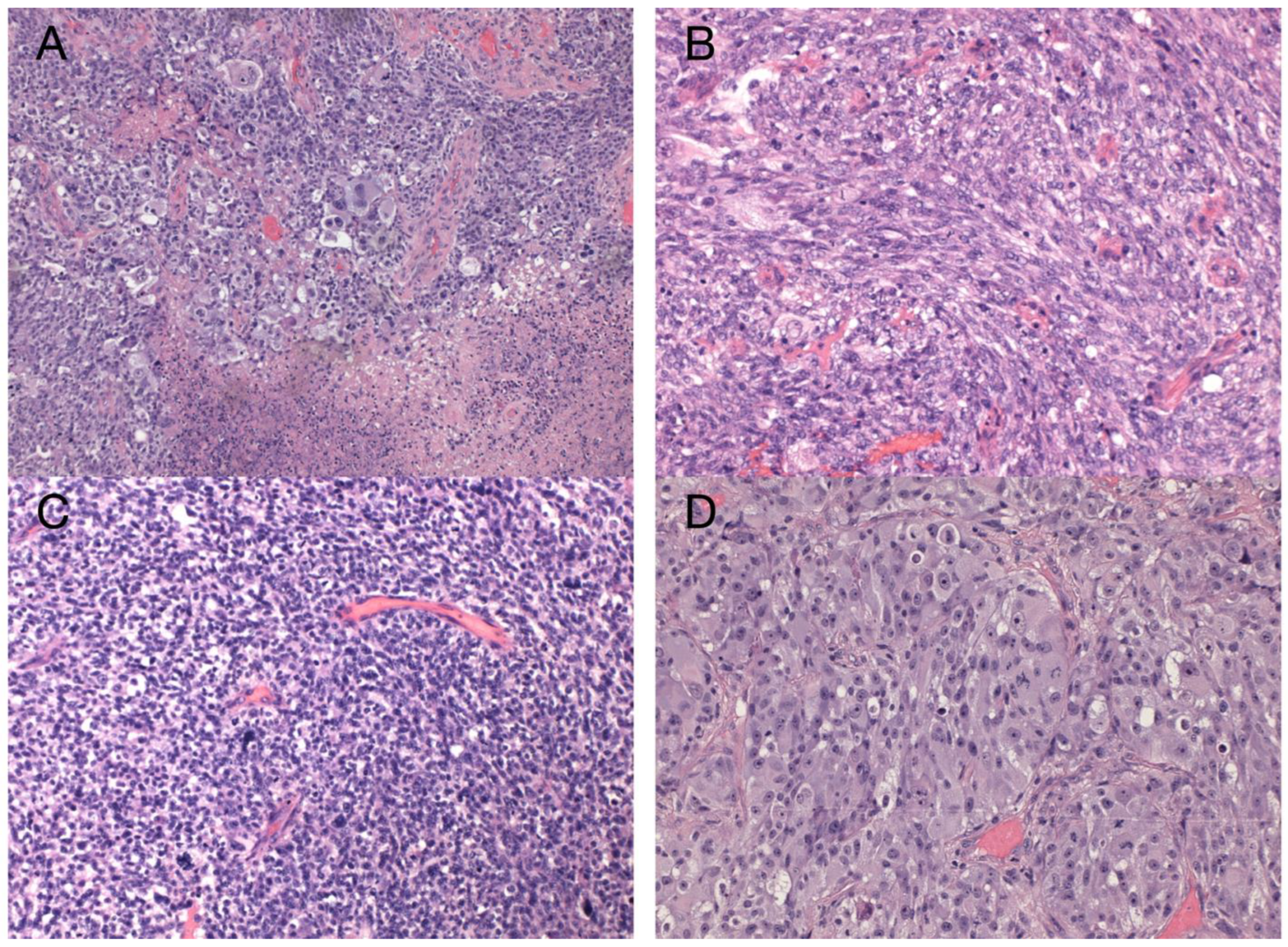
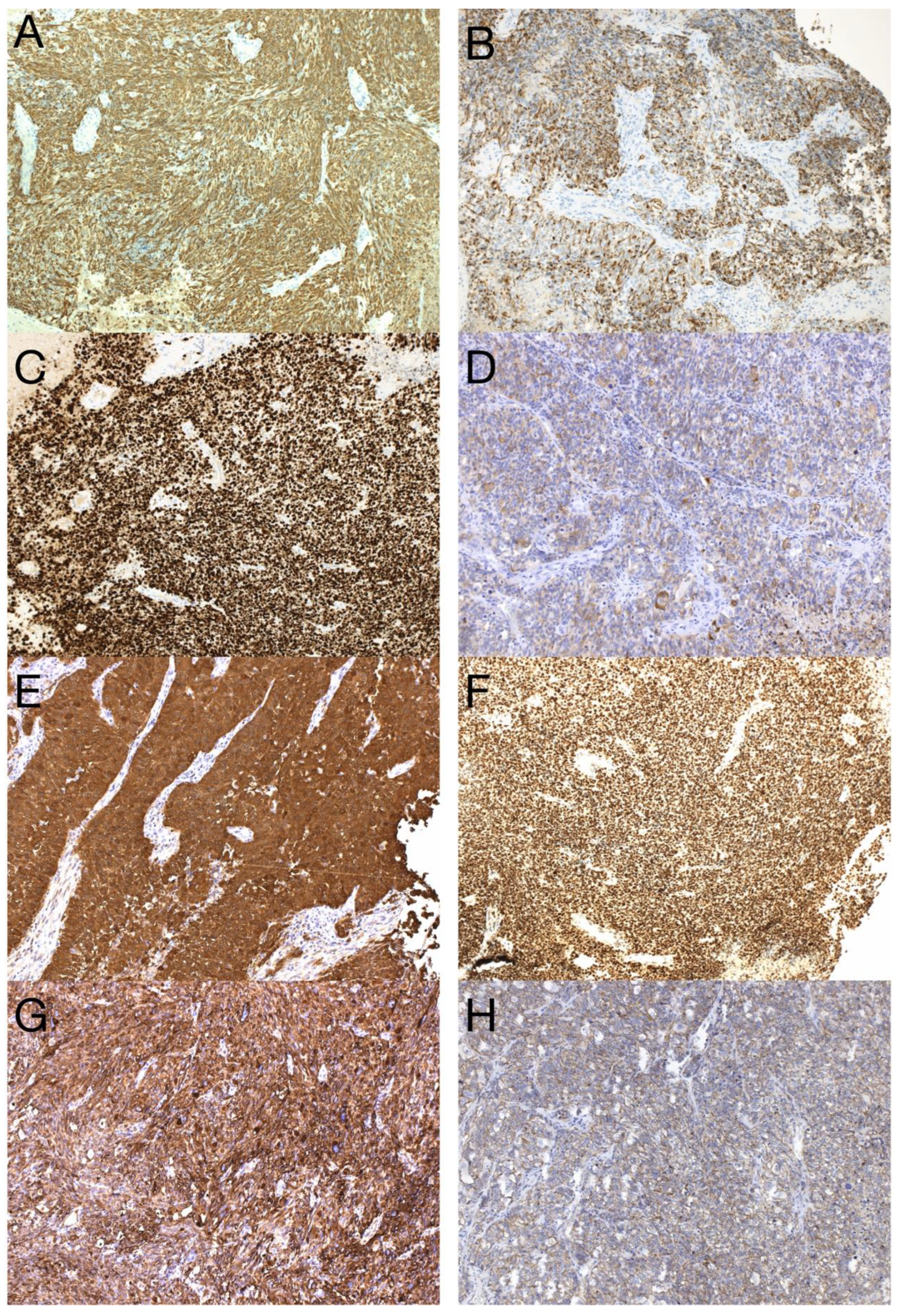
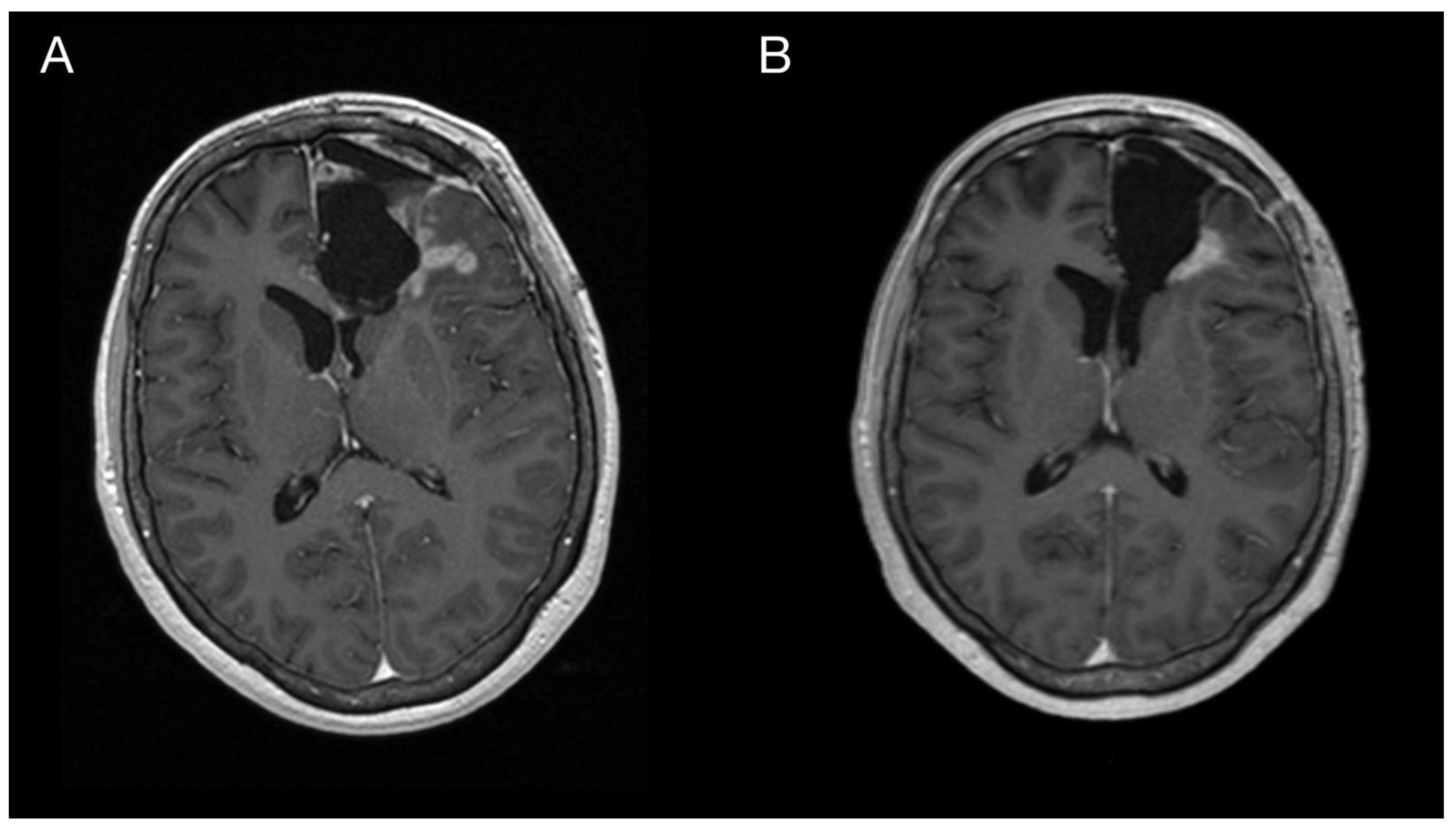
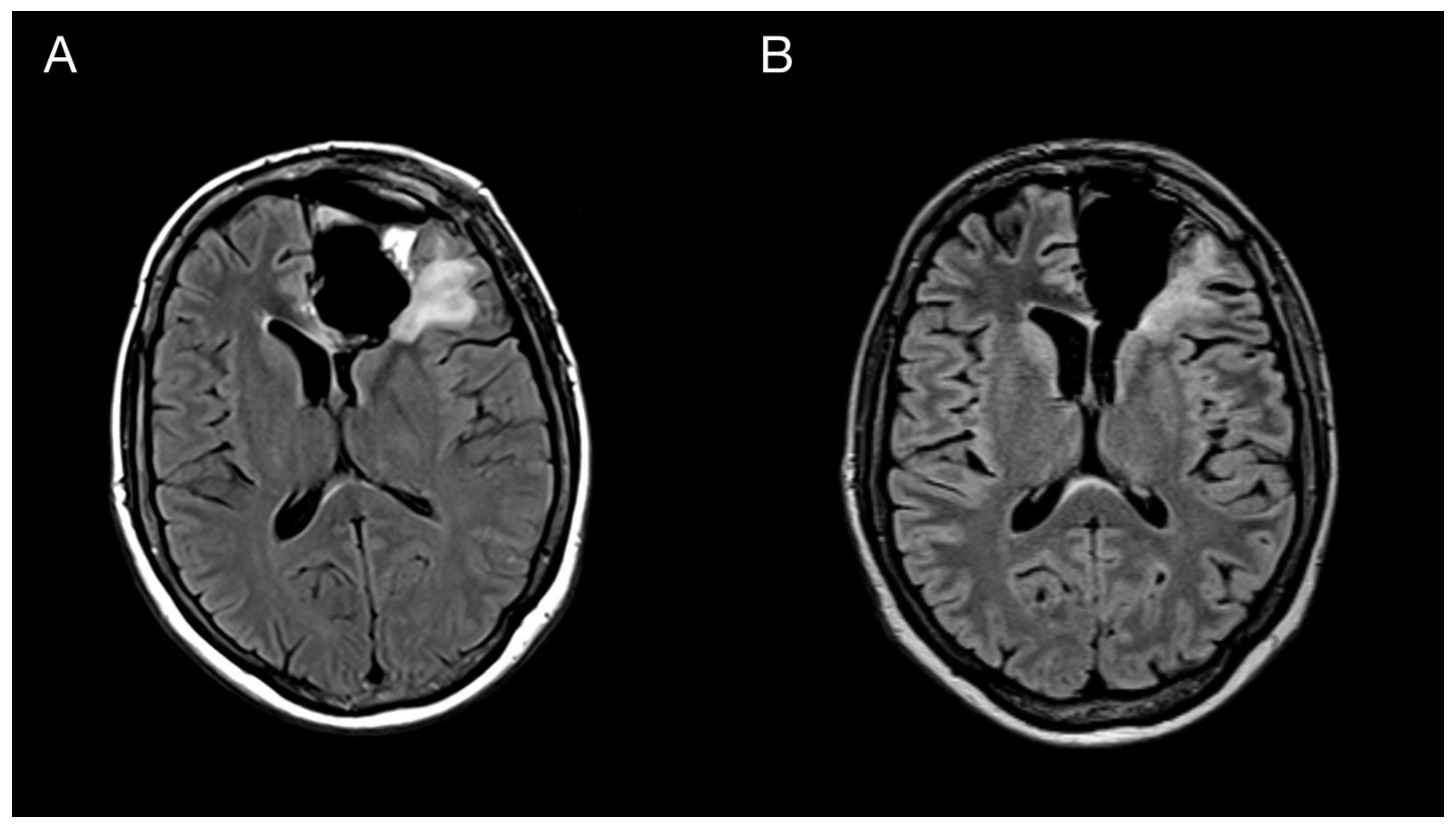
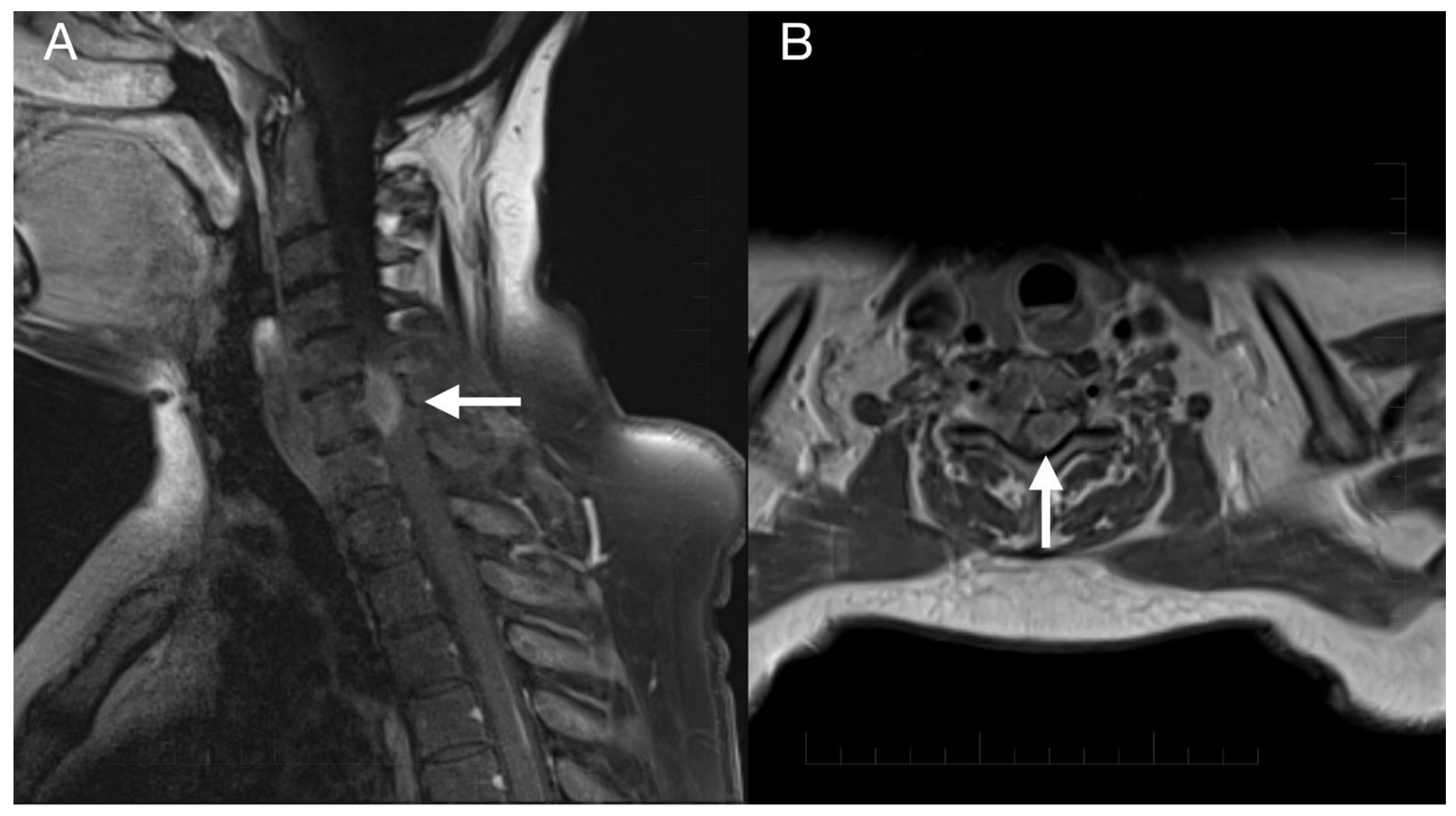
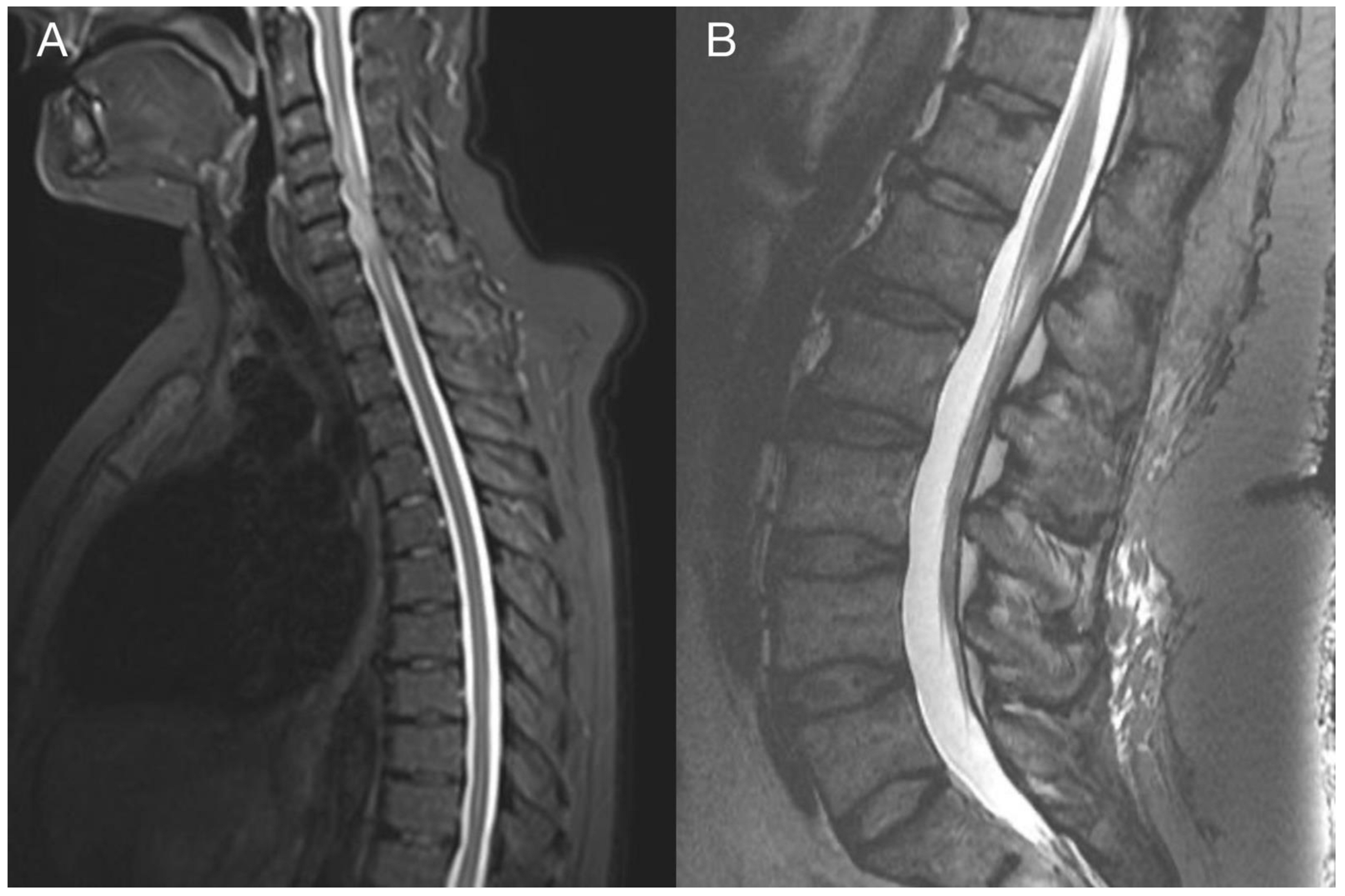
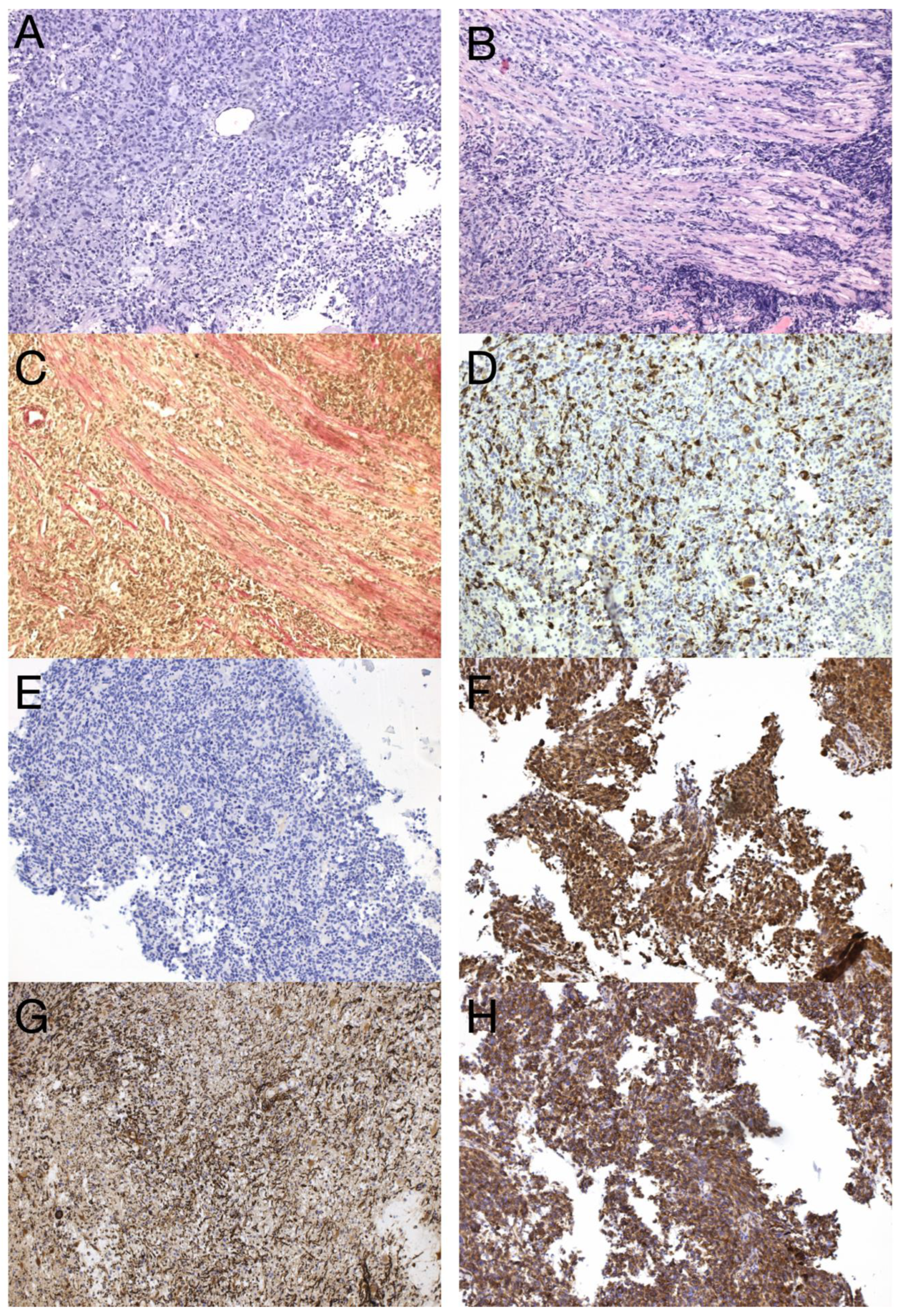
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ostrom, Q.T.; Cioffi, G.; Waite, K.; Kruchko, C.; Barnholtz-Sloan, J.S. CBTRUS Statistical Report: Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in 2014-2018. Neuro-Oncology 2021, 23, iii1–iii105. [Google Scholar] [CrossRef] [PubMed]
- Lakomy, R.; Kazda, T.; Selingerova, I.; Poprach, A.; Pospisil, P.; Belanova, R.; Fadrus, P.; Smrcka, M.; Vybihal, V.; Jancalek, R.; et al. Pre-Radiotherapy Progression after Surgery of Newly Diagnosed Glioblastoma: Corroboration of New Prognostic Variable. Diagnostics 2020, 10, 676. [Google Scholar] [CrossRef] [PubMed]
- Drumm, M.R.; Dixit, K.S.; Grimm, S.; Kumthekar, P.; Lukas, R.V.; Raizer, J.J.; Stupp, R.; Chheda, M.G.; Kam, K.-L.; McCord, M.; et al. Extensive brainstem infiltration, not mass effect, is a common feature of end-stage cerebral glioblastomas. Neuro-Oncology 2019, 22, 470–479. [Google Scholar] [CrossRef] [PubMed]
- Lakomy, R.; Kazda, T.; Selingerova, I.; Poprach, A.; Pospisil, P.; Belanova, R.; Fadrus, P.; Vybihal, V.; Smrcka, M.; Jancalek, R.; et al. Real-World Evidence in Glioblastoma: Stupp’s Regimen After a Decade. Front. Oncol. 2020, 10, 840. [Google Scholar] [CrossRef]
- Stupp, R.; Mason, W.; van den Bent, M.; Weller, M.; Fisher, B.; Taphoorn, M.; Belanger, K.; Brandes, A.; Marosi, C.; Bogdahn, U.; et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N. Engl. J. Med. 2005, 352, 987–996. [Google Scholar] [CrossRef] [Green Version]
- Amitendu, S.; Mak, S.K.D.; Ling, J.M.; Ng, W.H. A single institution experience of the incidence of extracranial metastasis in glioma. J. Clin. Neurosci. 2012, 19, 1511–1515. [Google Scholar] [CrossRef]
- Vertosick, F.T., Jr.; Selker, R.G. Brain stem and spinal metastases of supratentorial glioblastoma multiforme: A clinical series. Neurosurgery 1990, 27, 516–521. [Google Scholar] [CrossRef]
- Onda, K.; Tanaka, R.; Takahashi, H.; Takeda, N.; Ikuta, F. Cerebral glioblastoma with cerebrospinal fluid dissemination: A clinicopathological study of 14 cases examined by complete autopsy. Neurosurgery 1989, 25, 533–540. [Google Scholar] [CrossRef]
- Rosen, J.; Blau, T.; Grau, S.J.; Barbe, M.T.; Fink, G.R.; Galldiks, N. Extracranial Metastases of a Cerebral Glioblastoma: A Case Report and Review of the Literature. Case Rep. Oncol. 2018, 11, 591–600. [Google Scholar] [CrossRef] [Green Version]
- WHO Classification of Tumours Editorial Board. Central nervous system tumours. In WHO Classification of Tumours Series, 5th ed.; International Agency for Research on Cancer: Lyon, France, 2021; Volume 6, Available online: https://tumourclassification.iarc.who.int/chapters/45 (accessed on 26 March 2021).
- Suwala, A.; Stichel, D.; Schrimpf, D.; Maas, S.; Sill, M.; Dohmen, H.; Banan, R.; Reinhardt, A.; Sievers, P.; Hinz, F.; et al. Glioblastomas with primitive neuronal component harbor a distinct methylation and copy-number profile with inactivation of TP53, PTEN, and RB1. Acta Neuropathol. 2021, 142, 179–189. [Google Scholar] [CrossRef]
- Perry, A.; Miller, R.; Gujrati, M.; Scheithauer, B.; Zambrano, S.C.; Jost, S.; Raghavan, R.; Qian, J.; Cochran, E.; Huse, J.; et al. Malignant gliomas with primitive neuroectodermal tumor-like components: A clinicopathologic and genetic study of 53 cases. Brain Pathol. 2009, 19, 81–90. [Google Scholar] [CrossRef] [PubMed]
- Georgescu, M.M.; Olar, A. Genetic and histologic spatiotemporal evolution of recurrent, multifocal, multicentric and metastatic glioblastoma. Acta neuropathologica communications. Acta Neuropathol. Commun. 2020, 8, 10. [Google Scholar] [CrossRef] [PubMed]
- Franceschi, S.; Lessi, F.; Aretini, P.; Mazzanti, C.M.; Menicagli, M.; La Ferla, M.; De Gregorio, V.; Caramella, D.; Naccarato, A.G.; Bevilacqua, G.; et al. Molecular portrait of a rare case of metastatic glioblastoma: Somatic and germline mutations using whole-exome sequencing. Neuro-Oncology 2016, 18, 298–300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noch, E.K.; Sait, S.F.; Farooq, S.; Trippett, T.M.; Miller, A.M. A case series of extraneural metastatic glioblastoma at Memorial Sloan Kettering Cancer Center. Neuro Oncol. Pract. 2021, 8, 325–336. [Google Scholar] [CrossRef]
- Umphlett, M.; Shea, S.; Tome-Garcia, J.; Zhang, Y.; Hormigo, A.; Fowkes, M.; Tsankova, N.M.; Yong, R.L. Widely metastatic glioblastoma with BRCA1 and ARID1A mutations: A case report. BMC Cancer 2020, 20, 47. [Google Scholar] [CrossRef] [Green Version]
- Mohme, M.; Maire, C.L.; Schliffke, S.; Joosse, S.A.; Alawi, M.; Matschke, J.; Schüller, U.; Dierlamm, J.; Martens, T.; Pantel, K.; et al. Molecular profiling of an osseous metastasis in glioblastoma during checkpoint inhibition: Potential mechanisms of immune escape. Acta Neuropathol. Commun. 2020, 8, 1–13. [Google Scholar] [CrossRef]
- Boccaccio, C.; Comoglio, P.M. The MET oncogene in glioblastoma stem cells: Implications as a diagnostic marker and a therapeutic target. Cancer Res. 2013, 73, 3193–3199. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.-B.; Karpova, A.; Gritsenko, M.A.; Kyle, J.E.; Cao, S.; Li, Y.; Rykunov, D.; Colaprico, A.; Rothstein, J.H.; Hong, R.; et al. Proteogenomic and metabolomic characterization of human glioblastoma. Cancer Cell 2021, 39, 509–528.e20. [Google Scholar] [CrossRef]
- Lombard, A.; Goffart, N.; Rogister, B. Glioblastoma circulating cells: Reality, trap or illusion? Stem Cells Int. 2015, 2015, 182985. [Google Scholar] [CrossRef] [Green Version]
- Sullivan, J.P.; Nahed, B.V.; Madden, M.W.; Oliveira, S.M.; Springer, S.; Bhere, D.; Chi, A.S.; Wakimoto, H.; Rothenberg, S.M.; Sequist, L.V.; et al. Brain Tumor Cells in Circulation Are Enriched for Mesenchymal Gene Expression. Cancer Discov. 2014, 4, 1299–1309. [Google Scholar] [CrossRef]
- Brennan, C.W.; Verhaak, R.G.W.; McKenna, A.; Campos, B.; Noushmehr, H.; Salama, S.R.; Zheng, S.; Chakravarty, D.; Sanborn, J.Z.; Berman, S.H.; et al. The Somatic Genomic Landscape of Glioblastoma. Cell 2013, 155, 462–477. [Google Scholar] [CrossRef]
- Vizcaíno, M.A.; Shah, S.; Eberhart, C.G.; Rodriguez, F.J. Clinicopathologic implications of NF1 gene alterations in diffuse gliomas. Hum. Pathol. 2015, 46, 1323–1330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ricker, C.A.; Pan, Y.; Gutmann, D.; Keller, C. Challenges in Drug Discovery for Neurofibromatosis Type 1-Associated Low-Grade Glioma. Front. Oncol. 2016, 6, 259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coelho, B.P.; Fernandes, C.F.D.L.; Boccacino, J.M.; Souza, M.C.D.S.; Melo-Escobar, M.I.; Alves, R.N.; Prado, M.B.; Iglesia, R.P.; Cangiano, G.; Mazzaro, G.L.R.; et al. Multifaceted WNT Signaling at the Crossroads Between Epithelial-Mesenchymal Transition and Autophagy in Glioblastoma. Front. Oncol. 2020, 10, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Mahabir, R.; Tanino, M.; Elmansuri, A.; Wang, L.; Kimura, T.; Itoh, T.; Ohba, Y.; Nishihara, H.; Shirato, H.; Tsuda, M.; et al. Sustained elevation of Snail promotes glial-mesenchymal transition after irradiation in malignant glioma. Neuro-Oncology 2014, 16, 671–685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berthier, S.; Larrouquère, L.; Champelovier, P.; Col, E.; Lefebvre, C.; Cottet-Rouselle, C.; Arnaud, J.; Garrel, C.; Laporte, F.; Boutonnat, J.; et al. A New Patient-Derived Metastatic Glioblastoma Cell Line: Characterisation and Response to Sodium Selenite Anticancer Agent. Cancers 2019, 11, 12. [Google Scholar] [CrossRef] [Green Version]
- Xiu, M.; Wang, Y.; Li, B.; Wang, X.; Xiao, F.; Chen, S.; Zhang, L.; Zhou, B.; Hua, F. The Role of Notch3 Signaling in Cancer Stemness and Chemoresistance: Molecular Mechanisms and Targeting Strategies. Front. Mol. Biosci. 2021, 8, 1–17. [Google Scholar] [CrossRef]
- van Nes, J.; Chan, A.; van Groningen, T.; van Sluis, P.; Koster, J.; Versteeg, R. A NOTCH3 transcriptional module induces cell motility in neuroblastoma. Clin. Cancer Res. 2013, 19, 3485–3494. [Google Scholar] [CrossRef] [Green Version]
- Alqudah, M.A.Y.; Agarwal, S.; Al-Keilani, M.S.; Sibenaller, Z.A.; Ryken, T.C.; Assem, M. NOTCH3 Is a Prognostic Factor That Promotes Glioma Cell Proliferation, Migration and Invasion via Activation of CCND1 and EGFR. PLoS ONE 2013, 8, e77299. [Google Scholar] [CrossRef]
- Xu, S.; Tang, C. The Role of ARID1A in Tumors: Tumor Initiation or Tumor Suppression? Front. Oncol. 2021, 11, 1–18. [Google Scholar] [CrossRef]
- Shen, J.; Ju, Z.; Zhao, W.; Wang, L.; Peng, Y.; Ge, Z.; Nagel, Z.D.; Zou, J.; Wang, C.; Kapoor, P.; et al. ARID1A deficiency promotes mutability and potentiates therapeutic antitumor immunity unleashed by immune checkpoint blockade. Nat. Med. 2018, 24, 556–562. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gene Symbol | VID | cDOT | pDOT | Consequence | ACMG Classification |
|---|---|---|---|---|---|
| TP53 | 17:7577548:T | c.733G>A | p.Gly245Ser | missense_variant | Pathogenic |
| PTEN | 10:89717672:T | c.697C>T | p.Arg233Ter | stop_gained | Pathogenic |
| RB1 | 13:48955573:A | c.1689G>A | p.Trp563Ter | stop_gained | Likely pathogenic |
| DHFR | 5:79950728:79950727:CAGCGCCCC | c.420_428dup | - | 5_prime_UTR_variant | Likely pathogenic |
| MET | 7:116435786:G | c.3930A>G | p.Ile1310Met | missense_variant | Uncertain significance, some pathogenic evidence |
| INPP4B | 4:143003277:A | c.2549C>T | p.Ser850Leu | missense_variant | Uncertain significance, likely pathogenic—minor evidence |
| CTNNB1 | 3:41266897:T | c.568C>T | p.Arg190Cys | missense_variant | Uncertain significance, likely pathogenic—minor evidence |
| CDK6 | 7:92247520:T | c.700G>A | p.Val234Met | missense_variant, splice_region_variant | Uncertain significance, likely pathogenic—minor evidence |
| BRAF | 7:140508723:A | c.577G>T | p.Glu193Ter | stop_gained | Pathogenic |
| DNMT3A | 2:25463224:C | c.2269A>G | p.Asn757Asp | missense_variant | Likely pathogenic |
| CSF1R | 5:149440455:T | c.1939G>A | p.Val647Ile | missense_variant | Likely pathogenic |
| CARD11 | 7:2987212:T | c.217G>A | p.Ala73Thr | missense_variant | Uncertain significance, likely pathogenic—minor evidence |
| EP300 | 22:41572399:T | c.4928C>T | p.Ser1643Leu | missense_variant | Uncertain significance, some pathogenic evidence |
| NF1 | 17:29654741:A | c.5493G>A | p.Trp1831Ter | stop_gained | Pathogenic |
| CARD11 | 7:2984016:A | c.514G>T | p.Glu172Ter | stop_gained | Pathogenic |
| CREBBP | 16:3779578:T | c.5470G>A | p.Ala1824Thr | missense_variant | Likely pathogenic |
| NOTCH3 | 19:15290914:T | c.3296G>A | p.Cys1099Tyr | missense_variant | Likely pathogenic |
| ARID1A | 1:27094430:T | c.3138G>T | p.Arg1046Ser | missense_variant | Uncertain significance, likely pathogenic—minor evidence |
| MTOR | 1:11259396:T | c.4172G>A | p.Arg1391Gln | missense_variant | Uncertain significance, likely pathogenic—minor evidence |
| EGFR | 7:55233118:G | c.1868A>G | p.Asn623Ser | missense_variant | Uncertain significance, likely pathogenic—minor evidence |
| EGFR | 7:55273060:T | c.3383C>T | p.Pro1128Leu | missense_variant | Uncertain significance, likely pathogenic—minor evidence |
| CHEK1 | 11:125507382:G | c.757A>G | p.Arg253Gly | missense_variant | Uncertain significance, likely pathogenic—minor evidence |
| CDK4 | 12:58144737:T | c.491T>A | p.Ile164Asn | missense_variant | Uncertain significance, likely pathogenic—minor evidence |
| SLX4 | 16:3651029:A | c.1114C>T | p.Arg372Trp | missense_variant | Uncertain significance, likely pathogenic—minor evidence |
| NF1 | 17:29557364:T | c.3077G>T | p.Arg1026Ile | missense_variant | Uncertain significance, likely pathogenic—minor evidence |
| RAD51C | 17:56772457:A | c.311G>A | p.Cys104Tyr | missense_variant | Uncertain significance, likely pathogenic—minor evidence |
| NOTCH3 | 19:15285102:T | c.4513C>A | p.Pro1505Thr | missense_variant | Uncertain significance, likely pathogenic—minor evidence |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hendrych, M.; Solar, P.; Hermanova, M.; Slaby, O.; Valekova, H.; Vecera, M.; Kopkova, A.; Mackerle, Z.; Kazda, T.; Pospisil, P.; et al. Spinal Metastasis in a Patient with Supratentorial Glioblastoma with Primitive Neuronal Component: A Case Report with Clinical and Molecular Evaluation. Diagnostics 2023, 13, 181. https://doi.org/10.3390/diagnostics13020181
Hendrych M, Solar P, Hermanova M, Slaby O, Valekova H, Vecera M, Kopkova A, Mackerle Z, Kazda T, Pospisil P, et al. Spinal Metastasis in a Patient with Supratentorial Glioblastoma with Primitive Neuronal Component: A Case Report with Clinical and Molecular Evaluation. Diagnostics. 2023; 13(2):181. https://doi.org/10.3390/diagnostics13020181
Chicago/Turabian StyleHendrych, Michal, Peter Solar, Marketa Hermanova, Ondrej Slaby, Hana Valekova, Marek Vecera, Alena Kopkova, Zdenek Mackerle, Tomas Kazda, Petr Pospisil, and et al. 2023. "Spinal Metastasis in a Patient with Supratentorial Glioblastoma with Primitive Neuronal Component: A Case Report with Clinical and Molecular Evaluation" Diagnostics 13, no. 2: 181. https://doi.org/10.3390/diagnostics13020181
APA StyleHendrych, M., Solar, P., Hermanova, M., Slaby, O., Valekova, H., Vecera, M., Kopkova, A., Mackerle, Z., Kazda, T., Pospisil, P., Lakomy, R., Chrastina, J., Sana, J., & Jancalek, R. (2023). Spinal Metastasis in a Patient with Supratentorial Glioblastoma with Primitive Neuronal Component: A Case Report with Clinical and Molecular Evaluation. Diagnostics, 13(2), 181. https://doi.org/10.3390/diagnostics13020181