
Uterine Perforation as a Complication of the Intrauterine Procedures Causing Omentum Incarceration: A Review

 , , ,
, , ,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
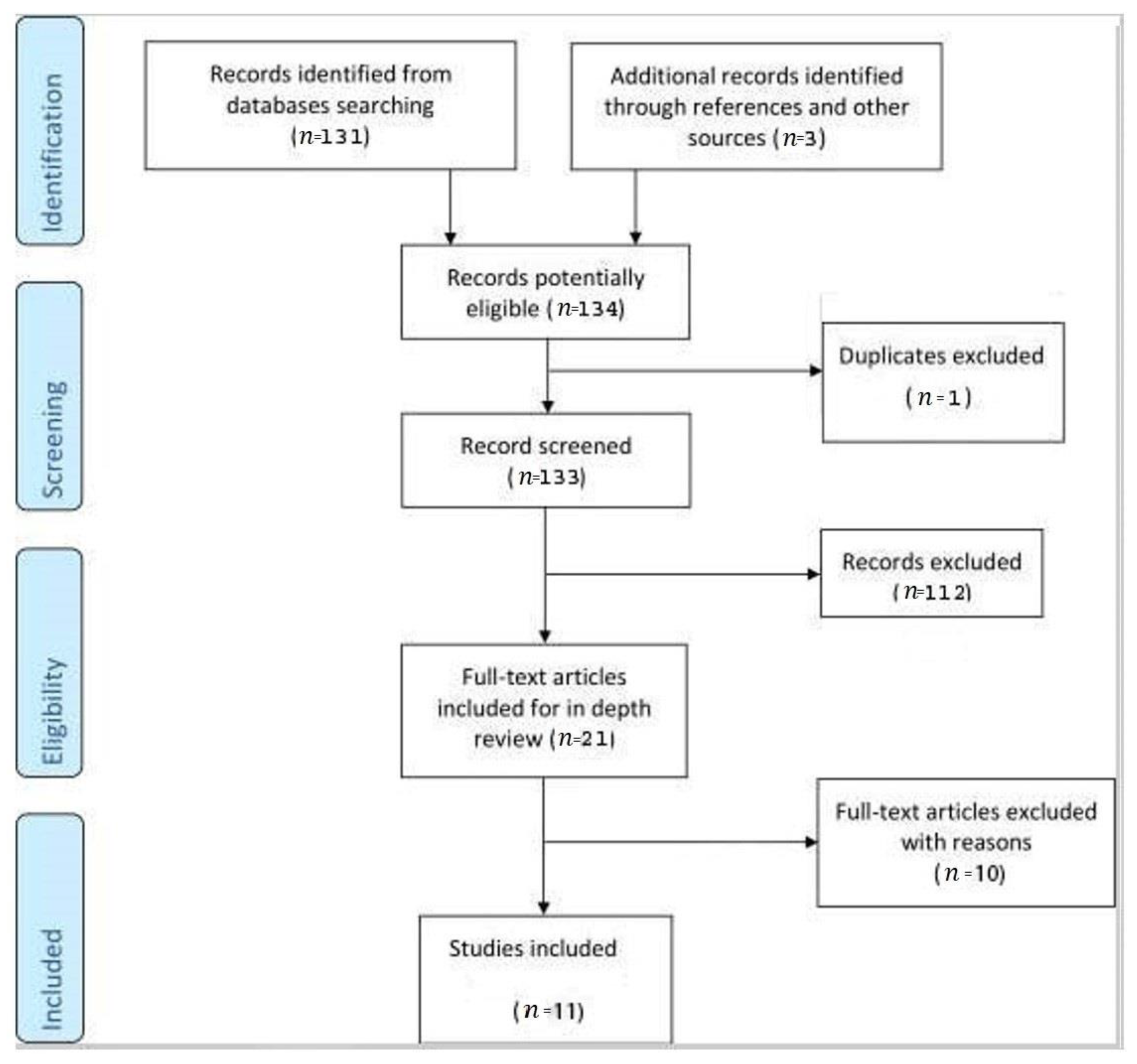
2.1. Study Selection
2.2. Data Synthesis
3. Results
4. Case Report
5. Discussion
5.1. Incidence and Risk Factors
5.2. Clinical Presentation
5.3. Imaging Examination
5.4. Timing of Diagnosis
5.5. Management
5.6. Outcome
5.7. Prevention of Uterine Perforation
5.8. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Coughlin, L.M.; Sparks, D.A.; Chase, D.M.; Smith, J. Incarcerated Small Bowel Associated with Elective Abortion Uterine Perforation. J. Emerg. Med. 2013, 44, e303–e306. [Google Scholar] [CrossRef] [PubMed]
- Augustin, G.; Majerović, M.; Luetić, T. Uterine perforation as a complication of surgical abortion causing small bowel obstruction: A review. Arch. Gynecol. Obstet. 2013, 288, 311–323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deffieux, X.; Kane, A.; Faivre, E.; Gervaise, A.; Frydman, R.; Fernandez, H. Intrauterine fallopian tube incarceration: An uncommon complication of termination of pregnancy by vacuum aspiration. Fertil. Steril. 2008, 90, 1938–1939. [Google Scholar] [CrossRef] [PubMed]
- Acharya, G.; Morgan, H.; Paramanantham, L.; Fernando, R. A randomized controlled trial comparing surgical termination of pregnancy with and without continuous ultrasound guidance. Eur. J. Obstet. Gynecol. Reprod. Biol. 2004, 114, 69–74. [Google Scholar] [CrossRef]
- Schwarzman, P.; Baumfeld, Y.; Mastrolia, S.A.; Yaniv-Salem, S.; Leron, E.; Silberstein, T. Obstetric Outcomes after Perforation of Uterine Cavity. J. Clin. Med. 2022, 11, 4439. [Google Scholar] [CrossRef]
- Alalade, A.O.; Odejinmi, F.O. Laparoscopic management of uterine perforation following surgical termination of pregnancy: A report of three cases and literature review. Gynecol. Surg. 2006, 3, 34–36. [Google Scholar] [CrossRef] [Green Version]
- Ben-Baruch, G.; Menczer, J.; Shalev, J.; Romem, Y.; Serr, D.M. Uterine perforation during curettage: Perforation rates and postperforation management. Isr. J. Med. Sci. 1980, 16, 821–824. [Google Scholar]
- Hefler, L.; Lemach, A.; Seebacher, V.; Polterauer, S.; Tempfer, C.; Reinthaller, A. The Intraoperative Complication Rate of Nonobstetric Dilation and Curettage. Obstet. Gynecol. 2009, 113, 1268–1271. [Google Scholar] [CrossRef]
- Kumar, N.P.; Rao, A.P. Laparoscopy as a Diagnostic and Therapeutic Technique in Uterine Perforations during First Trimester Abortions. Asia Ocean. J. Obstet. Gynaecol. 2010, 14, 55–59. [Google Scholar] [CrossRef]
- Kaali, S.G.; Szigetvari, I.A.; Bartfai, G.S. The frequency and management of uterine perforations during first-trimester abortions. Am. J. Obstet. Gynecol. 1989, 161, 406–408. [Google Scholar] [CrossRef]
- Royal College of Obstetricians and Gynaecologists. The Care Of Women Requesting Induced Abortion—Guideline Summary. Evidence-based Guideline No. 7. 2000. Available online: https://www.rcog.org.uk/media/wgalpxws/abortion_guideline_summary.pdf (accessed on 25 August 2022).
- Ziegler, N.; Korell, M.; Herrmann, A.; De Wilde, M.S.; La Roche, L.A.T.-D.; Larbig, A.; De Wilde, R.L. Uterine perforation following a fractional curettage successfully treated with the modified polysaccharide 4DryField® PH: A case report. J. Med Case Rep. 2016, 10, 243. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Q.; Yang, L.; Ashley, C.; Medlin, E.E.; Kushner, D.M.; Zheng, Y. Uterine rupture disguised by urinary retention following a second trimester induced abortion: A case report. BMC Women’s Health 2015, 15, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levy, B.; Falcone, T.; Chakrabarti, A. Uterine Perforation During Gynecologic Procedures; Post, T.W., Ed.; UpToDate, Uptodate Inc.: Waltham, MA, USA; Available online: https://www.medilib.ir/uptodate/show/3309 (accessed on 15 September 2022).
- Lancet, T. Abortion: Access and safety worldwide. Lancet 2018, 391, 1121. [Google Scholar] [CrossRef] [PubMed]
- Ganatra, B.; Tuncalp, O.; Johnston, H.B.; Johnson, B.R., Jr.; Gulmezoglu, A.M.; Temmerman, M. From concept to measurement: Operationalizing WHO’s definition of unsafe abortion. Bull. World Health Organ. 2014, 92, 155. [Google Scholar] [CrossRef] [PubMed]
- Pradana, A. Severe Complication of Uterine Perforation and Ileum Prolapse after Having Unsafe Abortion. Indones. J. Obstet. Gynecol. 2012, 36, 150–153. [Google Scholar] [CrossRef]
- Su, S.; Tao, G.; Dong, B.; Shi, L.; Dong, J. Delayed presentation of uterine perforation with ovary migration after dilatation and curettage. Int. J. Clin. Exp. Med. 2015, 8, 6311–6314. [Google Scholar]
- Dignac, A.; Novellas, S.; Fournol, M.; Caramella, T.; Bafghi, A.; Chevallier, P. Incarceration of the appendix complicating a uterine perforation following surgical abortion: CT aspects. Emerg. Radiol. 2008, 15, 267–269. [Google Scholar] [CrossRef]
- Alanbay, I.; DeDe, M.; Karasahin, E.; Üstün, Y.; Yenen, M.C.; Başer, I. Herniation of fallopian tube through perforated uterine wall during previous first trimester surgical abortion in an infertile patient. J. Obstet. Gynaecol. Res. 2009, 35, 997–999. [Google Scholar] [CrossRef]
- Cremieu, H.; Rubod, C.; Oukacha, N.; Poncelet, E.; Lucot, J.-P. À propos de deux cas d’incarcérations endo-utérines post-curetage aspiratif: Diagnostic et prise en charge. J. Gynécologie Obs. Biol. Reprod. 2012, 41, 387–392. [Google Scholar] [CrossRef]
- Damiani, G.R.; Tartagni, M.; Crescini, C.; Persiani, P.; Loverro, G.; Von Wunster, S. Intussusception and Incarceration of a Fallopian Tube: Report of 2 Atypical Cases, with Differential Considerations, Clinical Evaluation, and Current Management Strategies. J. Minim. Invasive Gynecol. 2011, 18, 246–249. [Google Scholar] [CrossRef]
- Trio, C.; Recalcati, D.; Sina, F.; Fruscio, R. Intrauterine fallopian tube incarceration after vacuum aspiration for pregnancy termination. Int. J. Gynecol. Obstet. 2010, 108, 157–158. [Google Scholar] [CrossRef]
- Alkhateeb, H.M.; Yaseen, E.M. Twin pregnancy in an accessory cavitated non-communicating uterus. Int. J. Surg. Case Rep. 2015, 10, 45–48. [Google Scholar] [CrossRef] [PubMed]
- Kim, M. Incarcerated Omentum with Tamponade Effect in the Uterine Perforation Scar after Dilation and Curettage: A Case Report. J. Med. Cases 2014, 5, 204–207. [Google Scholar] [CrossRef]
- Koshiba, A.; Koshiba, H.; Noguchi, T.; Iwasaku, K.; Kitawaki, J. Uterine perforation with omentum incarceration after dilatation and evacuation/curettage: Magnetic resonance imaging findings. Arch. Gynecol. Obstet. 2011, 285, 887–890. [Google Scholar] [CrossRef] [PubMed]
- La, S.; Mizia, K.; Arrage, N.; Kapurubandara, S. A delayed case of uterine perforation with omental adhesions. Gynecol. Minim. Invasive Ther. 2021, 10, 174. [Google Scholar] [CrossRef] [PubMed]
- Leibner, E.C. Delayed Presentation of Uterine Perforation. Ann. Emerg. Med. 1995, 26, 643–646. [Google Scholar] [CrossRef] [PubMed]
- Marsden, D.E. Omentum Presenting at the Vulva after a Normal Labor and Delivery. Acta Obstet. Gynecol. Scand. 1984, 63, 277–278. [Google Scholar] [CrossRef]
- Nam, G.; Lee, S.R.; Ko, Y.R.; Kim, G.J. Omental Incarceration over Twenty Years Presenting as a Hyperechoic Endometrial Mass in a Postmenopausal Woman. J. Menopausal Med. 2021, 27, 46–48. [Google Scholar] [CrossRef]
- Nayak, P.K.; Mitra, S.; Padma, A.; Agrawal, S. Late Presentation of Unsafe Abortion after 5 Years of Procedure. Case Rep. Obstet. Gynecol. 2014, 2014, 456017. [Google Scholar] [CrossRef] [Green Version]
- Sedrati, A.; Wong, A.J.; Alonso, L.; Carugno, J. Diagnosis and Management of Uterine Perforation with Omental Incarceration after Dilation and Curettage. J. Minim. Invasive Gynecol. 2022, 29, 1028–1029. [Google Scholar] [CrossRef]
- Chandi, A.; Jain, S.; Yadav, S.; Gurawalia, J. Vaginal evisceration as rare but a serious obstetric complication: A case series. Case Rep. Women’s Health 2016, 10, 4–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ozaki, K.; Suzuki, S. Uterine perforation with omentum incarceration after dilatation and evacuation/curettage. Arch. Gynecol. Obstet. 2013, 287, 607–608. [Google Scholar] [CrossRef]
- Kakinuma, T.; Kakinuma, K.; Sakamoto, Y.; Kawarai, Y.; Saito, K.; Ihara, M.; Matsuda, Y.; Sato, I.; Ohwada, M.; Yanagida, K.; et al. Safety and efficacy of manual vacuum suction compared with conventional dilatation and sharp curettage and electric vacuum aspiration in surgical treatment of miscarriage: A randomized controlled trial. BMC Pregnancy Childbirth 2020, 20, 695. [Google Scholar] [CrossRef]
- Osser, O.V.; Valentin, L. Clinical Importance of Appearance of Cesarean Hysterotomy Scar at Transvaginal Ultrasonography in Nonpregnant Women. Obstet. Gynecol. 2011, 117, 525–532. [Google Scholar] [CrossRef] [PubMed]
- Steinauer, J.; Barbieri, R.; Chakrabarti, A. Overview of Pregnancy Termination. Available online: https://www.uptodate.com/contents/overview-of-pregnancy-termination (accessed on 10 September 2022).
- Shakir, F.; Diab, Y.; Mrcog, F.S.M.B. The perforated uterus. Obstet. Gynaecol. 2013, 15, 256–261. [Google Scholar] [CrossRef]
- Shulman, S.G.; Bell, C.L.; Hampf, F.E. Uterine perforation and small bowel incarceration: Sonographic and surgical findings. Emerg. Radiol. 2006, 13, 43–45. [Google Scholar] [CrossRef] [PubMed]
- Boyon, C.; Giraudet, G.; Du Masgenêt, B.G.; Lucot, J.-P.; Goeusse, P.; Vinatier, D. Diagnostic et priseen charge des perforations utérines par dispositif intra-utérin: À partir de 11 cas. Gynécologie Obs. Fertil. 2013, 41, 314–321. [Google Scholar] [CrossRef]
- Rowlands, S.; Oloto, E.; Horwell, D. Intrauterine devices and risk of uterine perforation: Current perspectives. Open Access J. Contracept. 2016, 7, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Rodgers, S.K.; Kirby, C.L.; Smith, R.J.; Horrow, M.M. Imaging after Cesarean Delivery: Acute and Chronic Complications. Radiographics 2012, 32, 1693–1712. [Google Scholar] [CrossRef]
- Aboughalia, H.; Basavalingu, D.; Revzin, M.V.; Sienas, L.E.; Katz, D.S.; Moshiri, M. Imaging evaluation of uterine perforation and rupture. Abdom. Imaging 2021, 46, 4946–4966. [Google Scholar] [CrossRef]
- Jiang, L.; Wu, J.; Feng, X. The value of ultrasound in diagnosis of pneumoperitoneum in emergent or critical conditions: A meta-analysis. Hong Kong J. Emerg. Med. 2019, 26, 111–117. [Google Scholar] [CrossRef] [Green Version]
- Paspulati, R.M.; Dalal, T.A. Imaging of Complications Following Gynecologic Surgery. Radiographics 2010, 30, 625–642. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.Y.; Shin, J.H.; Kim, J.; Yoon, H.-K.; Ko, G.-Y.; Won, H.-S.; Gwon, D.I.; Kim, J.H.; Cho, K.S.; Sung, K.-B. Primary Postpartum Hemorrhage: Outcome of Pelvic Arterial Embolization in 251 Patients at a Single Institution. Radiology 2012, 264, 903–909. [Google Scholar] [CrossRef] [PubMed]
- Ganguli, S.; Stecker, M.; Pyne, D.; Baum, R.A.; Fan, C.-M. Uterine Artery Embolization in the Treatment of Postpartum Uterine Hemorrhage. J. Vasc. Interv. Radiol. 2011, 22, 169–176. [Google Scholar] [CrossRef]
- Sugai, S.; Nonaka, T.; Tamegai, K.; Sato, T.; Haino, K.; Enomoto, T.; Nishijima, K. Successful repeated uterine artery embolization in postpartum hemorrhage with disseminated intravascular coagulation: A case report and literature review. BMC Pregnancy Childbirth 2021, 21, 710. [Google Scholar] [CrossRef]
- Maheux-Lacroix, S.; Lemyre, M.; Laberge, P.Y.; Lamarre, A.; Bujold, E. Uterine Artery Embolization Complicated by Uterine Perforation at the Site of Previous Myomectomy. J. Minim. Invasive Gynecol. 2012, 19, 128–130. [Google Scholar] [CrossRef] [PubMed]
- Maebayashi, A.; Kato, K.; Hayashi, N.; Nagaishi, M.; Kawana, K. Importance of abdominal X-ray to confirm the position of levonorgestrel-releasing intrauterine system: A case report. World J. Clin. Cases 2022, 10, 4904–4910. [Google Scholar] [CrossRef]
- Tchuenkam, L.W.; Mbonda, A.N.; Tochie, J.N.; Mbem-Ngos, P.P.; Noah-Ndzie, H.G.; Bang, G.A. Transvaginal strangulated bowel evisceration through uterine perforation due to unsafe abortion: A case report and literature review. BMC Women’s Health 2021, 21, 98. [Google Scholar] [CrossRef]
- Cholkeri-Singh, A.; Sasaki, K.J. Hysteroscopy safety. Curr. Opin. Obstet. Gynecol. 2016, 28, 250–254. [Google Scholar] [CrossRef]
- Vecchio, R.; Marchese, S.; Leanza, V.; Leanza, A.; Intagliata, E. Totally Laparoscopic Repair of an Ileal and Uterine Iatrogenic Perforation Secondary to Endometrial Curettage. Int. Surg. 2015, 100, 244–248. [Google Scholar] [CrossRef] [Green Version]
- Cai, Y.-Q.; Liu, W.; Zhang, H.; He, X.-Q.; Zhang, J. Laparoscopic repair of uterine rupture following successful second vaginal birth after caesarean delivery: A case report. World J. Clin. Cases 2020, 8, 2855–2861. [Google Scholar] [CrossRef] [PubMed]
- Akdemir, A.; Cirpan, T. Iatrogenic uterine perforation and bowel penetration using a Hohlmanipulator: A case report. Int. J. Surg. Case Rep. 2014, 5, 271–273. [Google Scholar] [CrossRef] [PubMed]
- Sahoo, S.P.; Dora, A.K.; Harika, M.; Kumar, K.R. Spontaneous Uterine Perforation Due to Pyometra Presenting as Acute Abdomen. Indian J. Surg. 2011, 73, 370–371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heinemann, K.; Reed, S.; Moehner, S.; Minh, T.D. Risk of uterine perforation with levonorgestrel-releasing and copper intrauterine devices in the European Active Surveillance Study on Intrauterine Devices. Contraception 2015, 91, 274–279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seol, H.J.; Tong, S.Y.; Ki, K.-D. Secondary missed abdominal pregnancy due to iatrogenic uterine perforation: A case report. Clin. Exp. Obstet. Gynecol. 2012, 39, 376–378. [Google Scholar]
- Núñez, J.H.; Díaz, A.A.; Ndwambi, N.M.; Martínez, F.L. Ectopic abdominal pregnancy due to uterine perforation after an attempt to terminate pregnancy: A case presentation. Medwave 2017, 17, e7000. [Google Scholar] [CrossRef]
- Ruiter, L.; Kazemier, B.M.; Mol, B.W.; Pajkrt, E. Incidence and recurrence rate of postpartum hemorrhage and manual removal of the placenta: A longitudinal linked national cohort study in The Netherlands. Eur. J. Obstet. Gynecol. Reprod. Biol. 2019, 238, 114–119. [Google Scholar] [CrossRef]
- Choi, M.J.; Lim, C.M.; Jeong, D.; Jeon, H.-R.; Cho, K.J.; Kim, S.Y. Efficacy of intraoperative wireless ultrasonography for uterine incision among patients with adherence findings in placenta previa. J. Obstet. Gynaecol. Res. 2020, 46, 876–882. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Authors | Year | Study Type | Age 1 | Gravida/ Para | Pregnancy Status 2 | Risk Factors | Imaging | Time from the D&Cto Diagnosis 3 |
|---|---|---|---|---|---|---|---|---|
| Alkhateeb et al. [24] | 2015 | CR | 20 | G2P1 | 13w | Twin pregnancy | US | At the moment of curettage |
| Chandi et al. [33] | 2016 | CS | 24 | G2P1 | YES | Unsafe abortion | NO | 2 days |
| 26 | G3P2 | YES | Abortion | NO | 7 h | |||
| Myounghwan [25] | 2014 | CR | 26 | G2P1 | 11w | Abortion | US, CT | Immediate after the curettage |
| Koshiba et al. [26] | 2011 | CR | 31 | G4P3 | 17w | C-S | US, MRI | 28 days |
| La et al. [27] | 2021 | CR | 26 | G3P1 | YES miscarriage | C-S | US | 3 months |
| Leibner et al. [28] | 1995 | CR | 30 | G3P1 | first-trimester | Abortion | Rx | 17 days |
| Marsden et al. [29] | 1984 | CR | 25 | G4P1 | first-trimester | Abortion | NA | Immediate after birth |
| Nam et al. [30] | 2021 | CR | 57 | G2P2 | No | D&C | US | 28 days |
| Nayak et al. [31] | 2013 | CR | 32 | G3P2 | No | Unsafe abortion | US | 5 years |
| Ozaki et al. [34] | 2013 | LE | 28 | G2P0 | 16w | D&C | US | 2 years |
| Sedrati et al. [32] | 2022 | CR | 36 | G3P2 | NA | D&C for Incomplete Miscarriage | US | 7 months |
| Symptoms | Anamnesis | History of Intrauterine Applied Procedures | Clinic Examination | Imaging | |
|---|---|---|---|---|---|
| Alkhateebet al. [24] | - Lower abdominal pain | - 3 months later | - 3 consecutive D&C | - The omental tissue pulled out through the vagina | - Pelvic US: miscarriage 13 weeks of gestation |
| Chandiet al. [33] | - Vaginal bleeding | - Dai handling following spontaneous incomplete abortion | - Small gut along with omentum coming out of introitus | NA | |
| - Lower abdominal pain - Vaginal bleeding | - D&C 7hours previous | - The abdomen was soft, and the uterus corresponded 14 weeks in size Omentum was seen coming out through the os | NA | ||
| Myounghwan [25] | - Lower abdominal pain | - Uterine perforation during D&C | - Diffuse abdominal tenderness and rebound tenderness | - CT: no evidence of bowel injury except hematoma around the perforation scar | |
| Koshibaet al. [26] | - Lower abdominal pain - Vaginal bleeding | - D&C for a missed abortion | - MRI: fatty mass | ||
| La et al. [27] | - Vaginal bleeding - Lower abdominal pain. | - 3 months later | - Two consecutive D&C | - US: omentum embedded into the myometrium suggestive of a previous uterine perforation | |
| Leibneret al. [28] | - Upper abdominal pain - Nausea and vomiting (for two weeks’ duration). | - 1 day later | - Vacuum aspiration termination of pregnancy | - Radiographs of the chest and abdomen—ileus or partial small-bowel obstruction without evidence of free air | |
| Marsden et al. [29] | - 3 consecutive D&C | - Fatty tissue protruding from the cervical os following vaginal delivery | NA | ||
| Nam et al. [30] | - Abdominal pain - Menopausal vaginal bleeding | - No regular check-ups - Only Pap smears | - D&C 23 years ago for abnormal uterine bleeding | - US: a hyperechoic round mass with a thick band-like structure penetrating the uterine wall and blood vessels in it on colour Doppler exam | |
| Nayak et al. [31] | - Lower abdominal pain | - Abortion 5 years earlierafter4months of pregnancy | - The foreign body was hanging from the introitus | - US: a tubular and slender foreign body coiled up in the pelvis and probably in the uterine cavity | |
| Ozaki et al. [34] | - Asymptomatic - Referred to a hospital at 16 weeks gestation for a high-risk obstetric consultation | - 2 years later | - D&C | - US: a hyperechogenic structure in the anterior wall of the uterine body with suspected incarceration of the omentum or mesenteric fat | |
| Sedratiet al. [32] | - Amenorrhea - Lower abdominal pain for seven months post-operatively. | - D&C for incomplete miscarriage | - US: discontinuity in the uterine serosa with a hyperechoic mass protruding from the peritoneal cavity into the myometrium suggesting an incarcerated pelvic organ |
| Surgical Approach | Intraoperative Findings | Management | |
|---|---|---|---|
| Alkhateeb et al. [24] | - Laparotomy | - Uterine perforation at the fundus with the omentum pulled in through the perforation | - The omentum was drawn out of the uterus, transfixed, ligated by suture and trimmed. - Uterus perforation was sutured. |
| Chandi et al. [33] | Case 1 | - A rent of 7 × 3 cm was present in the lower uterine segment’s anterior wall of the uterus. | - Resection of the 20 cm of ileum and caecum was done, and ileo-ascending colon end-to-end anastomosis was performed. - 2 units of whole blood and 1 unit of FFP were transfused intraoperatively, and two units of FFP post-operatively. - Uterus perforation was sutured. |
| Chandi et al. [33] | Case 2 | - Hemoperitoneum of 200 cm3 - A rent of 5 cm was present in the anterior uterine wall in the lower uterine segment extending to the left laterally and downwards to the vagina. - Utero-vesical pouch was already breached. - The bladder wall was intact. -Fetal skull was removed from the UV pouch. - B/L tubes and ovaries were standard. - The gut and bladder were normal. | |
| Myounghwan [25] | - Laparoscopy | - Perforation scar of the uterine fundus | - Incarcerated omentum was incarcerated. - Suture at the perforation site - 4 units of packed red blood cells were transfused. |
| Koshiba et al. [26] | - Laparotomy | - Uterine perforation distant from the previous cesarean scar | - Dissection of the omental loop. - Uterine perforation was sutured. |
| La et al. [27] | - Laparoscopy | - Fundal defect | - Omentum was released. - The uterus defect was sutured. |
| Leibner et al. [28] | - Laparotomy | - 2 perforations of the body of the uterus 1 cm (one contained herniated omentum). - A strangulated 5-cm segment of the extrauterine small bowel with complete obstruction at this level. | - The ischemic segment of the bowel was resected with immediate end-to-end anastomosis. - The uterus was not repaired. |
| Marsden et al. [29] | - Laparotomy | - A portion of the greater omentum passed into the myometrium at the right corm of the uterus. | - Gentle traction was used to remove the omentum from the uterine cavity. - Uterine perforation was sutured. |
| Nam et al. [30] | - Office hysteroscopy | - A pale-yellowish mass with intrauterine adhesions was observed. | - Laparoscopic and hysteroscopic resection of the incarcerated omentum. - Uterine perforation was sutured. |
| - Laparoscopy | - An incarcerated omentum into the fundus of the uterine cavity through the uterine perforation site was noticed | ||
| Nayak et al. [31] | - Cystoscopy | - Excluded bladder involvement | |
| - Hysteroscopy | - Showed that the tube had pierced through the posterior wall of the uterus - There were no intrauterine adhesions. | ||
| - Laparoscopy | - Ryle’s tube had perforated the uterus through the posterior fundal wall. - Bowel and omental loops were adherents to the entire length of the intra-abdominal portion of the tube. | ||
| - Laparotomy | - Adhesiolysis and the freed tube was dragged out vaginally - Suture of the uterine fundus perforation -Bilateral tubectomy | ||
| Ozaki et al. [34] | -C-S | - Omentum was incarcerated in the anterior wall of the uterine body | - The omental loop was dissected. |
| Sedrati et al. [32] | - Hysteroscopy | - Severe intrauterine adhesions | - The omentum was excised. |
| - Laparoscopy | - Omental incarceration | - The uterine serosa was sutured. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zorilă, G.L.; Căpitănescu, R.G.; Drăgușin, R.C.; Istrate-Ofițeru, A.-M.; Bernad, E.; Dobie, M.; Bernad, S.; Craina, M.; Ceaușu, I.; Marinaş, M.C.; et al. Uterine Perforation as a Complication of the Intrauterine Procedures Causing Omentum Incarceration: A Review. Diagnostics 2023, 13, 331. https://doi.org/10.3390/diagnostics13020331
Zorilă GL, Căpitănescu RG, Drăgușin RC, Istrate-Ofițeru A-M, Bernad E, Dobie M, Bernad S, Craina M, Ceaușu I, Marinaş MC, et al. Uterine Perforation as a Complication of the Intrauterine Procedures Causing Omentum Incarceration: A Review. Diagnostics. 2023; 13(2):331. https://doi.org/10.3390/diagnostics13020331
Chicago/Turabian StyleZorilă, George Lucian, Răzvan Grigoraș Căpitănescu, Roxana Cristina Drăgușin, Anca-Maria Istrate-Ofițeru, Elena Bernad, Mădălina Dobie, Sandor Bernad, Marius Craina, Iuliana Ceaușu, Marius Cristian Marinaş, and et al. 2023. "Uterine Perforation as a Complication of the Intrauterine Procedures Causing Omentum Incarceration: A Review" Diagnostics 13, no. 2: 331. https://doi.org/10.3390/diagnostics13020331
APA StyleZorilă, G. L., Căpitănescu, R. G., Drăgușin, R. C., Istrate-Ofițeru, A. -M., Bernad, E., Dobie, M., Bernad, S., Craina, M., Ceaușu, I., Marinaş, M. C., Comănescu, M. -C., Zorilă, M. V., Drocaș, I., Berbecaru, E. I. A., & Iliescu, D. G. (2023). Uterine Perforation as a Complication of the Intrauterine Procedures Causing Omentum Incarceration: A Review. Diagnostics, 13(2), 331. https://doi.org/10.3390/diagnostics13020331