
Attention Deep Feature Extraction from Brain MRIs in Explainable Mode: DGXAINet


Abstract
:1. Introduction
1.1. Novelties and Contributions
- -
- We have used deep learning as preprocessing model to create an XAI model.
- -
- A patch-based deep feature extraction model has been proposed.
- -
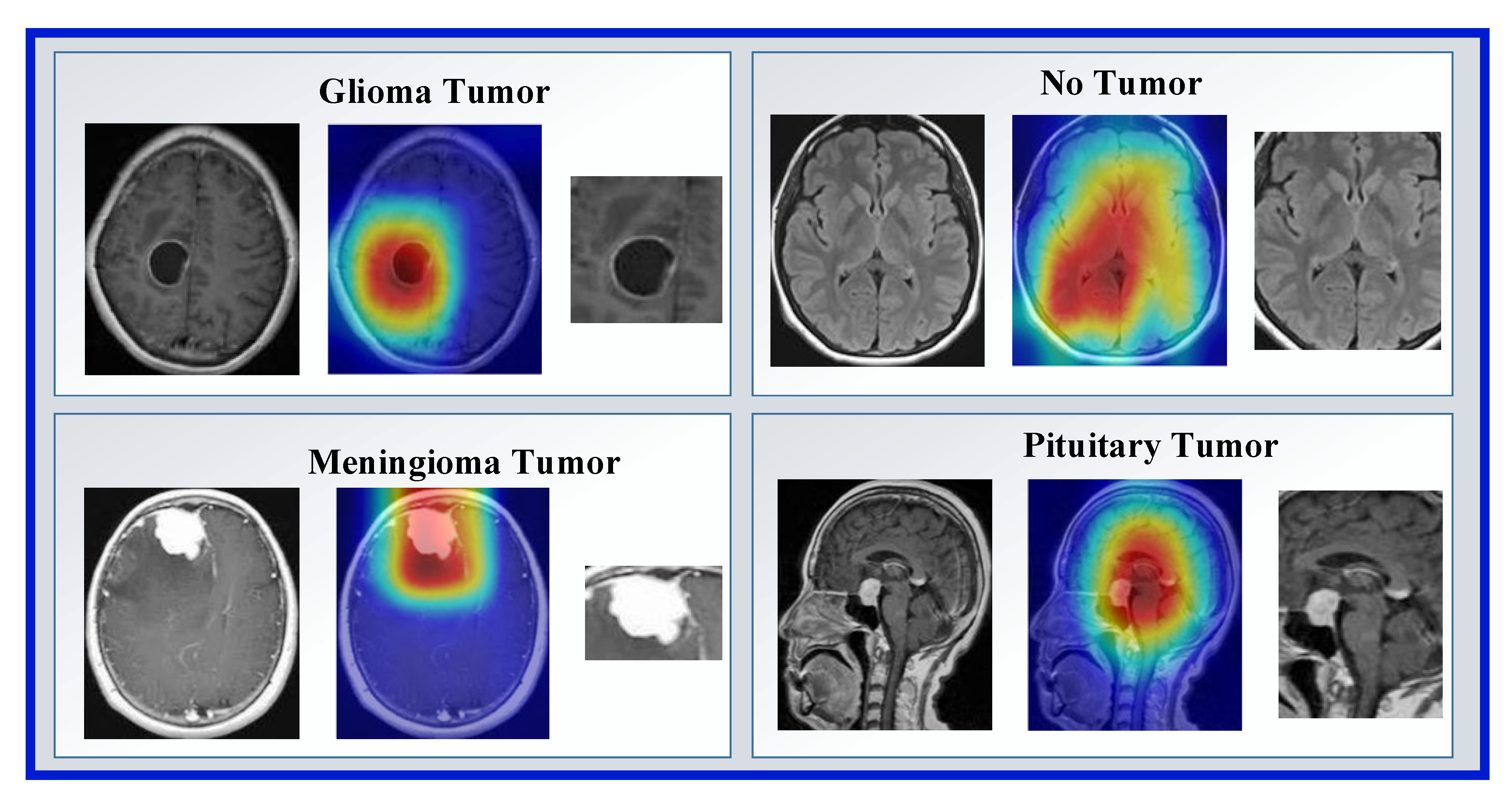
- A new XAI strategy has been used for brain tumor classification.
1.2. Contributions
- -
- Brain tumor classification is a hot-topic research area for biomedical image classification, and XAI models have been proposed in this area to assist medical professionals. However, there are limited XAI models. In this research, we have proposed an XAI model to fill this gap and increase classification performance.
- -
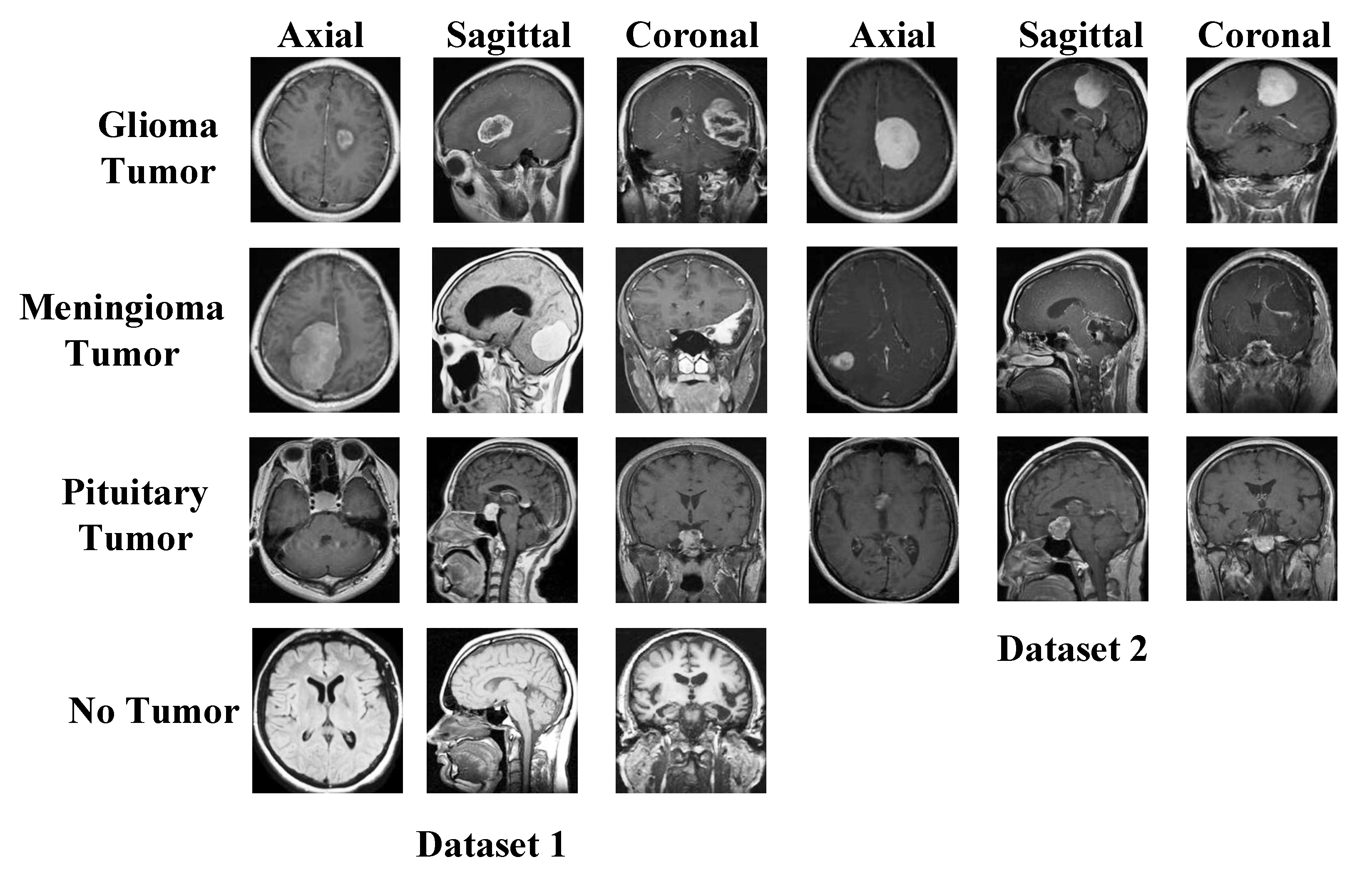
- To show the superiority of our proposal, we have used two public brain tumor image datasets. These datasets contain four and three categories. We obtained a pre-trained network by using a dataset with four classes and DenseNet201. Using this pretrained DenseNet201, preprocessing and feature extraction layers of our model have been created. In this respect, a deep learning-based cognitive model has been created. Moreover, our model attained superior classification performances than other state-of-art models.
2. Materials
2.1. Dataset I
2.2. Dataset II
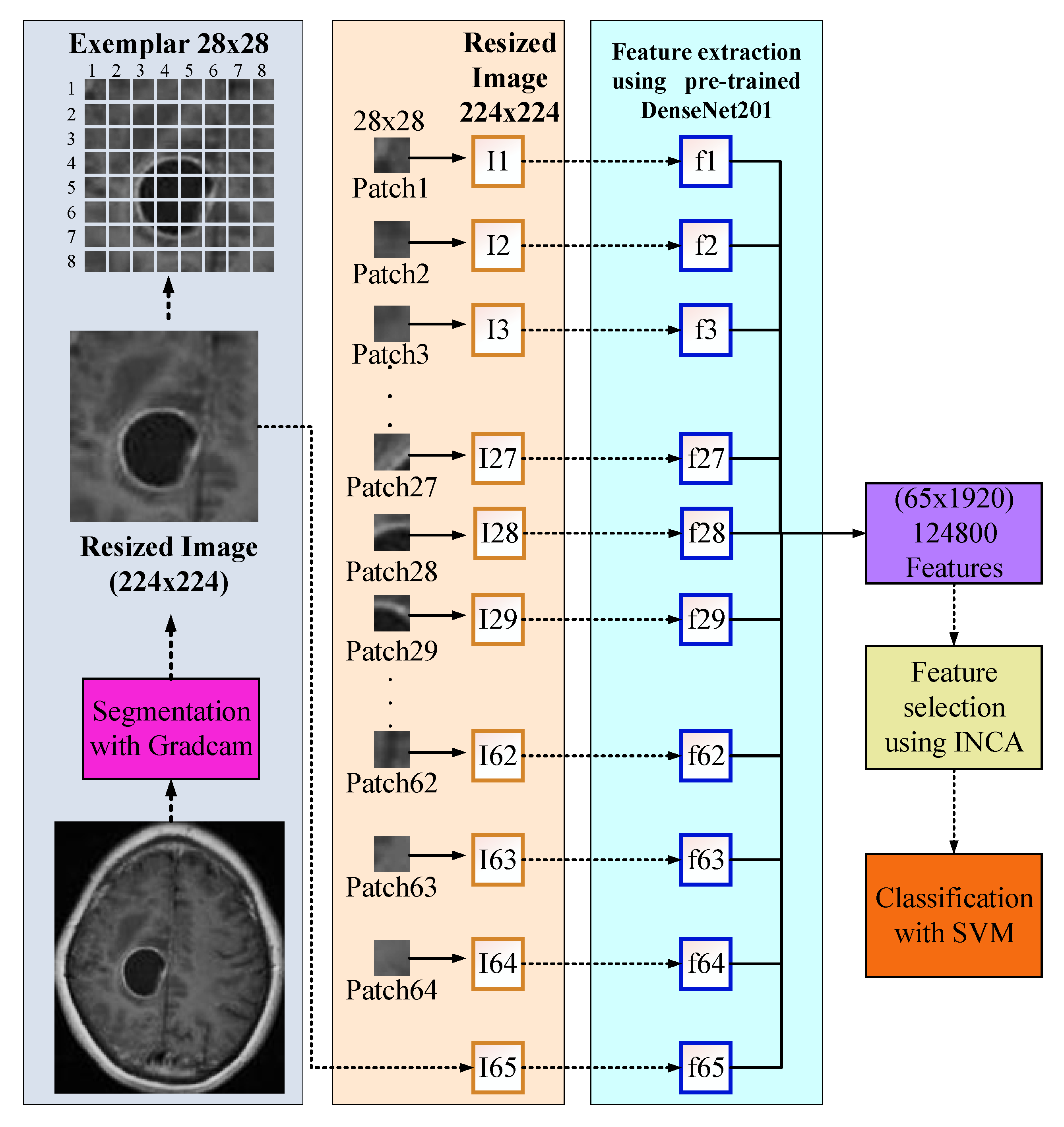
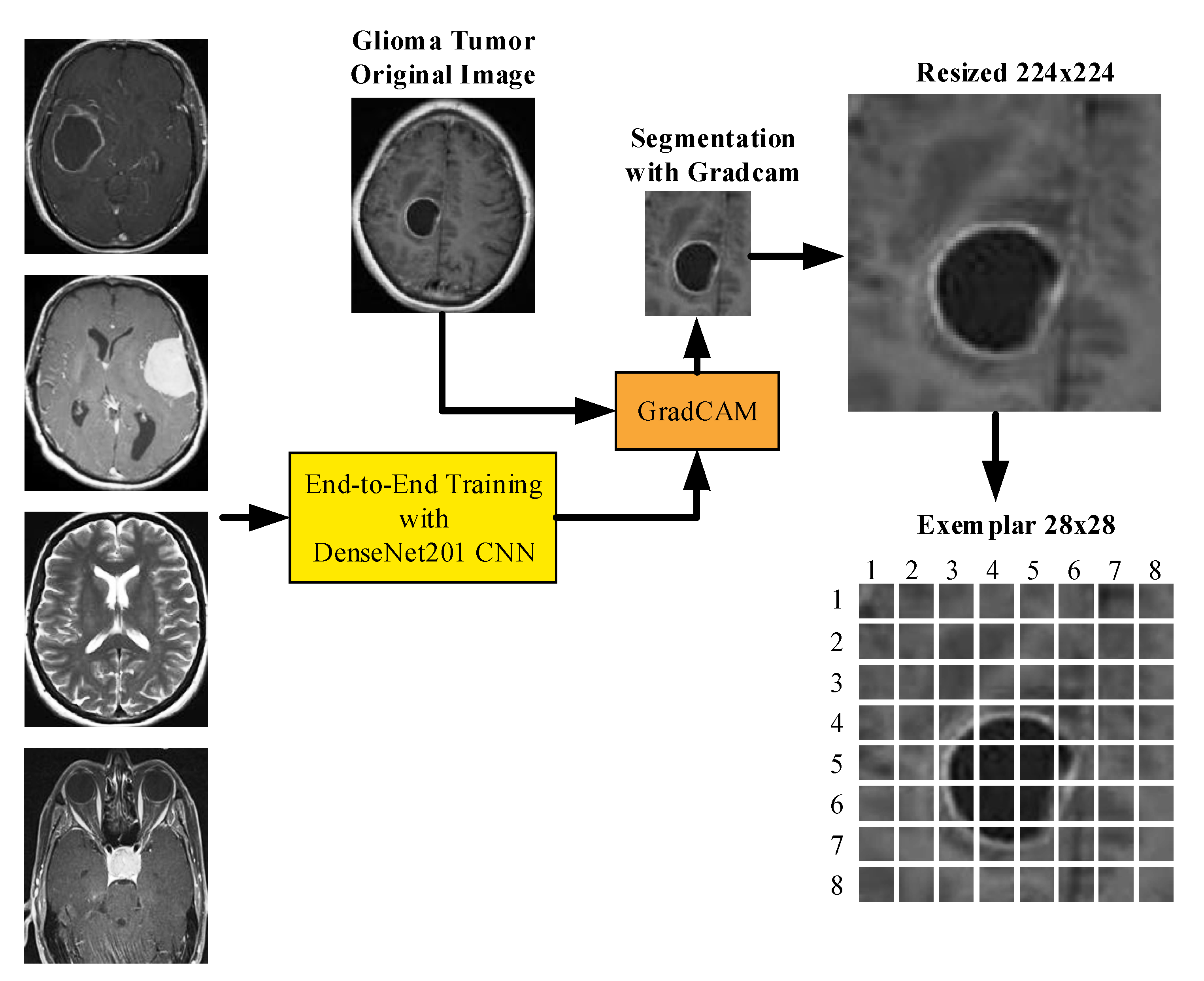
3. The Proposed DenseNet201 and Grad-Cam-Based Brain Tumor Detection Model
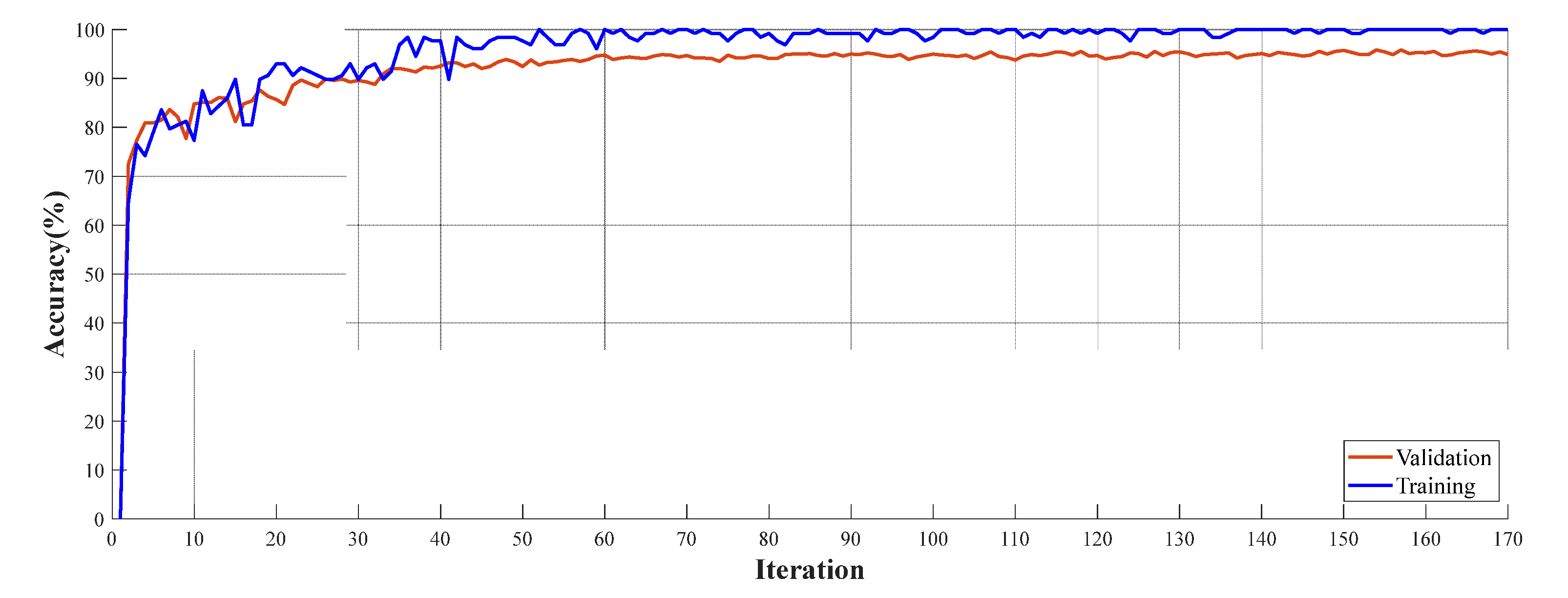
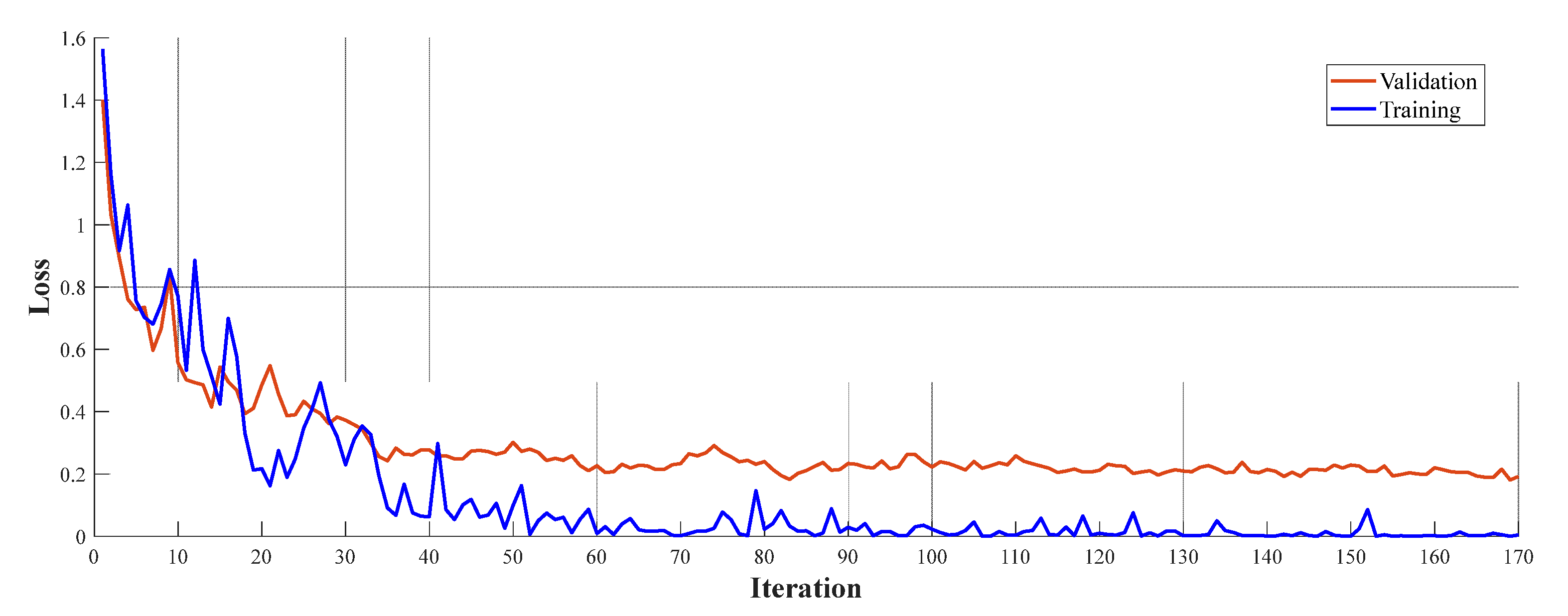
3.1. Training Dataset
3.2. Preprocessing
3.3. Feature Extraction
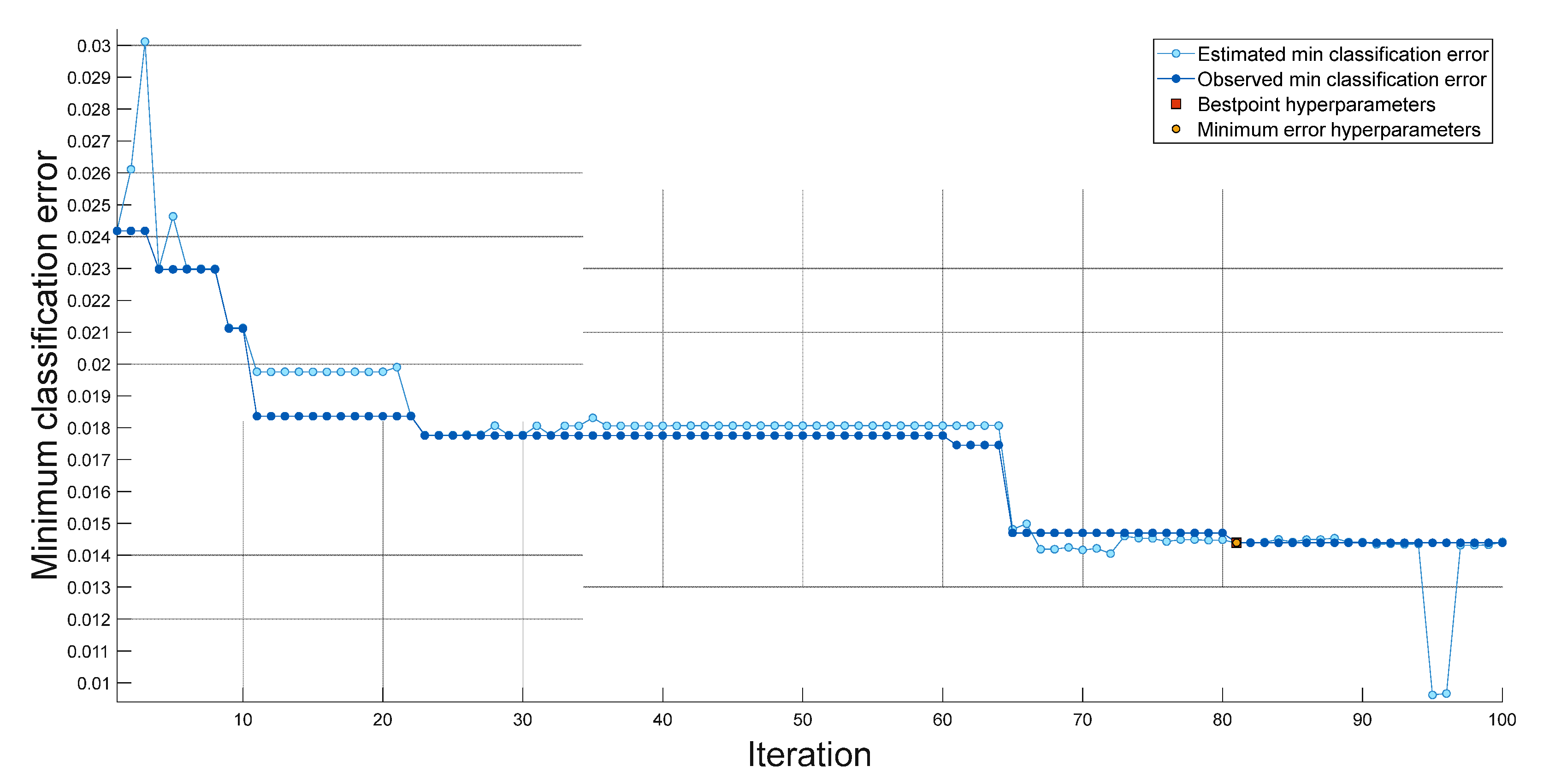
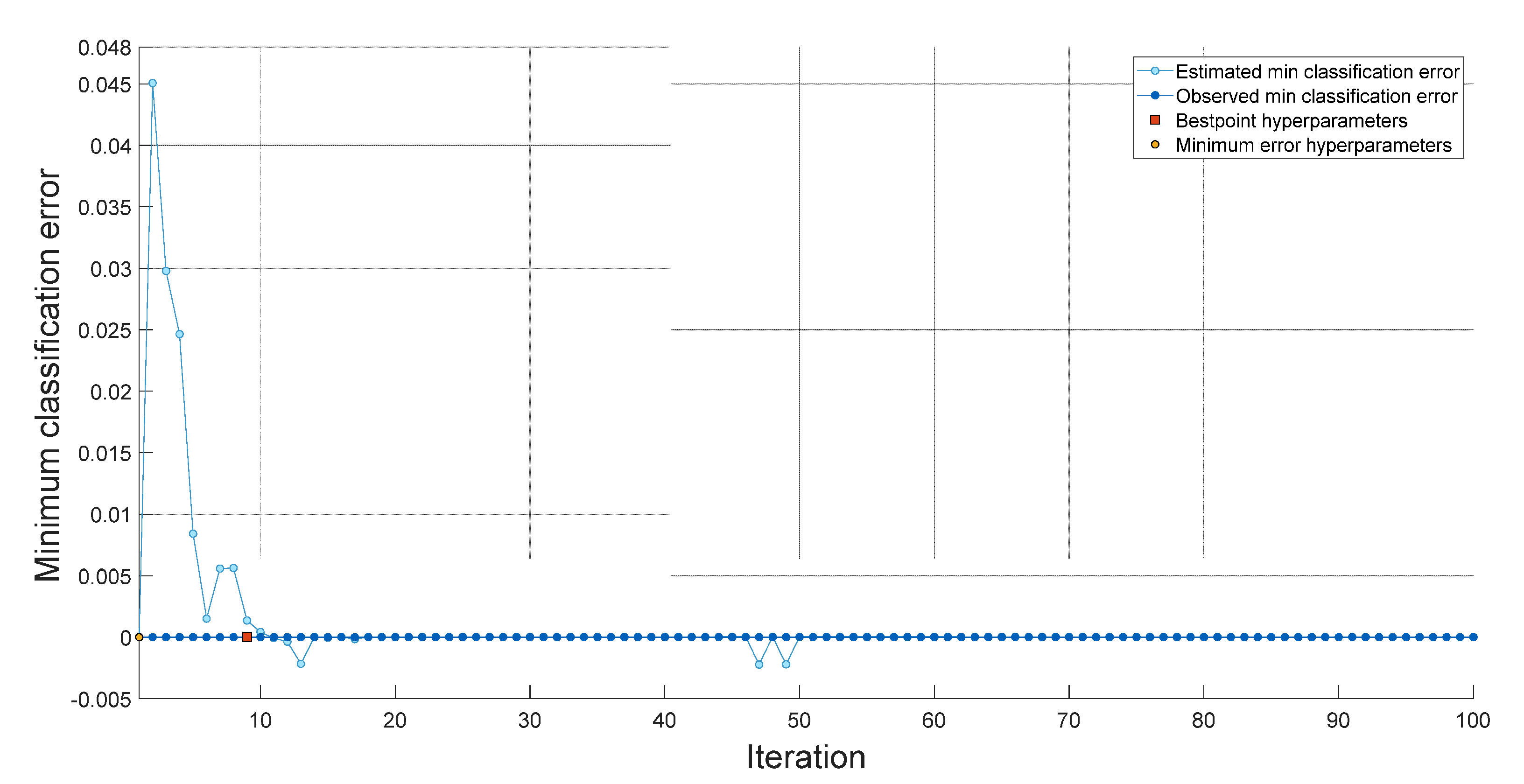
3.4. Feature Selection
3.5. Classification
- -
- As input for optimization, variable class values are used. The objective function is defined in the objective function with the valid values of the optimization variables in a table where each column name matches the variable name.
- -
- Training options for network architecture and optimization are defined.
- -
- The network is trained and validated.
- -
- The trained network is saved with training options on validation error and optimization.
4. Experimental Results
5. Discussion
6. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Parkin, D.M.; Piñeros, M.; Znaor, A.; Bray, F. Cancer statistics for the year 2020: An overview. Int. J. Cancer 2021, 149, 778–789. [Google Scholar] [CrossRef] [PubMed]
- Global Cancer Observatory (GCO). Available online: https://gco.iarc.fr/tomorrow/en/dataviz/isotype (accessed on 16 October 2022).
- Tandel, G.S.; Biswas, M.; Kakde, O.G.; Tiwari, A.; Suri, H.S.; Turk, M.; Laird, J.R.; Asare, C.K.; Ankrah, A.A.; Khanna, N. A review on a deep learning perspective in brain cancer classification. Cancers 2019, 11, 111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kleihues, P.; Burger, P.C.; Scheithauer, B.W. The new WHO classification of brain tumours. Brain Pathol. 1993, 3, 255–268. [Google Scholar] [CrossRef] [PubMed]
- Ronald Warnick, Y.G. Brain Tumors: An Introduction. Available online: https://mayfieldclinic.com/pe-braintumor.htm (accessed on 16 October 2022).
- Bauer, S.; Wiest, R.; Nolte, L.-P.; Reyes, M. A survey of MRI-based medical image analysis for brain tumor studies. Phys. Med. Biol. 2013, 58, R97. [Google Scholar] [CrossRef] [Green Version]
- Alberts, B.; Johnson, A.; Lewis, J.; Raff, M.; Roberts, K.; Walter, P. Blood vessels and endothelial cells. In Molecular Biology of the Cell, 4th ed.; Garland Science: New York, NY, USA, 2002. [Google Scholar]
- Nadeem, M.W.; Ghamdi, M.A.A.; Hussain, M.; Khan, M.A.; Khan, K.M.; Almotiri, S.H.; Butt, S.A. Brain tumor analysis empowered with deep learning: A review, taxonomy, and future challenges. Brain Sci. 2020, 10, 118. [Google Scholar] [CrossRef] [Green Version]
- Işın, A.; Direkoğlu, C.; Şah, M. Review of MRI-based brain tumor image segmentation using deep learning methods. Procedia Comput. Sci. 2016, 102, 317–324. [Google Scholar] [CrossRef] [Green Version]
- Gudigar, A.; Raghavendra, U.; San, T.R.; Ciaccio, E.J.; Acharya, U.R. Application of multiresolution analysis for automated detection of brain abnormality using MR images: A comparative study. Future Gener. Comput. Syst. 2019, 90, 359–367. [Google Scholar] [CrossRef]
- Akkus, Z.; Galimzianova, A.; Hoogi, A.; Rubin, D.L.; Erickson, B.J. Deep learning for brain MRI segmentation: State of the art and future directions. J. Digit. Imaging 2017, 30, 449–459. [Google Scholar] [CrossRef] [Green Version]
- Gudigar, A.; Raghavendra, U.; Ciaccio, E.J.; Arunkumar, N.; Abdulhay, E.; Acharya, U.R. Automated categorization of multi-class brain abnormalities using decomposition techniques with MRI images: A comparative study. IEEE Access 2019, 7, 28498–28509. [Google Scholar] [CrossRef]
- Zhao, X.; Wu, Y.; Song, G.; Li, Z.; Zhang, Y.; Fan, Y. A deep learning model integrating FCNNs and CRFs for brain tumor segmentation. Med. Image Anal. 2018, 43, 98–111. [Google Scholar] [CrossRef]
- Mohsen, H.; El-Dahshan, E.-S.A.; El-Horbaty, E.-S.M.; Salem, A.-B.M. Classification using deep learning neural networks for brain tumors. Future Comput. Inform. J. 2018, 3, 68–71. [Google Scholar] [CrossRef]
- Saba, T.; Mohamed, A.S.; El-Affendi, M.; Amin, J.; Sharif, M. Brain tumor detection using fusion of hand crafted and deep learning features. Cogn. Syst. Res. 2020, 59, 221–230. [Google Scholar] [CrossRef]
- Gudigar, A.; Raghavendra, U.; Hegde, A.; Kalyani, M.; Ciaccio, E.J.; Acharya, U.R. Brain pathology identification using computer aided diagnostic tool: A systematic review. Comput. Methods Programs Biomed. 2020, 187, 105205. [Google Scholar] [CrossRef]
- Raghavendra, U.; Gudigar, A.; Rao, T.N.; Rajinikanth, V.; Ciaccio, E.J.; Yeong, C.H.; Satapathy, S.C.; Molinari, F.; Acharya, U.R. Feature-versus deep learning-based approaches for the automated detection of brain tumor with magnetic resonance images: A comparative study. Int. J. Imaging Syst. Technol. 2022, 32, 501–516. [Google Scholar] [CrossRef]
- Gudigar, A.; Raghavendra, U.; Rao, T.N.; Samanth, J.; Rajinikanth, V.; Satapathy, S.C.; Ciaccio, E.J.; Wai Yee, C.; Acharya, U.R. FFCAEs: An efficient feature fusion framework using cascaded autoencoders for the identification of gliomas. Int. J. Imaging Syst. Technol. 2022, 1–12. [Google Scholar] [CrossRef]
- Lee, C.S.; Nagy, P.G.; Weaver, S.J.; Newman-Toker, D.E. Cognitive and system factors contributing to diagnostic errors in radiology. Am. J. Roentgenol. 2013, 201, 611–617. [Google Scholar] [CrossRef]
- Obermeyer, Z.; Emanuel, E.J. Predicting the Future—Big Data, Machine Learning, and Clinical Medicine. N. Engl. J. Med. 2016, 375, 1216–1219. [Google Scholar] [CrossRef] [Green Version]
- Arimura, H. Image-Based Computer-Assisted Radiation Therapy; Springer: Singapore, 2017. [Google Scholar]
- Dawson, L.A.; Jaffray, D.A. Advances in image-guided radiation therapy. J. Clin. Oncol. 2007, 25, 938–946. [Google Scholar] [CrossRef]
- Nishio, M.; Nagashima, C. Computer-aided diagnosis for lung cancer: Usefulness of nodule heterogeneity. Acad. Radiol. 2017, 24, 328–336. [Google Scholar] [CrossRef]
- Raza, A.; Ayub, H.; Khan, J.A.; Ahmad, I.; Salama, A.S.; Daradkeh, Y.I.; Javeed, D.; Ur Rehman, A.; Hamam, H. A hybrid deep learning-based approach for brain tumor classification. Electronics 2022, 11, 1146. [Google Scholar] [CrossRef]
- Khazaee, Z.; Langarizadeh, M.; Ahmadabadi, M.E.S. Developing an Artificial Intelligence Model for Tumor Grading and Classification, Based on MRI Sequences of Human Brain Gliomas. Int. J. Cancer Manag. 2022, 15, e120638. [Google Scholar] [CrossRef]
- El Hamdaoui, H.; Benfares, A.; Boujraf, S.; Chaoui, N.E.H.; Alami, B.; Maaroufi, M.; Qjidaa, H. High precision brain tumor classification model based on deep transfer learning and stacking concepts. Indones. J. Electr. Eng. Comput. Sci. 2021, 24, 167–177. [Google Scholar] [CrossRef]
- Tandel, G.S.; Tiwari, A.; Kakde, O. Performance optimisation of deep learning models using majority voting algorithm for brain tumour classification. Comput. Biol. Med. 2021, 135, 104564. [Google Scholar] [CrossRef] [PubMed]
- Rizwan, M.; Shabbir, A.; Javed, A.R.; Shabbir, M.; Baker, T.; Obe, D.A.-J. Brain tumor and glioma grade classification using gaussian convolutional neural network. IEEE Access 2022, 10, 29731–29740. [Google Scholar] [CrossRef]
- Tariciotti, L.; Caccavella, V.M.; Fiore, G.; Schisano, L.; Carrabba, G.; Borsa, S.; Giordano, M.; Palmisciano, P.; Remoli, G.; Remore, L.G.; et al. A Deep Learning Model for Preoperative Differentiation of Glioblastoma, Brain Metastasis and Primary Central Nervous System Lymphoma: A Pilot Study. Front. Oncol. 2022, 12, 816638. [Google Scholar] [CrossRef]
- Majib, M.S.; Rahman, M.M.; Sazzad, T.S.; Khan, N.I.; Dey, S.K. Vgg-scnet: A vgg net-based deep learning framework for brain tumor detection on mri images. IEEE Access 2021, 9, 116942–116952. [Google Scholar] [CrossRef]
- Mehrotra, R.; Ansari, M.; Agrawal, R.; Anand, R. A transfer learning approach for AI-based classification of brain tumors. Mach. Learn. Appl. 2020, 2, 100003. [Google Scholar] [CrossRef]
- Kaur, T.; Gandhi, T.K. Deep convolutional neural networks with transfer learning for automated brain image classification. Mach. Vis. Appl. 2020, 31, 20. [Google Scholar] [CrossRef]
- Begum, S.S.; Lakshmi, D.R. Combining optimal wavelet statistical texture and recurrent neural network for tumour detection and classification over MRI. Multimed. Tools Appl. 2020, 79, 14009–14030. [Google Scholar] [CrossRef]
- Marmolejo-Saucedo, J.A.; Kose, U. Numerical grad-CAM based explainable convolutional neural network for brain tumor diagnosis. Mob. Netw. Appl. 2022, 1–10. [Google Scholar] [CrossRef]
- Etminani, K.; Soliman, A.; Byttner, S.; Davidsson, A.; Ochoa-Figueroa, M. Peeking inside the box: Transfer Learning vs 3D convolutional neural networks applied in neurodegenerative diseases. In Proceedings of the 2021 International Conference on Computational Intelligence Methods for Bioinformatics and Biostatistics (CIBB 2021), Online, 15–17 November 2021. [Google Scholar]
- Kaur, A.; Dong, G.; Basu, A. GradXcepUNet: Explainable AI Based Medical Image Segmentation. In Proceedings of the Smart Multimedia: Third International Conference, ICSM 2022, Marseille, France, 25–27 August 2022; pp. 174–188. [Google Scholar]
- Bhuvaji, S.; Kadam, A.; Bhumkar, P.; Dedge, S.; Kanchan, S. Brain tumor classification (MRI). Kaggle 2020, 10. [Google Scholar] [CrossRef]
- Cheng, J. Brain Tumor Dataset; Figshare: London, UK, 2017. [Google Scholar] [CrossRef]
- Huang, G.; Liu, Z.; Van Der Maaten, L.; Weinberger, K.Q. Densely connected convolutional networks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 4700–4708. [Google Scholar]
- Loh, H.W.; Ooi, C.P.; Seoni, S.; Barua, P.D.; Molinari, F.; Acharya, U.R. Application of explainable artificial intelligence for healthcare: A systematic review of the last decade (2011–2022). Comput. Methods Programs Biomed. 2022, 226, 107161. [Google Scholar] [CrossRef]
- Selvaraju, R.R.; Cogswell, M.; Das, A.; Vedantam, R.; Parikh, D.; Batra, D. Grad-cam: Visual explanations from deep networks via gradient-based localization. In Proceedings of the IEEE International Conference on Computer Vision, Venice, Italy, 22–29 October 2017; pp. 618–626. [Google Scholar]
- GradCam. Available online: https://jp.mathworks.com/help/deeplearning/ref/gradcam.html (accessed on 29 October 2022).
- Goldberger, J.; Hinton, G.E.; Roweis, S.; Salakhutdinov, R.R. Neighbourhood components analysis. In Proceedings of the Advances in Neural Information Processing Systems 17, Vancouver, BC, Canada, 13–18 December 2004. [Google Scholar]
- Tuncer, T.; Ozyurt, F.; Dogan, S.; Subasi, A. A novel COVID-19 and pneumonia classification method based on F-transform. Chemom. Intell. Lab. Syst. 2021, 210, 104256. [Google Scholar] [CrossRef]
- Mockus, J. Bayesian Approach to Global Optimization: Theory and Applications; Springer Science & Business Media: Dordrecht, The Netherlands, 2012; Volume 37. [Google Scholar]
- Taşcı, B.; Acharya, M.R.; Barua, P.D.; Yildiz, A.M.; Gun, M.V.; Keles, T.; Dogan, S.; Tuncer, T. A new lateral geniculate nucleus pattern-based environmental sound classification using a new large sound dataset. Appl. Acoust. 2022, 196, 108897. [Google Scholar] [CrossRef]
- Macin, G.; Tasci, B.; Tasci, I.; Faust, O.; Barua, P.D.; Dogan, S.; Tuncer, T.; Tan, R.-S.; Acharya, U.R. An accurate multiple sclerosis detection model based on exemplar multiple parameters local phase quantization: ExMPLPQ. Appl. Sci. 2022, 12, 4920. [Google Scholar] [CrossRef]
- Demir, F. DeepCoroNet: A deep LSTM approach for automated detection of COVID-19 cases from chest X-ray images. Appl. Soft Comput. 2021, 103, 107160. [Google Scholar] [CrossRef]
- Tasci, B.; Tasci, I. Deep feature extraction based brain image classification model using preprocessed images: PDRNet. Biomed. Signal Process. Control 2022, 78, 103948. [Google Scholar] [CrossRef]
- Dogan, S.; Baygin, M.; Tasci, B.; Loh, H.W.; Barua, P.D.; Tuncer, T.; Tan, R.-S.; Acharya, U.R. Primate brain pattern-based automated Alzheimer’s disease detection model using EEG signals. Cogn. Neurodyn. 2022, 1–13. [Google Scholar] [CrossRef]
- Tasci, G.; Loh, H.W.; Barua, P.D.; Baygin, M.; Tasci, B.; Dogan, S.; Tuncer, T.; Palmer, E.E.; Tan, R.-S.; Acharya, U.R. Automated accurate detection of depression using twin Pascal’s triangles lattice pattern with EEG Signals. Knowl. Based Syst. 2023, 260, 110190. [Google Scholar] [CrossRef]
- Demir, F.; Akbulut, Y.; Taşcı, B.; Demir, K. Improving brain tumor classification performance with an effective approach based on new deep learning model named 3ACL from 3D MRI data. Biomed. Signal Process. Control 2023, 81, 104424. [Google Scholar] [CrossRef]
- Tasci, B. Automated ischemic acute infarction detection using pre-trained CNN models’ deep features. Biomed. Signal Process. Control 2023, 82, 104603. [Google Scholar] [CrossRef]
- Demir, F. DeepBreastNet: A novel and robust approach for automated breast cancer detection from histopathological images. Biocybern. Biomed. Eng. 2021, 41, 1123–1139. [Google Scholar] [CrossRef]
- Tasci, B.; Tasci, G.; Dogan, S.; Tuncer, T. A novel ternary pattern-based automatic psychiatric disorders classification using ECG signals. Cogn. Neurodyn. 2022, 1–14. [Google Scholar] [CrossRef]
- Alanazi, M.F.; Ali, M.U.; Hussain, S.J.; Zafar, A.; Mohatram, M.; Irfan, M.; AlRuwaili, R.; Alruwaili, M.; Ali, N.H.; Albarrak, A.M. Brain tumor/mass classification framework using magnetic-resonance-imaging-based isolated and developed transfer deep-learning model. Sensors 2022, 22, 372. [Google Scholar] [CrossRef] [PubMed]
- Başaran, E. A new brain tumor diagnostic model: Selection of textural feature extraction algorithms and convolution neural network features with optimization algorithms. Comput. Biol. Med. 2022, 148, 105857. [Google Scholar] [CrossRef]
- Belciug, S. Learning deep neural networks’ architectures using differential evolution. Case study: Medical imaging processing. Comput. Biol. Med. 2022, 146, 105623. [Google Scholar] [CrossRef]
- Ait Amou, M.; Xia, K.; Kamhi, S.; Mouhafid, M. A Novel MRI Diagnosis Method for Brain Tumor Classification Based on CNN and Bayesian Optimization. Healthcare 2022, 10, 494. [Google Scholar] [CrossRef]
- Asthana, P.; Hanmandlu, M.; Vashisth, S. Classification of brain tumor from magnetic resonance images using probabilistic features and possibilistic Hanman–Shannon transform classifier. Int. J. Imaging Syst. Technol. 2022, 32, 280–294. [Google Scholar] [CrossRef]
- Rasool, M.; Ismail, N.A.; Boulila, W.; Ammar, A.; Samma, H.; Yafooz, W.M.; Emara, A.-H.M. A Hybrid Deep Learning Model for Brain Tumour Classification. Entropy 2022, 24, 799. [Google Scholar] [CrossRef]
- Kumar, R.L.; Kakarla, J.; Isunuri, B.V.; Singh, M. Multi-class brain tumor classification using residual network and global average pooling. Multimed. Tools Appl. 2021, 80, 13429–13438. [Google Scholar] [CrossRef]
- Díaz-Pernas, F.J.; Martínez-Zarzuela, M.; Antón-Rodríguez, M.; González-Ortega, D. A deep learning approach for brain tumor classification and segmentation using a multiscale convolutional neural network. Healthcare 2021, 9, 153. [Google Scholar] [CrossRef] [PubMed]
- Noreen, N.; Palaniappan, S.; Qayyum, A.; Ahmad, I.; Alassafi, M.O. Brain tumor classification based on fine-tuned models and the ensemble method. Comput. Mater. Contin. 2021, 67, 3967–3982. [Google Scholar] [CrossRef]
- Kakarla, J.; Isunuri, B.V.; Doppalapudi, K.S.; Bylapudi, K.S.R. Three-class classification of brain magnetic resonance images using average-pooling convolutional neural network. Int. J. Imaging Syst. Technol. 2021, 31, 1731–1740. [Google Scholar] [CrossRef]
- Alhassan, A.M.; Zainon, W.M.N.W. Brain tumor classification in magnetic resonance image using hard swish-based RELU activation function-convolutional neural network. Neural Comput. Appl. 2021, 33, 9075–9087. [Google Scholar] [CrossRef]
- Gab Allah, A.M.; Sarhan, A.M.; Elshennawy, N.M. Classification of Brain MRI Tumor Images Based on Deep Learning PGGAN Augmentation. Diagnostics 2021, 11, 2343. [Google Scholar] [CrossRef] [PubMed]
- Gu, X.; Shen, Z.; Xue, J.; Fan, Y.; Ni, T. Brain tumor MR image classification using convolutional dictionary learning with local constraint. Front. Neurosci. 2021, 15, 679847. [Google Scholar] [CrossRef]
- Noreen, N.; Palaniappan, S.; Qayyum, A.; Ahmad, I.; Imran, M.; Shoaib, M. A deep learning model based on concatenation approach for the diagnosis of brain tumor. IEEE Access 2020, 8, 55135–55144. [Google Scholar] [CrossRef]
- Ghassemi, N.; Shoeibi, A.; Rouhani, M. Deep neural network with generative adversarial networks pre-training for brain tumor classification based on MR images. Biomed. Signal Process. Control 2020, 57, 101678. [Google Scholar] [CrossRef]
- Ismael, S.A.A.; Mohammed, A.; Hefny, H. An enhanced deep learning approach for brain cancer MRI images classification using residual networks. Artif. Intell. Med. 2020, 102, 101779. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Solver | Basic | Sequence | Advanced | ||||
|---|---|---|---|---|---|---|---|
| Solver | sgdm | Validation Frequency | 1 | Sequence Length | Longest | L2 Regularization | 0.0001 |
| Initial Learn Rate | 0.01 | Max Epochs | 20 | Sequence Padding Value | 0 | Gradient Threshold Method | I2norm |
| Iteration | 170 | Mini Batch Size | 128 | Sequence PaddingDirection | right | Shuffle | every Epoch |
| Hyperparameters | Dataset I | Dataset II |
|---|---|---|
| Multiclass method | One-vs-All | One-vs-One |
| Box Constraint level | 616.6747 | 987.8273 |
| Kernel Scale | 2.2347 | - |
| Kernel Function | Gaussian | Linear |
| Standardize data | False | False |
| Datasets | Patch Size | SVM (%) | Cubic KNN (%) | Fine Tree (%) | ANN (%) |
|---|---|---|---|---|---|
| Dataset I | 28 × 28 | 98.65 | 96.30 | 91.30 | 97.60 |
| 56 × 56 | 97.60 | 96.00 | 86.30 | 96.00 | |
| 112 × 112 | 96.70 | 95.40 | 85.90 | 95.60 | |
| Dataset II | 28 × 28 | 99.97 | 96.10 | 99.93 | 98.50 |
| 56 × 56 | 99.93 | 95.00 | 95.60 | 96.50 | |
| 112 × 112 | 96.50 | 95.70 | 85.30 | 95.60 |
| Datasets | Accuracy (% ± sd) | Precision (% ± sd) | Recall (% ± sd) | F1-Score (% ± sd) |
|---|---|---|---|---|
| Dataset I Glioma Tumor | 98.42 ± 0.11 | 97.99 ± 0.17 | 97.59 ± 0.19 | 98.40 ± 0.26 |
| Dataset I Meningioma Tumor | 97.63 ± 0.18 | 97.99 ± 0.23 | 97.28 ± 0.23 | |
| Dataset I No Tumor | 99.08 ± 0.12 | 99.06 ± 0.22 | 99.10 ± 0.12 | |
| Dataset I Pituitary Tumor | 99.30 ± 0.09 | 99.36 ± 0.16 | 99.24 ± 0.11 | |
| Dataset II Meningioma Tumor | 99.96 ± 0.01 | 100 ± 0.00 | 100 ± 0.00 | 100 ± 0.00 |
| Dataset II Glioma Tumor | 99.92 ± 0.02 | 100 ± 0.00 | 99.96 ± 0.01 | |
| Dataset II Pituitary Tumor | 100 ± 0.00 | 99.98 ± 0.03 | 99.94 ± 0.02 |
| Ref. (Year) | Dataset | Model | Split: Ratio | Results (%) |
|---|---|---|---|---|
| Alanazi et al. (2022) [56] | Dataset I Dataset II | 22 Layer CNN | 80:20 | Dataset I Accuracy = 95.75 Precision = 95.15 Sensitivity = 96.32 Dataset II Accuracy = 96.90 |
| Basaran et al. (2022) [57] | Dataset I | Gray level co-occurrence matrix (GLCM), Local Binary Pattern (LBP), AlexNet, VG16, EfficientNet, ResNet, PSO, GA, ABC, SVM | 5 Fold CV | Accuracy = 98.22 Precision = 97.84 Sensitivity = 98.27 Specificity = 99.43 F1 Score = 98.04 |
| Belciug et al. (2022) [58] | Dataset I | DE/CNN | Train:2870 image Test:394 image | Accuracy = 90.04 |
| Amou et al. (2022) [59] | Dataset II | Modified VGG16 CNN | 90:10 | Accuracy = 98.70 Precision = 98.30 Sensitivity = 98.60 F1 Score = 98.60 |
| Asthana et al. (2022) [60] | Dataset II | Hanman–Renyi transform, HSTC Classifier | 5 Fold CV | Accuracy = 98.91 Sensitivity = 98.92 Specificity = 99.47 |
| Rasool et al. (2022) [61] | Dataset II | Google-Net + SVM | 80:20 | Accuracy = 98.10 Precision = 98.20 Recall = 98.10 |
| Kumar et al. (2021) [62] | Dataset II | ResNet-50 CNN with global average pooling added | 5 Fold CV | Accuracy = 97.08 Precision = 98.3 Sensitivity = 98.6 F1 Score = 98.6 |
| Diaz-Pernaz et al. (2021) [63] | Dataset II | Multi-pathway CNN | 5 Fold CV | Accuracy = 97.30 |
| Noreen et al. (2021) [64] | Dataset II | Transfer learning with Inception-v3 Ensemble2 model | 10 Fold CV | Accuracy = 93.79 |
| Kakarla et al. (2021) [65] | Dataset II | Average pooling convolutional neural network (AP-CNN) model | 5 Fold CV | Accuracy = 97.42 Precision = 97.41 Recall = 97.42 |
| Alhassan et al. (2021) [66] | Dataset II | Hard swish-based RELU activation function-CNN | 80:20 | Accuracy = 98.60 Precision = 99.60 Recall = 98.60 F1 Score = 99.00 |
| Gab et al. (2021) [67] | Dataset II | PGGAN-augmentation VGG19 + Bi-GRU | Training:70 Test:15 Validation:15 | Accuracy = 98.54 Precision = 97.69 Sensitivity = 97.69 Specificity = 98.93 F1 Score = 97.69 |
| Gu et al.(2021) [68] | Dataset II | Custom CNN model (Convolutional dictionary learning with local constraint (CDLLC) | 5 Fold CV | Accuracy = 96.39 Precision = 94.61 Sensitivity = 94.64 F1 Score = 94.70 |
| Noreen et al.(2020) [69] | Dataset II | Transfer learning with Inception-v3, Densenet201 | 80:20 | Inception-v3 Accuracy = 99.34 Densenet201 Accuracy = 99.51 |
| Ghassemi et al.(2020) [70] | Dataset II | DCGAN CNN-GAN | 5 Fold CV | Accuracy = 95.60 Precision = 95.29 Sensitivity = 94.91 Specificity = 97.69 F1 Score = 95.10 |
| Ismael et al.(2020) [71] | Dataset II | ResNet50 CNN model | 80:20 | Accuracy = 99.00 Precision = 99.00 Recall = 99.00 F1 Score = 99.00 |
| Proposed Model | Dataset I Dataset II | Exemplar, DenseNet201, GradCam,SVM | 10 Fold CV | Dataset I Accuracy = 98.65 Pituitary Precision = 99.34 Recall = 99.56 F1 Score = 99.45 Dataset II Accuracy = 99.97 Meningioma Precision = 100 Recall = 100 F1 Score = 100 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Taşcı, B. Attention Deep Feature Extraction from Brain MRIs in Explainable Mode: DGXAINet. Diagnostics 2023, 13, 859. https://doi.org/10.3390/diagnostics13050859
Taşcı B. Attention Deep Feature Extraction from Brain MRIs in Explainable Mode: DGXAINet. Diagnostics. 2023; 13(5):859. https://doi.org/10.3390/diagnostics13050859
Chicago/Turabian StyleTaşcı, Burak. 2023. "Attention Deep Feature Extraction from Brain MRIs in Explainable Mode: DGXAINet" Diagnostics 13, no. 5: 859. https://doi.org/10.3390/diagnostics13050859
APA StyleTaşcı, B. (2023). Attention Deep Feature Extraction from Brain MRIs in Explainable Mode: DGXAINet. Diagnostics, 13(5), 859. https://doi.org/10.3390/diagnostics13050859