
A Study on the Role of Intraoperative Corticobulbar Motor Evoked Potentials for Improving Safety of Cerebellopontine Angle Surgery in Elderly Patients

 , , ,
, , ,  , , ,
, , ,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients Enrollment and Clinical Data
2.2. Intraoperative Neurophysiological Monitoring
2.3. Statistical Analysis
3. Results
3.1. Patients Characteristics
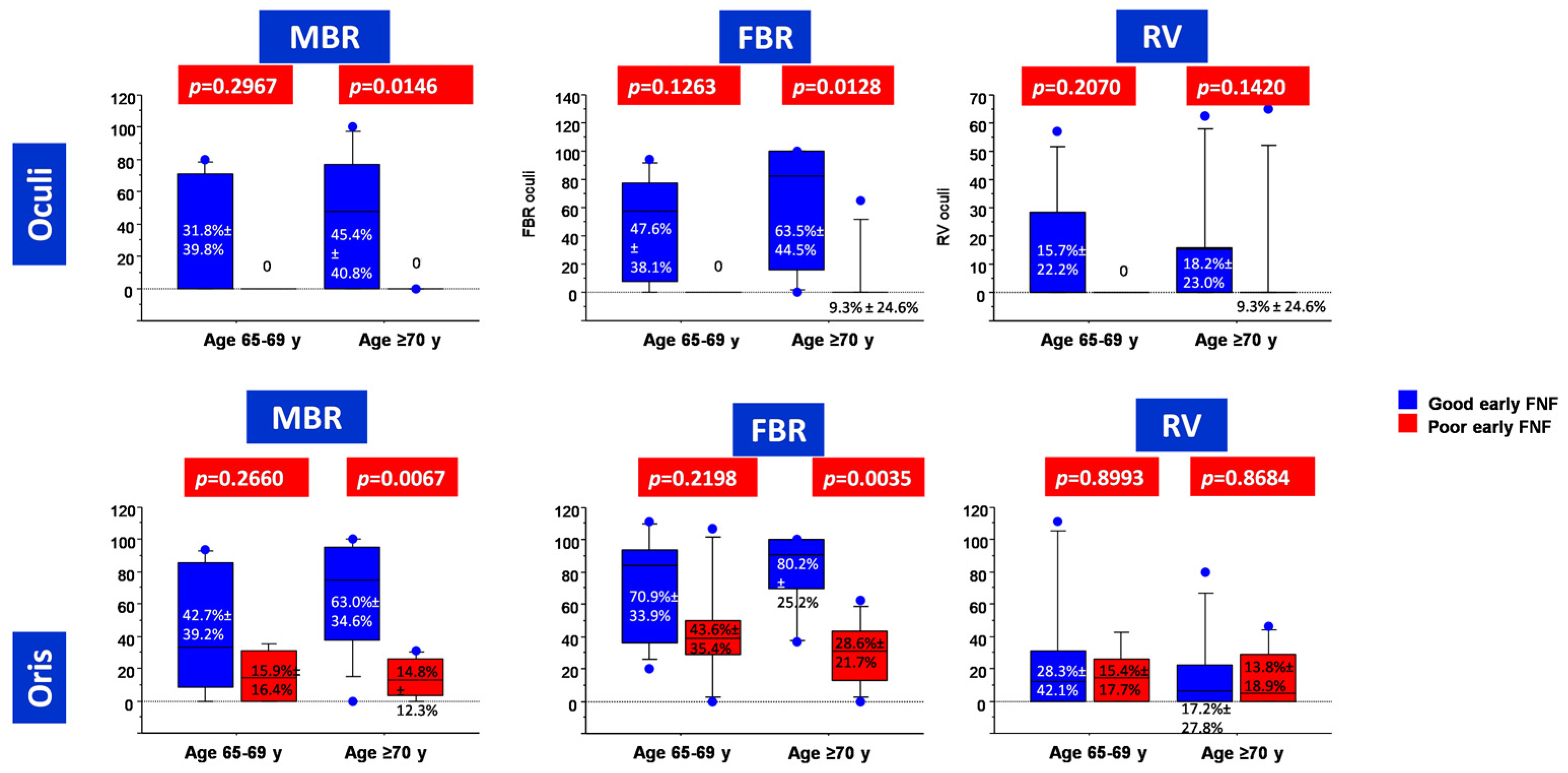
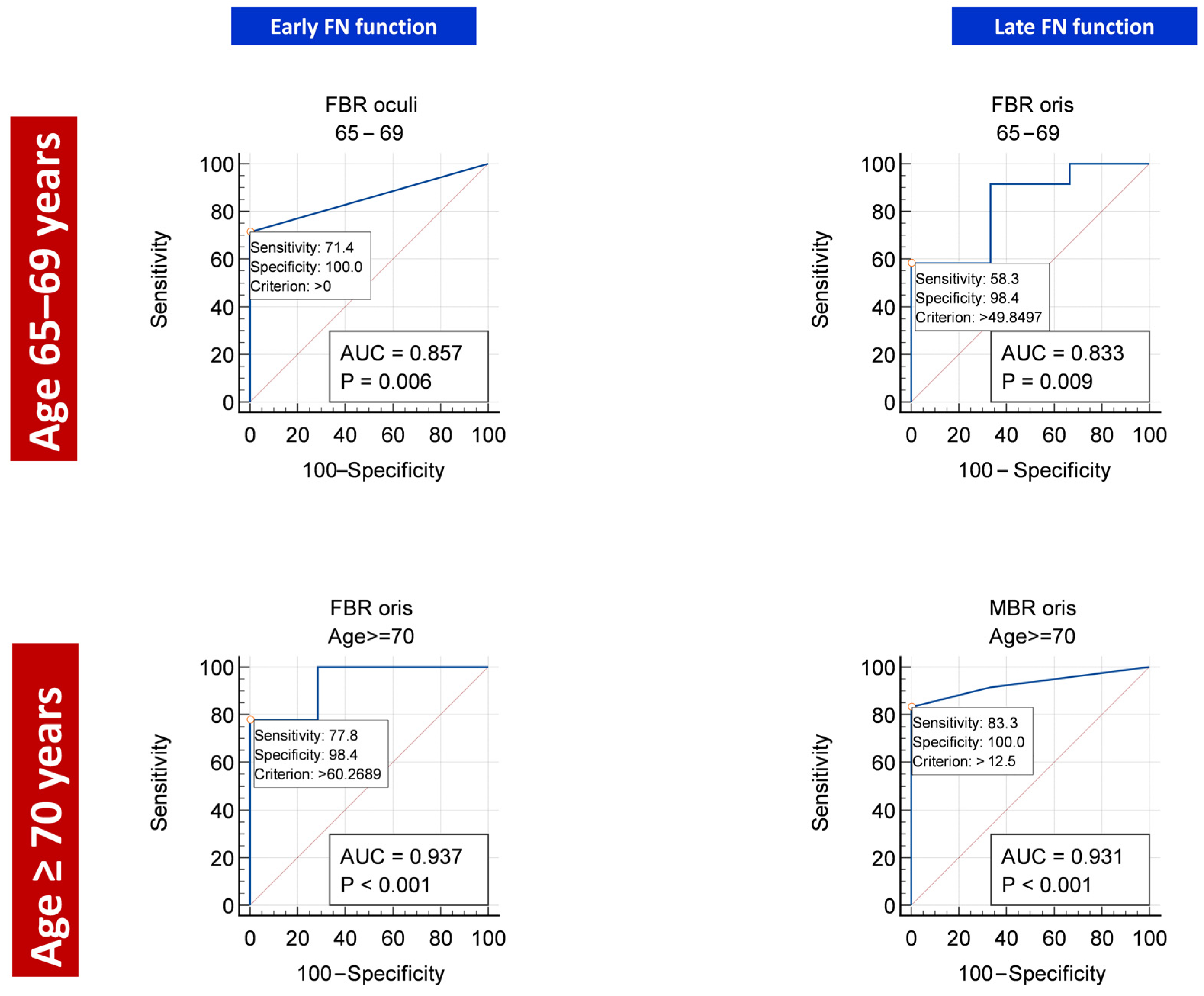
3.2. Predictors of Early Post-Operative FNF
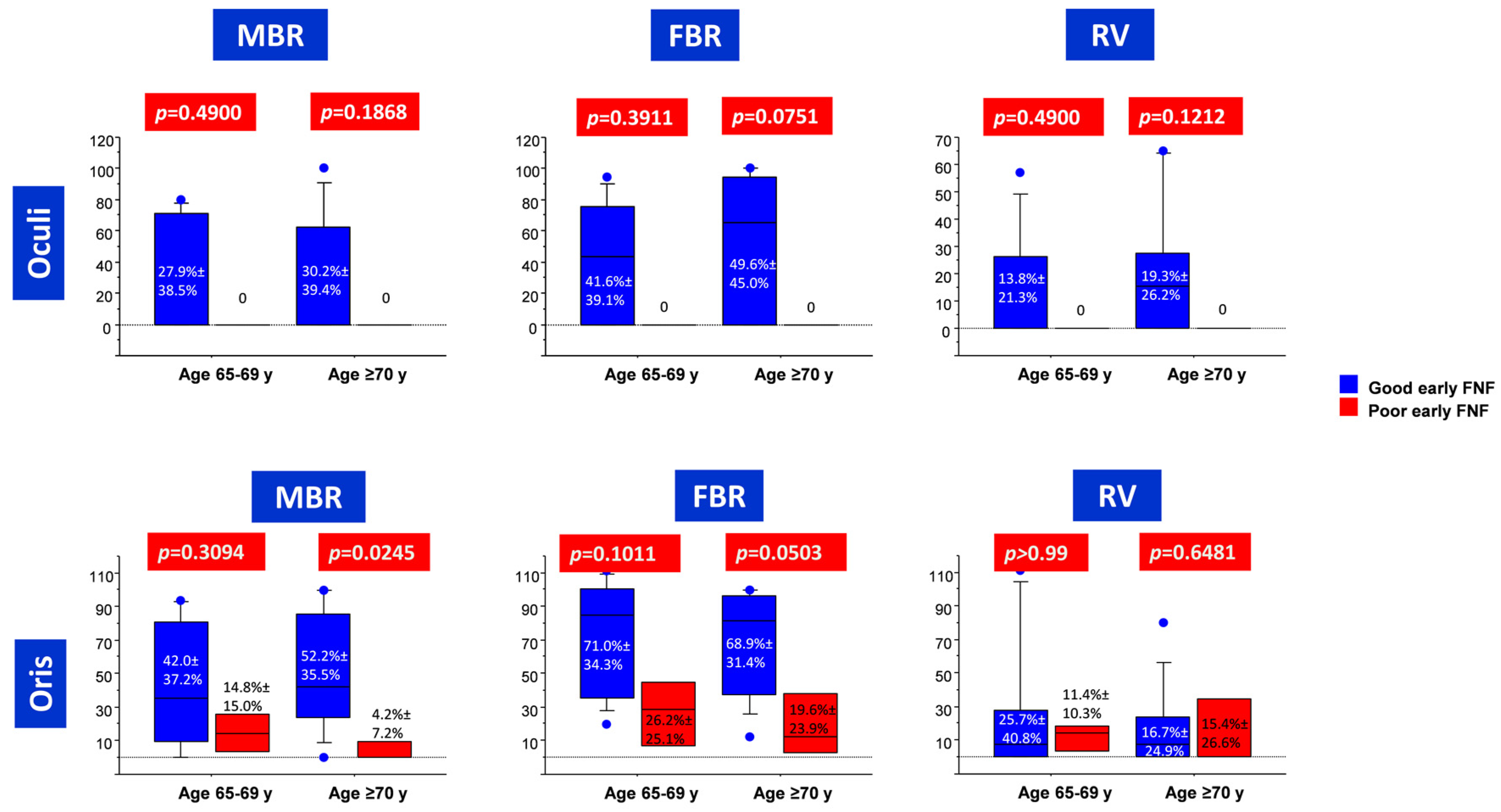
3.3. Predictors of Late Post-Operative FNF
4. Discussion
4.1. Safety of CPA Surgery in Elderly Patients
4.2. Predictors of FNF in Elderlies
4.3. Potential Implications for Neurosurgery in Other Brain Areas
4.4. Limitations
- -
- the retrospective nature of data collection;
- -
- a possible selection bias, since elderly patients with major contraindications to general anesthesia were a priori excluded; and
- -
- the relatively low number of patients, which reduces the statistical significance.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mercier, P.; Bernard, F. Surgical anatomy for hemifacial spasm. Neurochirurgie 2018, 64, 124–132. [Google Scholar] [CrossRef] [PubMed]
- Ling, M.; Tao, X.; Ma, S.; Yang, X.; Liu, L.; Fan, X.; Jia, G.; Qiao, H. Predictive value of intraoperative facial motor evoked potentials in vestibular schwannoma surgery under two anesthesia protocols. World Neurosurg. 2018, 111, e267–e276. [Google Scholar] [CrossRef] [PubMed]
- Rhoton, A.L., Jr. The cerebellar arteries. Neurosurgery 2000, 47 (Suppl. 3), S29–S68. [Google Scholar] [CrossRef] [PubMed]
- Winn, H.R. (Ed.) Youmans Neurological Surgery, 6th ed.; Elsevier: Philadelphia, PA, USA, 2011. [Google Scholar]
- Montano, N.; Signorelli, F.; Giordano, M.; D’Onofrio, F.G.; Izzo, A.; D’Ercole, M.; Ioannoni, E.; Pennisi, G.; Caricato, A.; Pallini, R.; et al. Factors associated with cerebrospinal fluid leak after a retrosigmoid approach for cerebellopontine angle surgery. Surg. Neurol. Int. 2021, 12, 258. [Google Scholar] [CrossRef]
- Foscolo, V.; de Gennaro, L.; Murri, A.; Speranzon, L.; Signorelli, F.; Quaranta, N.; Messina, R. Postoperative Impact of Pontocerebellar Angle Surgery on the Quality of Life in Patients with Vestibular Schwannoma. Audiol. Res. 2022, 12, 635–643. [Google Scholar] [CrossRef]
- Téllez, M.J.; Mirallave-Pescador, A.; Seidel, K.; Urriza, J.; Shoakazemi, A.; Raabe, A.; Ghatan, S.; Deletis, V.; Ulkatan, S. Neurophysiological monitoring of the laryngeal adductor reflex during cerebellar-pontine angle and brainstem surgery. Clin. Neurophysiol. 2021, 132, 622–631. [Google Scholar] [CrossRef]
- Rhoton, A.L., Jr. Microsurgical anatomy of the posterior fossa cranial nerves. Clin. Neurosurg. 1979, 26, 398–462. [Google Scholar] [CrossRef]
- Gazia, F.; Callejo, À.; Pérez-Grau, M.; Lareo, S.; Prades, J.; Roca-Ribas, F.; Amilibia, E. Pre- and intra-operative prognostic factors of facial nerve function in cerebellopontine angle surgery. Eur. Arch. Otorhinolaryngol. 2022, 280, 1055–1062, Epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Schär, R.T.; Tashi, S.; Branca, M.; Söll, N.; Cipriani, D.; Schwarz, C.; Pollo, C.; Schucht, P.; Ulrich, C.T.; Beck, J.; et al. How safe are elective craniotomies in elderly patients in neurosurgery today? A prospective cohort study of 1452 consecutive cases. J. Neurosurg. 2020, 134, 1113–1121. [Google Scholar] [CrossRef]
- Lutz, W.; Sanderson, W.; Scherbov, S. The coming acceleration of global population ageing. Nature 2008, 451, 716–719. [Google Scholar] [CrossRef]
- Hamel, M.B.; Henderson, W.G.; Khuri, S.F.; Daley, J. Surgical outcomes for patients aged 80 and older: Morbidity and mortality from major noncardiac surgery. J. Am. Geriatr. Soc. 2005, 53, 424–429. [Google Scholar] [CrossRef] [PubMed]
- Jablonski, S.G.; Urman, R.D. The Growing Challenge of the Older Surgical Population. Anesthesiol. Clin. 2019, 37, 401–409. [Google Scholar] [CrossRef] [PubMed]
- Etzioni, D.A.; Liu, J.H.; Maggard, M.A.; Ko, C.Y. The aging population and its impact on the surgery workforce. Ann. Surg. 2003, 238, 170–177. [Google Scholar] [CrossRef]
- Klingenschmid, J.; Krigers, A.; Kerschbaumer, J.; Thomé, C.; Pinggera, D.; Freyschlag, C.F. Surgical Management of Malignant Glioma in the Elderly. Front. Oncol. 2022, 12, 900382. [Google Scholar] [CrossRef] [PubMed]
- Ferroli, P.; Vetrano, I.G.; Schiavolin, S.; Acerbi, F.; Zattra, C.; Schiariti, M.; Leonardi, M.; Broggi, M. Brain Tumor Resection in Elderly Patients: Potential Factors of Postoperative Worsening in a Predictive Outcome Model. Cancers 2021, 13, 2320. [Google Scholar] [CrossRef] [PubMed]
- Quimby, A.E.; Lui, J.; Chen, J. Predictive ability of direct electrical stimulation on facial nerve function following vestibular schwannoma surgery: A systematic review and meta-analysis. Otol. Neurotol. 2021, 42, 493–504. [Google Scholar] [CrossRef] [PubMed]
- Matsushima, K.; Kohno, M.; Sakamoto, H.; Ichimasu, N.; Nakajima, N. Intraoperative continuous neuromonitoring for vestibular schwannoma surgery: Real-time, quantitative, and functional evaluation. World Neurosurg. 2021, 158, 159. [Google Scholar] [CrossRef]
- Della Pepa, G.M.; Stifano, V.; D’Alessandris, Q.G.; Menna, G.; Burattini, B.; Di Domenico, M.; Izzo, A.; D’Ercole, M.; Lauretti, L.; Olivi, A.; et al. Intraoperative Corticobulbar Motor Evoked Potential in Cerebellopontine Angle Surgery: A Clinically Meaningful Tool to Predict Early and Late Facial Nerve Recovery. Neurosurgery 2022, 91, 406–413. [Google Scholar] [CrossRef]
- Izzo, A.; Stifano, V.; Della Pepa, G.M.; Di Domenico, M.; D’Alessandris, Q.G.; Menna, G.; D’Ercole, M.; Lauretti, L.; Olivi, A.; Montano, N. Tailored Approach and Multimodal Intraoperative Neuromonitoring in Cerebellopontine Angle Surgery. Brain Sci. 2022, 12, 1167. [Google Scholar] [CrossRef]
- Matthies, C.; Raslan, F.; Schweitzer, T.; Hagen, R.; Roosen, K.; Reiners, K. Facial motor evoked potentials in cerebellopontine angle surgery: Technique, pitfalls and predictive value. Clin. Neurol. Neurosurg. 2011, 113, 872–879. [Google Scholar] [CrossRef]
- Acioly, M.A.; Liebsch, M.; de Aguiar, P.H.; Tatagiba, M. Facial nerve monitoring during cerebellopontine angle and skull base tumor surgery: A systematic review from description to current success on function prediction. World Neurosurg. 2013, 80, e271–e300. [Google Scholar] [CrossRef]
- Ren, Y.; MacDonald, B.V.; Tawfik, K.O.; Schwartz, M.S.; Friedman, R.A. Clinical Predictors of Facial Nerve Outcomes After Surgical Resection of Vestibular Schwannoma. Otolaryngol. Head Neck Surg. 2021, 164, 1085–1093. [Google Scholar] [CrossRef] [PubMed]
- Troude, L.; Boucekine, M.; Montava, M.; Lavieille, J.P.; Régis, J.M.; Roche, P.H. Predictive Factors of Early Postoperative and Long-Term Facial Nerve Function After Large Vestibular Schwannoma Surgery. World Neurosurg. 2019, 127, e599–e608. [Google Scholar] [CrossRef] [PubMed]
- Hiruta, R.; Sato, T.; Itakura, T.; Fujii, M.; Sakuma, J.; Bakhit, M.; Kojima, T.; Ichikawa, M.; Iwatate, K.; Saito, K. Intraoperative transcranial facial motor evoked potential monitoring in surgery of cerebellopontine angle tumors predicts early and late postoperative facial nerve function. Clin. Neurophysiol. 2021, 132, 864–871. [Google Scholar] [CrossRef]
- Legninda Sop, F.Y.; D’Ercole, M.; Izzo, A.; Rapisarda, A.; Ioannoni, E.; Caricato, A.; Olivi, A.; Montano, N. The Impact of Neuronavigation on the Surgical Outcome of Microvascular Decompression for Trigeminal Neuralgia. World Neurosurg. 2021, 149, 80–85. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, M.; Roser, F.; Dormiani, M.; Matthies, C.; Vorkapic, P.; Samii, M. Facial and cochlear nerve function after surgery of cerebellopontine angle meningiomas. Neurosurgery 2005, 57, 77–90. [Google Scholar] [CrossRef] [PubMed]
- Dong, C.C.; Macdonald, D.B.; Akagami, R.; Westerberg, B.; Alkhani, A.; Kanaan, I.; Hassounah, M. Intraoperative facial motor evoked potential monitoring with transcranial electrical stimulation during skull base surgery. Clin. Neurophysiol. 2005, 116, 588–596. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, M.; Oishi, M.; Takao, T.; Saito, A.; Fujii, Y. Facial nerve motor-evoked potential monitoring during skull base surgery predicts facial nerve outcome. J. Neurol. Neurosurg. Psychiatry 2008, 79, 1066–1070. [Google Scholar] [CrossRef] [PubMed]
- Bernardeschi, D.; Pyatigorskaya, N.; Vanier, A.; Bielle, F.; Smail, M.; Lamas, G.; Sterkers, O.; Kalamarides, M. Role of electrophysiology in guiding near-total resection for preservation of facial nerve function in the surgical treatment of large vestibular schwannomas. J. Neurosurg. 2018, 128, 903–910. [Google Scholar] [CrossRef] [PubMed]
- Tokimura, H.; Sugata, S.; Yamahata, H.; Yunoue, S.; Hanaya, R.; Arita, K. Intraoperative continuous monitoring of facial motor evoked potentials in acoustic neuroma surgery. Neurosurg. Rev. 2014, 37, 669–676. [Google Scholar] [CrossRef]
- Chibbaro, S.; Di Rocco, F.; Makiese, O.; Mirone, G.; Marsella, M.; Lukaszewicz, A.C.; Vicaut, E.; Turner, B.; Hamdi, S.; Spiriev, T.; et al. Neurosurgery and elderly: Analysis through the years. Neurosurg. Rev. 2010, 34, 229–234. [Google Scholar] [CrossRef]
- Edlmann, E.; Whitfield, P.C. The changing face of neurosurgery for the older person. J. Neurol. 2020, 267, 2469–2474. [Google Scholar] [CrossRef]
- Burke, S.N.; Barnes, C.A. Neural plasticity in the ageing brain. Nat. Rev. Neurosci. 2006, 7, 30–40. [Google Scholar] [CrossRef] [PubMed]
- Hembd, A.; Nagarkar, P.; Perez, J.; Gassman, A.; Tolley, P.; Reisch, J.; White, C.; Rozen, S.M. Correlation between Facial Nerve Axonal Load and Age and Its Relevance to Facial Reanimation. Plast. Reconstr. Surg. 2017, 139, 1459–1464. [Google Scholar] [CrossRef] [PubMed]
- Kawabuchi, M.; Tan, H.; Wang, S. Age affects reciprocal cellular interactions in neuromuscular synapses following peripheral nerve injury. Ageing Res. Rev. 2011, 10, 43–53. [Google Scholar] [CrossRef]
- Saito, T.; Muragaki, Y.; Tamura, M.; Maruyama, T.; Nitta, M.; Tsuzuki, S.; Fukui, A.; Koriyama, S.; Kawamata, T. Monitoring Cortico-cortical Evoked Potentials Using Only Two 6-strand Strip Electrodes for Gliomas Extending to the Dominant Side of Frontal Operculum During One-step Tumor Removal Surgery. World Neurosurg. 2022, 165, e732–e742. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Value (Age 65–69 Years) | Value (Age ≥ 70 Years) | p |
|---|---|---|---|
| n patients | 17 | 18 | NA |
| Age (mean ± SD) | 66.8 ± 1.5 years | 73.4 ± 2.8 years | NA |
| Sex (M:F, n (%)) | 7:10 (41.2%:58.8%) | 7:11 (38.9%:61.1%) | <0.99 # |
| Pathology Schwannoma Meningioma | 13 (76.5%) 4 (23.5%) | 10 (55.6%) 8 (44.4%) | 0.0315 # |
| Follow-up (median, range) | 12 months (6–41) | 13.5 months (6–33) | 0.0244 § |
| GTR, n (%) | 11 (64.7%) | 16 (88.9%) | 0.1212 # |
| Good FN function (House-Brackmann 1–2) Pre-operative Early post-operative Late post-operative * | 17 (100%) 10 (58.8%) 12 (75%) | 18 (100%) 10 (55.6%) 14 (82.4%) | >0.99 # >0.99 # 0.6880 # |
| Parameter | Age 65–70 Years | Age ≥ 70 Years | p § |
|---|---|---|---|
| Minimum-to-baseline amplitude ratio (MBR) (mean ± SD) Oculi Oris | 24.8% ± 37.2% 33.7% ± 35.1% | 20.9% ± 35.3% 41.9% ± 36.2% | 0.84 0.4379 |
| Final-to-baseline amplitude ratio (FBR) (mean ± SD) Oculi Oris | 37.0% ± 39.1% 60.8% ± 35.9% | 34.3% ± 43.8% 57.6% ± 35.0% | 0.9147 0.7343 |
| Recovery Value (RV) (mean ± SD) Oculi Oris | 11.0% ± 19.7% 24.0% ± 35.6% | 13.4% ± 23.3% 15.7% ± 23.6% | 0.7705 0.5379 |
| FMEP Index (Age) | Age 65–69 Years | Age ≥ 70 Years | |||
|---|---|---|---|---|---|
| AUC | p-Value | AUC | p-Value | ||
| Orbicularis oculi | MBR | 0.714 | 0.2453 | 0.833 | 0.0091 |
| FBR | 0.857 | 0.0062 | 0.881 | 0.0003 | |
| RV | 0.714 | 0.1992 | 0.714 | 0.1725 | |
| Orbicularis oris | MBR | 0.680 | 0.2024 | 0.905 | <0.0001 |
| FBR | 0.700 | 0.1513 | 0.937 | <0.0001 | |
| RV | 0.520 | 0.8999 | 0.524 | 0.8733 | |
| FMEP Index | Age 65–69 Years | Age ≥ 70 Years | |||
|---|---|---|---|---|---|
| AUC | p-Value | AUC | p-Value | ||
| Orbicularis oculi | MBR | NA | NA | 0.722 | 0.1433 |
| FBR | NA | NA | 0.833 | 0.0049 | |
| RV | NA | NA | 0.778 | 0.0416 | |
| Orbicularis oris | MBR | 0.697 | 0.1803 | 0.931 | <0.0001 |
| FBR | 0.833 | 0.0091 | 0.875 | 0.0005 | |
| RV | 0.500 | >0.99 | 0.583 | 0.6780 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
D’Alessandris, Q.G.; Menna, G.; Stifano, V.; Della Pepa, G.M.; Burattini, B.; Di Domenico, M.; Izzo, A.; D’Ercole, M.; Lauretti, L.; Montano, N.; et al. A Study on the Role of Intraoperative Corticobulbar Motor Evoked Potentials for Improving Safety of Cerebellopontine Angle Surgery in Elderly Patients. Diagnostics 2023, 13, 710. https://doi.org/10.3390/diagnostics13040710
D’Alessandris QG, Menna G, Stifano V, Della Pepa GM, Burattini B, Di Domenico M, Izzo A, D’Ercole M, Lauretti L, Montano N, et al. A Study on the Role of Intraoperative Corticobulbar Motor Evoked Potentials for Improving Safety of Cerebellopontine Angle Surgery in Elderly Patients. Diagnostics. 2023; 13(4):710. https://doi.org/10.3390/diagnostics13040710
Chicago/Turabian StyleD’Alessandris, Quintino Giorgio, Grazia Menna, Vito Stifano, Giuseppe Maria Della Pepa, Benedetta Burattini, Michele Di Domenico, Alessandro Izzo, Manuela D’Ercole, Liverana Lauretti, Nicola Montano, and et al. 2023. "A Study on the Role of Intraoperative Corticobulbar Motor Evoked Potentials for Improving Safety of Cerebellopontine Angle Surgery in Elderly Patients" Diagnostics 13, no. 4: 710. https://doi.org/10.3390/diagnostics13040710
APA StyleD’Alessandris, Q. G., Menna, G., Stifano, V., Della Pepa, G. M., Burattini, B., Di Domenico, M., Izzo, A., D’Ercole, M., Lauretti, L., Montano, N., & Olivi, A. (2023). A Study on the Role of Intraoperative Corticobulbar Motor Evoked Potentials for Improving Safety of Cerebellopontine Angle Surgery in Elderly Patients. Diagnostics, 13(4), 710. https://doi.org/10.3390/diagnostics13040710