
SARS-CoV-2 Detection via RT-PCR in Matched Saliva and Nasopharyngeal Samples Reveals High Concordance in Different Commercial Assays

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
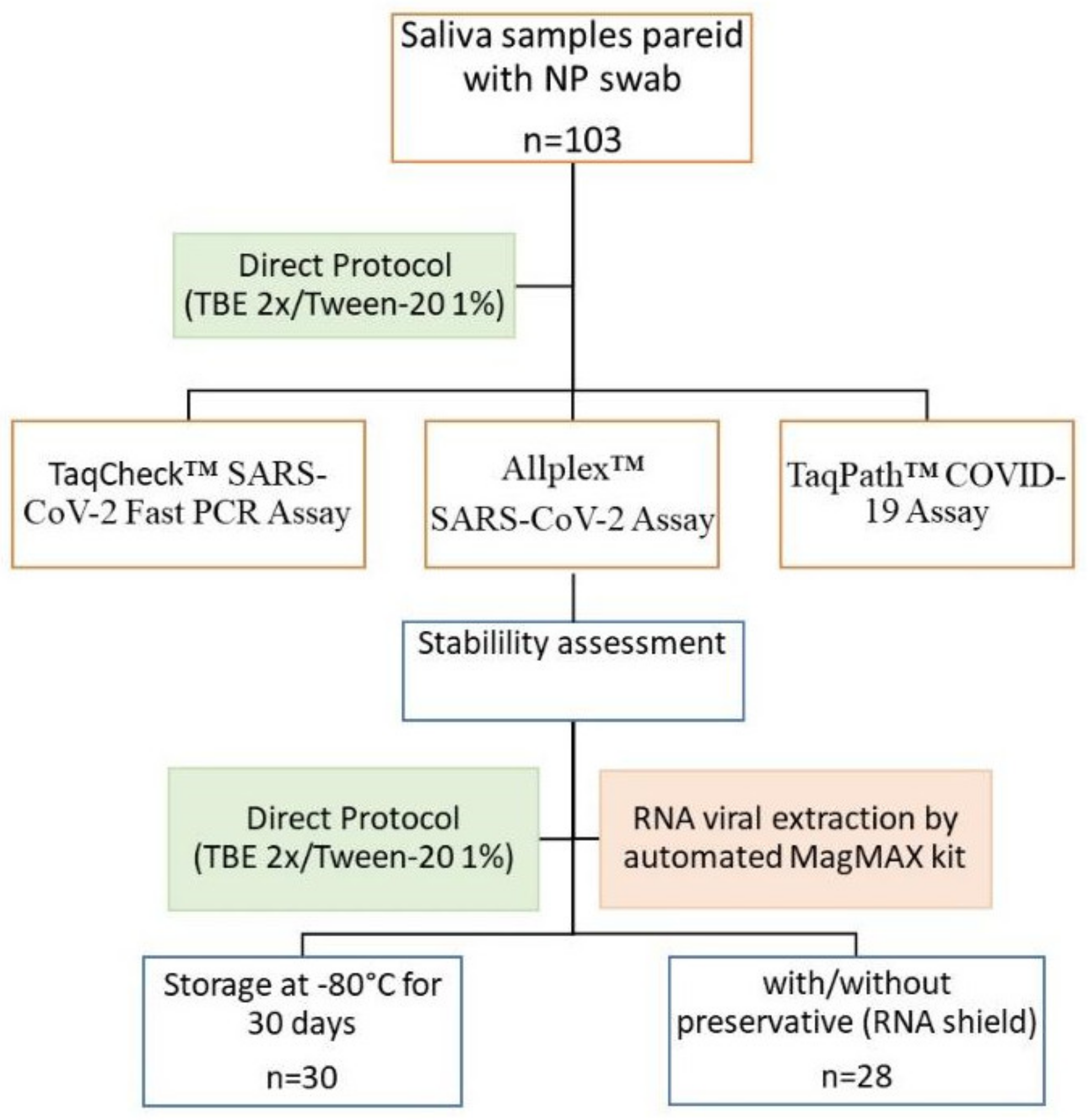
2.1. Patients and Sample Collection
2.2. Sample Processing and RT-PCR for SARS-CoV-2
2.3. Statistical Analysis
3. Results
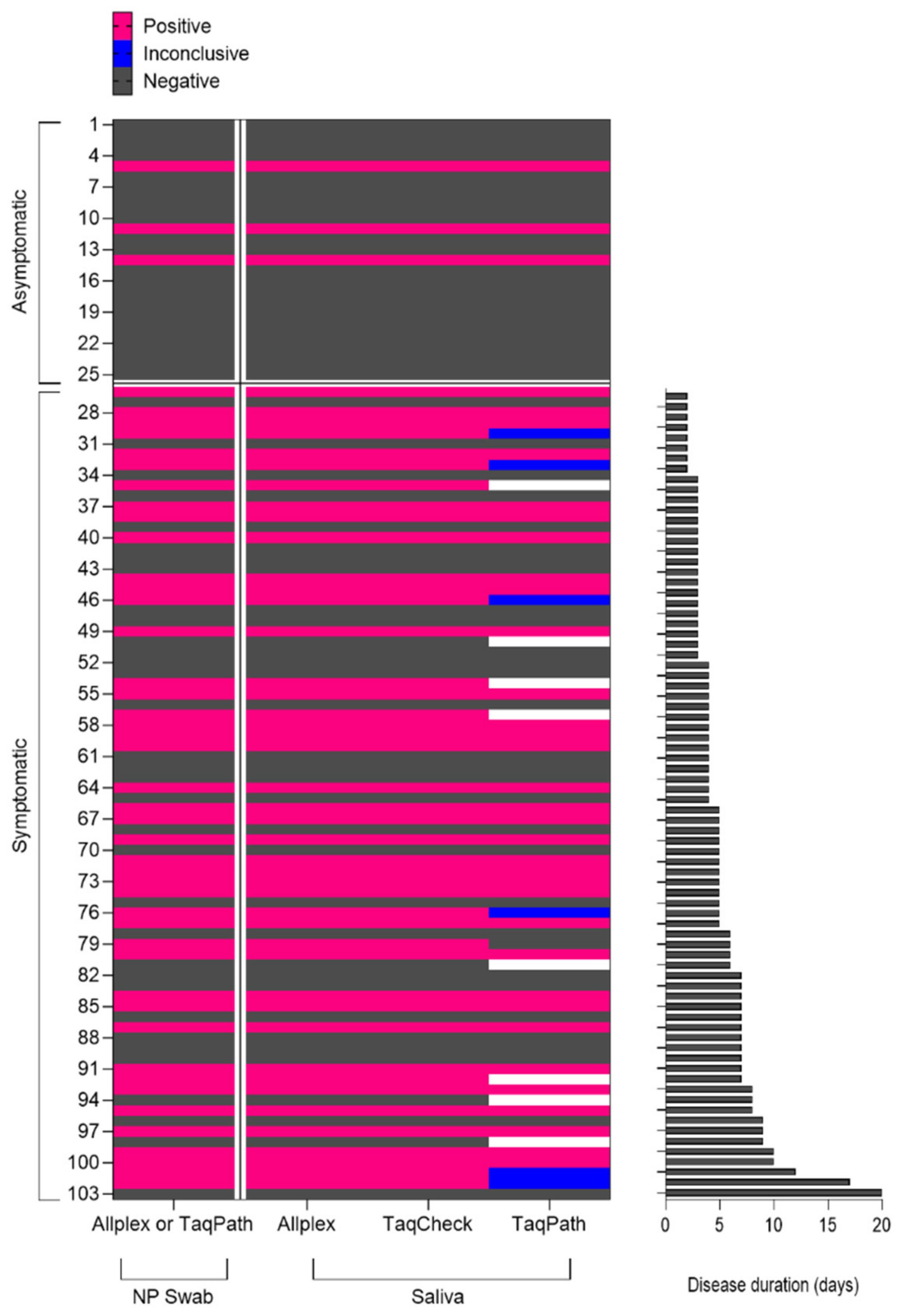
3.1. Comparative Performance of Self-Collected Saliva Samples via Extraction-Free Protocols
3.2. Evaluation of the Stability of Stored Saliva Samples
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Johanna, N.; Citrawijaya, H.; Wangge, G. Mass screening vs lockdown vs combination of both to control COVID-19: A systematic review. J. Public Health Res. 2020, 9, 523–531. [Google Scholar] [CrossRef] [PubMed]
- Woo, P.C.; Lau, S.K.; Lam, C.S.; Lau, C.C.; Tsang, A.K.; Lau, J.H.; Bai, R.; Teng, J.L.L.; Tsang, C.C.C.; Wang, M.; et al. Discovery of Seven Novel Mammalian and Avian Coronaviruses in the Genus Deltacoronavirus Supports Bat Coronaviruses as the Gene Source of Alphacoronavirus and Betacoronavirus and Avian Coronaviruses as the Gene Source of Gammacoronavirus and Deltacoronavirus. J. Virol. 2012, 86, 3995–4008. [Google Scholar] [PubMed] [Green Version]
- Granato, P.A.; Kimball, S.R.; Alkins, B.R.; Cross, D.C.; Unz, M.M. Comparative evaluation of the Thermo fisher TaqPathTM COVID-19 combo kit with the Cepheid Xpert® Xpress SARS-CoV-2 assay for detecting SARS-CoV-2 in nasopharyngeal specimens. BMC Infect. Dis. 2021, 21, 623. [Google Scholar] [CrossRef] [PubMed]
- Farfour, E.; Lesprit, P.; Visseaux, B.; Pascreau, T.; Jolly, E.; Houhou, N.; Mazaux, L.; Asso-Bonnet, M.; Vasse, M.; on behalf of the SARS-CoV-2 Foch Hospital Study Group. The Allplex 2019-nCoV (Seegene) assay: Which performances are for SARS-CoV-2 infection diagnosis? Eur. J. Clin. Microbiol. Infect. Dis. 2020, 39, 1997–2000. [Google Scholar] [CrossRef] [PubMed]
- Corman, V.M.; Landt, O.; Kaiser, M.; Molenkamp, R.; Meijer, A.; Chu, D.K.; Bleicker, T.; Brünink, S.; Schneider, J.; Schmidt, M.L.; et al. Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR. Eurosurveillance 2020, 25, 2000045. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kapoor, P.; Chowdhry, A.; Kharbanda, O.P.; Bablani Popli, D.; Gautam, K.; Saini, V. Exploring salivary diagnostics in COVID-19: A scoping review and research suggestions. BDJ Open 2021, 7, 8. [Google Scholar] [CrossRef]
- Kevadiya, B.D.; Machhi, J.; Herskovitz, J.; Oleynikov, M.D.; Blomberg, W.R.; Bajwa, N.; Soni, D.; Das, S.; Hasan, M.; Patel, M.; et al. Diagnostics for SARS-CoV-2 infections. Nat. Mater. 2021, 20, 593–605. [Google Scholar] [CrossRef]
- Vilela, A.C.S.; Costa, N.L. The COVID-19 and Saliva Paradox. J. Oral Maxillofac. Surg. 2020, 78, 2105. [Google Scholar] [CrossRef]
- Fernandes, L.L.; Pacheco, V.B.; Borges, L.; Athwal, H.K.; de Paula Eduardo, F.; Bezinelli, L.; Bezinelli, L.; Correa, L.; Jimenez, M.; Dame-Teixeira, N.; et al. Saliva in the Diagnosis of COVID-19: A Review and New Research Directions. J. Dent. Res. 2020, 99, 1435–1443. [Google Scholar] [CrossRef]
- Butler-Laporte, G.; Lawandi, A.; Schiller, I.; Yao, M.; Dendukuri, N.; McDonald, E.G.; Lee, T.C. Comparison of Saliva and Nasopharyngeal Swab Nucleic Acid Amplification Testing for Detection of SARS-CoV-2. JAMA Intern. Med. 2021, 181, 353–360. [Google Scholar] [CrossRef]
- Teo AK, J.; Choudhury, Y.; Tan, I.B.; Cher, C.Y.; Chew, S.H.; Wan, Z.Y.; Cheng, L.T.E.; Oon, L.L.E.; Tan, M.H.; Chan, K.S.; et al. Saliva is more sensitive than nasopharyngeal or nasal swabs for diagnosis of asymptomatic and mild COVID-19 infection. Sci. Rep. 2021, 11, 3134. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Wei, Q.; Alvarez, X.; Wang, H.; Du, Y.; Zhu, H.; Jiang, H.; Zhou, J.; Lam, P.; Zhang, L.; et al. Epithelial Cells Lining Salivary Gland Ducts Are Early Target Cells of Severe Acute Respiratory Syndrome Coronavirus Infection in the Upper Respiratory Tracts of Rhesus Macaques. J. Virol. 2011, 85, 4025–4030. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ning, B.; Yu, T.; Zhang, S.; Huang, Z.; Tian, D.; Lin, Z.; Hensley, K.; Threeton, B.; Lyon, C.J.; Yin, X.-M.; et al. A smartphone-read ultrasensitive and quantitative saliva test for COVID-19. Sci. Adv. 2021, 7, eabe3703. [Google Scholar] [CrossRef]
- Food and Drug Administration. FDA Authorizes First Diagnostic Test Using At-Home Collection of Saliva Specimens. 2020. Available online: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-authorizes-first-diagnostic-test-using-home-collection-saliva (accessed on 8 May 2020).
- Vogels, C.B.; Watkins, A.E.; Harden, C.A.; Brackney, D.E.; Shafer, J.; Wang, J.; Caraballo, C.; Kalinich, C.C.; Ott, I.M.; Fauver, J.R.; et al. SalivaDirect: A simplified and flexible platform to enhance SARS-CoV-2 testing capacity. Med 2021, 2, 263–280. [Google Scholar] [CrossRef]
- Oba, J.; Taniguchi, H.; Sato, M.; Takamatsu, R.; Morikawa, S.; Nakagawa, T.; Takaishi, H.; Saya, H.; Matsuo, K.; Nishihara, H. RT-PCR Screening Tests for SARS-CoV-2 with Saliva Samples in Asymptomatic People: Strategy to Maintain Social and Economic Activities while Reducing the Risk of Spreading the Virus. Keio J. Med. 2021, 70, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Zhao, J.; Peng, J.; Li, X.; Deng, X.; Geng, Z.; Shen, Z.; Guo, F.; Zhang, Q.; Jin, Y.; et al. Detection of SARS-CoV-2 in saliva and characterization of oral symptoms in COVID-19 patients. Cell Prolif. 2020, 53, e12923. [Google Scholar] [CrossRef] [PubMed]
- To, K.K.W.; Tsang, O.T.Y.; Yip, C.C.Y.; Chan, K.H.; Wu, T.C.; Chan, J.M.C.; Leung, W.-S.; Chik, T.S.-H.; Choi, C.Y.-C.; Kandamby, D.H.; et al. Consistent Detection of 2019 Novel Coronavirus in Saliva. Clin. Infect. Dis. 2020, 71, 841–843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coronavirus Disease (COVID-19) Situation Reports. Available online: https://www.o.int/emergencies/diseases/novel-coronavirus-2019/situation-reports (accessed on 1 May 2022).
- Mina, M.J.; Andersen, K.G. COVID-19 testing: One size does not fit all. Science 2021, 371, 126–127. [Google Scholar] [CrossRef]
- Hellewell, J.; Russell, T.W.; The SAFER Investigators and Field Study Team; The Crick COVID-19 Consortium; CMMID COVID-19 Working Group; Beale, R.; Kelly, G.; Houlihan, C.; Nastouli, E.; Kucharski, A.J. Estimating the effectiveness of routine asymptomatic PCR testing at different frequencies for the detection of SARS-CoV-2 infections. BMC Med. 2021, 19, 106. [Google Scholar] [CrossRef]
- Vogels, C.B.; Brito, A.F.; Wyllie, A.L.; Fauver, J.R.; Ott, I.M.; Kalinich, C.C.; Petrone, M.E.; Casanovas-Massana, A.; Muenker, M.C.; Moore, A.J.; et al. Analytical sensitivity and efficiency comparisons of SARS-CoV-2 RT–qPCR primer–probe sets. Nat. Microbiol. 2020, 5, 1299–1305. [Google Scholar] [CrossRef]
- Lippi, G.; Simundic, A.-M.; Plebani, M. Potential preanalytical and analytical vulnerabilities in the laboratory diagnosis of coronavirus disease 2019 (COVID-19). Clin. Chem. Lab. Med. 2020, 58, 1070–1076. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- To, K.K.W.; Tsang, O.T.Y.; Leung, W.S.; Tam, A.R.; Wu, T.C.; Lung, D.C.; Yip, C.C.-Y.; Cai, J.-P.; Chan, J.M.-C.; Chik, T.S.-H.; et al. Temporal profiles of viral load in posterior oropharyngeal saliva samples and serum antibody responses during infection by SARS-CoV-2: An observational cohort study. Lancet Infect. Dis. 2020, 20, 565–574. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Detection of SARS-CoV-2 | ||
|---|---|---|
| Positive (n = 46) | Negative (n = 57) | |
| Age (median) years | 40 (18–79) | 42 (18–79) |
| Male n(%) | 29 (63.04) | 24 (42.10) |
| Symptomatic n(%) | 44 (99.65) | 34 (59.65) |
| Fever n(%) | 21 (45.65) | 11 (19.29) |
| Cough n(%) | 30 (65.21) | 16 (28.07) |
| Sore throat n(%) | 10 (21.73) | 10 (17.54) |
| Dyspnea n(%) | 15 (32.60) | 6 (10.52) |
| Headache n(%) | 24 (52.17) | 19 (33.33) |
| Myalgia n(%) | 20 (43.47) | 13 (22.80) |
| Anosmia n(%) | 7 (15.21) | 1 (1.75) |
| Diarrhea n(%) | 2 (4.34) | 10 (17.54) |
| Vomiting n(%) | 3 (6.52) | 4 (7.01) |
| SARS-CoV-2 Detection Kit | Kappa | 95% CI |
|---|---|---|
| TaqCheck (saliva) vs. Allplex (NP) | 1.0 | 1.0–1.0 |
| TaqCheck (saliva) vs. Allplex (saliva) | 1.0 | 1.0–1.0 |
| TaqCheck (saliva) vs. TaqPath (saliva) | 0.923 | 0.849–0.997 |
| Allplex (NP) vs. Allplex (saliva) | 1.0 | 1.0–1.0 |
| Allplex (NP) vs. TaqPath (saliva) | 0.923 | 0.849–0.997 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Sousa, K.A.F.; Nonaka, C.K.V.; de Ávila Mendonça, R.N.; Mascarenhas, V.N.; Weber, T.G.L.; Regis Silva, C.G.; Mendes, A.V.A.; Khouri, R.; Souza, B.S.F.; Gurgel Rocha, C.A. SARS-CoV-2 Detection via RT-PCR in Matched Saliva and Nasopharyngeal Samples Reveals High Concordance in Different Commercial Assays. Diagnostics 2023, 13, 329. https://doi.org/10.3390/diagnostics13020329
de Sousa KAF, Nonaka CKV, de Ávila Mendonça RN, Mascarenhas VN, Weber TGL, Regis Silva CG, Mendes AVA, Khouri R, Souza BSF, Gurgel Rocha CA. SARS-CoV-2 Detection via RT-PCR in Matched Saliva and Nasopharyngeal Samples Reveals High Concordance in Different Commercial Assays. Diagnostics. 2023; 13(2):329. https://doi.org/10.3390/diagnostics13020329
Chicago/Turabian Stylede Sousa, Karoline Almeida Felix, Carolina Kymie Vasques Nonaka, Renata Naves de Ávila Mendonça, Verena Neiva Mascarenhas, Thamires Gomes Lopes Weber, Carlos Gustavo Regis Silva, Ana Verena Almeida Mendes, Ricardo Khouri, Bruno Solano Freitas Souza, and Clarissa Araújo Gurgel Rocha. 2023. "SARS-CoV-2 Detection via RT-PCR in Matched Saliva and Nasopharyngeal Samples Reveals High Concordance in Different Commercial Assays" Diagnostics 13, no. 2: 329. https://doi.org/10.3390/diagnostics13020329
APA Stylede Sousa, K. A. F., Nonaka, C. K. V., de Ávila Mendonça, R. N., Mascarenhas, V. N., Weber, T. G. L., Regis Silva, C. G., Mendes, A. V. A., Khouri, R., Souza, B. S. F., & Gurgel Rocha, C. A. (2023). SARS-CoV-2 Detection via RT-PCR in Matched Saliva and Nasopharyngeal Samples Reveals High Concordance in Different Commercial Assays. Diagnostics, 13(2), 329. https://doi.org/10.3390/diagnostics13020329