
Omicron in Infants—Respiratory or Digestive Disease?

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Methods
3. Results
3.1. General Data Analysis for the Whole Study Group On
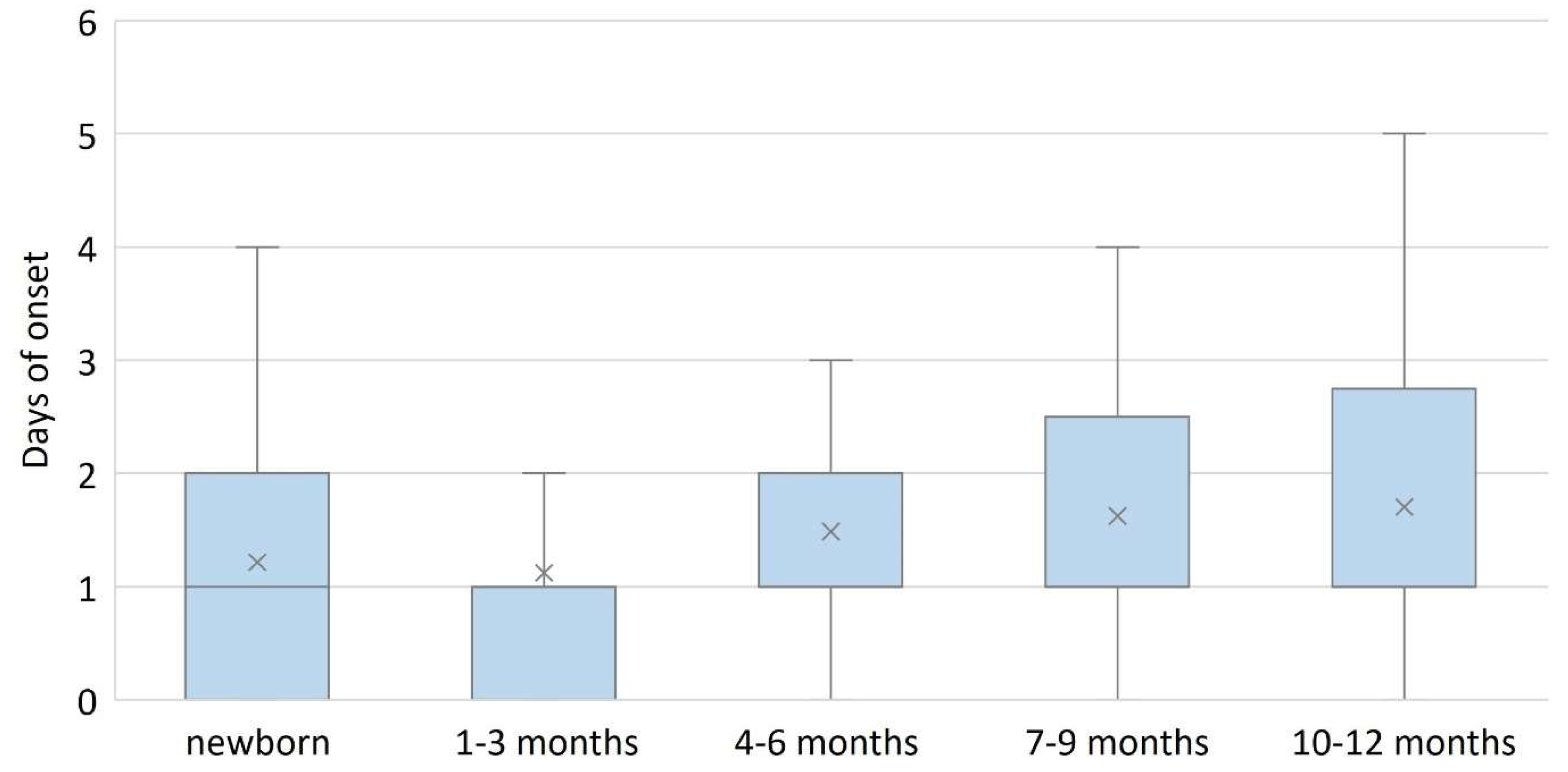
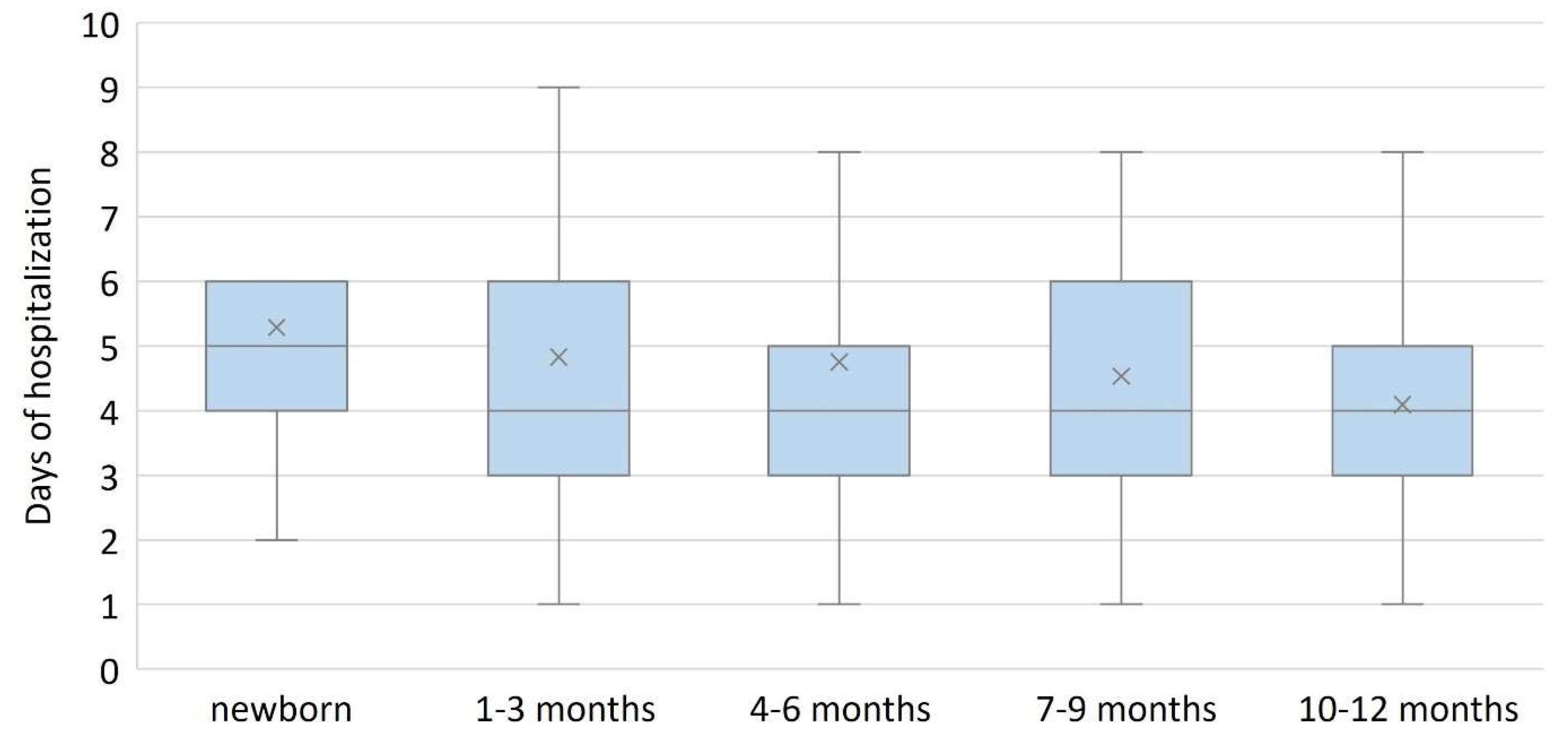
3.2. Data Analysis by Age Group
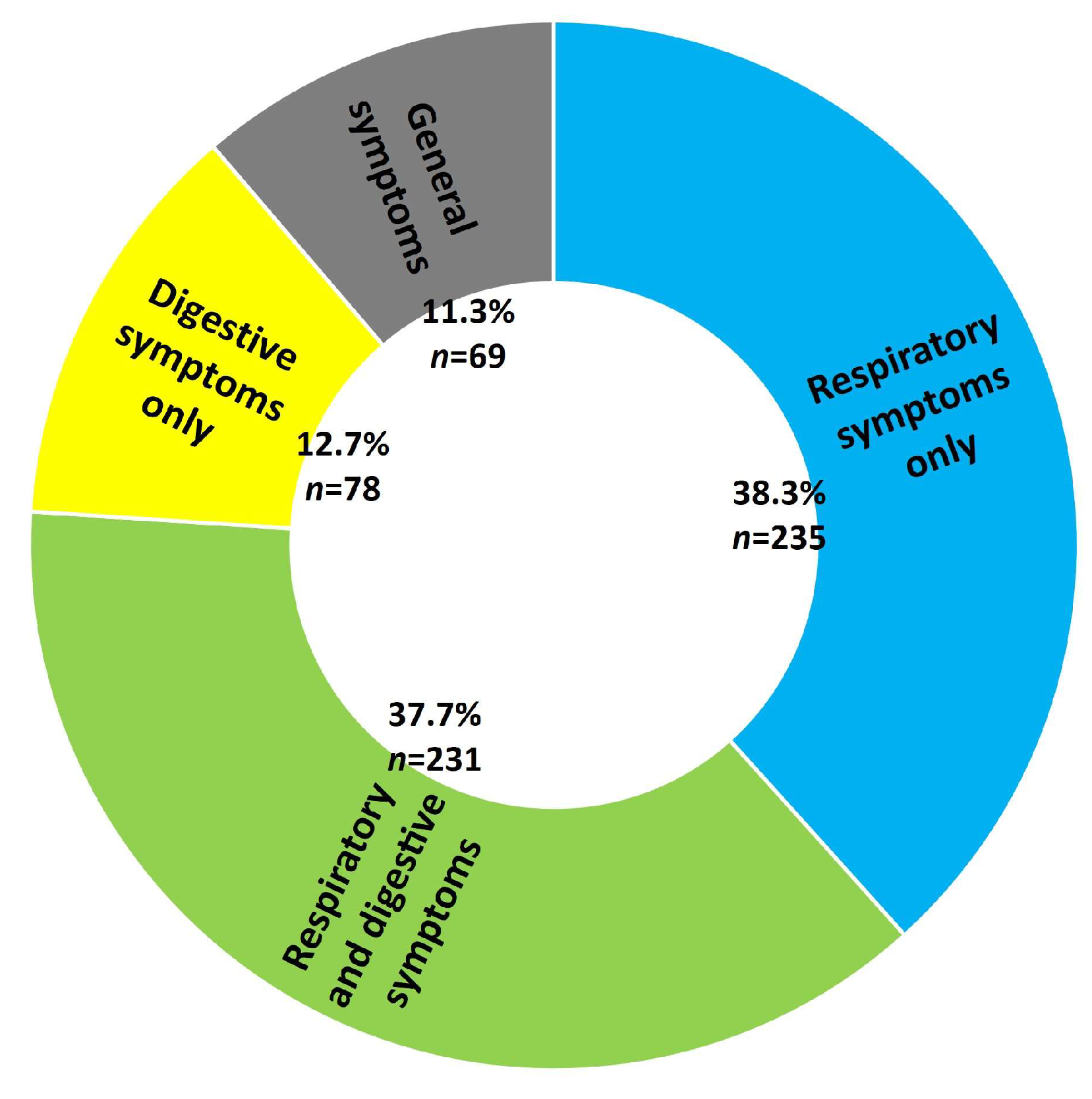
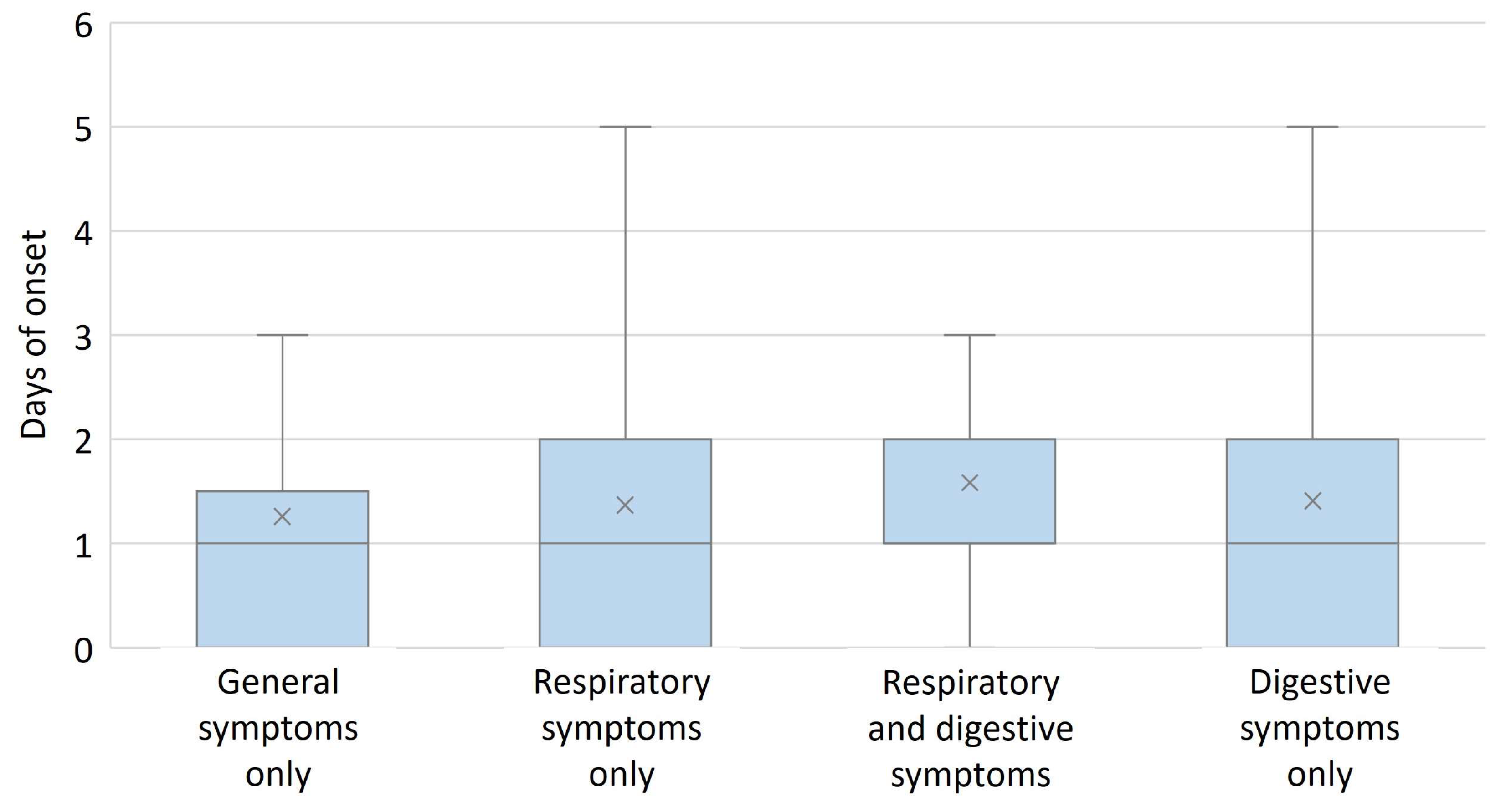
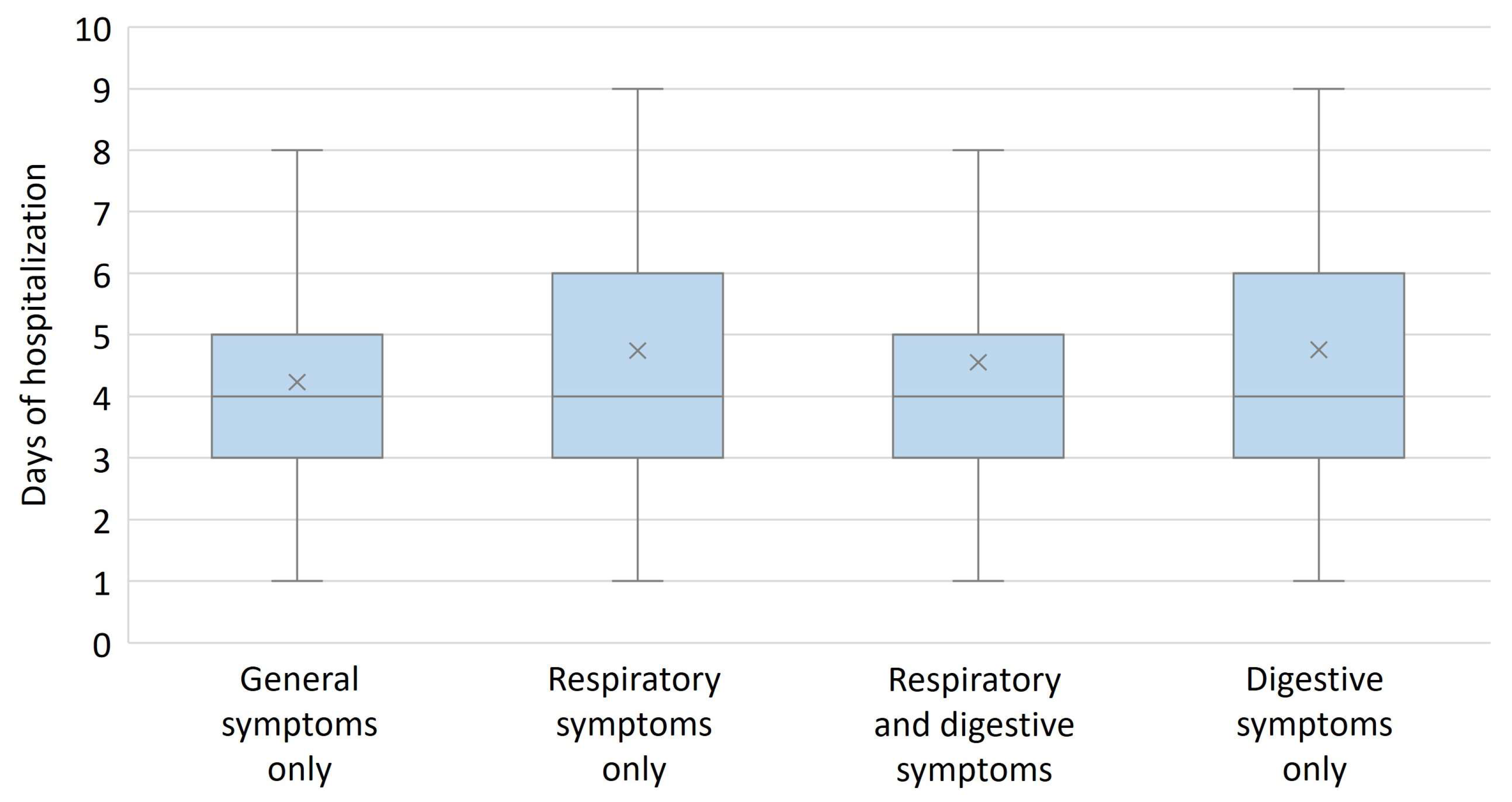
3.3. Analysis of Data by Type of Symptoms
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stringer, M.D. Anatomy of the Infant and Child. J. Pediatr. Surg. Gen. Princ. Newborn Surg. 2020, 83–101. [Google Scholar]
- Phillips, B. Neonates are not little children. Arch. Dis. Child. 2019, 104, 1013. [Google Scholar] [CrossRef]
- Miron, V.D.; Banica, L.; Sandulescu, O.; Paraschiv, S.; Surleac, M.; Florea, D.; Vlaicu, O.; Milu, P.; Streinu-Cercel, A.; Bilașco, A.; et al. Clinical and molecular epidemiology of influenza viruses from Romanian patients hospitalized during the 2019/20 season. PLoS ONE 2021, 16, e0258798. [Google Scholar] [CrossRef] [PubMed]
- Hall, C.B.; Weinberg, G.A.; Blumkin, A.K.; Edwards, K.M.; Staat, M.A.; Schultz, A.F.; Iwane, M.K. Respiratory syncytial virus-associated hospitalizations among children less than 24 months of age. Pediatrics 2013, 132, e341–e348. [Google Scholar] [CrossRef]
- McLaughlin, J.M.; Khan, F.; Schmitt, H.-J.; Agosti, Y.; Jodar, L.; Simões, E.A.F.; Swerdlow, D.L. Respiratory Syncytial Virus–Associated Hospitalization Rates among US Infants: A Systematic Review and Meta-Analysis. J. Infect. Dis. 2020, 225, 1100–1111. [Google Scholar] [CrossRef] [PubMed]
- Săndulescu, O. COVID-19 and cold season preparedness. Germs 2020, 10, 149. [Google Scholar] [CrossRef] [PubMed]
- Cruz, A.T.; Zeichner, S.L. COVID-19 in Children: Initial Characterization of the Pediatric Disease. Pediatrics 2020, 145, e20200834. [Google Scholar] [CrossRef] [Green Version]
- Swann, O.V.; Pollock, L.; Holden, K.A.; Munro, A.P.S.; Bennett, A.; Williams, T.C.; Turtle, L.; Fairfield, C.J.; Drake, T.M.; Faust, S.N.; et al. Comparison of UK paediatric SARS-CoV-2 admissions across the first and second pandemic waves. Pediatr Res. 2022, 1–10. [Google Scholar] [CrossRef]
- Nijman, R.G. The impact of the COVID-19 pandemic on child health. J. Lab. Med. 2021, 45, 249–258. [Google Scholar] [CrossRef]
- Perra, N. Non-pharmaceutical interventions during the COVID-19 pandemic: A review. Phys. Rep. 2021, 913, 1–52. [Google Scholar] [CrossRef]
- Miron, V.D. COVID-19 in the pediatric population and parental perceptions. Germs 2020, 10, 294. [Google Scholar] [CrossRef] [PubMed]
- Taylor, L. COVID-19: Omicron drives weekly record high in global infections. BMJ 2022, 376, o66. [Google Scholar] [CrossRef] [PubMed]
- Marks, K.J.; Whitaker, M.; Agathis, N.T.; Anglin, O.; Milucky, J.; Patel, K.; Pham, H.; Kirley, P.D.; Kawasaki, B.; Meek, J.; et al. Hospitalization of Infants and Children Aged 0-4 Years with Laboratory-Confirmed COVID-19—COVID-NET, 14 States, March 2020-February 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 429–436. [Google Scholar] [CrossRef]
- Vladescu, C.; Ciutan, M.; Rafila, A. In-hospital admissions and deaths in the context of the COVID-19 pandemic, in Romania. Germs 2022, 12, 169–179. [Google Scholar] [CrossRef]
- Streinu-Cercel, A.; Apostolescu, C.; Săndulescu, O.; Oţelea, D.; Streinu-Cercel, A.; Vlaicu, O.; Paraschiv, S.; Benea, O.E.; Bacruban, R.; Niţescu, M.; et al. SARS-CoV-2 in Romania—Analysis of the first confirmed case and evolution of the pandemic in Romania in the first three months. Germs 2020, 10, 132–134. [Google Scholar] [CrossRef] [PubMed]
- Streinu-Cercel, A.; Sandulescu, O.; Miron, V.D.; Paraschiv, S.; Casangiu, C.; Hohan, R.; Bănică, L.; Surleac, M.; Streinu-Cercel, A. Undetected Omicron Transmission in Romania-Report of the First Detected Case of Locally Acquired Omicron Infection and Complete Epidemiological Investigation. Diagnostics 2022, 12, 348. [Google Scholar] [CrossRef] [PubMed]
- Centrul Naţional de Supraveghere şi Control al Bolilor Transmisibile. COVID-19 Raport săptămânal de Supraveghere—Date Raportate până la Data de 11 Decembrie 2022. Available online: https://www.cnscbt.ro/index.php/analiza-cazuri-confirmate-covid19/3370-raport-saptamanal-episaptamana49-2022 (accessed on 17 December 2022).
- Maniu, I.; Maniu, G.; Totan, M. Clinical and Laboratory Characteristics of Pediatric COVID-19 Population—A Bibliometric Analysis. J. Clin. Med. 2022, 11, 5987. [Google Scholar] [CrossRef]
- Cloete, J.; Kruger, A.; Masha, M.; du Plessis, N.M.; Mawela, D.; Tshukudu, M.; Manyane, T.; Komane, L.; Venter, M.; Jassat, W.; et al. Paediatric hospitalisations due to COVID-19 during the first SARS-CoV-2 omicron (B.1.1.529) variant wave in South Africa: A multicentre observational study. Lancet Child Adolesc. Health 2022, 6, 294–302. [Google Scholar] [CrossRef]
- Torjesen, I. COVID-19: Omicron variant is linked to steep rise in hospital admissions of very young children. BMJ 2022, 376, o110. [Google Scholar] [CrossRef] [PubMed]
- Kozlov, M. Does Omicron hit kids harder? Nature 2022. [Google Scholar] [CrossRef]
- Bhuiyan, M.U.; Stiboy, E.; Hassan, M.Z.; Chan, M.; Islam, M.S.; Haider, N.; Jaffe, A.; Homaira, N. Epidemiology of COVID-19 infection in young children under five years: A systematic review and meta-analysis. Vaccine 2021, 39, 667–677. [Google Scholar] [CrossRef] [PubMed]
- Khemiri, H.; Ayouni, K.; Triki, H.; Haddad-Boubaker, S. SARS-CoV-2 infection in pediatric population before and during the Delta (B.1.617.2) and Omicron (B.1.1.529) variants era. Virol. J. 2022, 19, 144. [Google Scholar] [CrossRef] [PubMed]
- Sobolewska-Pilarczyk, M.; Pokorska-Śpiewak, M.; Stachowiak, A.; Marczyńska, M.; Talarek, E.; Ołdakowska, A.; Kucharek, I.; Sybilski, A.; Mania, A.; Figlerowicz, M.; et al. COVID-19 infections in infants. Sci. Rep. 2022, 12, 7765. [Google Scholar] [CrossRef] [PubMed]
- Ryu, B.-H.M.; Hong, S.I.M.; Lim, S.J.M.; Cho, Y.; Hong, K.-W.M.; Bae, I.-G.M.; Cho, O.-H.M. Features of COVID-19 among Children and Adolescents without Risk Factors before and after the Delta Variant Outbreak in South Korea. Pediatr. Infect. Dis. J. 2022, 41, e34–e35. [Google Scholar] [CrossRef]
- Nikolopoulou, G.B.; Maltezou, H.C. COVID-19 in Children: Where do we Stand? Arch. Med. Res. 2022, 53, 1–8. [Google Scholar] [CrossRef]
- Götzinger, F.; Santiago-García, B.; Noguera-Julián, A.; Lanaspa, M.; Lancella, L.; Carducci, F.; Gabrovska, N.; Velizarova, S.; Prunk, P.; Osterman, V.; et al. COVID-19 in children and adolescents in Europe: A multinational, multicentre cohort study. Lancet Child. Adolesc. Health 2020, 4, 653–661. [Google Scholar] [CrossRef]
- King, J.A.; Whitten, T.A.; Bakal, J.A.; McAlister, F.A. Symptoms associated with a positive result for a swab for SARS-CoV-2 infection among children in Alberta. CMAJ 2021, 193, E1–E9. [Google Scholar] [CrossRef]
- Zachariah, P.; Johnson, C.L.; Halabi, K.C.; Ahn, D.; Sen, A.I.; Fischer, A.; Banker, S.L.; Giordano, M.; Manice, C.S.; Diamond, R.; et al. Epidemiology, Clinical Features, and Disease Severity in Patients With Coronavirus Disease 2019 (COVID-19) in a Children’s Hospital in New York City, New York. JAMA Pediatr. 2020, 174, e202430. [Google Scholar] [CrossRef]
- Fleitas, P.E.; Paz, J.A.; Simoy, M.I.; Vargas, C.; Cimino, R.O.; Krolewiecki, A.J.; Aparicio, J.P. Clinical diagnosis of COVID-19. A multivariate logistic regression analysis of symptoms of COVID-19 at presentation. Germs 2021, 11, 221–237. [Google Scholar] [CrossRef] [PubMed]
- Zhou, G.Y.; Penwill, N.Y.; Cheng, G.; Singh, P.; Cheung, A.; Shin, M.; Nguyen, M.; Mittal, S.; Burrough, W.; Spad, M.-A.; et al. Utility of illness symptoms for predicting COVID-19 infections in children. BMC Pediatr. 2022, 22, 655. [Google Scholar] [CrossRef]
- Qi, K.; Zeng, W.; Ye, M.; Zheng, L.; Song, C.; Hu, S.; Duan, C.; Wei, Y.; Peng, J.; Zhang, W.; et al. Clinical, laboratory, and imaging features of pediatric COVID-19: A systematic review and meta-analysis. Medicine 2021, 100, e25230. [Google Scholar] [CrossRef] [PubMed]
- Dona, D.; Montagnani, C.; Di Chiara, C.; Venturini, E.; Galli, L.; Lo Vecchio, A.; Denina, M.; Olivini, N.; Bruzzese, E.; Campana, A.; et al. COVID-19 in Infants Less than 3 Months: Severe or Not Severe Disease? Viruses 2022, 14, 2256. [Google Scholar] [CrossRef] [PubMed]
- Lazova, S.; Alexandrova, T.; Gorelyova-Stefanova, N.; Atanasov, K.; Tzotcheva, I.; Velikova, T. Liver Involvement in Children with COVID-19 and Multisystem Inflammatory Syndrome: A Single-Center Bulgarian Observational Study. Microorganisms 2021, 9, 1958. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Frequency, n | Percentage, % |
|---|---|---|
| Male sex | 361 | 58.9 |
| Age groups | ||
| Newborn | 14 | 2.3 |
| 1–3 months | 182 | 29.7 |
| 4–6 months | 160 | 26.1 |
| 7–9 months | 149 | 24.3 |
| 10–12 months | 108 | 17.6 |
| Clinical features | ||
| Fever | 591 | 96.4 |
| Loss of appetite | 388 | 63.3 |
| Respiratory symptoms | 466 | 76.0 |
| Cough | 397 | 64.8 |
| Rhinorrhea | 295 | 48.1 |
| Dyspnea | 69 | 11.3 |
| Digestive symptoms | 309 | 49.6 |
| Vomiting | 148 | 24.1 |
| Diarrhea | 230 | 37.5 |
| Constipation | 21 | 3.4 |
| Preterm | 57 | 9.3 |
| At least one chronic condition | 69 | 11.3 |
| Laboratory Analysis | Results |
|---|---|
| WBC count, median (IQR) | 6800 (4900, 9500) cells/μL |
| WBC increase, n (%) | 151 (24.6) |
| WBC decrease, n (%) | 45 (7.3) |
| Lymphocytes count, median (IQR) | 3000 (1700, 5300) cells/μL |
| Lymphocytes decrease, n (%) | 84 (13.7) |
| Hemoglobin, median (IQR) | 10.9 (10.2, 11.7) g/dL |
| Anemia, n (%) | 508 (82.9) |
| Platelets count, median (IQR) | 278,000 (210,000, 356,000) cells/μL |
| Platelets increase, n (%) | 11 (1.8) |
| Platelets decrease, n (%) | 0 (0.0) |
| AST, median (IQR) | 66 (53, 82) U/L |
| AST increase, n (%) | 491 (80.1) |
| ALT, median (IQR) | 32 (25, 45) U/L |
| ALT increase, n (%) | 191 (31.2) |
| LDH, median (IQR) | 350 (304, 406) U/L |
| LDH increase, n (%) | 514 (83.8) |
| CRP, median (IQR) * | 2.7 (0.9, 7.6) mg/L |
| CRP increase, n (%) * | 182/509 (35.8) |
| IL-6, median (IQR) × | 177.7 (57.5, 1333.5) pg/mL |
| IL-6 increase, n (%) × | 88/91 (96.7) |
| Characteristics | Newborn N = 14 | 1–3 Months N = 182 | 4–6 Months N = 160 | 7–9 Months N = 149 | 10–12 Months N = 108 | p-Value for Comparison between All Groups |
|---|---|---|---|---|---|---|
| Male sex, n (%) | 10 (71.4) | 93 (51.1) | 96 (60.0) | 96 (64.4) | 66 (61.1) | 0.105 |
| Fever, n (%) | 12 (85.7) | 176 (96.7) | 155 (96.9) | 145 (97.3) | 103 (95.4) | 0.243 |
| Loss of appetite, n (%) | 11 (78.6) | 109 (59.9) | 93 (58.1) | 106 (71.1) | 69 (63.9) | 0.093 |
| Respiratory symptoms, n (%) | 8 (57.1) | 131 (72.0) | 122 (76.3) | 121 (81.2) | 84 (77.8) | 0.149 |
| Cough, n (%) | 3 (21.4) | 106 (58.2) | 111 (69.4) | 109 (73.2) + | 68 (63.0) | <0.001 |
| Rhinorrhea, n (%) | 6 (42.9) | 80 (44.0) | 76 (47.5) | 84 (56.4) | 84 (45.4) | 0.211 |
| Dyspnea, n (%) | 2 (14.3) | 15 (8.2) | 23 (14.4) | 15 (10.1) | 14 (13.0) | 0.433 |
| Digestive symptoms, n (%) | 5 (35.7) | 76 (41.8) | 84 (52.5) | 89 (59.7) + | 55 (50.9) | 0.016 |
| Vomiting, n (%) | 2 (14.3) | 20 (11.0) | 39 (24.4) | 49 (32.9) | 38 (35.2) + | <0.001 |
| Diarrhea, n (%) | 4 (28.6) | 59 (32.4) | 68 (42.5) | 65 (43.6) | 34 (31.5) | 0.083 |
| Constipation, n (%) | 0 (0.0) | 7 (3.8) | 7 (4.4) | 2 (1.3) | 5 (4.6) | 0.484 |
| Preterm, n (%) | 4 (28.6) | 17 (9.3) | 17 (10.6) | 10 (6.7) | 9 (8.3) | 0.099 |
| Chronic conditions, n (%) | 1 (7.1) | 19 (10.4) | 22 (13.8) | 13 (8.7) | 14 (13.2) | 0.622 |
| WBC increase, n (%) | 3 (21.4) | 29 (15.9) | 41 (25.6) | 42 (28.2) | 36 (33.3) + | 0.011 |
| WBC decrease, n (%) | 0 (0.0) | 17 (9.3) | 12 (7.5) | 9 (6.0) | 7 (6.5) | 0.614 |
| Lymphocytes decrease, n (%) | 1 (7.1) | 23 (12.6) | 19 (11.9) | 21 (14.1) | 20 (18.5) | 0.513 |
| Anemia, n (%) | 8 (57.1) | 173 (95.1) + | 132 (82.5) | 119 (79.9) | 76 (70.4) | <0.001 |
| AST increase, n (%) | 8 (57.1) | 128 (70.3) | 133 (83.1) | 131 (87.9) + | 91 (84.3) | <0.001 |
| ALT increase, n (%) | 3 (21.4) | 69 (37.9) + | 60 (37.5) + | 37 (24.8) | 22 (20.4) | 0.003 |
| LDH increase, n (%) | 13 (92.9) | 147 (80.8) | 133 (83.1) | 124 (83.2) | 97 (89.9) | 0.281 |
| CRP increase *, n (%) | 1/10 (10.0) | 25/140 (17.9) | 55/133 (41.4) | 56/136 (41.2) | 45/90 (50.0) + | <0.001 |
| IL-6 increase ×, n (%) | 1/1 (100) | 18/18 (100) | 21/21 (100) | 30/32 (93.8) | 18/19 (94.7) | 0.656 |
| Characteristics | General Symptoms Only, N = 69 | Respiratory Symptoms Only, N = 235 | Respiratory and Digestive Symptoms, N = 231 | Digestive Symptoms Only, N = 78 | p-Value |
|---|---|---|---|---|---|
| Male | 35 (50.7) | 140 (59.6) | 149 (64.5) + | 37 (47.4) | 0.027 |
| Female | 34 (49.3) | 95 (40.4) | 82 (35.5) | 41 (52.6) + | |
| Newborn | 3 (4.3) | 6 (2.6) | 2 (0.9) | 3 (3.8) | 0.049 |
| 1–3 months | 27 (39.1) | 79 (33.6) | 52 (22.5) | 24 (29.7) | |
| 4–6 months | 15 (21.7) | 61 (26.0) | 61 (26.4) | 23 (29.5) | |
| 7–9 months | 12 (17.4) | 48 (20.4) | 73 (31.6) + | 16 (20.5) | |
| 10–12 months | 12 (17.4) | 41 (17.4) | 43 (18.6) | 12 (15.4) | |
| Preterm | 2 (2.9) | 24 (10.2) | 28 (12.1) | 3 (3.8) | 0.056 |
| At least one chronic condition | 5 (7.2) | 32 (13.6) | 25 (10.8) | 7 (9.0) | 0.412 |
| WBC increase | 14 (20.3) | 70 (29.8) | 54 (23.4) | 13 (16.7) | 0.074 |
| WBC decrease | 5 (7.2) | 17 (7.2) | 16 (6.9) | 7 (9.0) | 0.947 |
| Lymphocytes decrease | 12 (17.4) | 29 (12.3) | 30 (13.0) | 13 (16.7) | 0.606 |
| Anemia | 60 (87.0) | 187 (79.6) | 193 (83.5) | 68 (87.2) | 0.295 |
| AST increase | 58 (84.1) | 178 (75.7) | 194 (84.0) | 61 (78.2) | 0.120 |
| ALT increase | 18 (26.1) | 61 (26.0) | 78 (34.2) | 34 (42.3) + | 0.044 |
| LDH increase | 54 (78.3) | 198 (84.3) | 198 (85.7) | 64 (82.1) | 0.494 |
| CRP increase * | 20/54 (37.0) | 74/193 (38.3) | 71/195 (36.4) | 17/67 (25.4) | 0.286 |
| IL-6 increase × | 7/7 (100) | 42/44 (95.5) | 32/33 (97.0) | 7/7 (100) | 0.873 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Drăgănescu, A.C.; Miron, V.D.; Săndulescu, O.; Bilaşco, A.; Streinu-Cercel, A.; Sandu, R.G.; Marinescu, A.; Gunșahin, D.; Hoffmann, K.I.; Horobeț, D.Ș.; et al. Omicron in Infants—Respiratory or Digestive Disease? Diagnostics 2023, 13, 421. https://doi.org/10.3390/diagnostics13030421
Drăgănescu AC, Miron VD, Săndulescu O, Bilaşco A, Streinu-Cercel A, Sandu RG, Marinescu A, Gunșahin D, Hoffmann KI, Horobeț DȘ, et al. Omicron in Infants—Respiratory or Digestive Disease? Diagnostics. 2023; 13(3):421. https://doi.org/10.3390/diagnostics13030421
Chicago/Turabian StyleDrăgănescu, Anca Cristina, Victor Daniel Miron, Oana Săndulescu, Anuţa Bilaşco, Anca Streinu-Cercel, Roxana Gabriela Sandu, Adrian Marinescu, Deniz Gunșahin, Karina Ioana Hoffmann, Daria Ștefana Horobeț, and et al. 2023. "Omicron in Infants—Respiratory or Digestive Disease?" Diagnostics 13, no. 3: 421. https://doi.org/10.3390/diagnostics13030421
APA StyleDrăgănescu, A. C., Miron, V. D., Săndulescu, O., Bilaşco, A., Streinu-Cercel, A., Sandu, R. G., Marinescu, A., Gunșahin, D., Hoffmann, K. I., Horobeț, D. Ș., Pițigoi, D., Streinu-Cercel, A., & Pleșca, D. A. (2023). Omicron in Infants—Respiratory or Digestive Disease? Diagnostics, 13(3), 421. https://doi.org/10.3390/diagnostics13030421