
Measurement of Uncertainty in Prediction of No-Reflow Phenomenon after Primary Percutaneous Coronary Intervention Using Systemic Immune Inflammation Index: The Gray Zone Approach

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Dataset
2.2. Coronary Procedures
2.3. Laboratory Measurements
2.4. Statistical Analysis
Determination of the Gray Zone
- (i)
- Grey Zone ApproachCoste and Pouchot [13] define the boundaries of the gray zone area via negative and positive likelihood ratios. To find the likelihood ratios, the following steps are used:
- (a)
- Specify the pre-test probabilities. The pre-test probabilities are chosen based on the prevalence of no-reflow in the sample. The number of patients in the no-reflow and normal flow groups was 110 and 400, respectively. Therefore, the pre-probabilities of having no-reflow and normal flow were taken as 110/510 = 0.216 and 400/510 = 0.784, respectively.
- (b)
- Specify the post-test probabilities. The post-test probabilities are specified as 0.6 and 0.95 for positive predictive and negative predictive values, respectively.
- (c)
- The positive likelihood ratio (LR+) and the negative likelihood ratio (LR-) are calculated using these test probabilities and were found to be 5.455 and 0.191 by using Equation (1).
- (ii)
- Uncertain Interval ApproachAn alternative approach to finding the inconclusive area has been proposed [14]. This approach depends on a different trichotomization method by using the two decision thresholds based on pre-selected values of sensitivity and specificity in this uncertain area. In this study, the pre-selected values are chosen as 0.55 for both sensitivity and specificity in the gray zone by considering the default values.
3. Results
4. Discussion
5. Conclusions
6. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Grüntzig, A.R.; Senning, Å.; Siegenthaler, W.E. Nonoperative dilatation of coronary-artery stenosis: Percutaneous transluminal coronary angioplasty. N. Engl. J. Med. 1979, 301, 61–68. [Google Scholar] [CrossRef]
- Rott, D. Advantage of percutaneous coronary intervention over medical therapy in angina relief and the placebo effect. J. Am. Coll. Cardiol. 2005, 45, 327–328. [Google Scholar] [CrossRef] [PubMed]
- Fajar, J.K.; Heriansyah, T.; Rohman, M.S. The predictors of no reflow phenomenon after percutaneous coronary intervention in patients with ST elevation myocardial infarction: A meta-analysis. Indian Heart J. 2014, 70, 406–418. [Google Scholar] [CrossRef] [PubMed]
- Jaffe, R.; Charron, T.; Puley, G.; Dick, A.; Strauss, B.H. Microvascular obstruction and the no-reflow phenomenon after percutaneous coronary intervention. Circulation 2008, 7, 3152–3156. [Google Scholar] [CrossRef]
- Pantea-Rosan, L.R.; Pantea, V.A.; Bungau, S.; Tit, D.M.; Behl, T.; Vesa, C.M.; Bustea, C.; Moleriu, R.D.; Rus, M.; Popescu, M.I.; et al. No-Reflow after PPCI-A Predictor of Short-Term Outcomes in STEMI Patients. J. Clin. Med. 2020, 2, 2956. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Gupta, M.M. No reflow phenomenon in percutaneous coronary interventions in ST-segment elevation myocardial infarction. Indian Heart J. 2016, 8, 539–551. [Google Scholar] [CrossRef]
- Hu, B.; Yang, X.R.; Xu, Y.; Sun, Y.F.; Sun, C.; Guo, W.; Zhang, X.; Wang, W.M.; Qiu, S.J.; Zhou, J.; et al. Systemic immune-inflammation index predicts prognosis of patients after curative resection for hepatocellular carcinoma. Clin. Cancer Res. 2014, 20, 6212–6222. [Google Scholar] [CrossRef]
- Seo, M.; Yamada, T.; Morita, T.; Furukawa, Y.; Tamaki, S.; Iwasaki, Y.; Kawaski, M.; Kikuchi, A.; Kawai, T.; Ikeda, I.; et al. Prognostic value of systemic immune-inflammation index in patients with chronic heart failure. Eur. Heart J. 2018, 39, 70–71. [Google Scholar] [CrossRef]
- Esenboga, K.; Kurtul, A.; Yamanturk, Y.Y.; Tan, S.T.; Tutar, E.D. Systemic immune-inflammation index predicts no-reflow phenomenon after primary percutaneous coronary intervention. Acta Cardiol. 2022, 77, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Feinstein, A.R. The inadequacy of binary models for the clinical reality of three-zone diagnostic decisions. J. Clin. Epidemiol. 1990, 3, 109–113. [Google Scholar] [CrossRef]
- Simel, D.L.; Samsa, G.P.; Matchar, D.B. Likelihood ratios for continuous test results—Making the clinicians job easier or harder? J. Clin. Epidemiol. 1993, 6, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Jamart, J. Chance-corrected sensitivity and specificity for three-zone diagnostic tests. J. Clin. Epidemiol. 1992, 5, 1035–1038. [Google Scholar] [CrossRef] [PubMed]
- Coste, J.; Pouchot, J. A grey zone for quantitative diagnostic and screening tests. Int. J. Epidemiol. 2002, 2, 304–313. [Google Scholar] [CrossRef]
- Landsheer, J.A. Interval of uncertainty: An alternative approach for the determination of decision thresholds, with an illustrative application for the prediction of prostate cancer. PLoS ONE 2016, 11, e0166007. [Google Scholar] [CrossRef]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2018, 9, 119–177. [Google Scholar]
- Sianos, G.; Papafaklis, M.I.; Serruys, P.W. Angiographic thrombus burden classification in patients with STsegment elevation myocardial infarction treated with percutaneous coronary intervention. J. Invasive Cardiol. 2010, 22 (Suppl. B), 6B–14B. [Google Scholar]
- Iwakura, K.; Ito, H.; Takiuchi, S.; Taniyama, Y.; Nakatsuchi, Y.; Negoro, S.; Higashino, Y.; Okamura, A.; Masuyama, T.; Hori, M.; et al. Alternation in the coronary blood flow velocity pattern in patients with no reflow and reperfused acute myocardial infarction. Circulation 1996, 4, 1269–1275. [Google Scholar] [CrossRef]
- Niccoli, G.; Burzotta, F.; Galiuto, L.; Crea, F. Myocardial no-reflow in humans. J. Am. Coll. Cardiol. 2009, 4, 281–292. [Google Scholar] [CrossRef]
- Hafez, T. Modification of Diet in Renal Disease (MDRD) estimated glomerular filtration rate (eGFR) formula. Am. J. Cardiol. 2007, 9, 584. [Google Scholar] [CrossRef]
- Kuhn, M. caret: Classification and Regression Training. R Package Version 6.0-91. Available online: https://CRAN.R-project.org/package=caret (accessed on 20 December 2022).
- IBM Corp. Released 2015. IBM SPSS Statistics for Windows; Version 23.0; IBM Corp: Armonk, NY, USA, 2015. [Google Scholar]
- Wickham, H. ggplot2: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2016. [Google Scholar]
- Landsheer, H. UncertainInterval: Uncertain Interval Methods for Three-Way Cut-Point Determination in Test Results. R Package Version 0.7.0. 2021. Available online: https://CRAN.R-project.org/package=UncertainInterval (accessed on 20 December 2022).
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021; Available online: https://www.R-project.org/ (accessed on 20 December 2022).
- Galasso, G.; Schiekofer, S.; D’Anna, C.; Gioia, G.D.; Piccolo, R.; Niglio, T.; Rosa, R.D.; Strisciuglio, T.; Cirillo, P.; Piscione, F.; et al. No-reflow phenomenon: Pathophysiology, diagnosis, prevention, and treatment. A review of the current literature and future perspectives. Angiology 2014, 65, 180–189. [Google Scholar] [CrossRef] [PubMed]
- Kurtul, A.; Yarlioglues, M.; Murat, S.N.; Ergun, G.; Duran, M.; Kasapkara, H.A.; Demircelik, M.B.; Cetin, M.; Ocek, A.H. Usefulness of the platelet-to-lymphocyte ratio in predicting angiographic reflow after primary percutaneous coronary intervention in patients with acute ST-segment elevation myocardial infarction. Am. J. Cardiol. 2014, 4, 342–347. [Google Scholar] [CrossRef] [PubMed]
- Caiazzo, G.; Musci, R.L.; Frediani, L.; Umińska, J.; Wanha, W.; Filipiak, K.J.; Kubica, J.; Navarese, E.P. State of the art: No-reflow phenomenon. Cardiol. Clin. 2020, 8, 563–573. [Google Scholar] [CrossRef] [PubMed]
- Rezkalla, S.H.; Stankowski, R.V.; Hanna, J.; Kloner, R.A. Management of no-reflow phenomenon in the catheterization laboratory. JACC Cardiovasc. Interv. 2017, 10, 215–223. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Grades of Angiographic Thrombus Burden | |
|---|---|
| Grade 0 | No thrombus |
| Grade 1 | Thrombus may exist |
| Grade 2 | The thrombus’ largest size is less than half a vessel in diameter |
| Grade 3 | The largest dimension is between one half and two vessels in diameter |
| Grade 4 | There are more than two vessel diameters in the largest dimension |
| Grade 5 | The thrombus completely occludes the vessel |
| Variable | Normal Flow (n = 400) | No-Reflow (n = 110) | Test Statistic | p-Value |
|---|---|---|---|---|
| Age | 62 (54–70) | 62.50 (53–70) | 0.039 | 0.969 |
| Male | 314 (78.5) | 77 (70) | NA | 0.074 |
| History of hypertension | 237 (59.25) | 57 (51.818) | NA | 0.191 |
| History of diabetes | 151 (37.75) | 34 (30.909) | NA | 0.218 |
| Smoking | 133 (33.250) | 29 (26.364) | NA | 0.203 |
| History of hyperlipidemia | 124 (31) | 31 (28.182) | NA | 0.640 |
| Family history of coronary heart disease | 85 (21.25) | 29 (26.364) | NA | 0.301 |
| Prior stroke | 7 (1.75) | 5 (4.545) | NA | 0.145 |
| Time from pain to intervention (>6 h) | 89 (22.25) | 19 (17.273) | NA | 0.293 |
| Prior aspirin therapy | 134 (33.5) | 21 (19.091) | NA | 0.003 |
| Prior statin therapy | 109 (27.25) | 20 (18.182) | NA | 0.063 |
| Prior clopidogrel therapy | 32 (8) | 7 (6.364) | NA | 0.687 |
| In hospital statin therapy | 400 (100) | 110 (100) | NA | NA |
| Gp IIb/IIIa inhibitor therapy | 41 (10.25) | 15 (13.636) | NA | 0.306 |
| Killip class (3–4) | 33 (8.25) | 19 (17.273) | NA | 0.012 |
| Anterior infarction location | 188 (47) | 62 (56.364) | NA | 0.086 |
| Left ventricular ejection fraction | 45 (40–45) | 45 (40–50) | −0.931 | 0.352 |
| Variable | Normal Flow (n = 400) | No-Reflow (n = 110) | Test Statistic | p-Value |
|---|---|---|---|---|
| Platelet count (×10/L) | 239 (204–278) | 354.5 (284–377) | −10.464 | <0.001 |
| Neutrophil count (×10/L) | 6.2 (4.915–8.295) | 11.63 (7.18–15.12) | −8.843 | <0.001 |
| Lymphocyte count (×10/L) | 2.005 (1.5–2.955) | 1.695 (1.13–2.34) | −3.541 | <0.001 |
| Neutrophil to lymphocyte ratio | 2.903 (1.767–5.074) | 7.13 (3.456–11.874) | −7.826 | <0.001 |
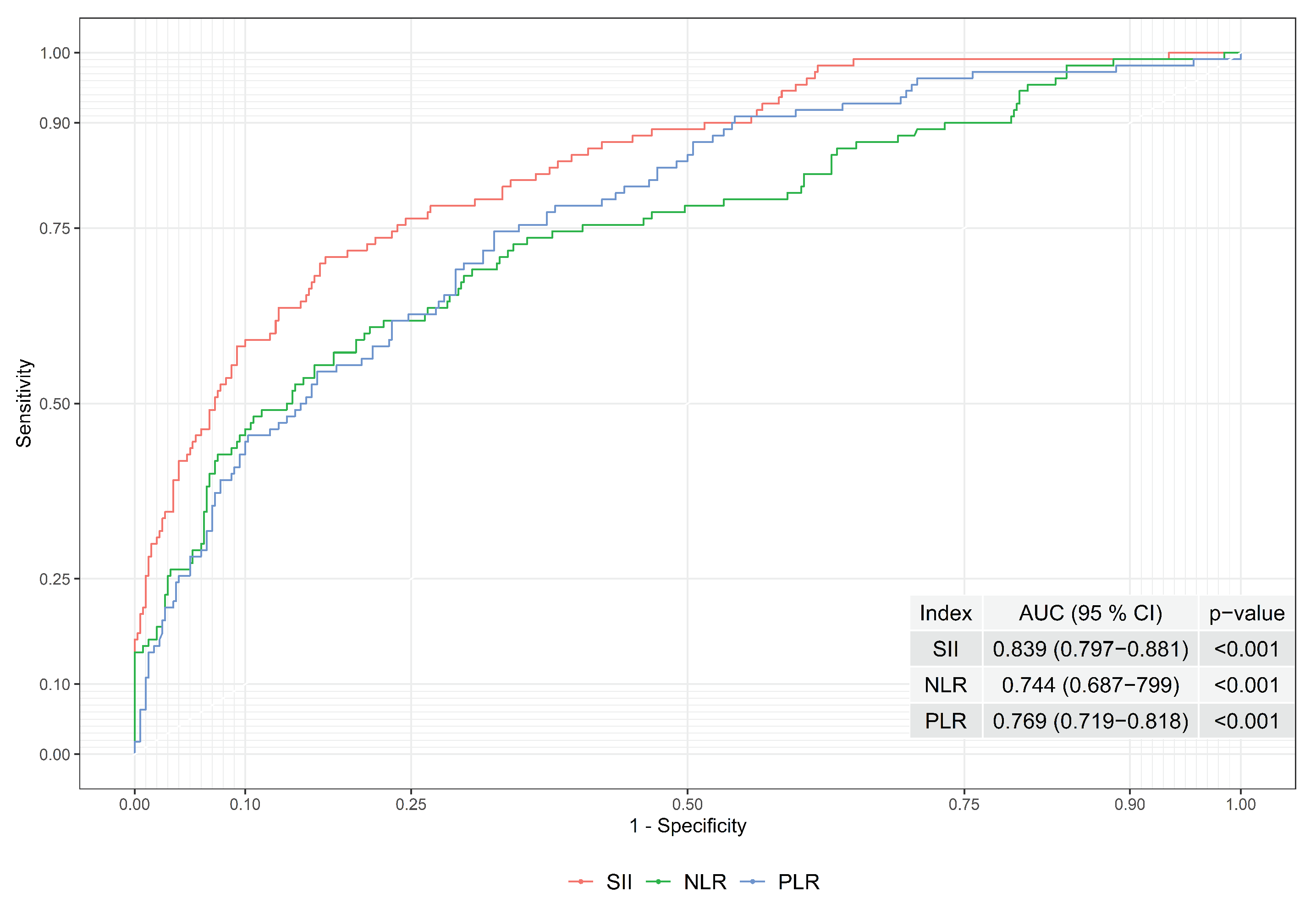
| Systemic immune-inflammation index | 690.791 (413.911–1161.518) | 2066.281 (1190.72–3493.188) | −10.893 | <0.001 |
| Platelet to lymphocyte ratio | 113.231 (80.776–161.786) | 190.788 (138.153–299.18) | −8.63 | <0.001 |
| Serum glucose (mg/dL) | 118 (99–160.5) | 129 (105–171) | −1.819 | 0.069 |
| Serum creatinine (mg/dL) | 0.88 (0.75–1.06) | 0.92 (0.77–1.09) | −1.233 | 0.218 |
| C-reactive protein (mg/dL) | 6.3 (2.6–18.3) | 13.95 (5.9–63.6) | −4.885 | <0.001 |
| Peak cardiac troponin (ng/dL) | 294.5 (40.6–3142.3) | 773.9 (47.63–6702) | −1.681 | 0.093 |
| Total cholesterol (mg/dL) | 185 (160–221.5) | 193.5 (152–236) | −0.347 | 0.728 |
| Low-density lipoprotein cholesterol (mg/dL) | 120 (94–146.5) | 123 (89–163) | −0.619 | 0.536 |
| High-density lipoprotein cholesterol (mg/dL) | 39 (33–45) | 39 (33–49) | −0.672 | 0.501 |
| Triglyceride (mg/dL) | 134 (90–199) | 122.5 (88–160) | −1.744 | 0.081 |
| Hemoglobin (g/dL) | 14.5 (12.9–15.6) | 13.7 (11.5–15.1) | −3.237 | 0.001 |
| Glomerular filtration rate (mL/min/1.73 m) | 88 (72.5–94) | 84.5 (65–92) | −1.546 | 0.122 |
| Type of intervention | ||||
| Direct Stenting | 36 (9) | 11 (10) | NA | 0.713 |
| Balloon angioplasty before stenting | 364 (91) | 99 (90) | ||
| Thrombus aspiration | 7 (1.75) | 2 (1.818) | NA | >0.999 |
| Intra-aortic balloon pump use | 6 (1.5) | 0 (0) | NA | 0.346 |
| Total stent length (mm) | 30 (22–46) | 33 (24–56) | −1.238 | 0.216 |
| Stent diameter (mm) | 2.75 (2.5–3) | 2.875 (2.5–3) | −0.495 | 0.621 |
| Multi-vessel disease | 155 (38.75) | 39 (35.455) | 0.398 | 0.528 |
| Approaches | Gray Zone Limits | Patients Inside Gray Zone | Patients Outside Gray Zone | |||||
|---|---|---|---|---|---|---|---|---|
| Lower Limit– Upper Limit | Size | Total | No-Reflow | Normal Flow | Accuracy | Sensitivity | Specificity | |
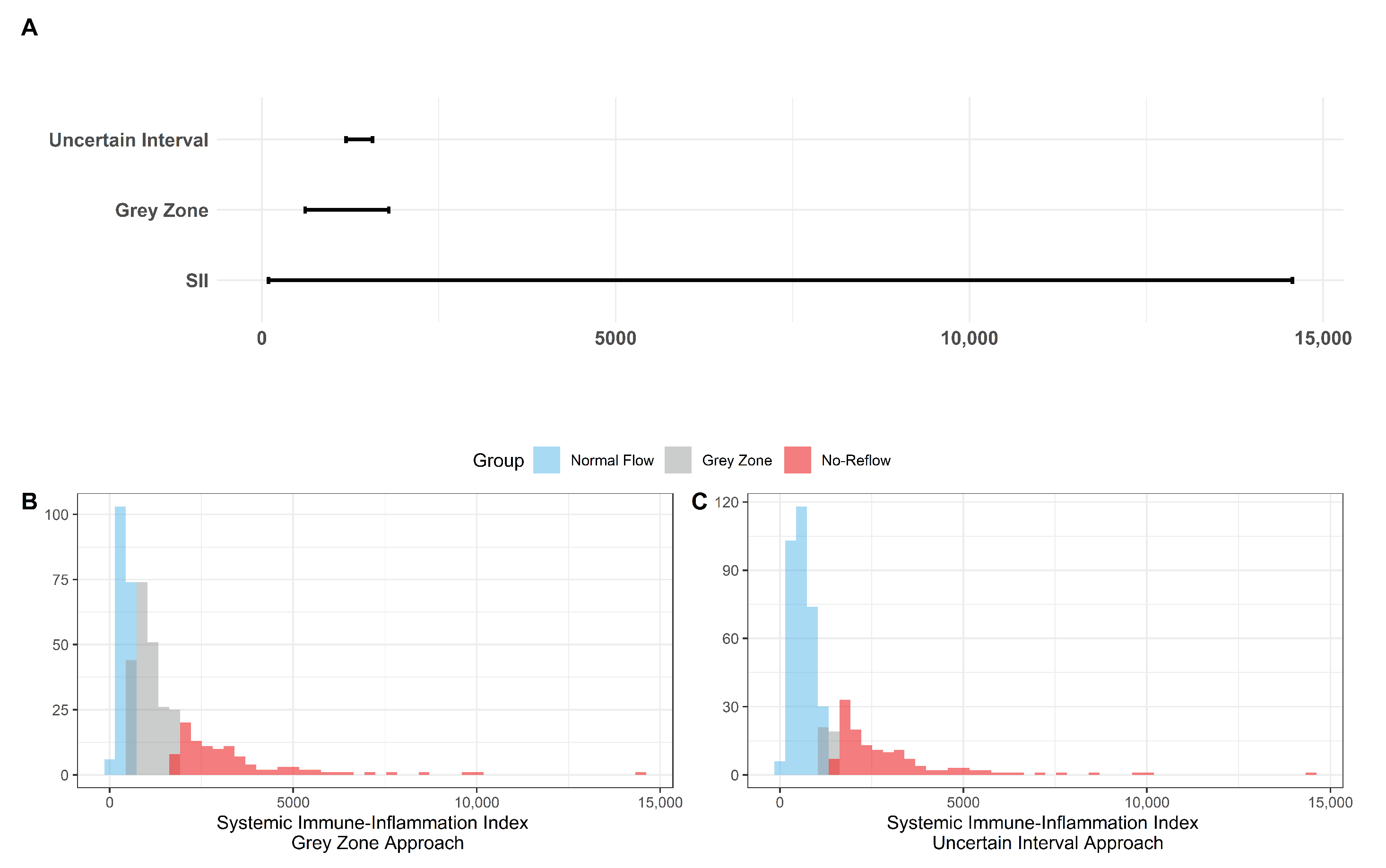
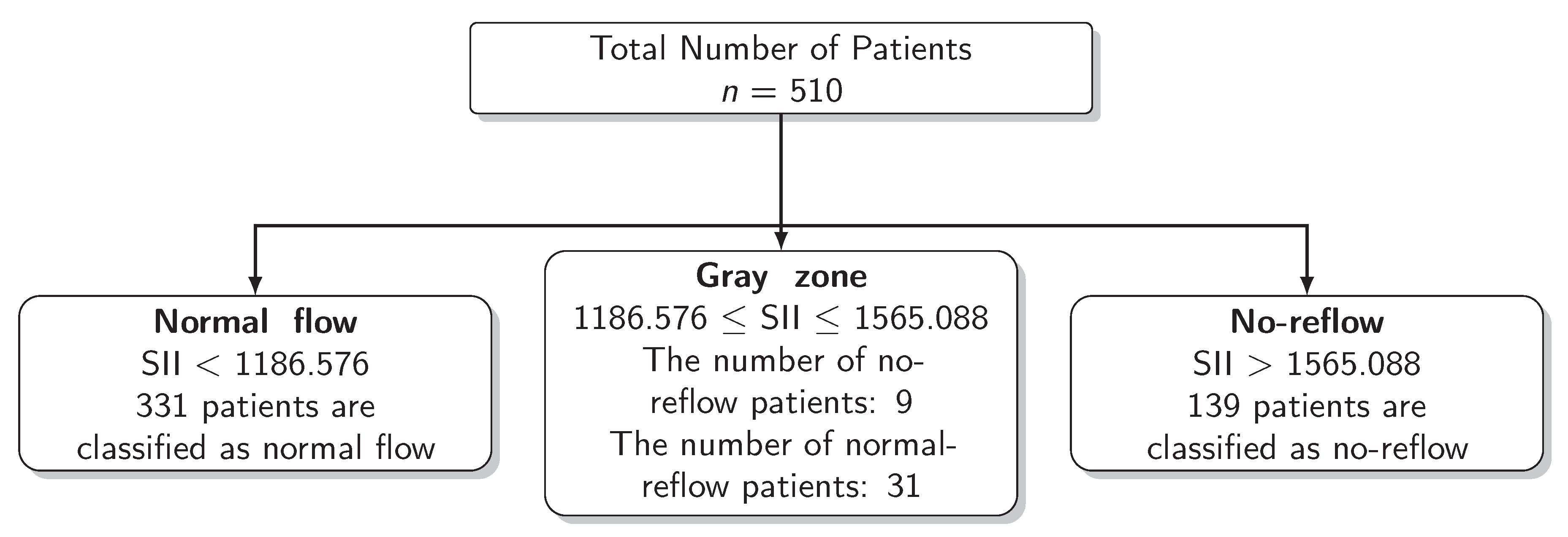
| Uncertain Interval | 1186.576–1565.088 | 378.5125 | 40 | 9 | 31 | 0.804 | 0.732 | 0.824 |
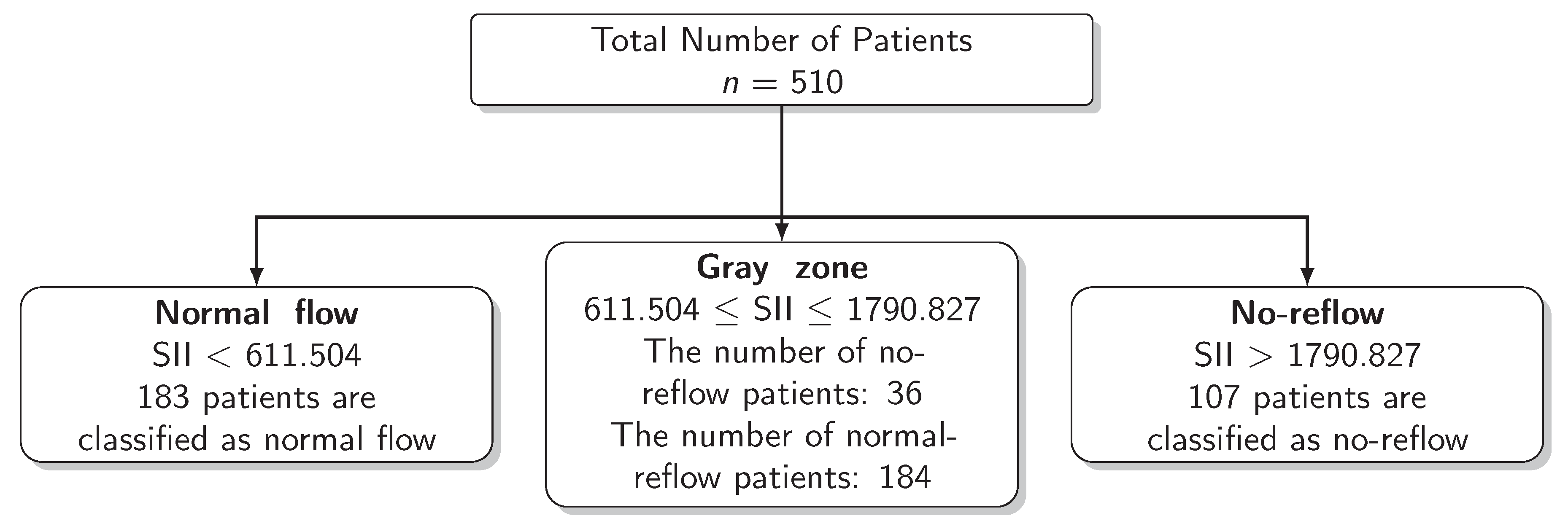
| Grey Zone | 611.504–1790.827 | 1179.323 | 220 | 36 | 184 | 0.824 | 0.878 | 0.806 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ozturk, E.; Esenboga, K.; Kurtul, A.; Kilickap, M.; Karaagaoglu, E.; Karakaya, J. Measurement of Uncertainty in Prediction of No-Reflow Phenomenon after Primary Percutaneous Coronary Intervention Using Systemic Immune Inflammation Index: The Gray Zone Approach. Diagnostics 2023, 13, 709. https://doi.org/10.3390/diagnostics13040709
Ozturk E, Esenboga K, Kurtul A, Kilickap M, Karaagaoglu E, Karakaya J. Measurement of Uncertainty in Prediction of No-Reflow Phenomenon after Primary Percutaneous Coronary Intervention Using Systemic Immune Inflammation Index: The Gray Zone Approach. Diagnostics. 2023; 13(4):709. https://doi.org/10.3390/diagnostics13040709
Chicago/Turabian StyleOzturk, Ebru, Kerim Esenboga, Alparslan Kurtul, Mustafa Kilickap, Ergun Karaagaoglu, and Jale Karakaya. 2023. "Measurement of Uncertainty in Prediction of No-Reflow Phenomenon after Primary Percutaneous Coronary Intervention Using Systemic Immune Inflammation Index: The Gray Zone Approach" Diagnostics 13, no. 4: 709. https://doi.org/10.3390/diagnostics13040709
APA StyleOzturk, E., Esenboga, K., Kurtul, A., Kilickap, M., Karaagaoglu, E., & Karakaya, J. (2023). Measurement of Uncertainty in Prediction of No-Reflow Phenomenon after Primary Percutaneous Coronary Intervention Using Systemic Immune Inflammation Index: The Gray Zone Approach. Diagnostics, 13(4), 709. https://doi.org/10.3390/diagnostics13040709