
Head-to-Head Comparison of Nasopharyngeal, Oropharyngeal and Nasal Swabs for SARS-CoV-2 Molecular Testing

 , and
, and 
Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Procedures for Collecting Upper Respiratory Specimens
2.3. Laboratory Methods
2.4. Outcome Measures
2.5. Statistical Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Centers for Disease Control and Prevention. Centers for Disease Control and Prevention. 8 July 2020. Interim Guidelines for Collecting, Handling, and Testing Clinical Specimens for COVID-19. Available online: https://www.cdc.gov/coronavirus/2019-ncov/lab/guidelines-clinical-specimens.html (accessed on 20 October 2022).
- Zayed, R.A.; Omran, D.; Zayed, A.A. COVID-19 clinical and laboratory diagnosis overview. J. Egypt. Public Health Assoc. 2021, 96, 25. [Google Scholar] [CrossRef]
- Lee, R.A.; Herigon, J.C.; Benedetti, A.; Pollock, N.R.; Denkinger, C.M. Performance of saliva, oropharyngeal swabs, and nasal swabs for SARS-CoV-2 molecular detection: A systematic review and meta-analysis. J. Clin. Microbiol. 2021, 59, e02881-20. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Xu, Y.; Gao, R.; Lu, R.; Han, K.; Wu, G.; Tan, W. Detection of SARS-CoV-2 in different types of clinical specimens. JAMA 2020, 323, 1843–1844. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kojima, N.; Turner, F.; Slepnev, V.; Bacelar, A.; Deming, L.; Kodeboyina, S.; Klausner, J.D. Self-collected oral fluid and nasal swabs demonstrate comparable sensitivity to clinician collected nasopharyngeal swabs for coronavirus disease 2019 detection. Clin. Infect. Dis. 2021, 73, e3106–e3109. [Google Scholar] [CrossRef] [PubMed]
- Jakobsen, K.K.; Jensen, J.S.; Todsen, T.; Kirkby, N.; Lippert, F.; Vangsted, A.M.; Klokker, M.; von Buchwald, C. Accuracy of anterior nasal swab rapid antigen tests compared with RT-PCR for massive SARS-CoV-2 screening in low prevalence population. APMIS Acta Pathol. Microbiol. Et. Immunol. Scandinavica. 2022, 130, 95–100. [Google Scholar] [CrossRef]
- He, X.; Lau, E.H.Y.; Wu, P.; Deng, X.; Wang, J.; Hao, X.; Lau, Y.C.; Liao, B.; Chen, W.; Hu, F.; et al. Temporal dynamics in viral shedding and transmissibility of COVID-19. Nat. Med. 2020, 26, 672–675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zou, L.; Ruan, F.; Huang, M.; Liang, L.; Huang, H.; Hong, Z.; Yu, J.; Kang, M.; Song, Y.; Xia, J.; et al. SARS-CoV-2 viral load in upper respiratory specimens of infected patients. N. Engl. J Med. 2020, 382, 1177–1179. [Google Scholar] [CrossRef]
- Huang, Y.; Chen, S.; Yang, Z.; Guan, W.; Liu, D.; Lin, Z.; Zhang, Y.; Xu, Z.; Liu, X.; Li, Y. SARS-CoV-2 viral load in clinical samples from critically ill patients. Am. J. Respir. Crit. Care Med. 2020, 201, 1435–1438. [Google Scholar] [CrossRef] [Green Version]
- Todsen, T.; Benfield, T. Comparison of SARS-CoV-2 reverse transcriptase polymerase chain reaction and binaxnow rapid antigen tests at a community site during an omicron surge. Ann. Intern. Med. 2022, 175, W119. [Google Scholar] [CrossRef]
- Jensen, M.M.; Larsen, K.D.; Homøe, A.-S.; Simonsen, A.L.; Arndal, E.; Koch, A.; Samuelsen, G.B.; Nielsen, X.C.; Todsen, T.; Homøe, P. Subjective and psychophysical olfactory and gustatory dysfunction among COVID-19 outpatients; short- and long-term results. PLoS ONE 2022, 17, e0275518. [Google Scholar] [CrossRef]
- Callesen, R.; Kiel, C.; Hovgaard, L.; Jakobsen, K.; Papesch, M.; von Buchwald, C.; Todsen, T. Optimal insertion depth for nasal mid-turbinate and nasopharyngeal swabs. Diagnostics 2021, 11, 1257. [Google Scholar] [CrossRef] [PubMed]
- Todsen, T.; Kirkby, N.; Lippert, F.; Benfield, T.; von Buchwald, C. Methods for collecting upper respiratory tract specimens for COVID-19 diagnostics. Ugeskr Laeger 2021, 183, V03210265. [Google Scholar] [PubMed]
- Charlton, C.L.; Babady, E.; Ginocchio, C.C.; Hatchette, T.F.; Jerris, R.C.; Li, Y.; Loeffelholz, M.; McCarter, Y.S.; Miller, M.B.; Drews, S.J. Practical guidance for clinical microbiology laboratories: Viruses causing acute respiratory tract infections. Clin. Microbiol. Rev. 2019, 32, e00042-18. [Google Scholar] [PubMed] [Green Version]
- Ursic, T.; Kogoj, R.; Sikonja, J.; Roskaric, D.; Jevsnik Virant, M.; Bogovic, P.; Petrovec, M. Performance of nasopharyngeal swab and saliva in detecting Delta and Omicron SARS-CoV-2 variants. J. Med. Virol. 2022, 94, 4704–4711. [Google Scholar] [CrossRef] [PubMed]
- Fall, A.; Eldesouki, R.E.; Sachithanandham, J.; Morris, C.P.; Norton, J.M.; Gaston, D.C.; Forman, M.; Abdullah, O.; Gallagher, N.; Li, M.; et al. The displacement of the SARS-CoV-2 variant Delta with Omicron: An investigation of hospital admissions and upper respiratory viral loads. EBioMedicine 2022, 79, 104008. [Google Scholar] [CrossRef]
- Hanson, K.E.; Caliendo, A.M.; Arias, C.A.; Hayden, M.K.; Englund, J.A.; Lee, M.J.; Loeb, M.; Patel, R.; El Alayli, A.; Altayar, O.; et al. The infectious diseases society of america guidelines on the diagnosis of COVID-19: Molecular diagnostic testing. Clin. Infect. Dis. 2021. [Google Scholar] [CrossRef]
- Tsang, N.N.Y.; So, H.C.; Ng, K.Y.; Cowling, B.J.; Leung, G.M.; Ip, D.K.M. Diagnostic performance of different sampling approaches for SARS-CoV-2 RT-PCR testing: A systematic review and meta-analysis. Lancet Infect. Dis. 2021, 21, 1233–1245. [Google Scholar] [CrossRef]
- Todsen, T.; Bohr, A.; Hovgaard, L.H.; Eieth, R.C.; Benfield, T.; Svendsen, M.B.S.; Kirkby, N.; Konge, L.; von Buchwald, C.; Melchiors, J.; et al. Valid and reliable assessment of upper respiratory tract specimen collection skills during the COVID-19 pandemic. Diagnostics 2021, 11, 1987. [Google Scholar] [CrossRef]
- CDC. Intertim Guidelines for Collecting and Handling of Clinical Specimens for COVID-19 Testing. Updated 25 October 2021. Available online: https://www.cdc.gov/coronavirus/2019-ncov/lab/guidelines-clinical-specimens.html (accessed on 20 October 2022).
- Wang, X.; Tan, L.; Wang, X.; Liu, W.; Lu, Y.; Cheng, L.; Sun, Z. Comparison of nasopharyngeal and oropharyngeal swabs for SARS-CoV-2 detection in 353 patients received tests with both specimens simultaneously. Int. J. Infect. Dis. 2020, 94, 107–109. [Google Scholar] [CrossRef]
- Palmas, G.; Moriondo, M.; Trapani, S.; Ricci, S.; Calistri, E.; Pisano, L.; Perferi, G.; Galli, L.; Venturini, E.; Indolfi, G.; et al. Nasal swab as preferred clinical specimen for COVID-19 testing in children. Pediatr. Infect. Dis. J. 2020, 39, e267–e270. [Google Scholar] [CrossRef]
- Berenger, B.M.; Fonseca, K.; Schneider, A.R.; Hu, J.; Zelyas, N. Clinical evaluation of nasopharyngeal, midturbinate nasal and oropharyngeal swabs for the detection of SARS-CoV-2. Diagn. Microbiol. Infect. Dis. 2022, 102, 115618. [Google Scholar] [CrossRef] [PubMed]
- Therchilsen, J.H.; Von Buchwald, C.; Koch, A.; Nielsen, S.D.; Rasmussen, D.B.; Thudium, R.F.; Kirkby, N.S.; Raaschou-Pedersen, D.E.T.; Bundgaard, J.S.; Iversen, K.; et al. Self-collected versus healthcare worker-collected swabs in the diagnosis of severe acute respiratory syndrome coronavirus 2. Diagnostics 2020, 10, 678. [Google Scholar] [CrossRef] [PubMed]
- Bundgaard, J.S.; Raaschou-Pedersen, D.T.; Todsen, T.; Ringgaard, A.; Torp-Pedersen, C.; Von Buchwald, C.; Iversen, K.; Bundgaard, H. Danish citizens’ preferences for at-home oropharyngeal/nasal SARS-CoV-2 specimen collection. Int. J. Infect. Dis. 2021, 109, 195–198. [Google Scholar] [CrossRef] [PubMed]
- Ramdas, K.; Darzi, A.; Jain, S. ‘Test, re-test, re-test’: Using inaccurate tests to greatly increase the accuracy of COVID-19 testing. Nat. Med. 2020, 26, 810–811. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| OPS | NPS | Nasal Swab | OPS/NPS | OPS/Nasal Swab | |
|---|---|---|---|---|---|
| Positive | 48 | 47 | 42 | 51 | 49 |
| Negative | 3 | 4 | 9 | 0 | 2 |
| Sensitivity (%) | 94.1 | 92.2 | 82.4 | 100 | 96 |
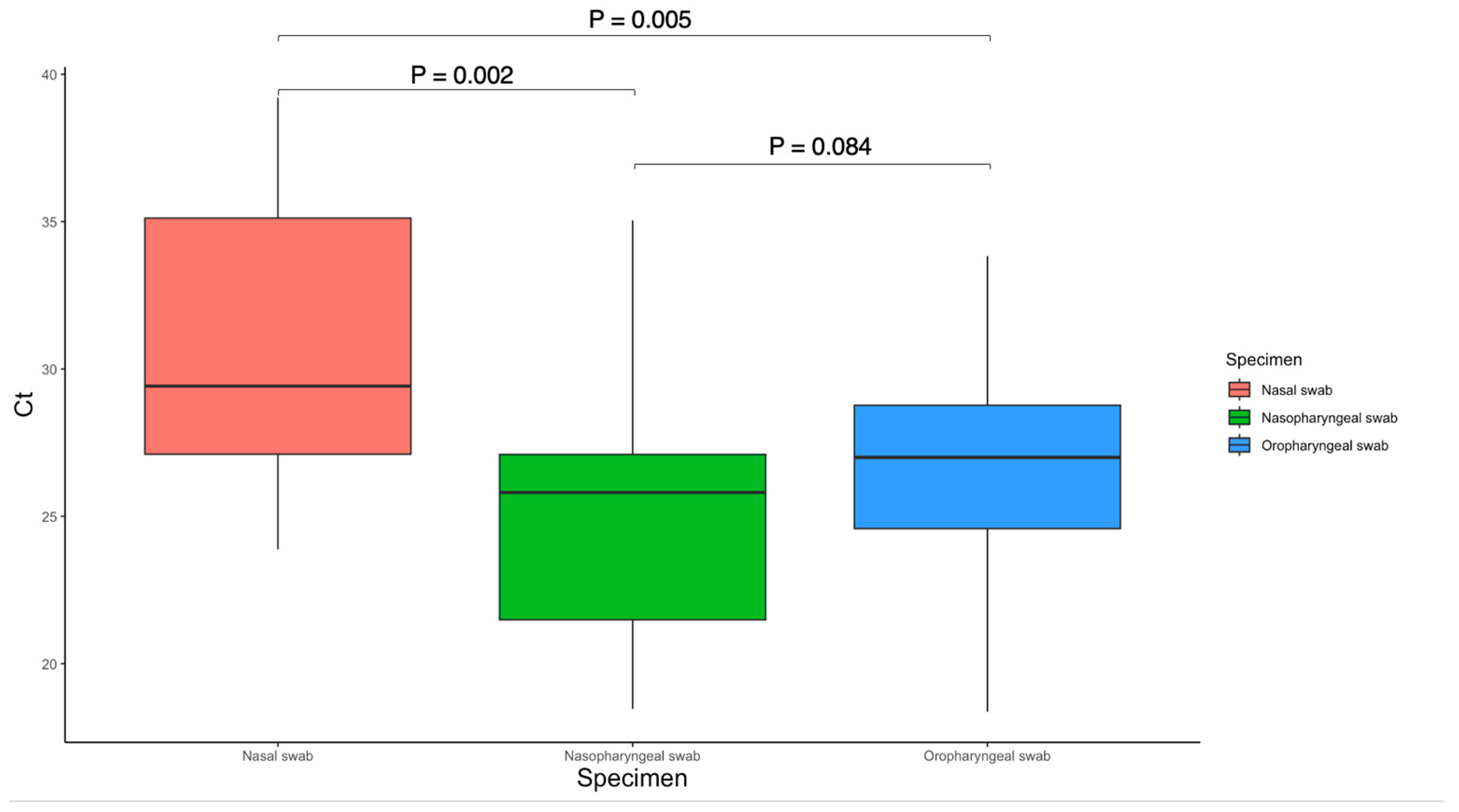
| Mean Ct value | 26.63 * | 24.98 * | 30.60 * | - | - |
| Specimen Type | ΔSensitivity | p-Value * |
|---|---|---|
| OPS vs. NPS | 1.6% | 1.000 |
| NPS vs. Nasal swab | 9.8% | 0.063 |
| OPS vs. Nasal swab | 11.7% | 0.070 |
| OPS/NPS vs. OPS | 5.8% | 0.250 |
| OPS/NPS vs. NPS | 7.8% | 0.125 |
| OPS/NPS vs. Nasal swab | 17.6% | 0.004 |
| OPS/Nasal swab vs. OPS | 3.9% | 1.000 |
| OPS/Nasal swab vs. NPS | 5.8% | 1.000 |
| OPS/Nasal swab vs. NMTS | 15.7% | 0.031 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Larsen, K.D.; Jensen, M.M.; Homøe, A.-S.; Arndal, E.; Samuelsen, G.B.; Koch, A.; Nielsen, X.C.; Homøe, P.; Todsen, T. Head-to-Head Comparison of Nasopharyngeal, Oropharyngeal and Nasal Swabs for SARS-CoV-2 Molecular Testing. Diagnostics 2023, 13, 283. https://doi.org/10.3390/diagnostics13020283
Larsen KD, Jensen MM, Homøe A-S, Arndal E, Samuelsen GB, Koch A, Nielsen XC, Homøe P, Todsen T. Head-to-Head Comparison of Nasopharyngeal, Oropharyngeal and Nasal Swabs for SARS-CoV-2 Molecular Testing. Diagnostics. 2023; 13(2):283. https://doi.org/10.3390/diagnostics13020283
Chicago/Turabian StyleLarsen, Kasper Daugaard, Mads Mose Jensen, Anne-Sophie Homøe, Elisabeth Arndal, Grethe Badsberg Samuelsen, Anders Koch, Xiaohui Chen Nielsen, Preben Homøe, and Tobias Todsen. 2023. "Head-to-Head Comparison of Nasopharyngeal, Oropharyngeal and Nasal Swabs for SARS-CoV-2 Molecular Testing" Diagnostics 13, no. 2: 283. https://doi.org/10.3390/diagnostics13020283
APA StyleLarsen, K. D., Jensen, M. M., Homøe, A. -S., Arndal, E., Samuelsen, G. B., Koch, A., Nielsen, X. C., Homøe, P., & Todsen, T. (2023). Head-to-Head Comparison of Nasopharyngeal, Oropharyngeal and Nasal Swabs for SARS-CoV-2 Molecular Testing. Diagnostics, 13(2), 283. https://doi.org/10.3390/diagnostics13020283