
Amide Proton Transfer–Chemical Exchange Saturation Transfer Imaging of Intracranial Brain Tumors and Tumor-like Lesions: Our Experience and a Review
 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
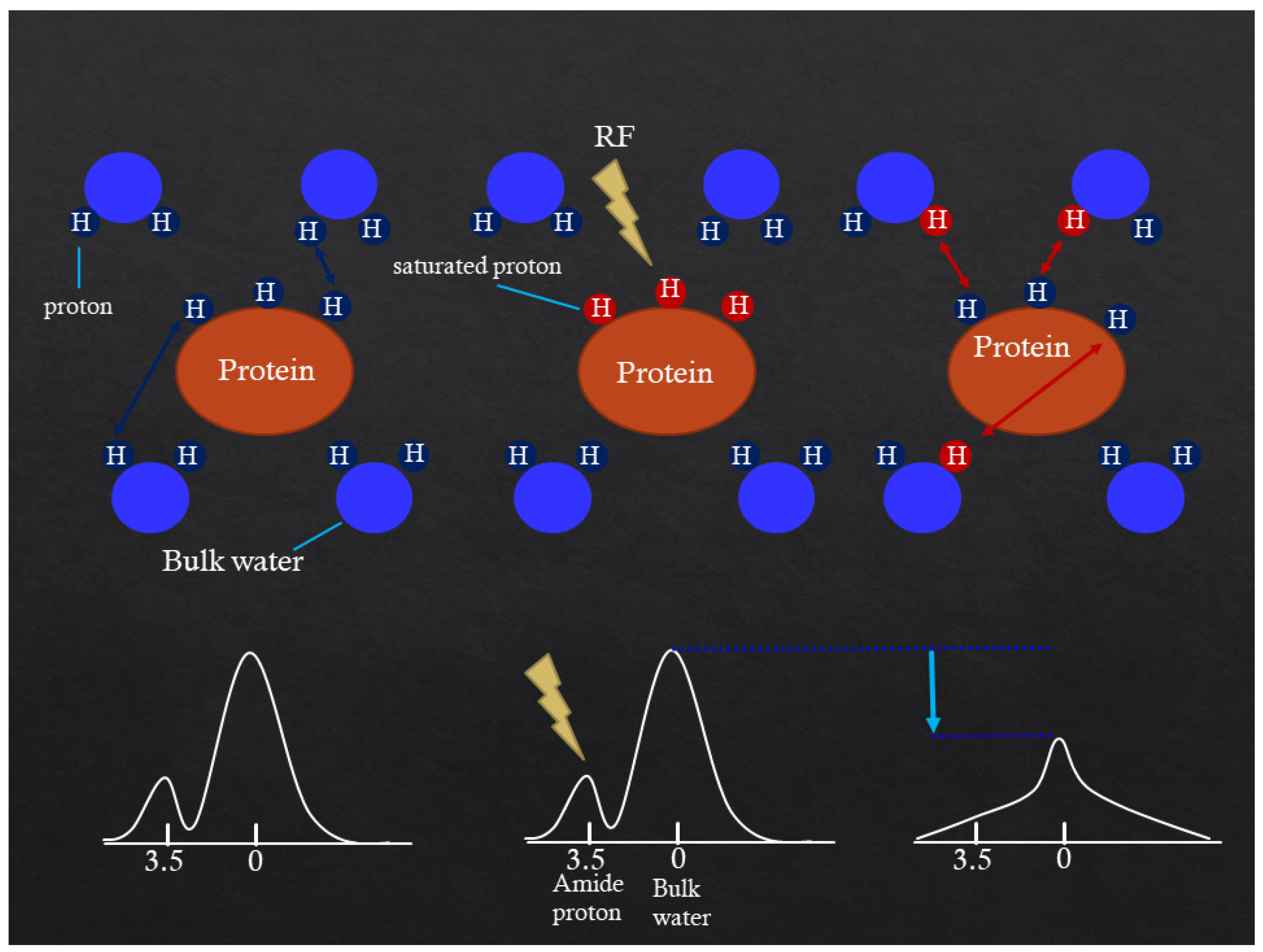
2. Mechanism of APT CEST Imaging
3. MRI Protocol
4. APT-CEST Image Processing
5. APT-CEST Imaging of Malignant Tumor
5.1. Oligodendroglioma
5.2. Diffuse Astrocytoma
5.3. Glioblastoma
5.4. Malignant Lymphoma
5.5. Brain Metastasis
6. APT-CEST Imaging of Meningioma
7. APT-CEST Imaging of Benign Lesion
7.1. Sphenoid Sinus Mucocele
7.2. Solitary Fibrous Tumor
7.3. Schwannoma
7.4. Lipoma
8. APT-CEST Imaging of Demyelinating Disease and Tumor-like Lesion
8.1. Radiation Necrosis
8.2. Leukoencephalopathy
8.3. Tuberous Sclerosis Complex
8.4. Progressive Multifocal Leukoencephalopathy
8.5. Hippocampal Sclerosis
9. Discussion
10. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- van Zijl, P.C.M.; Yadav, N.N. Chemical exchange saturation transfer (CEST): What is in a name and what isn’t? Magn. Reson. Med. 2011, 65, 927–948. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ward, K.M.; Aletras, A.H.; Balaban, R.S. A new class of contrast agents for MRI based on proton chemical exchange dependent saturation transfer (CEST). J. Magn. Reson. 2000, 143, 79–87. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Lal, B.; Wilson, D.A.; Laterra, J.; van Zijl, P.C.M. Amide proton transfer (APT) contrast for imaging of brain tumors. Magn. Reson. Med. 2003, 50, 1120–1126. [Google Scholar] [CrossRef]
- Zhou, J.; Payen, J.F.; Wilson, D.A.; Traystman, R.J.; van Zijl, P.C.M. Using the amide proton signals of intracellular proteins and peptides to detect pH effects in MRI. Nat. Med. 2003, 9, 1085–1090. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Tryggestad, E.; Wen, Z.; Lal, B.; Zhou, T.; Grossman, R.; Wang, S.; Yan, K.; Fu, D.X.; Ford, E.; et al. Differentiation between glioma and radiation necrosis using molecular magnetic resonance imaging of endogenous proteins and peptides. Nat. Med. 2011, 17, 130–134. [Google Scholar] [CrossRef] [Green Version]
- Togao, O.; Yoshiura, T.; Keupp, J.; Hiwatashi, A.; Yamashita, K.; Kikuchi, K.; Suzuki, Y.; Suzuki, S.O.; Iwaki, T.; Hata, N.; et al. Amide proton transfer imaging of adult diffuse gliomas: Correlation with histopathological grades. Neuro Oncol. 2014, 16, 441–448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, J.; Zhu, H.; Lim, M.; Blair, L.; Quinones-Hinojosa, A.; Messina, S.A.; Eberhart, C.G.; Pomper, M.G.; Laterra, J.; Barker, P.B.; et al. Three-dimensional amide proton transfer MR imaging of gliomas: Initial experience and comparison with gadolinium enhancement. J. Magn. Reson. Imaging 2013, 38, 1119–1128. [Google Scholar] [CrossRef] [Green Version]
- Wen, Z.; Hu, S.; Huang, F.; Wang, X.; Guo, L.; Quan, X.; Wang, S.; Zhou, J. MR imaging of high-grade brain tumors using endogenous protein and peptide-based contrast. Neuroimage 2010, 51, 616–622. [Google Scholar] [CrossRef] [Green Version]
- Jones, C.K.; Schlosser, M.J.; van Zijl, P.C.; Pomper, M.G.; Golay, X.; Zhou, J. Amide proton transfer imaging of human brain tumors at 3T. Magn. Reson. Med. 2006, 56, 585–592. [Google Scholar] [CrossRef]
- Sagiyama, K.; Mashimo, T.; Togao, O.; Vemireddy, V.; Hatanpaa, K.J.; Maher, E.A.; Mickey, B.E.; Pan, E.; Sherry, A.D.; Bachoo, R.M.; et al. In vivo chemical exchange saturation transfer imaging allows early detection of a therapeutic response in glioblastoma. Proc. Natl. Acad. Sci. USA 2014, 111, 4542–4547. [Google Scholar] [CrossRef] [Green Version]
- Scheidegger, R.; Wong, E.T.; Alsop, D.C. Contributors to contrast between glioma and brain tissue in chemical exchange saturation transfer sensitive imaging at 3Tesla. Neuroimage 2014, 99, 256–268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ng, M.C.; Hua, J.; Hu, Y.; Luk, K.D.; Lam, E.Y. Magnetization transfer (MT) asymmetry around the water resonance in human cervical spinal cord. J. Magn. Reson. Imaging 2009, 29, 523–528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Z.; Pardini, M.; Yaldizli, Ö.; Sethi, V.; Muhlert, N.; Wheeler-Kingshott, C.A.; Samson, R.S.; Miller, D.H.; Chard, D.T. Magnetization transfer ratio measures in normal-appearing white matter show periventricular gradient abnormalities in multiple sclerosis. Brain 2015, 138, 1239–1246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Henkelman, R.M.; Stanisz, G.J.; Graham, S.J. Magnetization transfer in MRI: A review. NMR Biomed. 2001, 14, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Wesseling, P.; Capper, D. WHO 2016 Classification of Gliomas. Neuropathol. Appl. Neurobiol. 2018, 44, 139–150. [Google Scholar] [CrossRef]
- Wesseling, P.; van den Bent, M.; Perry, A. Oligodendroglioma: Pathology, Molecular Mechanisms and Markers. Acta Neuropathol. 2015, 129, 809–827. [Google Scholar] [CrossRef] [Green Version]
- Louis, D.N.; Perry, A.; Reifenberger, G.; von Deimling, A.; Figarella-Branger, D.; Cavenee, W.K.; Ohgaki, H.; Wiestler, O.D.; Kleihues, P.; Ellison, D.W. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A summary. Acta Neuropathol. 2016, 131, 803–820. [Google Scholar] [CrossRef] [Green Version]
- Kleihues, P.; Soylemezoglu, F.; Schäuble, B.; Scheithauer, B.W.; Burger, P.C. Histopathology, classification, and grading of gliomas. Glia 1995, 15, 211–221. [Google Scholar] [CrossRef]
- Ohgaki, H.; Kleihues, P. Epidemiology and etiology of gliomas. Acta Neuropathol. 2005, 109, 93–108. [Google Scholar] [CrossRef]
- Tamimi, A.F.; Juweid, M. Epidemiology and Outcome of Glioblastoma. Brisbane (AU). In Glioblastoma; Codon Publications: Singapore, 2017. [Google Scholar] [CrossRef]
- Batash, R.; Asna, N.; Schaffer, P.; Francis, N.; Schaffer, M. Glioblastoma Multiforme, Diagnosis and Treatment; Recent Literature Review. Curr. Med. Chem. 2017, 24, 3002–3009. [Google Scholar] [CrossRef]
- Slone, H.W.; Blake, J.J.; Shah, R.; Guttikonda, S.; Bourekas, E.C. CT and MRI findings of intracranial lymphoma. Am. J. Roentgenol. 2005, 184, 1679–1685. [Google Scholar] [CrossRef]
- Schwingel, R.; Reis, F.; Zanardi, V.A.; Queiroz, L.S.; França, M.C., Jr. Central nervous system lymphoma: Magnetic resonance imaging features at presentation. Arq. Neuropsiquiatr. 2012, 70, 97–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dolecek, T.A.; Propp, J.M.; Stroup, N.E.; Kruchko, C. CBTRUS statistical report: Primary brain and central nervous system tumors diagnosed in the United States in 2005–2009. Neuro Oncol. 2012, 14 (Suppl. 5), v1–v49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, S.; Yu, H.; Wang, X.; Lu, S.; Li, Y.; Feng, L.; Zhang, Y.; Heo, H.Y.; Lee, D.H.; Zhou, J.; et al. Molecular MRI differentiation between primary central nervous system lymphomas and high-grade gliomas using endogenous protein-based amide proton transfer MR imaging at 3 Tesla. Eur. Radiol. 2016, 26, 64–71. [Google Scholar] [CrossRef] [Green Version]
- Barnholtz-Sloan, J.S.; Sloan, A.E.; Davis, F.G.; Vigneau, F.D.; Lai, P.; Sawaya, R.E. Incidence proportions of brain metastasis in patients diagnosed (1973 to 2001) in the Metropolitan Detroit Cancer Surveillance System. J. Clin. Oncol. 2004, 22, 2865–2872. [Google Scholar] [CrossRef]
- Yu, H.; Lou, H.; Zou, T.; Wang, X.; Jiang, S.; Huang, Z.; Du, Y.; Jiang, C.; Ma, L.; Zhu, J.; et al. Applying protein-based amide proton transfer MR imaging to distinguish solitary brain metastases from glioblastoma. Eur. Radiol. 2017, 27, 4516–4524. [Google Scholar] [CrossRef] [PubMed]
- Kamimura, K.; Nakajo, M.; Yoneyama, T.; Fukukura, Y.; Hirano, H.; Goto, Y.; Sasaki, M.; Akamine, Y.; Keupp, J.; Yoshiura, T. Histogram analysis of amide proton transfer-weighted imaging: Comparison of glioblastoma and solitary brain metastasis in enhancing tumors and peritumoral regions. Eur. Radiol. 2019, 29, 4133–4140. [Google Scholar] [CrossRef]
- Vernooij, M.; Ikram, M.A.; Tanghe, H.L.; Vincent, A.J.P.E.; Hofman, A.; Krestin, G.P.; Niessen, W.J.; Breteler, M.M.; van der Lugt, A. Incidental findings on brain MRI in the general population. N. Engl. J. Med. 2007, 357, 1821–1828. [Google Scholar] [CrossRef]
- Central Brain Tumor Registry of the United States (CBTRUS). CBTRUS Statistical Report: Primary Brain and Central Nervous System Tumors Diagnosed in the United States in 2004–2006; Central Brain Tumor Registry of the United States (CBTRUS): Hinsdale, IL, USA, 2010. [Google Scholar]
- Louis, D.N.; Ohgaki, H.; Wiestler, O.D.; Cavenee, W.K. WHO Classification of Tumours of the Central Nervous System; IARC: Lyon, France, 2007; pp. 164–172. [Google Scholar] [CrossRef] [Green Version]
- Joo, B.; Han, K.; Choi, Y.S.; Lee, S.K.; Ahn, S.S.; Chang, J.H.; Kang, S.G.; Kim, S.H.; Zhou, J. Amide proton transfer imaging for differentiation of benign and atypical meningiomas. Eur. Radiol. 2018, 28, 331–339. [Google Scholar] [CrossRef]
- Koike, H.; Morikawa, M.; Ideguchi, R.; Uetani, M.; Hiu, T.; Matsuo, T. Amide proton transfer and chemical exchange saturation transfer MRI differentiates between growing and non-growing intracranial meningiomas: A pilot study. Clin. Radiol. 2022, 77, e295–e301. [Google Scholar] [CrossRef]
- Kim, L.J.; Albuquerque, F.C.; Aziz-Sultan, A.; Spetzler, R.F.; McDougall, C.G. Low morbidity associated with use of N-butyl cyanoacrylate liquid adhesive for preoperative transarterial embolization of central nervous system tumors. Neurosurgery 2006, 59, 98–103. [Google Scholar] [CrossRef] [PubMed]
- Sluzewski, M.; van Rooij, W.J.; Lohle, P.N.; Beute, G.N.; Peluso, J.P. Embolization of meningiomas: Comparison of safety between calibrated microspheres and polyvinyl-alcohol particles as embolic agents. Am. J. Neuroradiol. 2013, 34, 727–729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friedman, A.; Batra, P.S.; Fakhri, S.; Citardi, M.J.; Lanza, D.C. Isolated sphenoid sinus disease: Etiology and management. Otolaryngol. Head Neck Surg. 2005, 133, 544–550. [Google Scholar] [CrossRef]
- Dalaqua, M.; do Nascimento, F.B.P.; Miura, L.K.; Garcia, M.R.T.; Barbosa Junior, A.A.; Reis, F. Magnetic resonance imaging of the cranial nerves in infectious, neoplastic, and demyelinating diseases, as well as other inflammatory diseases: A pictorial essay. Radiol. Bras. 2022, 55, 38–46. [Google Scholar] [CrossRef]
- Koike, H.; Morikawa, M.; Ishimaru, H.; Ideguchi, R.; Uetani, M.; Hiu, T.; Matsuo, T.; Miyoshi, M. Quantitative Chemical Exchange Saturation Transfer Imaging of Amide Proton Transfer Differentiates between Cerebellopontine Angle Schwannoma and Meningioma: Preliminary Results. Int. J. Mol. Sci. 2022, 23, 10187. [Google Scholar] [CrossRef] [PubMed]
- Loddenkemper, T.; Morris, H.H.; Diehl, B.; Lachhwani, D.K. Intracranial lipomas and epilepsy. J. Neurol. 2006, 253, 590–593. [Google Scholar] [CrossRef]
- Jabot, G.; Stoquart-Elsankari, S.; Saliou, G.; Toussaint, P.; Deramond, H.; Lehmann, P. Intracranial lipomas: Clinical appearances on neuroimaging and clinical significance. J. Neurol. 2009, 256, 851–855. [Google Scholar] [CrossRef] [PubMed]
- Yildiz, H.; Hakyemez, B.; Koroglu, M.; Yesildag, A.; Baykal, B. Intracranial lipomas: Importance of localization. Neuroradiology 2006, 48, 1–7. [Google Scholar] [CrossRef]
- Truwit, C.L.; Barkovich, A.J. Pathogenesis of intracranial lipoma: An MR study in 42 patients. Am. J. Neuroradiol. 1990, 11, 665–674. [Google Scholar] [CrossRef]
- Cheung, M.C.; Chan, A.S.; Law, A.C.; Chan, J.H.; Tse, V.K. Impact of radionecrosis on cognitive dysfunction in patients after radiotherapy for nasopharyngeal carcinoma. Cancer 2003, 97, 2019–2026. [Google Scholar] [CrossRef]
- Filley, C.M.; Kleinschmidt-DeMasters, B.K. Toxic leukoencephalopathy. N. Engl. J. Med. 2001, 345, 425–432. [Google Scholar] [CrossRef] [PubMed]
- Sparagana, S.P.; Roach, E.S. Tuberous sclerosis complex. Curr. Opin. Neurol. 2000, 13, 115–119. [Google Scholar] [CrossRef] [PubMed]
- Koralnik, I.J. Progressive multifocal leukoencephalopathy revisited: Has the disease outgrown its name? Ann. Neurol. 2006, 60, 162–173. [Google Scholar] [CrossRef]
- Major, E.O.; Yousry, T.A.; Clifford, D.B. Pathogenesis of progressive multifocal leukoencephalopathy and risks associated with treatments for multiple sclerosis: A decade of lessons learned. Lancet Neurol. 2018, 17, 467–480. [Google Scholar] [CrossRef] [Green Version]
- Yang, C.-D.; Wang, X.-D.; Ye, S.; Gu, Y.-Y.; Bao, C.-D.; Wang, Y.; Chen, S.-L. Clinical features, prognostic and risk factors of central nervous system infections in patients with systemic lupus erythematosus. Clin. Rheumatol. 2007, 26, 895–901. [Google Scholar] [CrossRef] [PubMed]
- de Amorim, J.C.; Torricelli, A.K.; Frittoli, R.B.; Lapa, A.T.; Dertkigil, S.S.J.; Reis, F.; Costallat, L.T.; França Junior, M.C.; Appenzeller, S. Mimickers of neuropsychiatric manifestations in systemic lupus erythematosus. Best Pract. Res. Clin. Rheumatol. 2018, 32, 623–639. [Google Scholar] [CrossRef]
- Blumcke, I.; Spreafico, R. Cause matters: A neuropathological challenge to human epilepsies. Brain Pathol. 2012, 22, 347–349. [Google Scholar] [CrossRef]
- Gomez-Brouchet, A.; Delisle, M.B.; Cognard, C.; Bonafe, A.; Charlet, J.P.; Deguine, O.; Fraysse, B. Vestibular schwannomas: Correlations between magnetic resonance imaging and histopathologic appearance. Otol. Neurotol. 2001, 22, 79–86. [Google Scholar] [CrossRef]
- Zhang, H.-W.; Liu, X.-L.; Zhang, H.-B.; Li, Y.-Q.; Wang, Y.-L.; Feng, Y.-N.; Deng, K.; Lei, Y.; Huang, B.; Lin, F. Differentiation of Meningiomas and Gliomas by Amide Proton Transfer Imaging: A Preliminary Study of Brain Tumour Infiltration. Front. Oncol. 2022, 12, 886968. [Google Scholar] [CrossRef]





















Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koike, H.; Morikawa, M.; Ishimaru, H.; Ideguchi, R.; Uetani, M.; Miyoshi, M. Amide Proton Transfer–Chemical Exchange Saturation Transfer Imaging of Intracranial Brain Tumors and Tumor-like Lesions: Our Experience and a Review. Diagnostics 2023, 13, 914. https://doi.org/10.3390/diagnostics13050914
Koike H, Morikawa M, Ishimaru H, Ideguchi R, Uetani M, Miyoshi M. Amide Proton Transfer–Chemical Exchange Saturation Transfer Imaging of Intracranial Brain Tumors and Tumor-like Lesions: Our Experience and a Review. Diagnostics. 2023; 13(5):914. https://doi.org/10.3390/diagnostics13050914
Chicago/Turabian StyleKoike, Hirofumi, Minoru Morikawa, Hideki Ishimaru, Reiko Ideguchi, Masataka Uetani, and Mitsuharu Miyoshi. 2023. "Amide Proton Transfer–Chemical Exchange Saturation Transfer Imaging of Intracranial Brain Tumors and Tumor-like Lesions: Our Experience and a Review" Diagnostics 13, no. 5: 914. https://doi.org/10.3390/diagnostics13050914
APA StyleKoike, H., Morikawa, M., Ishimaru, H., Ideguchi, R., Uetani, M., & Miyoshi, M. (2023). Amide Proton Transfer–Chemical Exchange Saturation Transfer Imaging of Intracranial Brain Tumors and Tumor-like Lesions: Our Experience and a Review. Diagnostics, 13(5), 914. https://doi.org/10.3390/diagnostics13050914